
Abstract
Background
Dual-task capacity, which might be impaired poststroke, is needed for daily functions. Therefore, dual-task capacity should be assessed during rehabilitation. The Dual Overload Interference Test (DO-IT) is a new upper extremity (UE) protocol for assessment, combining The Box and Block Test with the Counting Backwards Test.
Objectives
To validate DO-IT by comparing between (1) young and older healthy, (2) stroke and healthy participants. Additionally, to correlate DO-IT with (3) walking-cognitive dual-task assessment (healthy), and (4) standardized cognitive and EF assessments (stroke).
Methods
A cross-sectional study included younger and older community-dwelling healthy individuals (N = 32), and younger and older individuals with stroke (N = 83). DO-IT was administered to all participants. The #blocks transferred (motor) and #correct numbers counted (cognitive) were recorded for single and dual conditions. The walking-cognitive dual-task test was administered to the healthy participants. Motor and cognitive costs were calculated as the difference between single and dual tasks. The Montreal Cognitive Assessment test (MoCA) and the Color Trail Test (CTT) assessed cognition post stroke.
Results
Older healthy adults had significantly lower dual-task motor capacity compared to younger adults (median [interquartile range] blocks: older 26 [21-38], younger 46 [38-52], P < .01). Participants with stroke showed higher motor costs than healthy participants. Dual-task costs correlated between DO-IT to walking-cognitive (motor; r = .37-.41, cognitive; r = .41-.47, P < .05). DO-IT motor cost negatively correlated with MoCA (r = −.27, P < .05), and DO-IT motor performance correlated with MoCA/CTT-A\B (r = .29-.60, P < .05).
Conclusions
UE-Cognitive dual-task capacity is affected post-stroke. DO-IT shows potential for use in stroke rehabilitation and its validity should be further researched.
Introduction
Executive function (EF) deficits, common post-stroke, negatively impact independence in daily living. EFs are higher cognitive abilities involving working memory, cognitive flexibility, and dual-task capacity. 1 EF deficits, reported in 43% to 75% of individuals post-stroke 2 have consistently found to predict negative functional outcomes. 3 EFs are essential for performing complex daily tasks such as cooking or trip planning. 4 Therefore, it is important to assess EF post-stroke to accurately plan a therapeutic intervention.
EF are assessed using different tools to obtain different types of information. Pen and paper neuropsychological assessments 5 assess specific EF components, but transfer to real life performance is limited. 6 Performance-based assessments, where participants are requested to perform tasks, such as cooking, 7 evaluate the impact of EF on daily functioning and can provide information regarding EF deficits. These tasks involve hand functions (mixing/pouring) and cognitive tasks (such as recipe following, planning, organization, and safety and judgment), 8 however, hand function is not assessed. To understand how the cognitive load impacts hand function, clinicians should use an upper extremity (UE)-cognitive dual-task assessment.
Dual-task includes performing two tasks simultaneously, 1 usually a motor and a cognitive task: each task has a different purpose and can be performed and measured separately. 9 Executing the dual-task adds cognitive load, causes motor-cognitive interference,9,10 and leads to reduced performance in either the motor or cognitive-task (or both tasks) 11 due to the “cost” of simultaneously execution. Dual-task capacity can be quantified by the performance during the dual-task condition (termed “dual-task performance”) or by calculating the change between single- and dual-task performance (termed motor/cognitive cost). 12
UE-cognitive dual-task assessments have been used mainly with older adults and individuals with different neurological conditions12 -14 to assess mild cognitive impairments and EFs. The studies that did include individuals with stroke15 -19 still don’t allow for a clear understanding of dual-task capacity post stroke due to the following reasons. The motor tasks used to assess dual-task capacity are not suitable for individuals with stroke with significant motor impairments because they entail small pieces (such as the Purdue Pegboard Test 20 ) or require in-hand manipulation (such as the Functional Dexterity Test 21 ). Therefore, motor tasks used with individuals post stroke are not functional and entail proximal arm movements 19 using kinematic measures. 22 In addition, there is no gold standard for assessing UE dual-task capacity and different research groups23,24 have used different combinations of motor and cognitive tasks. 12 Some of the motor-tasks that have been used as single tasks already require cognitive abilities, 12 such as copying shapes 25 or tapping in a sequence. 26 Lastly, dual-task capacity has mainly been researched in laboratories, 14 or by utilizing technologies,19,27 that do not exist in most clinical settings. In order to clearly demonstrate that EFs are required for performing complex everyday tasks, it is also important to assess associations between assessments of UE-cognitive dual-task and assessments of EFs. A systematic review conducted recently by our group demonstrated these challenges in the assessment of dual-task capacity. 12 This helped us identify the need for a practical and affordable UE-cognitive dual-task assessment, specifically for individuals with stroke.
We therefore developed the Dual Overload Interference Test, or for short: DO-IT. The DO-IT protocol includes the Box and Block Test (BTT) 28 in conjunction with Backward Counting by Threes Test 29 (a very commonly used cognitive-task). The BBT is a relatively simple motor-task, that does not impose a high cognitive load, making it suitable as a single motor task for individuals with stroke. Despite this fact, BBT does not closely resemble real-life daily tasks, which limits its ecological validity.
This study aims to utilize the DO-IT to assess dual-task capacity involving the UE post stroke. Specifically, we aimed to validate DO-IT by comparing between (1) young and older healthy participants, and (2) stroke and healthy participants. Additionally, we aimed to correlate DO-IT with (3) walking-cognitive dual-task assessment in healthy participants, (4) and standardized cognitive and EF assessments in the stroke group. These aims support the recommendations of a recent Think Tank meeting of the International Stroke Recovery and Rehabilitation Alliance (May 2024), which stated that “cognitive-motor interactions are infrequently studied but that they deserve attention”. If the validity of DO-IT is supported in this study, DO-IT can be used in rehabilitation as tool for assessing EF post stroke.
Methods
A cross-sectional study was conducted.
The study was approved by the University ethics committee (healthy) and the Hospital’s Helsinki committees.
Population
We recruited younger (20-54 years old) and older (55-90 years old) participants. All participants provided written informed consent before participating in the study.
Community-dwelling healthy individuals were recruited from the community (via What’s App groups) and snowball sampling. Participants with right-hand dominance (verified 30 ), who reported being overall healthy with full hand function, were included.
Individuals with stroke, were recruited from an in-patient subacute and an out-patient rehabilitation setting. Inclusion criteria: sustained a stroke (confirmed by computed tomography [CT]/magnetic resonance imaging [MRI]), can understand simple instructions, were independent in basic activities of daily living and had full hand function before the stroke (self-report), without other neurological or psychiatric conditions.
Tools
Assessment of Dual-Task Capacity
DO-IT utilizes the BBT 28 as a single motor-task and Counting Backwards in Threes Test (CBT) 29 as a single cognitive-task. These tests were administered separately (termed: single motor and single-cognitive) and then simultaneously (termed: dual-task motor and dual-task cognitive), each lasting 1-minute for each hand. Participants were instructed to perform the motor task as quickly as possible and were informed that both, the motor and cognitive tasks, were equally important. To eliminate any potential learning effect, half of the healthy participants started with the right UE and half started with the left UE for the single and dual-tasks, but participants with stroke always started with their less-affected UE.
Scoring DO-IT: Motor performance—the number of blocks transferred and cognitive performance—the number of correct numbers counted for both single and dual conditions. In addition, the motor and cognitive dual-task costs (termed DO-IT motor cost and DO-IT cognitive cost, respectively) were calculated as the difference between the single and dual motor/cognitive-task for each hand. We calculated dual-task costs,10,12 using the following commonly used equation (although other calculations are available). 12 (single task − dual task)/single task) × 100 = motor/cognitive cost. Henceforth, the term dual task capacity using DO-IT refers to performance and costs.
The BBT 28 measures gross manual dexterity. Participants are asked to transfer as many blocks as possible, 1 block at a time from 1 side of a wooden box to the other side, within 1 minute. The score for each hand is the number of blocks transferred within 1-minute. The test has high test–retest reliability and high Inter-rater reliability (r = 0.91). 28 This test has been widely used to monitor UE progress post-stroke. 31
The CBT 29 assesses working memory needed for transient holding and processing of new and existing information. Participants are requested to count backwards by threes starting from a 3-digit number. The number of correct answers in 1 minute is recorded. This test is widely used in dual-task paradigm testing.32,33 CBT was administered 4 times for stroke participants or 5 times for healthy participants, including during the walking-cognitive dual-task assessment. Participants were asked to count backwards starting from the following 3-digit numbers (399, 398, 397, 396, and 395).
Walking-cognitive dual-task assessment: 34 Participants were asked to walk indoors at a comfortable speed for 1-minute and the number of meters was recorded (walking single motor). The track was 10 m long and participants walked back and forth until the time was up. Then participants were asked to walk for 1-minute while performing the CBT. Dual-task performance (number of meters walked [walking dual-task motor] and number of correct answers [walking dual-task cognitive]) was recorded. The motor and cognitive dual-task costs (termed walking-motor cost and walking-cognitive cost, respectively) were calculated using the equation above. This assessment was administered only to healthy participants due to the fact that some participants were in the early stages post-stroke and were not able to ambulate.
Cognitive Assessments
In addition to the Counting Backwards by Three test 29 (which assesses working memory), as part of DO-IT, the following commonly-used assessments were used. The MoCA to measure general cognition including EFs and the Color Trails Test (CTT) to assess a specific component of EFs; cognitive flexibility, which includes normative data adjusted for education and age.
Montreal Cognitive Assessment (MoCA) 35 is a screening test to detect mild cognitive impairment including EFs. The MoCA assesses 8 cognitive domains: attention and concentration, EFs, memory, language, visuo-constructional skills, conceptual thinking, calculations, and orientation. Score ranges from 0 to 30 points; a score of 26 and above is considered normal cognition. 35 MoCA had sensitivity of 83% to 94% and specificity of 46% to 59% to detect mild cognitive impairment. 36
CTT 37 is a brief paper and pencil assessment to assess EF, specifically attention, speed processing and cognitive flexibility. Participants are instructed to draw a line in the correct order between colored numbers scattered on a page (1, 2, 3, and 4; part A) and alternating between numbers in pink and yellow circles (1—yellow, 2—pink, 3—yellow, 4—pink, etc.; Part B). Completion time for each part is recorded and compared to normative data using T-scores; higher scores indicate better EFs.
Demographic information (age, sex, and education) was collected from all participants, as well as stroke information (date, side, MRI/CT findings, and lesion location). The Functional Independence Measure score, 38 to assess independence in basic activities of daily living and the Fugl-Meyer Motor Assessment (FMA) 39 to assess UE-motor impairment (administered max 1-week apart from data collected), were extracted from the medical file for individuals with stroke.
Procedure
Assessments were administered by trained occupational therapists in a quiet room. The assessments were performed in the following order for both groups: MoCA, CTT, and the DO-IT (single tasks first) and walking-cognitive dual-task assessment (healthy).
Data Analysis
Data were input and analyzed using IBM Statistical Package for Social Sciences Statistics (Version 27). The continuous variables were not normally distributed, so descriptive statistics were presented as median and interquartile range (IQR), and non-parametric statistics were used. Descriptive statistics described the sample and study variables. Chi-square test was used to assess differences in sex between groups. Mann–Whitney U tests were used to compare between the following groups: (1) young and older healthy participants, and (2) healthy and stroke groups. To understand the magnitude of the between-group differences, we calculated, Cohen’s r effect size based on the calculation of the formula z/√n, where z was retrieved from the Mann–Whitney output and n is the sample size. The effect size values were considered weak (0.01-0.06), moderate (0.06-0.14), and large (≥ 0.14). 40 Spearman’s rank correlation coefficient was used to assess the correlations between dual-task capacity as assessed by the DO-IT and walking-cognitive dual-task (for healthy participants) as well as between DO-IT to the cognitive assessments (stroke participants). For the stroke group, in order to eliminate the effect of the motor impairments of the affected UE and to include all participants, only data of the less-affected UE was used for the correlations. In addition, correlations were assessed between time since stroke and dominance of the affected UE to dual-task capacity using DO-IT. As this is an exploratory study, using DO-IT for the first time, the sample size was not calculated. The findings of this study can inform future studies and sample size can be calculated. The level of significance was set at 0.05.
Results
Healthy Participants
Thirty-two healthy right-handed participants: 16 young adults (22-54 years old), and 16 older adults (56-87 years old) without differences in years of education between subgroups (see Table 1). The cognitive assessments demonstrated overall better cognitive abilities of the younger adults compared to older adults, with the MoCA showing a statistically significant difference) (χ2 = −2.08, P > .05). The median (IQR) MoCA score for the young group was 29.0 (28-30), compared with the older group (27.0 [26-28]). The other cognitive assessments did not reach statistical significance.
Characteristics and Dual-task Capacity Assessed by DO-IT of All Healthy and Stroke Participants.

Abbreviations: FIM, Functional Independence Measure; MoCA, Montreal Cognitive Assessment; CTT (part A+B), Color Trails Test-(T)-t-scores; CBT, Counting Backward Test; Single-motor, Box and Block Test; DO-IT, Dual-task motor and cognitive, Box and Block Test (UE) or walking (Cognitive-Walking Dual-task) in conjunction with the CBT; Cohen’s r effect size values were considered weak (0.01-0.06), moderate (0.06-0.14), and large (≥ 0.14); Mann–Whitney U test was used to compare between groups; P < .05, P < .001.
For the healthy group; differences and the effect size between young versus older subgroups are presented.
The single-motor task using both hands, was not significantly different between age groups but the DO-IT dual-task motor capacity of the young group was significantly better (with large effect size values) than the older group. The DO-IT dual-task cognitive capacity (left and right) of the older group was not significantly different than the younger group but effect size values were large (Cohen’s r < .16). Possibly, larger subgroups would show statistically significant differences. The characteristics, single tasks and dual-task capacity of all the healthy participants and the age subgroups are presented in Table 1.
In addition, the walking-cognitive dual-task capacity was significantly different between age groups with large effect size values. The walking single and walking-motor dual-task performance of the young was significantly better than the older healthy group (χ2 = −3.02-3.93, P < .001). No significant differences were found for the walking dual-task cognitive performance and the walking-motor and cognitive costs.
Stroke Group
Eighty-three individuals with stroke (45.7% women) aged 22 to 87 years old, were included with dominance affected hand in 51.8% of participants. Participants with stroke were 10-143 days post-stroke onset; 16% of them sat in a wheelchair, 52% had a right-sided stroke, and 81% had an ischemic stroke (see Table 2). Participants exhibited a range of cognitive abilities, from mild cognitive deficits to intact cognition, but none of the participants had a significant cognitive decline.
Demographic and Clinical Data of the Participants With Stroke Compared to the Healthy Participants Within the Young and Older Groups.

Abbreviations: MoCA, Montreal Cognitive Assessment; CTT (part A+B), Color Trails Test-(T)-t-scores; FIM, Functional Independence Measure.
Cohen’s r effect size values were considered weak (0.01-0.06), moderate (0.06-0.14), and large (≥ 0.14); Mann–Whitney U test was used to compare between groups; P < .05, P < .001.
All 83 participants completed the dual-task assessment with their less-affected hand (ipsilateral to the brain lesion), and 74 participants (89%) also completed DO-IT with their affected UE (contralateral to the brain lesion). These participants had higher UE-motor ability of their affected UE (FMA scores ranged from 27-66 points, median [IQR] 57.0, 51-63) compared with participants who could not perform the DO-IT (FMA scores ranged from 1-21 points, median [IQR] 5.5 [2-18] out of a maximum score of 66 points). Dual-task capacity as assessed by DO-IT was not correlated to time since stroke onset (P > .05) or to dominance of the affected UE (P > .05).
Comparing Cognitive Abilities and DO-IT Dual-Task Capacity Between Healthy and Stroke Groups
Significant differences with medium-large effect size values (Cohen’s r = .06-.14) were found for MoCA between stroke and healthy participants. The median (IQR) MoCA score of the young healthy group was 29.0 (28-30) versus 25.0 (23-27) of young stroke group (z = −4.36, P < .001), and 27.0 (26-28) of the older healthy group versus 23.0 (19-25) for the older stroke group (z = -4.68, P < .001).
Significant differences in dual-task capacity, as assessed by DO-IT, were found between stroke and healthy groups across young and older groups, with medium-to-large effect size values (Cohen’s r = .06-.14). Among younger participants, the healthy group performed significantly better than the stroke group across all parameters, except for the DO-IT cognitive cost of the right and left hands versus the affected and less-affected hands in the stroke group (see Table 2). For the older participants, the healthy group demonstrated significantly better dual-task performance compared to the stroke group, but the DO-IT motor and cognitive costs of both hands, which were very low or negative for all groups, showed no significant differences (see Table 3 and Figure 1).
Dual Task Capacity Assessed by DO-IT Of Participants With Stroke Compared to Healthy Participants Within the Young and the Older Groups.

Abbreviations: CBT, counting backward test; Single motor, Box and Block Test; Dual-task motor and cognitive, Box and Block Test in conjunction with the CBT.
Cohen’s r effect size values were considered weak (0.01-0.06), moderate (0.06-0.14), and large (≥ 0.14); Mann–Whitney U tests were used to compare between groups.
P < .05. P < .001.
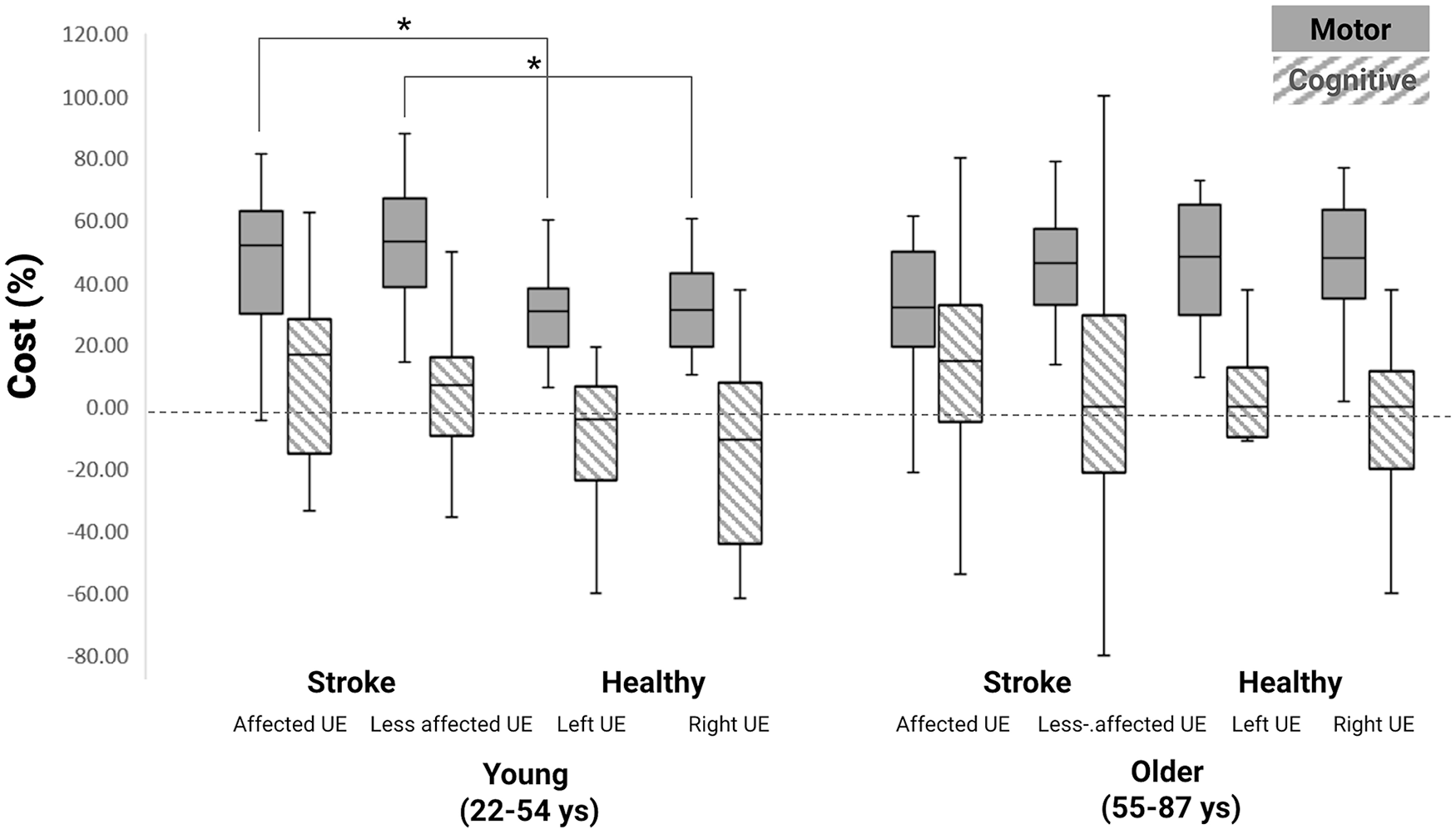
Comparing DO-IT motor and cognitive costs (%) of both hands as assessed by DO-IT between healthy (n = 32) and stroke participants (n = 83) according to age groups.
Correlations Between DO-IT and the Walking-Cognitive Dual-Task Assessment
Among all healthy participants, moderate significant correlations were found between DO-IT motor costs and the walking-cognitive dual-task assessment motor cost for left (r = .37, P < .05) and the right UE (r = .41, P < .05). Similarly, moderate significant correlations were found between DO-IT cognitive costs and the walking-cognitive dual-task assessment cognitive cost for left (r = .47, P > .001) and the right UE (r = .41, P > .001). In addition, moderate to strong significant correlations were found for dual-task motor performance between the 2 assessments (left r = .62, P < .001 and the right UE—r = .59, P < .001). Strong significant correlations were also found for dual-task cognitive performance for left (r = .82, P < .001) and right UE (r = .81, P < .001).
Correlations Between DO-IT and the Cognitive Assessments for the Stroke Group
For the less-affected UE of all the stroke participants (n = 83), weak to moderate significant correlations were found between dual-task capacity and the cognitive assessments (see Table 4). Specifically, MoCA was correlated to dual-task cognitive performance (r = .61, P < .001), dual-task motor performance (r = .52, P < .001), motor cost (r = −.32, P < .001), and cognitive cost (r = −.23, P < .05). The CTT (A + B) was correlated with dual-task cognitive performance (A: r = .45, B: 0.50, P < .001) and dual-task motor performance (A: r = .31, B: 0.43, P < .001). These correlations indicate that lower dual-task motor and cognitive performance and higher motor and cognitive costs were correlated with more cognitive deficits.
Correlations Between DO-IT (Parameters of the Less-affected UE) to Cognitive Assessments
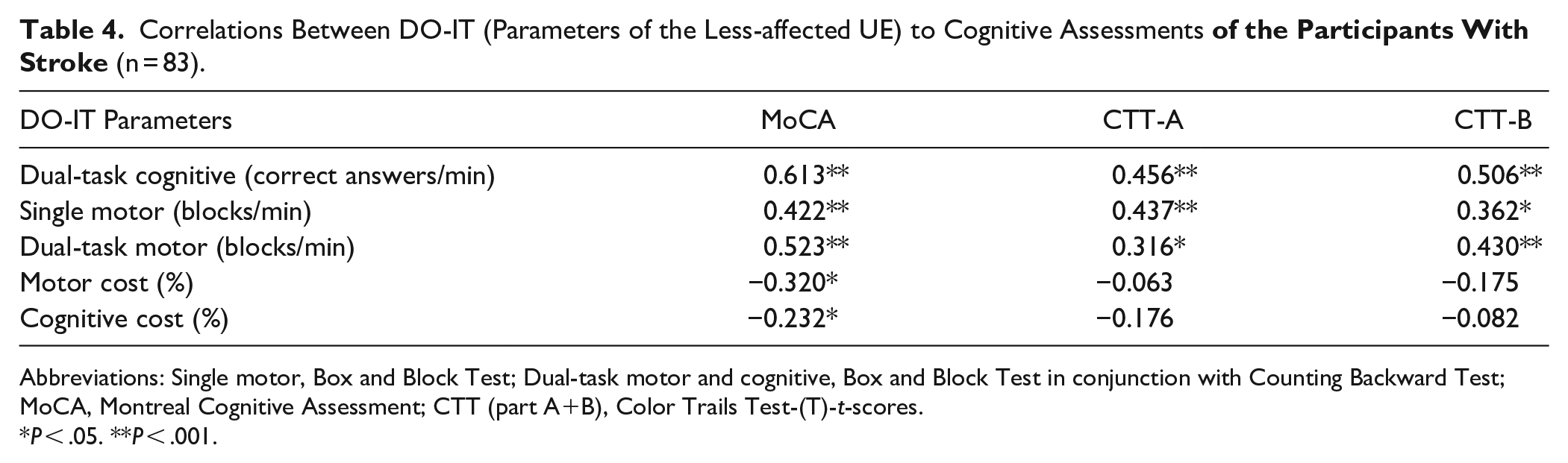
Abbreviations: Single motor, Box and Block Test; Dual-task motor and cognitive, Box and Block Test in conjunction with Counting Backward Test; MoCA, Montreal Cognitive Assessment; CTT (part A+B), Color Trails Test-(T)-t-scores.
P < .05. **P < .001.
Discussion
Many of our daily functions include performing cognitive tasks while simultaneously using our hands. The capacity to perform dual-task requires EF, which might be impaired in older adults and individuals with stroke. Our study aimed to provide initial validity of DO-IT, an UE-cognitive dual-task assessment to assess EF. By using a practical UE-cognitive dual-task assessment in rehabilitation, clinicians can assess EF and the impact of these deficits on hand function post-stroke in order to plan an effective therapeutic intervention. Our study included older and younger healthy adults as well as individuals with stroke. We will first discuss the age-related differences within the healthy group and then compare between groups (while controlling for age).
Healthy older participants exhibited lower dual-task motor performance (UE- and walking single motor tasks) and lower cognitive abilities (assessed by MoCA) compared to the younger the group.41,42 These between age-group differences were also found for dual-task capacity as assessed by DO-IT, as well as for the dual walking-cognitive assessment. These findings, which are supported by other studies,19,43,44 could be attributed to age-related brain changes, that lead to deficits in EF in general and specifically in working memory, cognitive flexibility and dual-task capacity in older adults. 41 In addition, when walking, older adults tend to focus on their safety, therefore to prioritize their motor function over cognitive tasks, especially in threatening situations of compromised balance (to prevent falls). 34 While safety primarily applies to walking, it is not yet understood if it might be relevant to UE tasks, particularly those requiring precision, where older adults may prioritize motor control to avoid errors. Therefore, these differences between age groups support the construct validity of DO-IT, which demonstrated differences between age-groups expected to differ in terms of EFs.
Dual-task capacity of the healthy participants, as assessed using their UE (DO-IT), showed moderate to strong significant correlations to dual-task capacity assessed by walking-cognitive dual-task assessment. This further supports the criterion validity of DO-IT. These findings indicate that working memory and divided attention are required for both assessments while prioritizing the motor and cognitive-tasks in real time. Correlations are possibly only moderate because hand function and walking have different demands; walking is a rhythmic, continuous ability, which is more automatic, while transferring blocks is discrete and involves eye–hand coordination. Not many studies have assessed correlations between UE- and walking-cognitive dual-task assessments. Moderate correlations between dual-task capacity between UE (elbow range of motion repetitions and other associated parameters) and walking-cognitive dual-task assessment were reported only by 1 research group22,24,33 and our study extends these correlations to UE functional activity.
When comparing the CTT and MoCA scores between groups, the participants with stroke demonstrated deficits in EF compared to the healthy participants. This was evident in both the younger groups (MoCA and CTT-A scores) and the older groups (MoCA and CTT-A+B scores).The presence of EF deficits post-stroke has been studied extensively2,45,46; researchers have compared individuals with stroke to healthy controls utilizing neuropsychological assessments47,48 as well as performance-based assessments.49,50 Our study extends these findings to dual-task capacity utilizing DO-IT. Future studies should correlate DO-IT to performance-based assessments to further validate DO-IT as an ecological measure to assess EF.
DO-IT demonstrated differences between the stroke and healthy groups. Although motor performance of the (young and older) healthy groups were significantly better than the stroke groups, motor cost was significantly different only for young participants (stroke vs healthy). These findings support a recent systematic review, which showed that stroke patients exhibited on average a 19% increase in dual-task capacity compared to age-matched healthy controls. 19 Whereas previous research post stroke assessed dual-task capacity as a whole while using proximal motor tasks, 19 in this study we differentiated between dual-task performance and dual-task cost and used a test of manual dexterity. Our DO-IT also assessed dual-task capacity while testing both hands, which addresses a significant gap in the literature. Previous studies mainly focused on testing dual-task capacity only of the affected hand,15,18 which limits the generalization to individuals with significant motor impairments. Studies that did examine both hands lacked the use of functional tools for assessing the motor task.16,18 Testing both hands also helps to distinguish between the motor impairment (apparent mainly on the affected side) and the impairments in EFs (apparent on both sides).
High motor costs with low or negative cognitive costs, indicating a clear preference for the cognitive-task, were found for both age-groups within the healthy group and for the stroke group. In other words, overcompensation when performing the cognitive-task on account of the motor-task was observed. Furthermore, DO-IT cognitive cost was not significantly different between stroke and healthy (for both hands). This cognitive prioritization might be related to the easy motor-task used in this study. 51 Similar findings 52 have been reported regarding walking-cognitive dual-task capacity; poorer walking performance, such as slower gait speed, reduced stride length, and balance impairments occurred when healthy older adults 53 and individuals with stroke54,55 prioritized the cognitive-task over the motor-task. Therefore, it can be assumed that the cognitive prioritization does not stem from motor difficulties but rather has a cognitive basis. The impact of the interference of DO-IT’s cognitive-task should be further investigated.
In individuals with stroke, dual-task capacity as assessed by DO-IT was significantly correlated with EF and cognitive assessments, which further confirms that DO-IT assesses EF, thereby establishing convergent construct validity. Although similar correlations have been previously shown in patients with neurological populations,32,33 including stroke,15 -18 the motor-tasks that were used required cognitive abilities 12 (such as copying a shape and memorizing finger sequences). Therefore, DO-IT has an advantage because the BBT is simple motor task and is relatively easy for individuals with stroke to perform, even when using their affected UE. Only 7 participants with stroke were unable to perform DO-IT using their affected UE, but it was still possible to assess UE-cognitive dual-task capacity through the use of their less-affected UE. Another advantage of DO-IT is that it can be administered to participants with stroke who cannot ambulate. In our study, some of the stroke participants sat in a wheelchair (16%); therefore, the walking-cognitive dual-task assessment could not be used.
Dual-task capacity using a walking-cognitive dual-task paradigm has been found to be correlated with cognitive assessments in neurological populations56,57 as well as in individuals with stroke. 58 Individuals with neurological conditions may be particularly susceptible to dual-task interference because of the relative increase in attentional demands required to control motor performance; therefore, there are fewer attentional resources available for the simultaneous performance of secondary tasks. 11
Our study has several limitations. Our sample of healthy participants was not very large, they were predominantly female (71.3%) and the age groups were relatively small (resulting in lack of statistical significance with a large effect size). Most participants with stroke did not have a moderate/severe motor impairment of their affected UE; therefore, the findings cannot be generalized to these individuals. In addition, individuals varied considerably in terms of time post stroke. While this might be a limitation, it also offers an opportunity to demonstrate dual-task capacity across different recovery stages. Whereas, only right-handed healthy participants were included, this was not the case for the participants with stroke. Although correlations were not found between DO-IT and dominance of the affected hand, it might be important to consider hand dominance of participants with stroke in future studies and to match hand dominance when comparing healthy to stroke participants. Also, in future research, DO-IT should be used with older healthy adults and individuals with stroke with varying cognitive abilities. The walking-cognitive dual-task assessment, which was not administered to the individuals with stroke, should be administered in the future to individuals with stroke who can ambulate. This will further support the criterion validity of DO-IT. In addition, years of education was significantly different between the stroke and healthy groups, which might explain potential differences in cognitive performance but the scoring of the MoCA and the CTT, takes this into account.
Conclusion
UE-Cognitive dual-task capacity is affected post-stroke. This exploratory study supports the validity of DO-IT for assessing EFs related to UE-cognitive dual-task capacity post-stroke. DO-IT, which is a new protocol for assessing dual-task capacity, shows potential for use in stroke rehabilitation, but further research is needed.
Footnotes
Authors’ Note
This study was presented at the 12th World Congress for Neurorehabilitation, Vienna, Austria, 2022 and at the 72th Conference of the Israeli Association of Ppothsical Medicine & Rehabilitation, Tel Aviv, 2022.
Author Contributions
YBK: Conceptualization; Data curation; Formal analysis; Investigation; Methodology; Writing—original draft; and Writing—review & editing. STL: Data curation; Investigation; and Writing—review & editing. TW: Data curation; Investigation; and Writing—review & editing. DD: Investigation; Project administration; and Writing—review & editing. MB: Investigation; Project administration; and Writing—review & editing. RC: Investigation; Project administration; and Writing—review & editing. DR: Conceptualization; Formal analysis; Investigation; Methodology; Supervision; and Writing—review & editing.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: The Rivka Nacht z"l Fund and the Lizzy and Arthur Levenstein Fund.