
Abstract
Background and Objective. Mirror therapy is a new form of stroke rehabilitation that uses the mirror reflection of the unaffected hand in place of the affected hand to augment movement training. The mechanism of mirror therapy is not known but is thought to involve changes in cerebral organization. We used magnetoencephalography (MEG) to measure changes in cortical activity during mirror training after stroke. In particular, we examined movement-related changes in the power of cortical oscillations in the beta (15-30 Hz) frequency range, known to be involved in movement. Methods. Ten stroke patients with upper limb paresis and 13 healthy controls were recorded using MEG while performing bimanual hand movements in 2 different conditions. In one, subjects looked directly at their affected hand (or dominant hand in controls), and in the other, they looked at a mirror reflection of their unaffected hand in place of their affected hand. The movement-related beta desynchronization was calculated in both primary motor cortices. Results. Movement-related beta desynchronization was symmetrical during bilateral movement and unaltered by the mirror condition in controls. In the patients, movement-related beta desynchronization was generally smaller than in controls, but greater in contralesional compared to ipsilesional motor cortex. This initial asymmetry in movement-related beta desynchronization between hemispheres was made more symmetrical by the presence of the mirror. Conclusions. Mirror therapy could potentially aid stroke rehabilitation by normalizing an asymmetrical pattern of movement-related beta desynchronization in primary motor cortices during bilateral movement.
Introduction
Mirror therapy (MT) is emerging as an adjunct to physical therapy in the treatment of upper limb impairment after stroke.1,2 MT involves asking patients to attempt synchronous bilateral hand movements while observing the mirror reflection of their unaffected limb in the position of their affected limb. MT has been found to have a significant positive effect on motor function in stroke patients, 3 but there is little understanding as to its mechanism of action.
Studies have been performed using mirror visual feedback in healthy subjects using both transcranial magnetic stimulation (TMS) and functional magnetic resonance imaging (fMRI). TMS studies using MT found that it increased excitability in primary motor cortex (M1) in both hemispheres,4-6 but this has not been tested in stroke patients.
A number of fMRI studies have investigated using mirror visual feedback in healthy subjects using unimanual movements and have found areas that differ in their activation between mirror and no mirror conditions.7-9 Most of these were areas outside the motor network, although Hamzei et al 8 did find changes in premotor areas during MT.
The few fMRI studies to explore MT in stroke patients have used protocols that do not match what is performed in a clinical setting (ie, bilateral movement with mirror reflection of unaffected hand in place of affected hand).10,11 Michielsen et al 12 recorded fMRI while performing MT with bilateral movement but found no main effect of mirror. They performed another study exploring the effect of 6 weeks training with MT and observed a shift of brain activation evoked by movement of the affected hand toward the lesioned hemisphere. 13
Based on the studies described above, we hypothesized that MT acts by simultaneously enhancing the potential for neuroplastic change in surviving motor regions and networks, and then taking advantage of this enhancement with concurrent repeated movement. In this study, we therefore asked both healthy subjects and stroke patients to perform movements using mirror visual feedback while measuring brain activity using magnetoencephalography (MEG). MEG is a brain imaging technique that directly measures cortical neural activity at different frequencies (termed oscillations), and unlike blood oxygenation level dependent signal used by fMRI, it is unaffected by neurovascular uncoupling. MEG can detect the oscillatory signals generated predominantly by changes in the postsynaptic fields of pyramidal cells. 14 Pyramidal cells are reciprocally connected to GABAergic interneurons and so changes in oscillatory signals are dependent on the balance between inhibition and excitation within these microcircuits. 15 As such, it is possible that oscillatory changes could tell us something about the potential for both local and network plasticity; however, there is much more to be understood about this relationship. 16 Oscillations in the beta frequency band (15-30 Hz) are known to be important in movement. In M1, they are present at rest and are suppressed during movement (movement-related beta desynchronization [MRBD]). 17 The power of resting beta oscillations and MRBD are both enhanced by benzodiazepines (GABAA-agonists), suggesting they reflect the degree of GABAergic inhibition in M1.18,19 MEG has been used to examine changes in beta oscillations during MT and concurrent median nerve stimulation in healthy subjects20,21 but MT has not been assessed in stroke patients.
In this study, we were interested in the effect of MT on beta oscillations during movement. We were keen to assess MRBD during attempted movement in these patients (ie, practice) as motor practice is what will drive behavioral improvement.
MEG studies of bilateral hand movement performed by healthy volunteers have observed that beta power in both primary motor cortices decreases during movement,22,23 and here given that our paradigm involves synchronous bilateral hand movements, we expected to see the same. Following stroke, however, there is thought to be a disruption in the relationship between motor cortices in each hemisphere.24,25 Specifically, just prior to movement, there is an increased level of inhibition from contralesional to ipsilesional M1. 25 Although this finding was observed during unilateral movement, we hypothesize that a similar reduction in contralesional to ipsilesional M1 interhemispheric inhibition during bilateral hand movement in our patient group might occur and be reflected in altered MRBD. If this were the case, we would not see such a symmetrical change in MRBD in our patients compared to controls, and in particular we would expect MRBD to be enhanced in M1 of the lesioned hemisphere, reflecting increased overall levels of task-related inhibition in this cortical region. The key question is then how does adding in MT to bilateral hand movement alter this, and it is tempting to speculate that MT may “normalize” this imbalance. In this study, we therefore hypothesized that (a) in healthy controls, during bilateral movement, there would be a symmetrical decrease in beta band power in both primary motor cortices; (b) following stroke, MRBD during bilateral movement would not be symmetrical, but would be greater (ie, a larger decrease) in the lesioned hemisphere reflecting increased inhibition; and (c) MT would normalize this imbalance in the patient group. Given that our protocol is identical to that implemented in clinical practice, we suggest that this differential interaction between MT and hemisphere in stroke patients and controls might represent its mechanism of action.
Materials and Methods
Subjects
Ten stroke patients (mean age 56 ± 12 years, range 30-71 years, 3 female, 6 dominant-hand affected, 1 left-handed) and 13 control participants were recruited to this study (mean age 45 ± 15 years, age range 22-67 years, 9 female, 2 left-handed). All patients suffered from first-ever stroke and weakness of at least wrist and finger extensors and hand interossei. Patients were not suffering from any other neurological disorder. Full written consent was obtained from all subjects in accordance with the Declaration of Helsinki. The study was approved by the Joint Ethics Committee of the Institute of Neurology, UCL and National Hospital for Neurology and Neurosurgery, UCL Hospitals NHS Foundation Trust, London.
Behavioral Testing
All stroke patients were scored on the Nine Hole Peg Test (NHPT), Action Research Arm Test (ARAT), Box and Blocks test and Grip strength. All scores were given in terms of measures for the affected hand as a percentage of the unaffected hand. A principal component analysis (PCA) was performed on all behavioral scores in order to account for ceiling and floor effects in these measures and to create a single motor impairment score (a lower PCA score corresponding to greater impairment).
Motor Task
Subjects made alternating flexion and extension movements synchronously with both hands in response to an auditory cue every 5 seconds. There were 2 cues, one high pitch followed by one at a lower pitch (this alternated between the 2 across the recording) and the participant was asked to open their hand (extension) on the high pitch cue and close their hand into a fist (flexion) on the low pitch cue. The participants were instructed to relax their hands after having made each movement. The movements were performed in 2 different conditions. Patients looked either toward their affected hand (1) directly (no mirror) or (2) as a reflection of their unaffected hand (mirror) (Figure 1). Controls looked either toward their dominant hand (1) directly (no mirror) or (2) as a reflection of their nondominant hand (mirror), but gaze was always in the same direction in all subjects. The other hand was covered up in order not to distract from the observed/mirrored hand. The order of conditions was randomized. There were 60 movements in each block, 30 flexion and 30 extension, each block lasting 5 minutes.
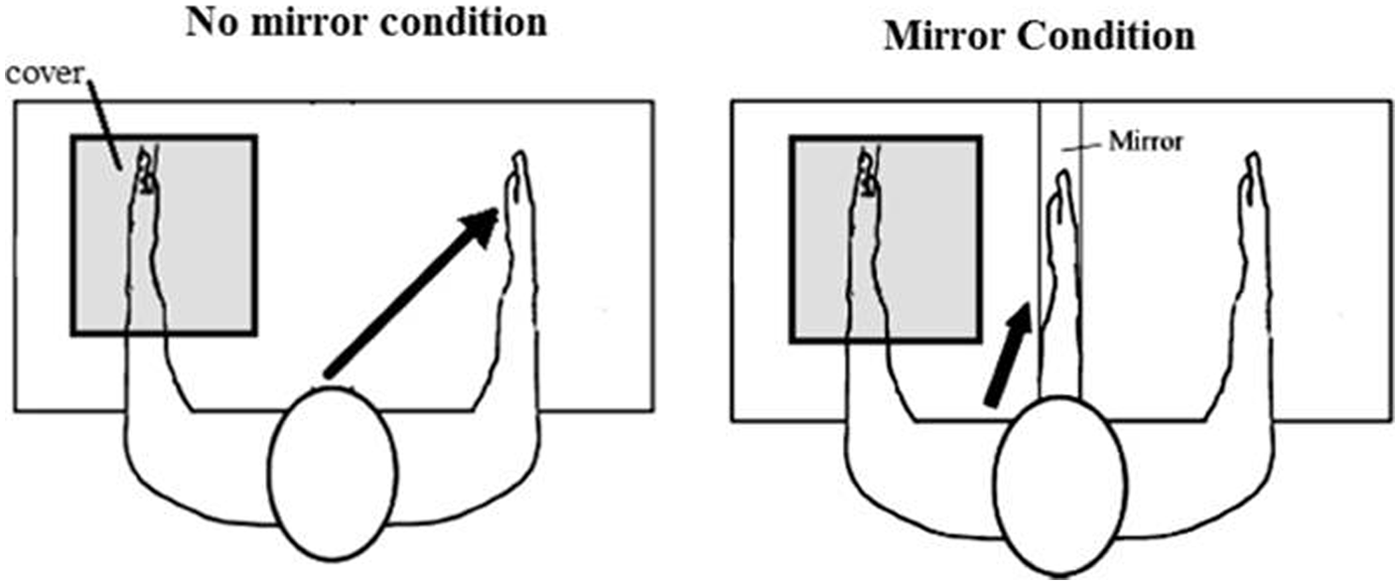
Illustration of experimental conditions.
Data Analysis
MEG signals were measured continuously during the task using a whole-head CTF Omega 275 MEG system (CTF, Vancouver, Canada).
Head localization was monitored continuously during the MEG recordings to check for excessive movement. The MEG data were preprocessed offline using SPM8 (Wellcome Trust Centre for Neuroimaging, www.fil.ion.ucl.ac.uk/spm). 26 EMG was recorded from the forearm muscles as part of the MEG data set. Data were down-sampled to 300 Hz and were filtered from 5 to 100 Hz. Data were epoched from −2.5 seconds to +2.5 seconds where time 0 indicated onset of the auditory cue. The different pitch auditory cues had different markers, and therefore at this stage, the data were split into flexion and extension movements and analyzed separately. Trials with large eye blinks or other artifacts were excluded.
Coregistration to the Montreal Neurological Institute (MNI) coordinates was based on 3 fiducial points: nasion and left and right preauricular points. We used a single-shell (rather than single sphere) model fit, based on spherical harmonic series, 27 to the inner skull surface of the inverse normalized SPM template to more precisely characterize the MEG forward model.
Oscillatory changes in the beta band between rest and grip were localized using the Linearly Constrained Maximal Variance (LCMV) beamformer28,29 as part of the SPM8 software. The beamforming method is based on the linear projection of sensor data using a spatial filter computed from the lead field of the source of interest and the data covariance. 30 We computed the data covariance matrix using 2 time windows (passive and active). The passive time window was taken from −2 seconds to −1 seconds with 0 as the onset of the auditory cue. The active time window was from 0.35 to 1.35 seconds following the auditory cue onset, this was guided by the EMG across participants. The frequency band used for the beamformer was 15 to 30 Hz. We made volumetric t-statistic images per subject using a grid spacing of 10 mm. At each location, the source orientation was taken to be in the direction yielding maximal signal variance. 31 From these t-statistic images, we extracted the source signal from the location of peak change in beta power (15-30 Hz) within the primary motor cortices both contralateral (CM1) and ipsilateral (IM1) to the observed hand. Morlet-wavelet time-frequency analysis was used to explore the changes in beta across a trial from these locations. The spectrograms were rescaled to show percentage change from baseline (−2.5 seconds to 0 seconds) and averaged across trials. The mean movement-related percentage beta desynchronization (MRBD; 15-30 Hz) was then extracted from the 2-seconds movement period for primary motor cortex contralateral to the hand being observed (CM1) and ipsilateral to the hand being observed (IM1) for each participant.
A mixed-effects ANOVA was performed on MRBD comprising 2 within-subjects factors (mirror, hemisphere) and 1 between-subjects factor (group). This was done for both flexion and extension movements separately. A correlation was performed on MRBD and motor impairment.
An asymmetry index was also calculated from the MRBD values by taking (CM1_MRBD − IM1_MRBD)/(CM1_MRBD + IM1_MRBD). A mixed-effects ANOVA was performed on this index with the within-subject factor of mirror (no mirror vs mirror conditions) and the between subjects factor of group (patients vs controls).
T-tests were then performed as post hoc analysis to interpret further the results of the ANOVA.
Results
Behavioral scores were as follows (all scores given with affected hand as percentage of unaffected hand); NHPT mean = 25 ± 23%, box and block mean = 42 ± 29%, grip strength mean = 51 ± 30%, ARAT mean = 70 ± 31%. The raw behavioral scores are shown in Table 1. Lesion maps for all patients can be seen in Figure 5.
Demographic Information and Raw Behavioral Scores for Each Patient’s Affected (Aff) and Unaffected (Un) Hand on the 4 Motor Tasks Performed.
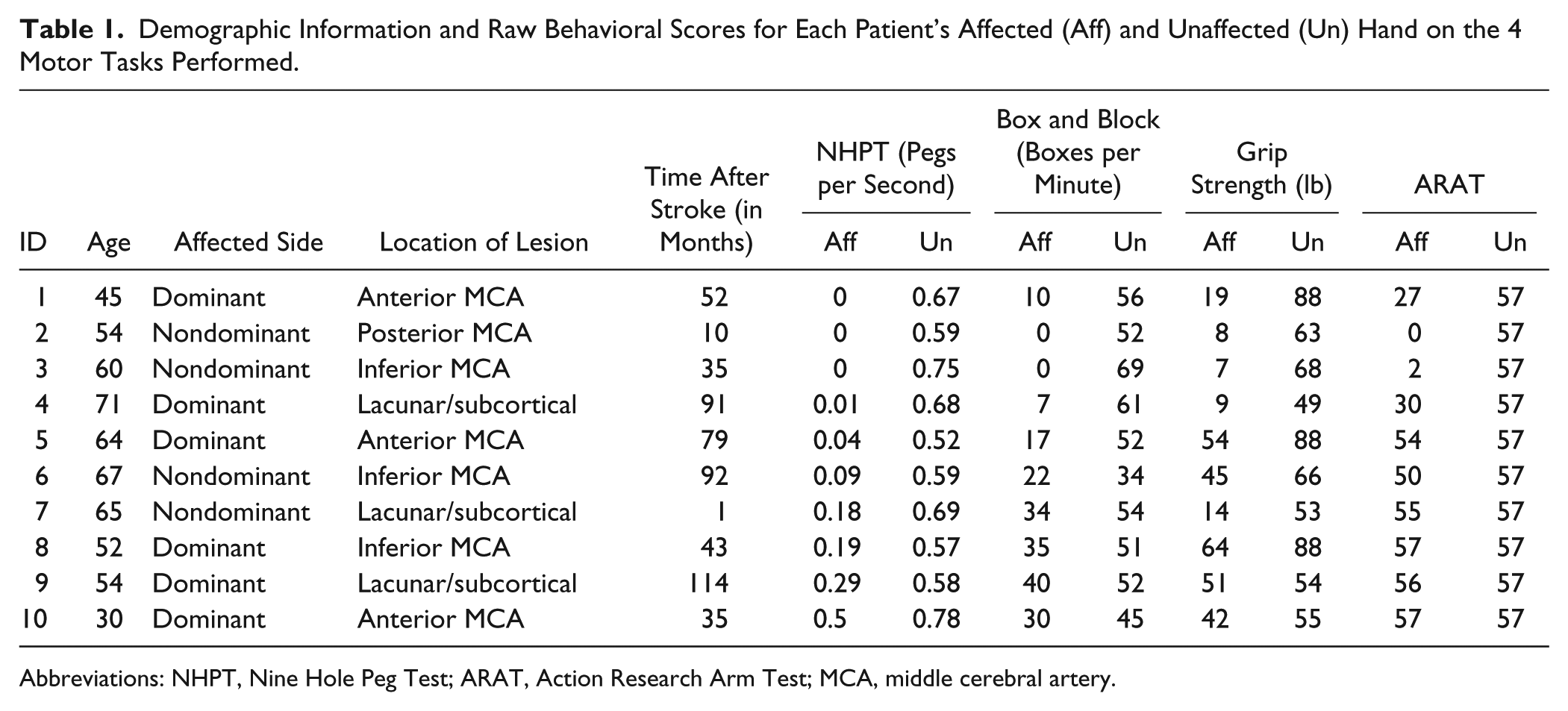
Abbreviations: NHPT, Nine Hole Peg Test; ARAT, Action Research Arm Test; MCA, middle cerebral artery.
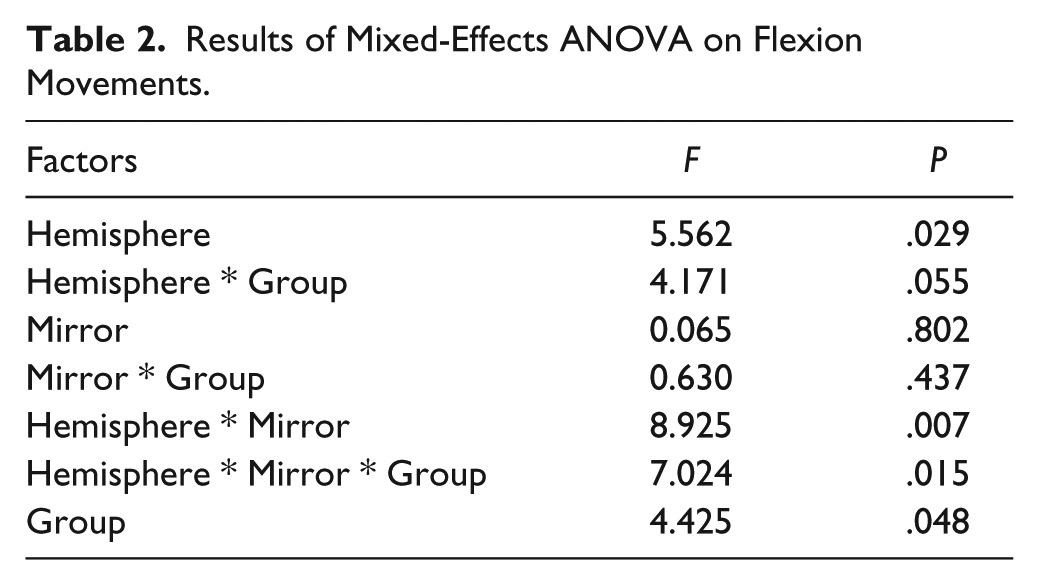
Figure 2 shows group average time-frequency spectrograms for each condition; beta MRBD is clear in all conditions as a blue patch following the auditory cue to move at 0 seconds. An ANOVA of MRBD focusing on flexion movements revealed a significant effect of group (F = 4.43, P = .048) and of hemisphere (F = 5.56, P = .03), a significant interaction between hemisphere and mirror condition (F = 8.93, P = .007) and also a significant 3-way interaction between hemisphere * mirror * group (F = 7.02, P = .015). Table 2 shows all the results of this ANOVA. Performing post hoc t-tests on these data, we find that in the no mirror condition of the contralateral M1, there is a significantly smaller MRBD in patients than controls (P = .01). There is also a significantly smaller MRBD in CM1 as compared to IM1 in the no mirror condition in the patient group (P = .005).
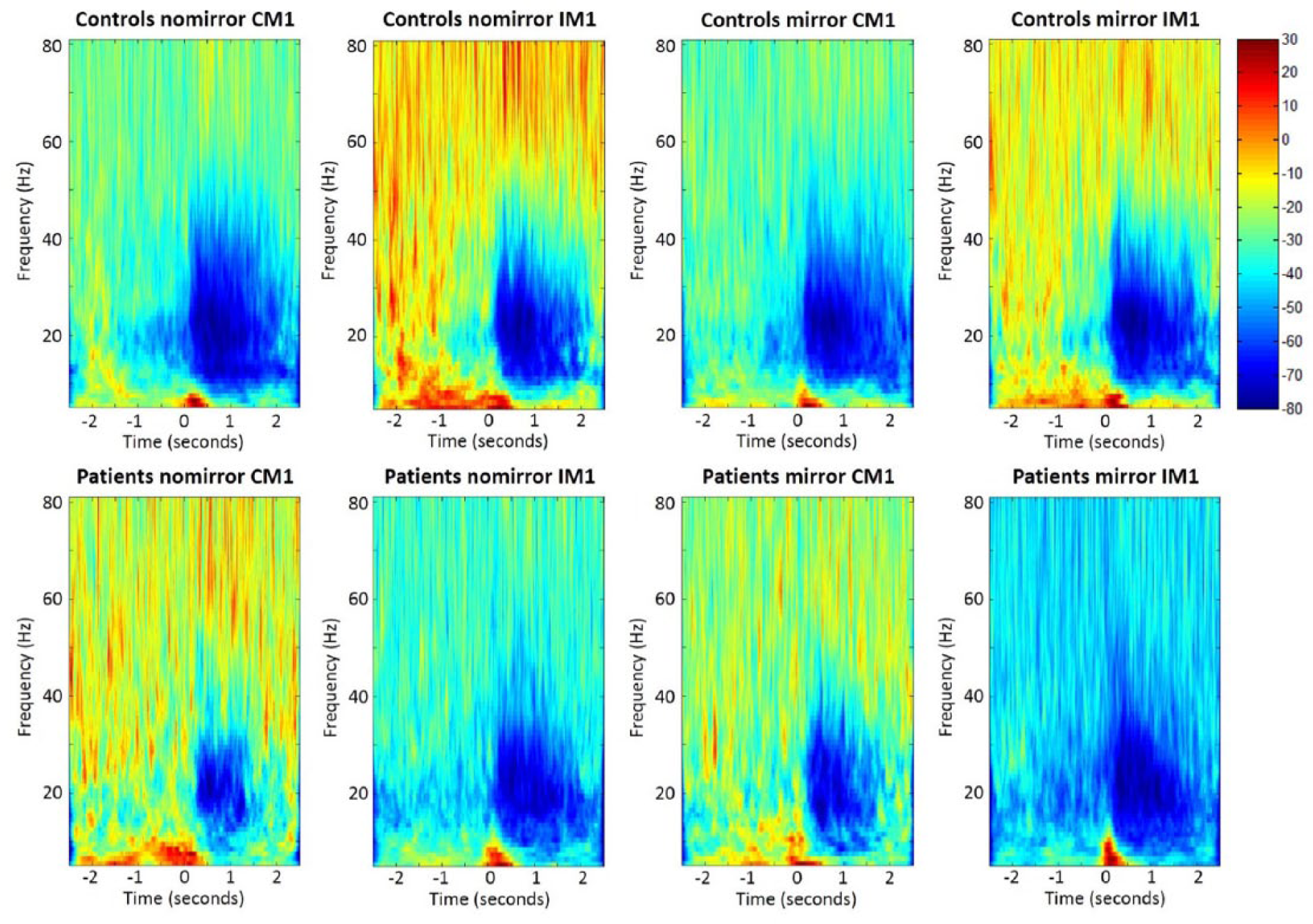
Group-averaged spectrograms of each condition with controls on the top row and stroke patients on the bottom row.
Results of Mixed-Effects ANOVA on Flexion Movements.
An ANOVA of the asymmetry index for flexion movements indicated that there was a very significant effect of condition (F = 9.09, P = .007). The effect of group did not quite reach significance (F = 3.89, P = .063); however, there was a significant interaction between condition and group (F = 7.20, P = .014). Performing post hoc t-tests on these data, we find that there is a significant difference in the asymmetry index between patients and controls in the no mirror condition (P = .009) and that there is a significant difference between the mirror versus no mirror condition in patients (P = .02). So the asymmetry index was different between patients and controls in the control no mirror condition, and in the patient group, the asymmetry index was altered by the addition of the mirror. This can be seen in the box plot in Figure 4.
Figure 3 shows a summary of MRBD across all these conditions. MRBD was smaller in patients compared to controls, especially in CM1 (M1 of the lesioned hemisphere in patients). In the control group, there was no effect of mirror condition on MRBD in either hemisphere. However, in the patient group, MRBD was greater in IM1 (M1 of the intact hemisphere) than CM1 (M1 of the lesioned hemisphere). Furthermore, the presence of the mirror reduced MRBD in IM1 but increased it in CM1. In other words, MRBD became less asymmetric when the mirror was introduced.
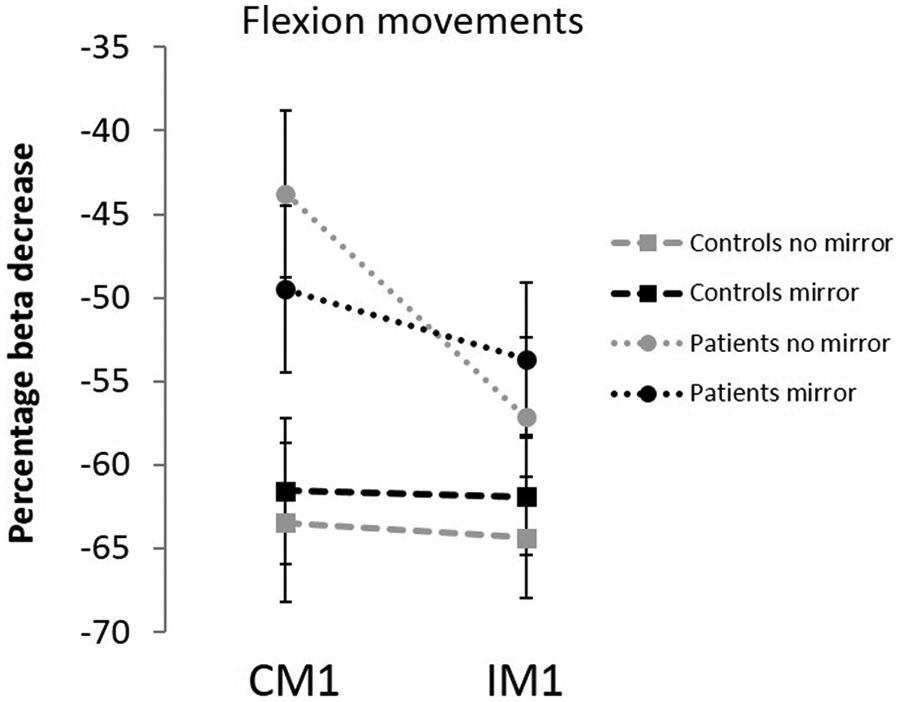
Movement-related beta desynchronization (MRBD) during bilateral hand movement.
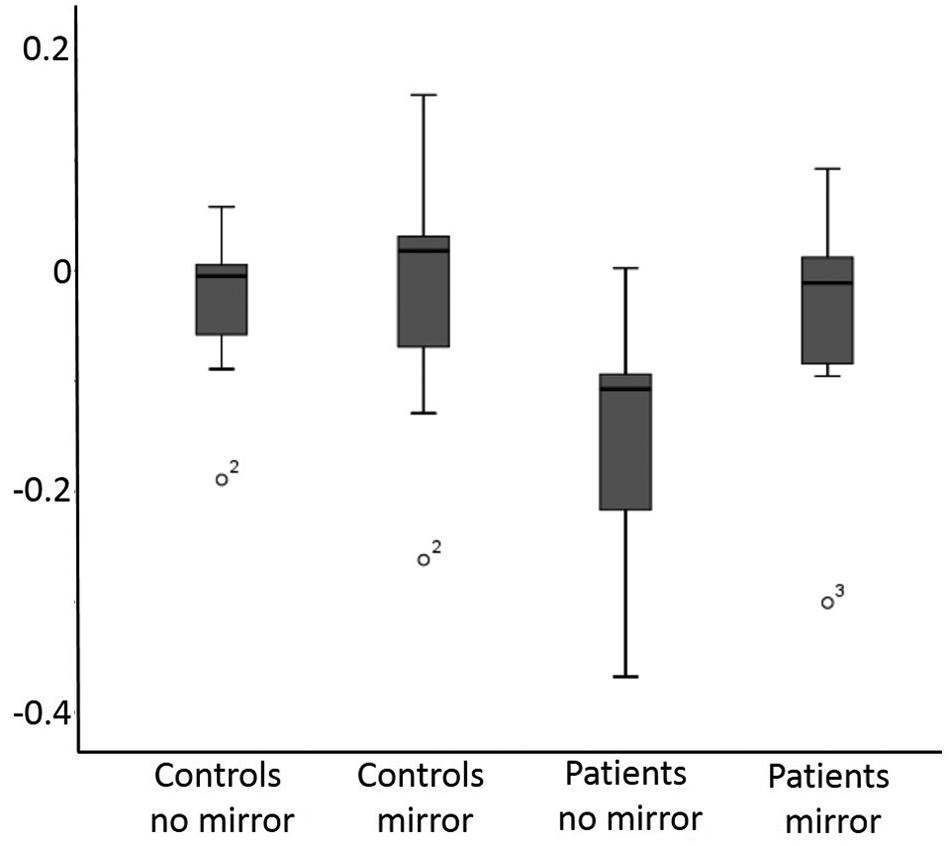
Box plot of asymmetry index for patients and controls in both no mirror and mirror conditions.
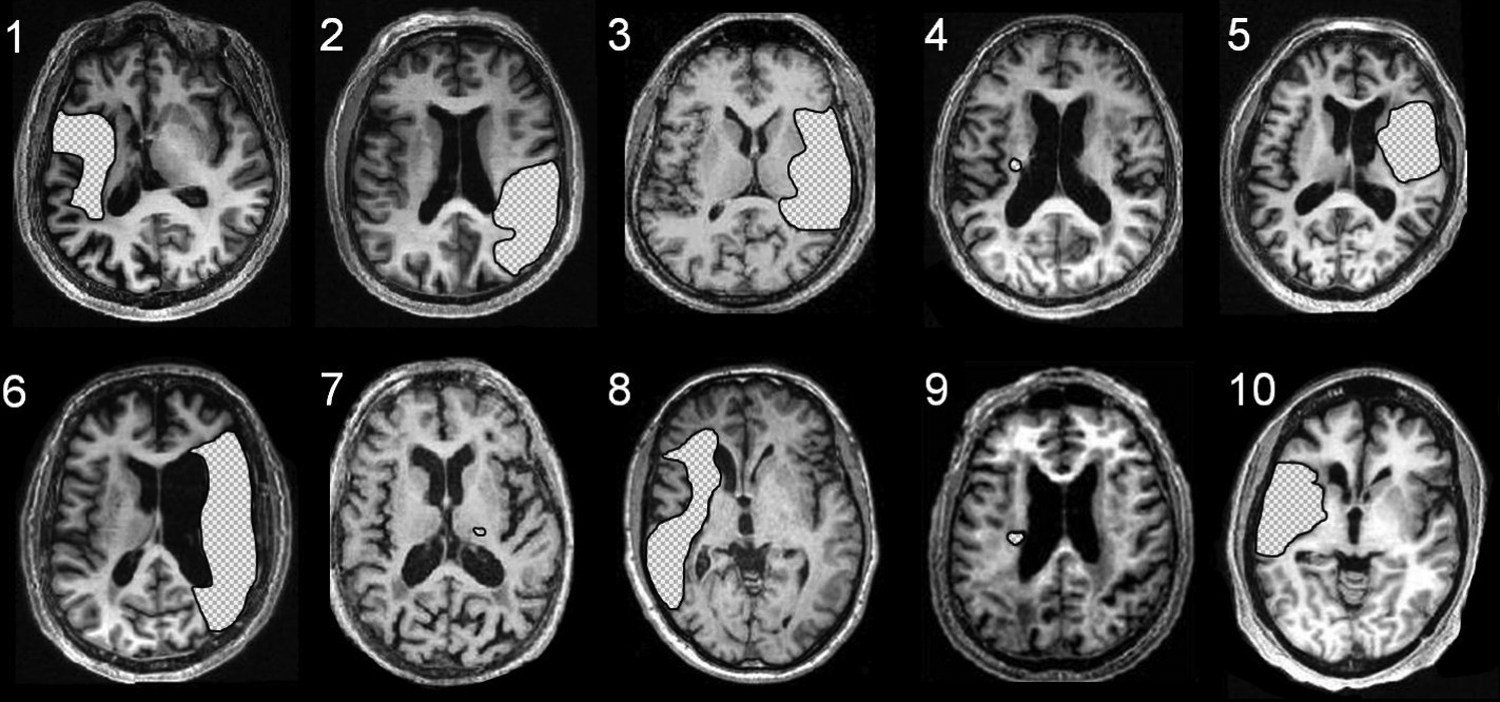
Location of each patient’s lesion shown as axial sections on their structural MRIs.
Baseline beta values were extracted and no significant differences were found in beta values at rest between patients and controls. We also explored mu oscillations (7-14 Hz) and saw a desynchronization in this frequency during movement. When an ANOVA was performed on these data using the same factors as in the beta band, a significant difference was found between patients and controls but no differences were found due to hemisphere or mirror condition. MRBD in both CM1 and IM1 was not found to correlate with motor impairment in any of the conditions. With regard to extension movements, there were no significant differences in any of the comparisons including the ANOVAs.
Discussion
Our results show that the effect of MT on motor cortex function in each hemisphere during bilateral hand movements was different in stroke patients compared to healthy controls. In controls, MRBD was the same in each hemisphere and unaltered by MT. In the patient group, however, an imbalance in MRBD between hemispheres during bilateral hand movement was made more symmetrical by MT (Figure 3). It is interesting to consider what this tells us about how MT might work. One possibility is that relative change in MRBD in each hemisphere represents a “normalization” of the balance in motor cortex activity in ipsilesional and contralesional hemispheres.
The balance of activity between ipsilesional and contralesional motor cortices after stroke has been investigated in previous work. For example, excessive task-related inhibition from contralesional to ipsilesional motor cortex has been observed following stroke. 25 Indeed, a number of noninvasive brain stimulation studies have attempted to reverse this imbalance and so facilitate recovery after stroke by reducing excitability in contralesional motor cortex. This finding was obtained during unimanual affected hand movement, and so may not be relevant for interpreting our findings during bilateral movement. In our study, MRBD was equal in both hemispheres during bilateral movements in healthy controls but not in patients. MRBD in the ipsilateral (contralesional) M1 was larger than in contralateral (ipsilesional) M1 pointing to a significant imbalance of activity between hemispheres before MT was introduced. With the mirror in place, this asymmetry of MRBD became less marked in patients, but was unaltered in healthy controls. This “normalization” of MRBD balance between the hemispheres could represent a readjustment of a stroke-related excitatory–inhibitory imbalance between the 2 motor cortices, creating a pattern of activity more similar to healthy controls.
It is tempting to speculate whether the effect of MT is related to differential effects on movement-related intracortical GABAergic inhibition in each hemisphere. From what we know about the relationship between beta power and intracortical GABAergic inhibition,18,19 our results suggest that in stroke patients, MT reduces GABAergic inhibition in contralesional rather than M1 of the lesioned hemisphere. A reduction in inhibitory mechanisms is thought to be an important factor in enhancing long-term potentiation and therefore experience-dependent plasticity.32,33 This might suggest that in the patient group, we see an increase in the potential for experience-dependent plasticity during the mirror condition in the ipsilateral (contralesional) M1 rather than the contralateral (ipsilesional) M1. Although this might seem surprising at first, there is a body of literature indicating that the activations seen in contralesional motor cortex following stroke can aid functional recovery. 34 Nevertheless, it seems more likely that MT involving bilateral movement works through altering the balance of activity between hemispheres rather than on one hemisphere or the other. Although our results do not specifically measure interhemispheric influences, they do point toward alterations in hemispheric balance.
Generally, the studies that have looked at the mirror illusion in fMRI have not performed MT as it would be done clinically (ie, bilateral movement with a mirror in place of the affected hand), they have mainly used unilateral movements11,12 and some have used virtual reality videos of hand movements in place of a mirror setup. 10 In the present study, we were careful to use a protocol that reflected a clinical MT protocol and so we feel more able to relate our results to a mechanism of the clinically applied MT.
In this study, we found no correlation between MRBD and motor impairment. This is in keeping with the findings of Saleh et al who found no correlation between degree of fMRI activation and hand function in stroke patients during the mirror condition. 10 This suggests that if our findings reflect the mechanism of action of MT, then it would work as effectively in patients with differing levels of impairment. We studied patients with a wide range of impairment and also a varying amount of time after stroke. This wide range of time after stroke may have led to greater variability in our results as the excitatory–inhibitory balance may vary at different stages following stroke. Having said that, all but one of our patients were at a chronic stage (see Table 1) and so are likely to have plateaued in terms of their recovery. We also performed a correlation between months after stroke and MRBD amplitude in the patient group and this was not found to be significant (P > .24). It would be of interest to look longitudinally at these changes within patients and see how these results changed over time. There was also a mixture of dominant and nondominant hemisphere affected, which may have added to the variability across patients. The fact that we see a change in the MRBD despite these sources of variability might point to the general applicability of MT, but the effects of these sources of variability need to be explored further in larger groups to be certain.
Anecdotally, most patients were very engaged in the therapy and were often fascinated by the illusion of seeing the reflection of their unaffected hand. It would be interesting to investigate the effect of the belief in the illusion on the results we describe here. It is possible that stronger effects are seen in those with a more convincing illusion.
No significant differences were found between MT and non-MT conditions during extension movements. Finger extension was generally more difficult than flexion for our stroke patients. It might be that some degree of illusion is required for the effect and this is more difficult when the discrepancy between real and mirrored movement is too great. This could obviously have a negative effect on the applicability of MT clinically.
There was some difference in the average age between patients and controls, but having correlated all MRBD measures with age in the control group, there was no significant correlation and so we do not believe that this would have unduly affected our results.
Structural information on the site of stroke was not available for all patients and therefore it is not possible to make any statement about how this may have affected MRBD in our study. It would be interesting to investigate how MRBD results may be affected by lesion location/volume in a future study.
In this study, we chose to use observation of the dominant hand in our healthy subjects as a control comparison to observation of the affected hand. In a previous data set, we have directly compared nondominant and dominant hand measures of MRBD in a control group while performing unimanual movements and found no significant differences (under review) so we were comfortable using the dominant hand as a comparison. Also, in this study participants were performing bilateral movement and it was only the focus of their gaze that was toward the dominant hand. We would not expect this to make a significant difference as the controls were receiving the same visual feedback in the mirror and no-mirror condition as they could complete the movement correctly. The control group provided a baseline level of MRBD as a comparison for the patients and the direction of their gaze is unlikely to have influenced the results in this case.
As the patients were impaired, the movement amplitude and accuracy is likely to have differed between patients and controls. While this is a possible limitation, it is unlikely to explain the difference due to the addition of the mirror in the patient group.
In summary, this study is the first to measure cortical activity directly during MT using MEG and to examine the differential effects in controls and stroke patients. Our results suggest a rebalancing of MRBD between hemispheres in stroke patients. Alterations in beta oscillations have been linked to changes in intracortical GABAergic inhibitory function, and it is interesting to speculate on whether our results reflect an MT-enhanced potential for experience-dependent plasticity within motor networks. In future studies, it would be of interest to determine whether the effects of MT on cortical physiology that we have observed here are necessary (ie, biomarkers) for a beneficial effect on motor function.
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This research was supported by the European Commission under the 7th Framework Program-HEALTH-Collaborative Project Plasticise (Contract No. 223524), ![]() (Dr Rossiter), and The Wellcome Trust (Mr Robin Borchert, Dr Nick Ward).
(Dr Rossiter), and The Wellcome Trust (Mr Robin Borchert, Dr Nick Ward).