
Abstract
Background. Mirror visual feedback (MVF), a phenomenon where movement of one limb is perceived as movement of the other limb, has the capacity to alleviate phantom limb pain or promote motor recovery of the upper limbs after stroke. The tool has received great interest from health professionals; however, a clear understanding of the mechanisms underlying the neural recovery owing to MVF is lacking. Objective. We performed a systematic review to assess the effect of MVF on brain activation during a motor task. Methods. We searched PubMed, CINAHL, and EMBASE databases for neuroimaging studies investigating the effect of MVF on the brain. Key details for each study regarding participants, imaging methods, and results were extracted. Results. The database search yielded 347 article, of which we identified 33 suitable for inclusion. Compared with a control condition, MVF increases neural activity in areas involved with allocation of attention and cognitive control (dorsolateral prefrontal cortex, posterior cingulate cortex, S1 and S2, precuneus). Apart from activation in the superior temporal gyrus and premotor cortex, there is little evidence that MVF activates the mirror neuron system. MVF increases the excitability of the ipsilateral primary motor cortex (M1) that projects to the “untrained” hand/arm. There is also evidence for ipsilateral projections from the contralateral M1 to the untrained/affected hand as a consequence of training with MVF. Conclusion. MVF can exert a strong influence on the motor network, mainly through increased cognitive penetration in action control, though the variance in methodology and the lack of studies that shed light on the functional connectivity between areas still limit insight into the actual underlying mechanisms.
Introduction
Often a source of fascination, or perhaps frustration, optical illusions have captivated people since ancient times. For instance, curved surfaces and the absence of right angles in archaic Greek temples suggest that its architects attempted to optically correct the illusion of slanted columns or curved tympanums; however, others believe these features may serve engineering purposes or reflect aesthetic preference. 1 As much as they are a source of excitement, for neuroscientists optical illusions are considered a backdoor into people’s mind and provide an excellent way to study the neural mechanisms underlying perception and action. 2
Interestingly, although optical illusions are known to deceive the individual, the false reality may fool the brain, such that the outcome is beneficial. One such an illusion is the mirror illusion, which has been found to have therapeutic benefits over the past 2 decades. When a mirror is placed, along the midsagittal plane in between the 2 limbs, the reflection of the limb in front of the mirror is superimposed on the contralateral limb. Any motion of the limb in front of the mirror induces the illusion of 2 synchronously moving limbs. After Ramachandran and his colleagues found that this illusion could alleviate phantom pain in a proportion of the patients, 3 mirror visual feedback (MVF) was introduced as a neurorehabilitation tool to treat other unilateral pain disorders, such as complex regional pain syndrome (CRPS). In addition, the paradigm is now used to promote motor recovery (eg, in hemiparetic patients or after hand surgery).
Despite its widespread use in neurorehabilitation and the claims that MVF therapy would lead to neuroplastic changes, there is no consensus about the underlying mechanism and speculation often lacks the neuroscientific proof. The aim of this review is therefore to bring together current knowledge on the effect of MVF on the brain as has been described in neuroimaging studies, in order to explore potential processes underlying the beneficial clinical effects of MVF. To acquaint the reader with MVF and its current applications, we will first revisit Ramachandran’s rationale for MVF, followed by a narrative review of the clinical neurorehabilitation research that followed in his footsteps. At the end of this section, we introduce 3 hypotheses that have been proposed to explain the positive effects related to MVF. Part 2 provides a systematic review and discussion of studies that examined the effect of MVF on brain activation patterns using neuroimaging or electrophysiological techniques. Finally, in Part 3 we discuss the findings of the systematic review in relation to the hypotheses introduced in Part 1 and we identify where further research is required.
Part 1: Mirror Therapy—Background, Current Applications, and Potential Mechanisms
The idea of using MVF for the management of phantom limb pain was inspired by early findings on the integration of perception and action, in particular the principle of reafference.4,5 Reafference is afferent sensory information caused by a motor command (eg, signals from muscle spindles in M. biceps brachii when the arm is actively flexed), as opposed to exafferent information, which results from factors outside the individual (eg, signals from muscle spindles in M. biceps brachii when the arm is flexed passively). To distinguish between these 2 sensory stimuli, it is maintained that the generation of a motor command is accompanied by a parallel signal, termed efference copy, which contains the sensory feedback to be expected due to this command. Comparison of all afferent signals with the efference copy provides a way to separate signals that originate from bodily movements and those from outside the individual. As a consequence, motor commands that are not instantaneously followed by the expected reafferent feedback will be modified in an attempt to evoke the expected sensory afference. 5 It is this conflictive state that, according to some,6,7 may evolve into a form of “learned paralysis” accompanied by a feeling of painful spasms, * as experienced by a proportion of patients who have had an arm or leg amputated. The goal of MVF is to restore the efference–afference loop that has been interrupted. MVF of the intact limb deceives the individual and elicits the awareness that the amputated limb is still intact, not at least due to the dominance of the visual system over other modalities.8,9 Indeed, when the illusion was tested in arm amputees with complaints of “clenching spasms” and phantom limb pain, the spasms were eliminated and the pain was relieved immediately after exposure to MVF in a proportion of the sample. 3
The novelty and simplicity of the idea, in combination with the far-reaching potential of MVF, prompted clinicians and researchers to replicate the initial findings of Ramachandran and colleagues. Consistent with the earlier observations, follow-up studies have confirmed that MVF treatment has the capacity to reduce phantom limb pain intensity and duration.10,11 Moreover, the notion that many neurological disorders with unilateral pain and motor symptoms may be (partly) caused by maladaptive cortical reorganization involving a disruption of the efference–afference loop, led others to apply MVF to a wide range of conditions. Hemiparesis after stroke is perhaps the most striking example. In a proportion of the patients the paresis is thought to be a form of “learned paralysis” due to a nonpermanent blocking of corticofugal fibers by swelling after the trauma. 12 A recent Cochrane Review exploring the effectiveness of MVF therapy in patients after stroke (13 randomized controlled trials, 506 patients) concluded that mirror therapy indeed might be more effective in promoting motor function than a control intervention † when used as an adjunct to conventional therapy. 13 Furthermore, the meta-analysis indicated that the effects were retained, up to 6 months after the intervention, and that MVF therapy had a significantly greater effect than control interventions on activities of daily living and on pain, though the latter was found only in a subgroup with CRPS after stroke.
To date, MVF is administered to treat various unilateral pain and/or motor disorders, including CRPS,14-18 hemiparesis after stroke,19,20 reduced mobility after wrist fracture, 21 and spastic hemiparetic cerebral palsy (SHCP).22,‡ The findings of these studies tend to corroborate the initial work, that is, a reduction in pain and improvement in motor function. Still, it should be noted that publication bias toward a selection of positive results may be likely and additional placebo-controlled studies are needed for all conditions or symptoms. In this respect, it is worth mentioning that Brodie et al found that the attenuating effect of MVF on pain was not stronger than a control condition in lower limb amputees. 23
Despite the fact that there appear to be parallels in the pathophysiology of unilateral pain and motor disorders as described by Ramachandran and Altschuler, 12 the 2 phenomena should be considered separately, hence the focus of this review will be on the effects of MVF on sensorimotor control. To fully exploit the potential of MVF, a better insight into the processes that underlie the beneficial effects on motor function is required. Not only would this knowledge advance our theoretical understanding of the brain, it may also provide guidelines as to when MVF may be useful and how it should be applied.
When the individual is required to perform bilateral, symmetrical motor tasks, MVF therapy may be considered a special form of bilateral training, and hence exploit similar mechanisms (see Cauraugh and Summers for a review 24 ). However, in search of the added value of MVF researchers have invoked 3 (not mutually exclusive) hypotheses to account for the positive effects of MVF on motor recovery. A first hypothesis relates to the mirror neuron system.17,19,20 Mirror neurons fire both when an individual observes an action and when he/she performs a similar action. The network, including the premotor cortex, supplementary motor area, inferior frontal gyrus, and inferior parietal lobule of the brain, is thought to play an important role in action recognition and motor learning or rehabilitation. 25 An observation/execution matching mechanism, whereby action observation activates crucial parts of the motor system, is hypothesized to induce motor learning.25,26 It is known that action observation facilitates the corticospinal pathway and this paradigm is already used in neurorehabilitation as mental practice aimed at improving motor function. 27 According to this hypothesis, a “mirror box” is a means to facilitate action observation and therefore MVF is thought to activate the mirror neuron system in a similar way to action observation (Hypothesis 1). In line with this is the notion that MVF may elicit or enhance motor imagery, 28 that is, internal simulation of movement without overt action. Just like action observation motor imagery has been attributed therapeutic capacities because it activates neural circuits involved in motor control. 29
Second, MVF might promote recruitment of ipsilateral motor pathways. 30 These motor pathways, originating in the unaffected hemisphere and projecting ipsilaterally to the paretic body-side, have been attributed a nontrivial role in the restoration of motor function in hemiparesis.31-34 It is hypothesized that MVF might facilitate the unmasking of “dormant” ipsilateral projections, which are normally inhibited (Hypothesis 2).
Finally, MVF or the associated illusion is thought to increase an individual’s (spatial) attention toward the unseen (affected) limb. 35 It is known that hemiparetic patients may end up in a state of “learned nonuse,” by continuously avoiding the use of the paretic hand or by pathophysiological disruption of the efference–afference loop. 36 In keeping with the rationale for using constraint-induced movement therapy, 36 the increased attention toward the affected limb, mediated by the illusory image of a “healed” paretic limb, may activate motor networks (Hypothesis 3).
In sum, an increasing body of evidence underpins the potential of MVF to facilitate recovery of motor function. Still, the neural mechanism of MVF, whether the behavioral effect is accompanied by neuroplastic changes, and what this reorganization would involve is unclear. The hypotheses invoked to explain MVF effects are based on known concepts in neurorehabilitation, but they remain speculative. Recent experimental neuroimaging research has begun to reveal the extent of brain activation during movement with MVF, and its modulatory effects on brain processes compared with normal visual conditions. In the following part of this article, the findings of these studies will be systematically reviewed. This will serve as a validity test of the proposed hypotheses.
Part 2: The Neural Correlates of Mirror Visual Feedback
Purpose
The purpose of this systematic review was to identify the areas in the brain that are differentially affected or modulated by MVF compared with a condition with normal or without visual feedback.
Literature Search
A literature search using the electronic databases PubMed, CINAHL, and EMBASE (1972 to January 2014) was conducted. Search terms included “mirror therapy” or “mirror visual feedback” combined with “functional magnetic resonance imaging (fMRI),” “positron emission topography (PET),” “transcranial magnetic stimulation (TMS),” “magnetoencephalography (MEG),” “electroencephalography (EEG),” or “near infra-red spectrometry (NIRS).” In addition, we checked our personal database and the reference list of included articles. Our search was restricted to peer-reviewed full articles written in English.
Inclusion criteria were the following:
Experimental studies or clinical trials
Normal and/or motor-impaired human participants
Use of neuroimaging techniques (fMRI, PET, MEG, EEG, NIRS) or TMS to study the effect of MVF * on cortical activation (and related motor performance or perceptual measures)
Exclusion criterion was the following:
Studies that do not assess effect of MVF on sensorimotor control, but focus on pain and/or tactile perception.
The records identified by this search were screened independently by 2 authors of this systematic review (FD and AS) in 2 stages: a first stage screening of titles and abstracts and a second stage using the full text of the remaining article. The lists of eligible articles identified by the independent reviewers were compared, and any disagreements were resolved through discussion (and referral to the text of the articles in question).
Results
The electronic database search yielded 347 unique articles, of which 33 were deemed eligible for this systematic review (see Figure 1 for an overview of the selection process). Across the selected articles, the most commonly used scanning technique was fMRI (12 studies).37-47 MEG was the neuroimaging modality in 5 article,48-52 EEG in 4,53-56 PET in 2,57,58 and NIRS in 2.59,60 Nine studies investigated the effect of MVF on cortical activation with TMS47,61-68; 1 study used both TMS and fMRI. 47 In Tables 1 to 4, the included articles and their methodologies are listed according to modality. The majority of the studies (n = 27) examined immediate modulatory effects when exposed to MVF, of which 22 focused on healthy individuals and 5 on stroke patients (Tables 1-3). In 16 studies, MVF was provided in a bilateral fashion, that is, not obscuring the active hand. Six studies assessed neuroplastic changes in response to a bout of practice or an intervention in healthy individuals (n = 3) or stroke patients (n = 3). Here, bilateral MVF was used in all but one study (Table 4 and Supplementary Material). The variance in methodology and motor task, which may be unilateral or contralateral, complicates the overall interpretation of the observations. A factor that adds to this difficulty is the absence of a standard control condition. In some studies, MVF is contrasted with normal full vision of the 2 limbs, whereas in others visual feedback of the active or static limb only is used as a control. Furthermore, to isolate the effect of MVF on brain activation it is crucial to keep the movement (range, frequency, intensity) constant across MVF and control conditions, which a number of studies have failed to do or to control for (see Table 1-4 for details).
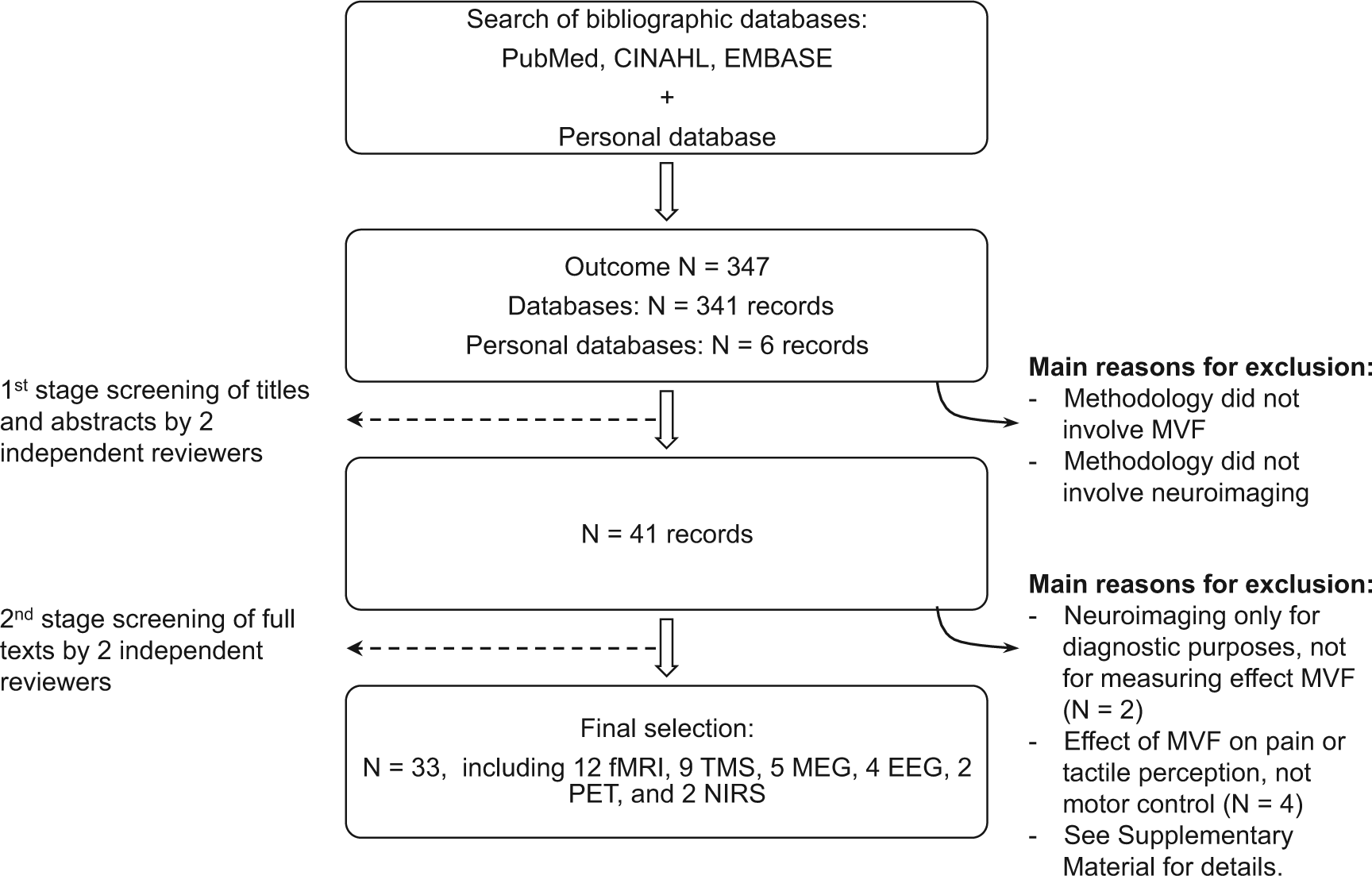
Flow diagram of the article selection process.
Outline of the Methodology, Type of MVF, Measures to Avoid Systematic Variation in Movement Across Conditions, and Known Potential Confounds in All Experimental Studies Using fMRI Included in the Systematic Review.
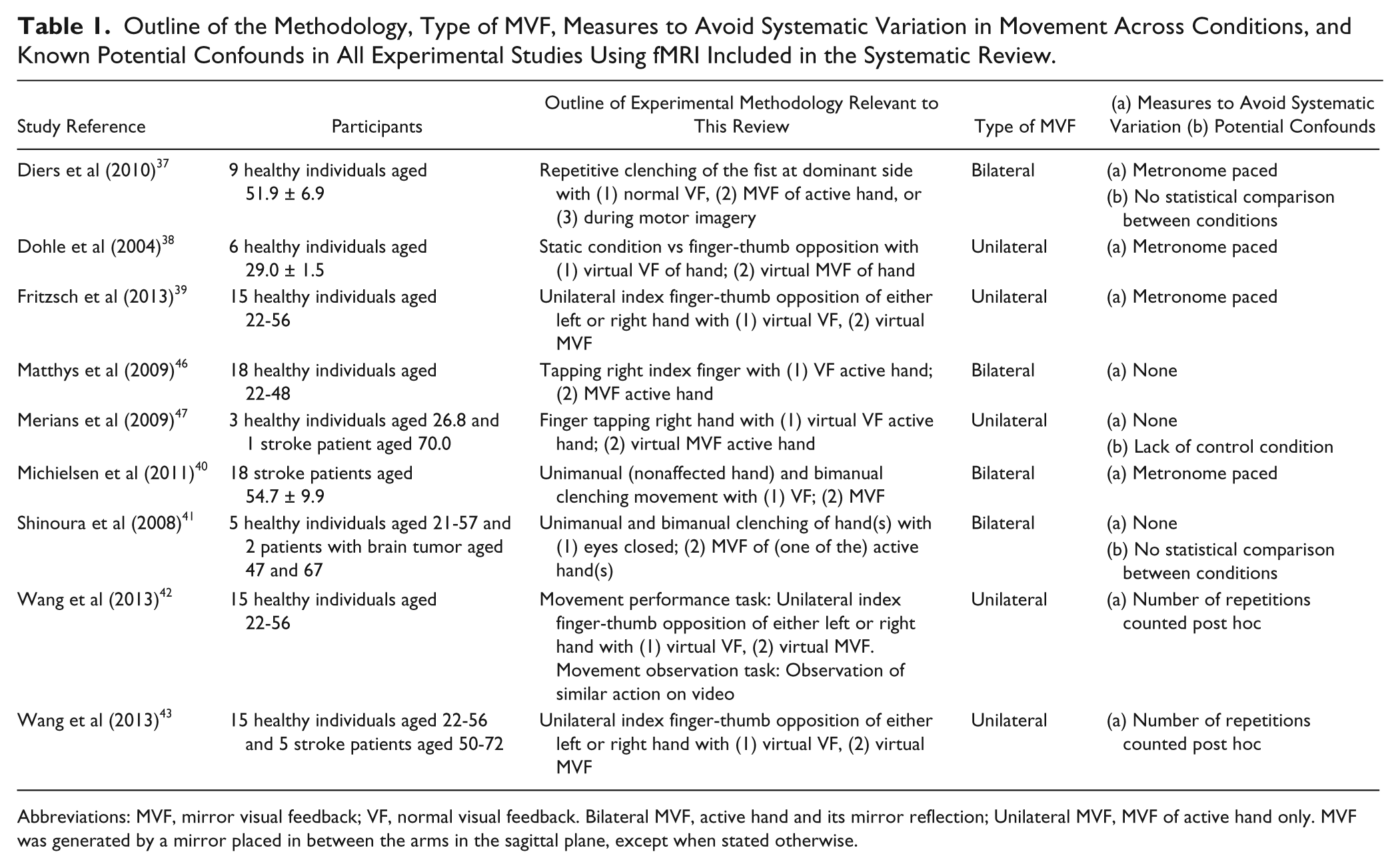
Abbreviations: MVF, mirror visual feedback; VF, normal visual feedback. Bilateral MVF, active hand and its mirror reflection; Unilateral MVF, MVF of active hand only. MVF was generated by a mirror placed in between the arms in the sagittal plane, except when stated otherwise.
Outline of the Methodology, Type of MVF, Measures to Avoid Systematic Variation in Movement Across Conditions, and Known Potential Confounds in All Experimental Studies Using TMS Included in the Systematic Review.
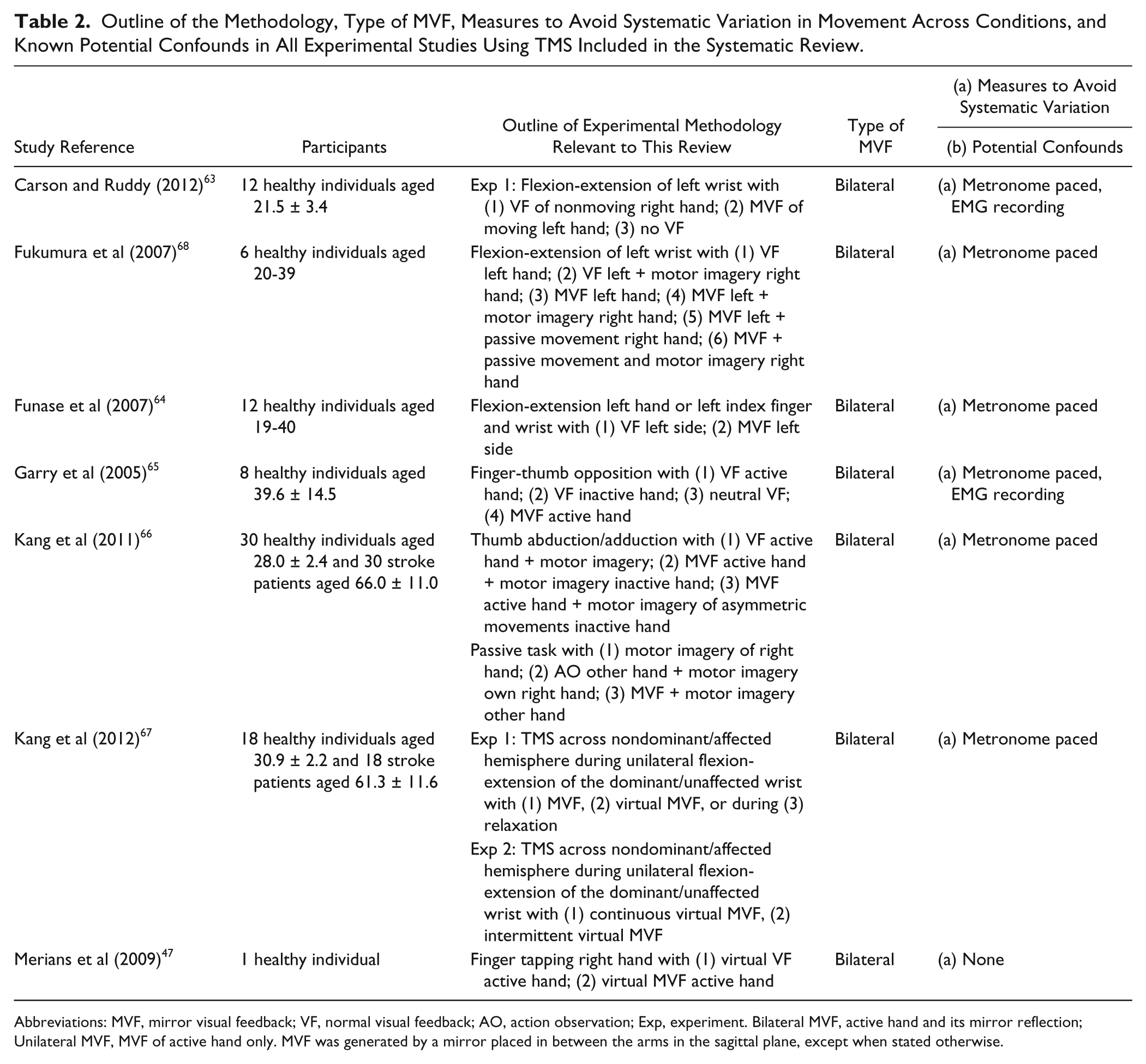
Abbreviations: MVF, mirror visual feedback; VF, normal visual feedback; AO, action observation; Exp, experiment. Bilateral MVF, active hand and its mirror reflection; Unilateral MVF, MVF of active hand only. MVF was generated by a mirror placed in between the arms in the sagittal plane, except when stated otherwise.
Outline of the Methodology, Type of MVF, Measures to Avoid Systematic Variation in Movement Across Conditions, and Known Potential Confounds in All Experimental Studies Using PET, MEG, EEG, and NIRS Included in the Systematic Review.
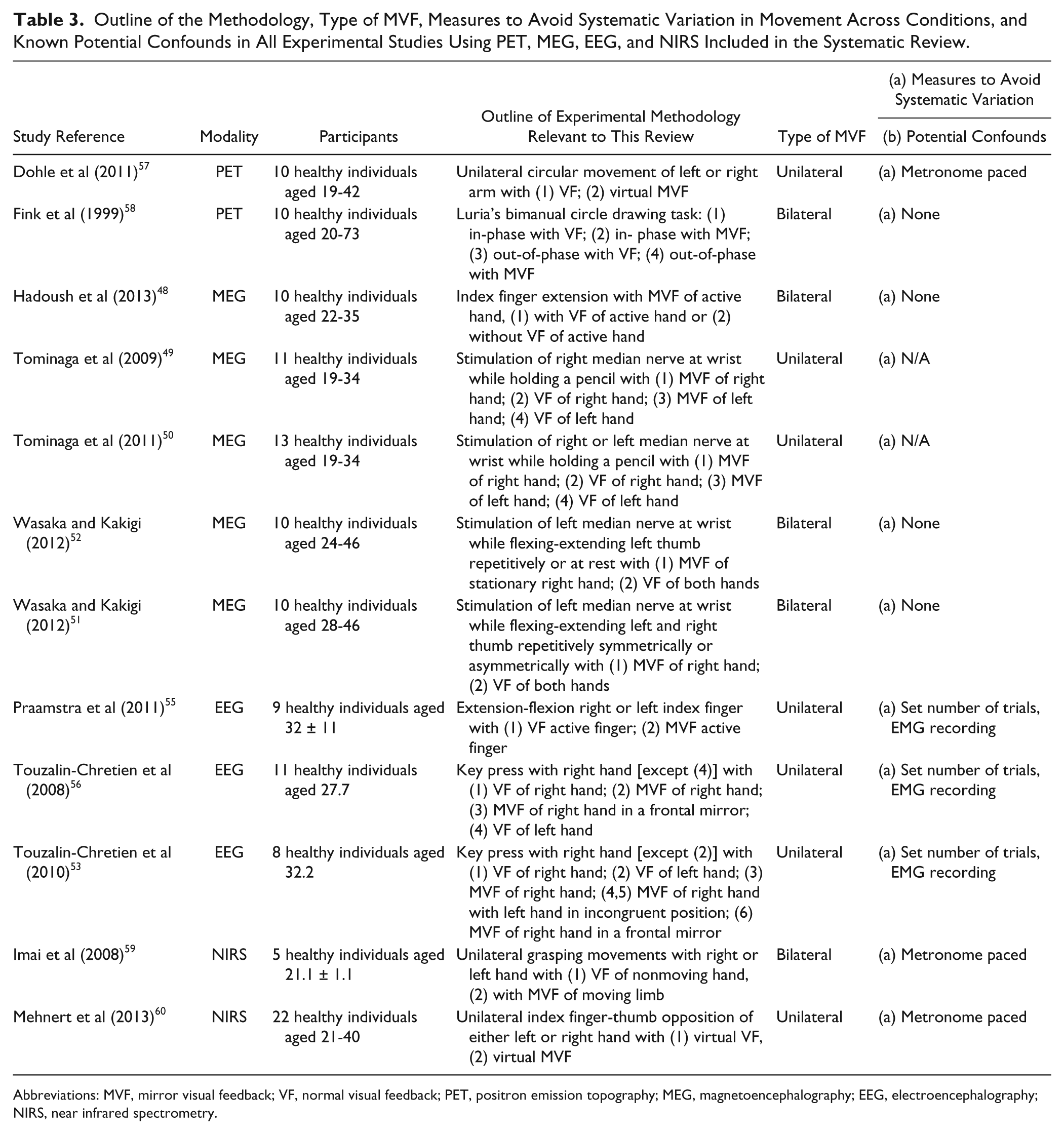
Abbreviations: MVF, mirror visual feedback; VF, normal visual feedback; PET, positron emission topography; MEG, magnetoencephalography; EEG, electroencephalography; NIRS, near infrared spectrometry.
Outline of the Methodology in All Clinical or Training Studies Included in the Systematic Review.
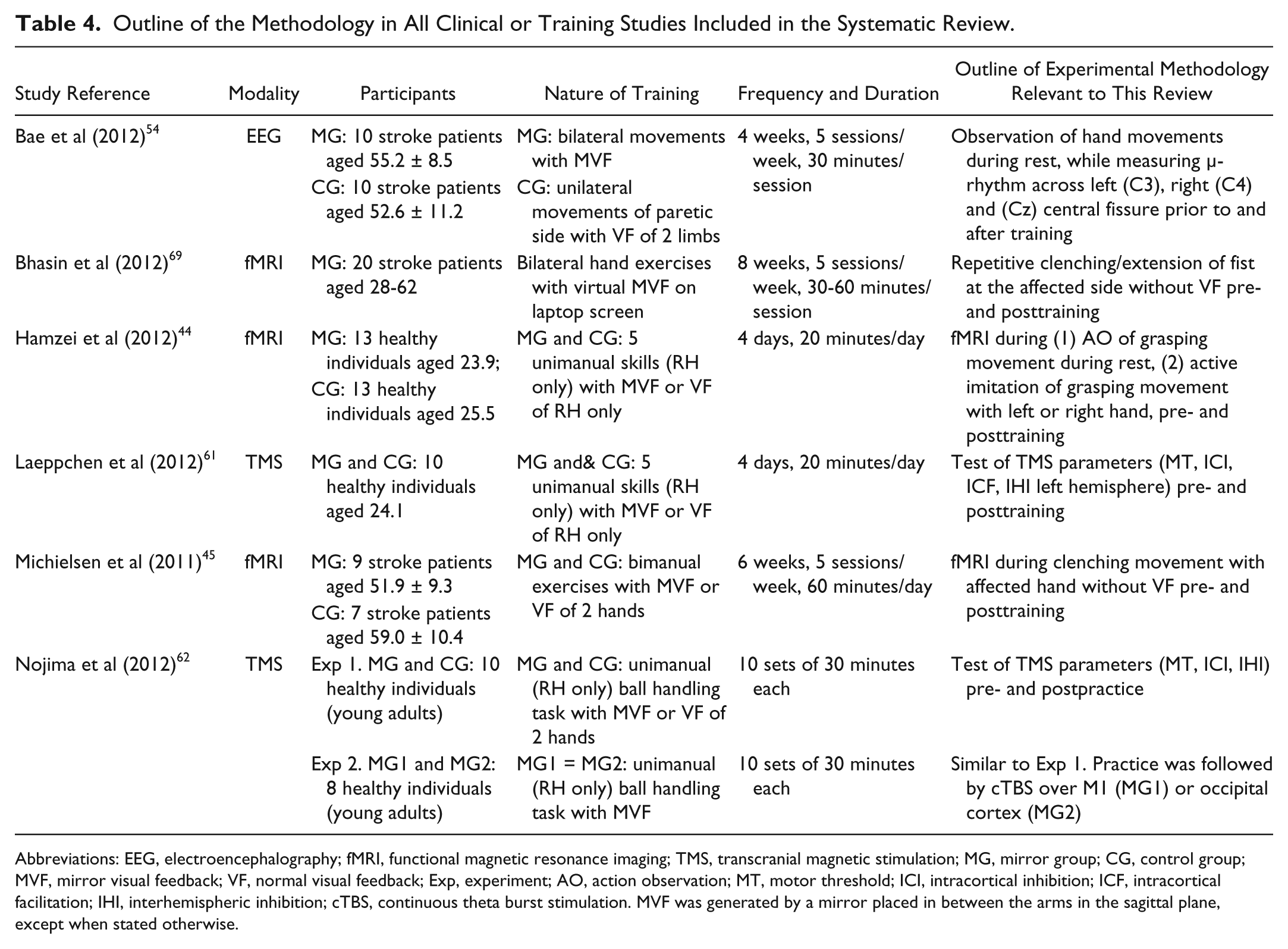
Abbreviations: EEG, electroencephalography; fMRI, functional magnetic resonance imaging; TMS, transcranial magnetic stimulation; MG, mirror group; CG, control group; MVF, mirror visual feedback; VF, normal visual feedback; Exp, experiment; AO, action observation; MT, motor threshold; ICI, intracortical inhibition; ICF, intracortical facilitation; IHI, interhemispheric inhibition; cTBS, continuous theta burst stimulation. MVF was generated by a mirror placed in between the arms in the sagittal plane, except when stated otherwise.
Instant Neuromodulatory Effects of MVF
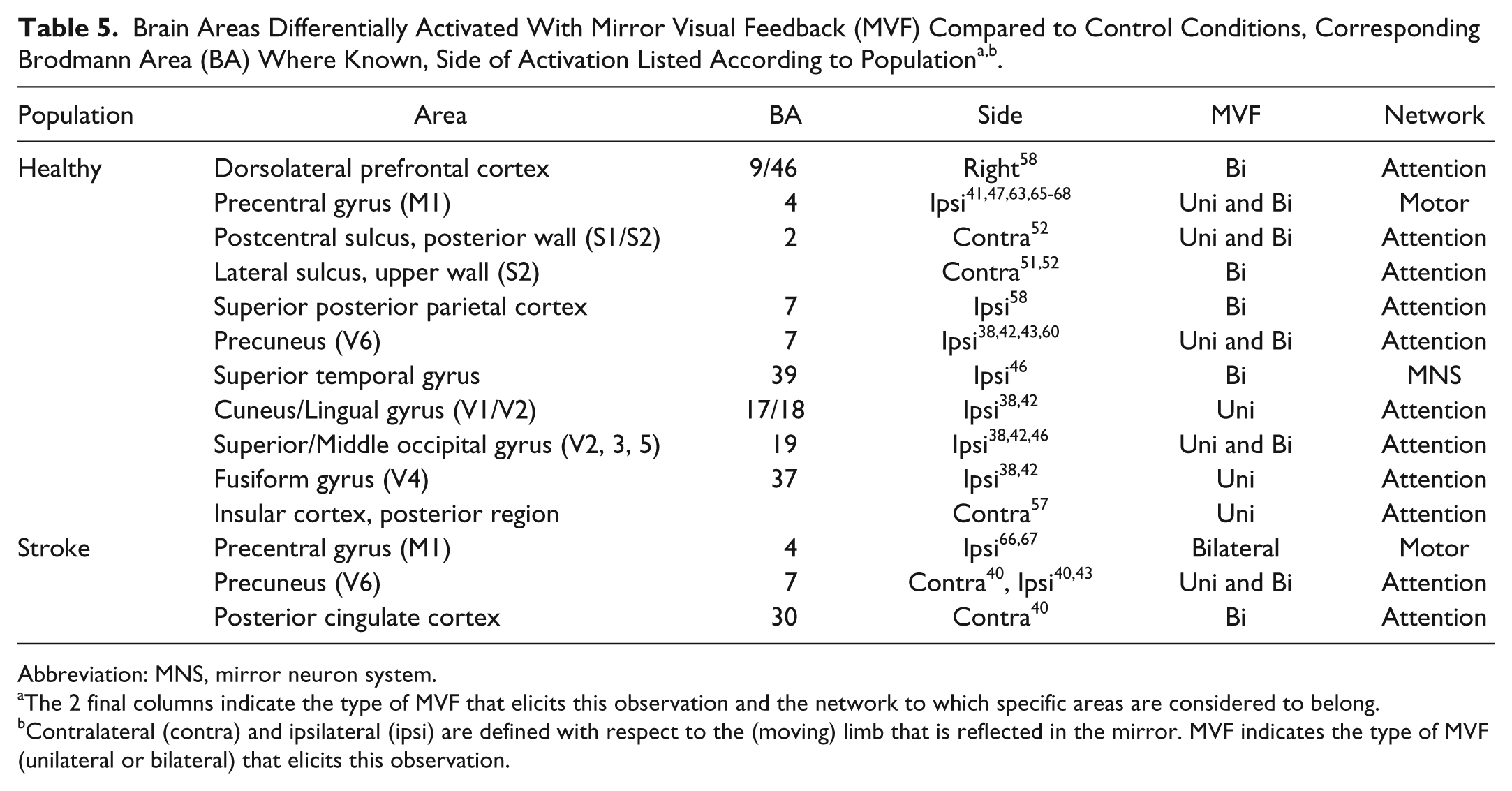
The neuromodulatory effects of MVF refer to changes in activity or excitation that are evoked by MVF, that is, revealed by direct comparison of MVF with a control condition (listed in Table 5). MVF evokes a conflict between expected and actual feedback (cognitive conflict) and between visual and kinaesthetic feedback (perceptual conflict). This conflict is most obvious when performing unimanual or asymmetric bimanual tasks, although even during symmetric bimanual actions, the perfect interlimb symmetry is perceived as surreal. In this latter case, MVF is accompanied with an increase of activity within the superior parietal lobe (precuneus [bilateral] and superior posterior parietal cortex [contralateral] 40 ), the posterior cingulate cortex, 58 and ipsilateral lateral sulcus51,52 compared to a condition with full vision of the 2 hands.
Brain Areas Differentially Activated With Mirror Visual Feedback (MVF) Compared to Control Conditions, Corresponding Brodmann Area (BA) Where Known, Side of Activation Listed According to Populationa,b.
Abbreviation: MNS, mirror neuron system.
The 2 final columns indicate the type of MVF that elicits this observation and the network to which specific areas are considered to belong.
Contralateral (contra) and ipsilateral (ipsi) are defined with respect to the (moving) limb that is reflected in the mirror. MVF indicates the type of MVF (unilateral or bilateral) that elicits this observation.
MVF inducing a more extreme conflict (during unimanual actions) stimulates activity within primary visual and somatosensory areas, as well as higher order processing areas in the occipital and parietal cortex ipsilateral to the moving limb.38,39,42,43,46,60 In fact, the mirror inverts the lateralization that is normally associated with the presentation of a right or left hand in these regions. Note, however, that these observations stem from studies that contrasted virtual MVF of the active hand with virtual VF displayed in the frontal plane (on a screen or onto MRI-compatible goggles). Other studies show increased activation in the right dorsolateral prefrontal cortex (DLPFC), 58 the contralateral secondary sensory cortex (SII), 51 the ipsilateral superior temporal gyrus (STG), 46 and the contralateral insular cortex.52,57
Finally, MVF modulates activity of the primary motor cortex, both ipsilateral and contralateral to the active hand reflected into the mirror, though the findings are somewhat inconsistent. The majority of the studies suggest an increase in ipsilateral M1 excitability or increased ipsilateral activation as indicated by a change in laterality index (vs a control condition).47,53,55,56,63,65 -68 Hadoush et al claim that this effect is more prominent for unimanual MVF, that is, when the active hand (reflected into the mirror) is covered. 48 Others show that the increase in excitability is observed particularly when MVF and motor imagery are combined.66,68 Investigation of the potential mediators of this effect suggests that MVF has the capacity to neutralize the (interhemispheric) inhibition from contralateral to ipsilateral hemisphere. Still, it should be noted that a number of studies could not find changes in activity within the ipsilateral M1 evoked by MVF.39,60,64
Neuroplastic Effects Due to Practice or Intervention With MVF
Six studies have examined the effect of a bout of practice or treatment with MVF on motor function while also measuring the change in brain activity pre and post training (see Table 4 for details).44,45,54,61,62,69 Consistent with earlier reports training with MVF resulted in a gain in motor function of the untrained or affected hand in all studies. This gain seems to be related to an enhanced excitatory function of the (contralateral) corticospinal pathway projecting to this hand (ie, decrease in motor threshold and intracortical inhibition within M1 ipsilateral to the trained hand).61,62 After training the activation balance when moving the affected hand has shifted toward M1 of the affected hemisphere, indicating increased activation of the affected side and/or decreased activation of the contralesional side.45,54,69 This would imply a reestablishment the hemispheric balance that was disrupted by the insult. Another study suggests, however, that the improvement of untrained hand is related to the establishment of a functional connection between this hand and the ipsilateral motor cortex (ie, M1 contralateral to the trained hand). 44 Dynamic causal modeling and functional connectivity analysis further indicates that this reorganization is mediated by enhanced connectivity between the premotor cortices (both left and right) and the ipsilateral supplementary motor area.
Discussion
This systematic review aimed to identify instant and long-term neuromodulatory effects associated with MVF. The findings of the 33 articles indicate that MVF engages a distributed network within the brain, including regions related to perceptual, motor, and higher cognitive functions, though it is important to acknowledge a number of limitations. Clearly, the variety of methodologies impedes the ability to draw firm conclusions. In addition, a large number of studies had relatively small sample sizes (N ≤ 10 in 17 out of 33 studies) and a number of studies fail to meet all methodological requirements, for example, equal performance across experimental manipulations or adequate control intervention (see Tables 1-3 and Supplementary Material). These limitations highlight that future research should primarily focus on isolating the effect of MVF from the mechanisms associated with bilateral training. Despite these limitations, this first systematic review of the effect of MVF on the brain reveals useful information with respect to the underlying mechanisms of MVF for both researchers and practitioners in neurorehabilitation.
Overall, the findings suggest that MVF may affect perceptuo-motor control processes via (parts of) 3 functional networks. First, the increase in activity in primary and secondary visual and somatosensory areas suggests a rise in attentional resources to resolve the perceptual incongruence.51,52 This is associated with conscious awareness of sensory feedback or control of agency, as observed in the activity within the insular cortex, 70 and enhanced monitoring of the movement, as found in the involvement of the right DLPFC.58,71 Furthermore, greater activation of the posterior aspect of the parietal and cingulate cortex supports the notion of greater attentional demands. The posterior cingulate cortex, highly interconnected with various brain regions, is considered a hub for information exchange 72 and a prominent role in the cognitive control of behavior is attributed to this region. 73 The nearby superior posterior parietal cortex and its medial extension (precuneus) are known to be involved in visuospatial information processing and directing spatial attention, especially during bimanual coordination tasks.74,75 This probably explains why the effect of MVF on the precuneus is primarily observed in studies that use virtual MVF of the hand in the frontal plane.38,39,42,43,60 Notably, a number of studies have shown that the precuneus is particularly active during motor imagery, 76 which may account for the combined effect of imagery and MVF.
Second, MVF seems to cause increased immediate activation of STG 46 and elevated engagement of PMC 44 after training. Both areas have been associated with the mirror neuron system. STG is often linked to its neighboring superior temporal sulcus and is involved in the visual identification of biological motion. 77 Combined with the PMC, it forms a network that subserves the imitation of biological motion and the acquisition of motor skills.25,78,79 The activation of PMC, especially at the side of the lesion, is in keeping with earlier research that has attributed a prominent role to this region in motor recovery after stroke.80,81
A third functional network on which MVF appears to exert a modulatory effect is the motor network. The primary motor cortex (M1) ipsilateral to the active (reflected) hand, that is, M1 projecting to the unseen hand behind the mirror, is considered the final common pathway for the beneficial effect of MVF according to various studies. A complete reversal of lateralization when moving a limb that is reflected by a mirror (ie, the ipsilateral side taking over control), as put forward by some,53,56,59 is unlikely; however, there is accumulating evidence that MVF decreases the motor threshold and enhances corticospinal output of the ipsilesional M1 in stroke patients.55,63,65-68 This is probably mediated through a reduction in interhemispheric inhibition (from contralateral/lesional to ipsilateral/lesional) 63 and/or a reduction of intracortical inhibition. 61 In view of the notion that functional recovery is correlated with the extent of involvement of the ipsilesional (here: contralateral) motor network, 82 this seems a promising therapeutic effect of MVF. Other findings in healthy adults, however, indicate that improved motor skill of the untrained hand is achieved by establishing a functional connection with the ipsilateral motor cortex via MVF, a mechanism that has been associated with poorer motor recovery compared with normalization of the hemispheric balance. 83 This discrepancy might reflect 2 stages in the recovery process or a population-specific response and warrants further investigation.
The effect of MVF on brain activation is likely dependent on the specific nature of the feedback. In this respect it is remarkable that the effect on primary and secondary visual processing areas is primarily related to unilateral MVF. Bimanual MVF, in contrast, seems to engage more frontal and parietal regions related to higher cognitive functions like attention and monitoring (see Table 5).
Finally, it is noteworthy that the findings for individuals with stroke are in accordance with those for healthy people, insofar as the limited number of studies allows this comparison (see Table 5). There is evidence of increased activation of higher order areas involved with attentional processes (precuneus and posterior cingulate cortex) and the ipsilateral M1.
Part 3: Summary and Future Directions
Convergent evidence suggests that MVF may be used as a tool to promote functional recovery in patients with unilateral motor impairments. A systematic review of neuroimaging research was conducted to test the validity of the 3 hypotheses proposed to explain the positive effects associated with MVF. The findings of this review, suggesting substantial overlap between MVF-related activity and regions subserving attention-related processes, confirm that MVF activates a broad network dedicated to attention and action monitoring (Hypothesis 3). This is consistent with known motor learning principles, which attribute success of motor practice to attentional focus and cognitive processing. Furthermore, the positive effect on motor function is associated with facilitation of M1 contralateral to the affected or untrained hand (here: referred to as ipsilateral to the moving hand that is mirrored). However, there is also evidence to support a mechanism that exploits ipsilateral control of the affected limb, which has been associated with suboptimal recovery after other therapeutic interventions (Hypothesis 2). Regions that have been linked with the mirror neuron system (PMC, STG) may play a mediating role in connecting perceptual and motor areas (Hypothesis 1). Still, the current evidence indicates that MVF therapy is certainly not a substitute for observational therapy or motor imagery, given that MVF activates only isolated parts of the MNS. Future research using recent advances in graph theory may elucidate functional connectivity within and between the involved networks. 84
To date the majority of evidence stems from studies in healthy adult individuals and the few studies that have examined a patient population only considered people who survived a stroke. It remains unclear to what extent these hypotheses may be valid for other clinical conditions for which MVF has been suggested an adjunct to conventional therapy (eg, SHCP22,85-87 and CRPS14-18). The finding that MVF may have an impact on multiple functional networks may mean it can serve as a versatile tool to promote motor recovery, of which the actual mechanism is dependent on the specific condition or damage. Large-scale clinical trials that include measurement of brain function and structure are to examine the efficacy and the underlying mechanisms of MVF in different populations, and potential differences between them. Although further research is warranted to fully understand and exploit the potential of MVF in neurorehabilitation, it is indisputable that MVF can exert a strong modulatory influence on the motor system.
Footnotes
Acknowledgements
The authors wish to thank Prof Karen Caeyenberghs and two anonymous reviewers for their advice and suggestions.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This work was partly supported by a research grant from Sparks, registered charity 1003825 (England & Wales), to Geert Savelsbergh and Frederik Deconinck (Grant 09MMU01).
Supplementary Material
*
In their recent review article, Ramachandran and Altshuler 9 recognize that the origin of phantom pain is still poorly understood and may be related to other factors, for example, persistence of preamputation pain and pathological “remapping” among others (see also Ramachandran and Hirstein 6 ). The rationale to use MVF, however, is based on the notion of a mismatch between motor output and visual and/or proprioceptive feedback.
†
The effect of MVF therapy was significantly larger than control interventions.
*
Mirror visual feedback could be induced by a real mirror or using a virtual reality environment.
‡
See Ramachandran and Altschuler 9 for a list of clinical cases where the use of MVF has been observed informally but has not been described in the literature.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.