
Abstract
Background and Objective. γ-Aminobutyric acid (GABA) is the dominant inhibitory neurotransmitter in the brain and is important in motor learning. We aimed to measure GABA content in primary motor cortex poststroke (using GABA-edited magnetic resonance spectroscopy [MRS]) and in relation to motor recovery during 2 weeks of constraint-induced movement therapy (CIMT). Methods. Twenty-one patients (3-12 months poststroke) and 20 healthy subjects were recruited. Magnetic resonance imaging structural T1 and GABA-edited MRS were performed at baseline and after CIMT, and once in healthy subjects. GABA:creatine (GABA:Cr) ratio was measured by GABA-edited MRS. Motor function was measured using Wolf Motor Function Test (WMFT). Results. Baseline comparison between stroke patients (n = 19) and healthy subjects showed a significantly lower GABA:Cr ratio in stroke patients (P < .001) even after correcting for gray matter content in the voxel (P < .01) and when expressing GABA relative to N-acetylaspartic acid (NAA; P = .03). After 2 weeks of CIMT patients improved significantly on WMFT, but no consistent change across the group was observed for the GABA:Cr ratio (n = 17). However, the extent of improvement on WMFT correlated significantly with the magnitude of GABA:Cr changes (P < .01), with decreases in GABA:Cr ratio being associated with better improvements in motor function. Conclusions. In patients 3 to 12 months poststroke, GABA levels are lower in the primary motor cortex than in healthy subjects. The observed association between GABA and recovery warrants further studies on the potential use of GABA MRS as a biomarker in poststroke recovery.
Introduction
Despite recent advances in acute stroke treatment and post stroke rehabilitation, many stroke survivors suffer long-lasting impairment. The typical stroke patient slowly regains partial function during the first months after stroke. 1 This recovery depends on factors such as lesion size and location, 2 but the neuronal underpinnings of successful stroke recovery remain poorly understood.
Poststroke recovery and rehabilitation rely on mechanisms of learning and brain plasticity. 3 Such mechanisms appear to be modulated by GABAergic inhibition, as demonstrated in animal studies of cortical learning and plasticity. For example, reduced inhibition can unmask unused synapses in motor cortex. 4 Furthermore, long-term potentiation (LTP), an important cellular learning mechanism, depends on decreased GABAergic activity in the motor cortex. 4 Consistent with this role of GABA (γ-aminobutyric acid), recent neuroimaging studies have shown that the modulation of cortical GABAergic activity is a key factor in human motor learning. 5 Together, this evidence suggests that GABAergic inhibition has relevance to recovery after stroke.
GABAergic activity poststroke has been investigated using techniques such as paired-pulse transcranial magnetic stimulation (TMS),6-9 positron emission tomo-graphy (PET), 10 and pharmacological challenges. 11 Most studies have reported a decrease in inhibitory activity, but interpretations of this finding vary and neither PET nor TMS measures the amount of GABA directly; rather they detect changes in receptor levels or a combination of receptor and transmitter changes.
GABA-edited MEGA-PRESS magnetic resonance spectroscopy (MRS) is a noninvasive technique sensitive to the amount of GABA in tissue. 12 We hypothesized that, in patients suffering from motor deficits after stroke, the concentration of GABA in motor cortex is reduced so as to facilitate motor recovery. Moreover, we aimed to investigate changes in GABA levels during motor recovery. We performed GABA-edited MEGA-PRESS MRS before and after training in a cohort of stroke patients undergoing two weeks of constraint-induced movement therapy (CIMT). 13 CIMT combines mass practice of the impaired hand/arm with immobilization of the unaffected hand in patients with arm paresis. The short- and long-term effect of CIMT for stroke patients has been investigated in randomized trials,13-15 and a Cochrane review has found CIMT to be associated with a moderate reduction in disability. 16 The present results are part of a larger study for which motor and cognitive performance in these patients have been reported. 17
Methods
The study was approved by the local ethics committee (De Videnskabsetiske Komitéer for Region Midtjylland) and all participants gave written informed consent.
Subjects
During a 12-month period, all patients undergoing CIMT at a local rehabilitation hospital (Hammel Neuroreha-bilitation and Research Centre) were screened. Participants between 18 and 80 years were included if they had suffered from a single clinical stroke 3 to 12 months earlier and had persistent motor impairment of the upper extremity, with at least 10° of active wrist extension, at least 10° of thumb abduction/extension, and at least 10° of extension in at least 2 additional digits (as in the lower functioning group in the EXCITE trial 13 ). Patients were excluded if they had contraindications to magnetic resonance imaging (MRI) or suffered from other neurological disorders, such as epilepsy or dementia. Twenty-one patients (12 male, mean age 60 years, range 36-75 years) were recruited (see Table 1). A control group consisting of 20 age- and gender-matched healthy subjects (11 male, mean age 61 years, range 40-75 years, all right-handed) were scanned for comparison.
Patient Characteristics.
No follow-up because of illness during constraint-induced movement therapy. The patient was unable to complete the training.
Left-handed, all other patients were right-handed.
Intervention and Outcome Measure
Patients completed 2 weeks of CIMT as described in the EXCITE trial, 13 except that the patients were trained in groups of 4 participants, each group being trained by a physiotherapist and occupational therapist. Motor performance was measured before and after CIMT using Wolf Motor Function Test (WMFT). 18 The test was performed by the clinical physiotherapist, who was blinded to the MR analyses.
Magnetic Resonance Imaging and Spectroscopy
Participants were scanned on a 3T MR system (Siemens Trio, Erlangen, Germany). Patients were scanned before (mean 4 days) and after (mean 3 days) the 2 weeks of training, whereas healthy subjects were scanned only once. The scan protocol included structural T1 (MPRAGE), GABA-edited MRS, BOLD (blood oxygen level–dependent) functional and resting-state MRI with a total scan time close to 1 hour. The results from the functional and resting-state data will be published separately. A T1 MPRAGE scan (TR/TE 2420/3.7 ms, 1 mm isotropic resolution, scan time 5.5 minutes) was performed and used for voxel placement and post hoc tissue segmentation. GABA-edited MRS was performed using MEGA-PRESS (TR/TE = 2500/68 ms). Editing was achieved with a 14-ms dual-banded Gaussian editing pulse with 1 inversion band alternating between 1.9 ppm (edit-on) and 7.5 ppm (edit-off) in even and odd acquisitions, respectively, and a water suppression band centered at 4.7 ppm. A 2 × 2 × 2 cm voxel was placed in the “hand knob” area 19 of the affected hemisphere of the patients (Figure 1) and in the dominant hemisphere of the healthy subjects. A total of 186 averages each of edit-on and edit-off spectra were recorded leading to a scan time of 15.5 minute for MRS. A water reference scan was also acquired using 8 averages without an editing pulse.
Example of magnetic resonance spectroscopy voxel placement in the affected hemisphere.
Magnetic Resonance Analysis
A semiautomated preprocessing routine was applied to all spectra to remove motion corrupted averages, and to correct for frequency and phase drifts. 20 Apodization was performed with a 5-Hz filter in all spectra. Zero- and first-order phase corrections were applied. Then, GABA, creatine (Cr), and N-acetyl aspartate (NAA) peaks were estimated using AMARES 21 within jMRUI. 22 GABA and NAA amplitudes were measured from the difference between the 2 subspectra (even − odd; Figure 2), while Cr was measured from the sum of the subspectra (even + odd). GABA:Cr ratio was the primary outcome measure as Cr is often used as reference compound in in vivo GABA MRS. 23 To evaluate GABA relative to neuronal content within the voxel GABA:NAA ratio was determined. The researcher performing the analysis was blind to the time point at which the spectra were acquired and to whether the spectra were acquired from a patient or healthy control.
Example of a filtered difference spectrum in a patient. Arrow indicating the GABA (γ-aminobutyric acid) peak at 3 ppm.
To control for potential differences in gray matter (GM) volume between patients and controls, the fraction of GM within the voxel was determined by segmentation of the T1 images using the segmentation tool within the Statistical Parametric Mapping software (SPM8, http://www.fil.ion.ucl.ac.uk/spm/). 24
Statistics
For baseline comparison between patients and healthy subjects, GABA:Cr ratios were compared using an independent t test, as data were normally distributed. Within-subject changes in GABA:Cr ratios after training were tested using a paired t test. To correct for neuronal- and GM-content within the voxel, a second analysis was performed using GABA:NAA and GABA/GM/Cr ratios. We tested whether changes in motor functional recovery (WMFT) were related to GABA changes, GM changes, or both, by simple and multiple regression. The quality measure from WMFT was used as primary outcome measure as the time component data was not normally distributed. All statistical analyses were performed using Matlab (R2010b).
Results
One patient did not complete the 2-week training and follow-up scan because of an unrelated infection. In 3 stroke patients, MRS could not be collected due to technical problems (2 baseline and 1 follow-up), leading to a total of 19 baseline and 17 complete pre- and posttraining patient datasets. Patients were typically treated with standard secondary prophylactic drugs (antithrombotic, antihypertensive, and anticholesterols). Moreover, 15 out of 21 patients were treated with antidepressants (mainly selective serotonin reuptake inhibitors [SSRIs]), while no patients received benzodiazepines or antiepileptic drugs. All medications were kept stable during the study period.
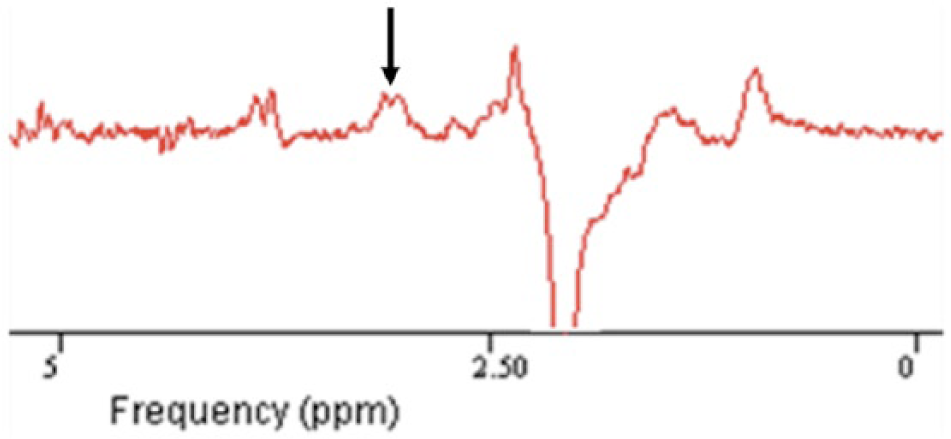
We first directly compared GABA levels before the intervention between patients and controls. In patients, pretraining GABA:Cr ratios were significantly lower (mean 0.33, SD 0.06) than those of healthy controls (mean 0.42, SD 0.08), t(37) = −3.88, P < .001 (Figure 3). The amount of GM within the voxel was similar between patients (34%) and healthy subjects (35%), and after correcting for GM volume, patients still had significantly lower GABA:Cr ratio, t(37) = −2.75, P < .01. The GABA:NAA ratios were also significantly lower in patients than in healthy controls, t(37) = −2.24, P = .03, whereas no significant difference could be found for NAA:Cr (P = .15). We observed no difference in GABA:Cr between patients on antidepressants (0.33, SD 0.06) and the rest of the patients (0.33, SD 0.06), and when comparing the subgroup of patients not taking antidepressant (0.33, SD 0.06) with healthy subjects (0.42, SD 0.08) we still observed a lower GABA:Cr ratio in patients, t(24) = −2.57, P = .02. No correlation between GABA:Cr and time since stroke was observed (P > .05). To address a possible confound of variation in GABA between the dominant and nondominant hemisphere, the subgroup of right-handed patients with left hemisphere stroke (n = 8) was compared with the healthy control group (all with left hemisphere voxel placement); this also showed a significantly lower GABA:Cr (P < .05).
GABA:Cr (mean, SEM) was significantly lower in patients post stroke and prior to CIMT, compared to healthy subjects
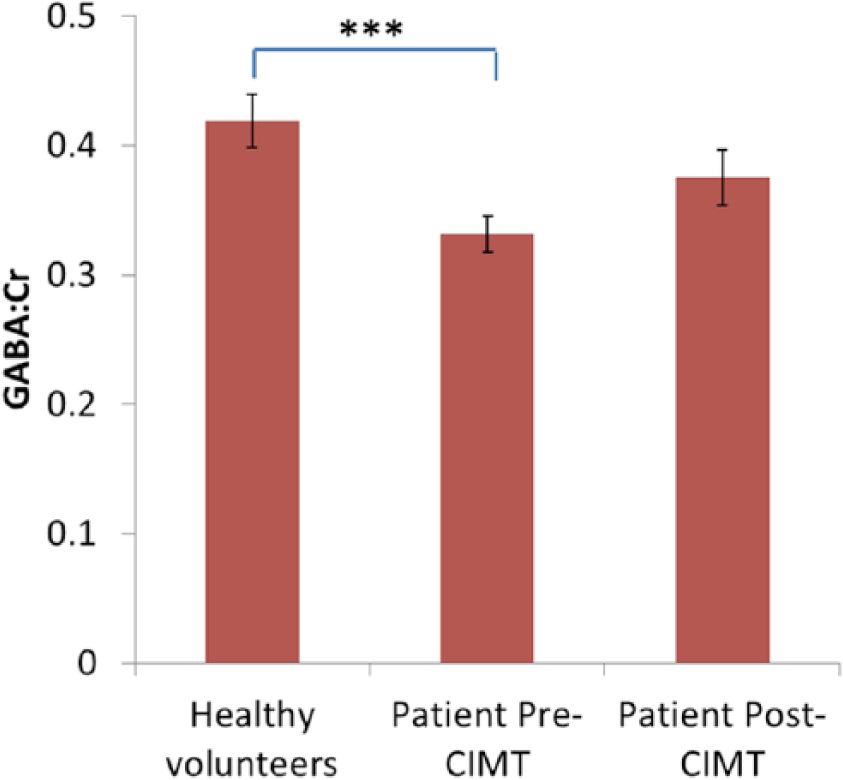
After 2 weeks of training, patients improved significantly on the WMFT (for the 17 patients with complete MRS data sets, t(16) = 9.82, P < .001). Somewhat counterintuitively, GABA:Cr ratios tended to increase during training (Figure 3; GABA:Cr pretraining mean 0.34 [SD 0.06]; posttraining mean 0.38 [SD 0.09]), t(16) = −1.97, P = .07; but after correcting for GM content at each time point no significant difference was observed, t(16) = −0.82, P = .42. The GABA:NAA ratio did not change significantly during training, t(16) = −0.21, P = .83. The improvement in WMFT quality scores was negatively correlated with the fractional GABA:Cr changes ([GABA:CRpost − GABA:CRpre]/GABA:CRpre) (R2 = 0.38, R = −0.61, P = .009), with patients with the largest improvement in WMFT scores showing smaller increases, or even decreases, in GABA:Cr ratios post training (Figure 4). No significant correlation between pre- or posttraining GABA:Cr and WMFT changes was found. However, a trend was observed between high GABA:Cr ratios at baseline and larger improvements in WMFT (P = .17). Also, there was no significant correlation between functional improvement and GM changes within the MRS voxel (R2 = .0028, R = −0.053, P = .84). Using both GABA:Cr changes and GM changes as explanatory variables to model the WMFT score changes in a multiple regression model, only a significant effect of GABA:Cr changes was shown (overall model, R2 = 0.41, P = .024; GABA:Cr changes, β = −7.31, P = .0075; GM volume changes, β = −2.95, P = .36, where β denotes the estimated regression coefficient), supporting the hypothesis that it was GABA:Cr changes, rather than GM volume changes, that explained the WMFT score changes. To address the possibility that changes in Cr could explain the observed correlation between GABA:Cr and WMFT, we tested whether changes in NAA:Cr correlated with changes in WMFT, but found no significant association between the two (P = .11).
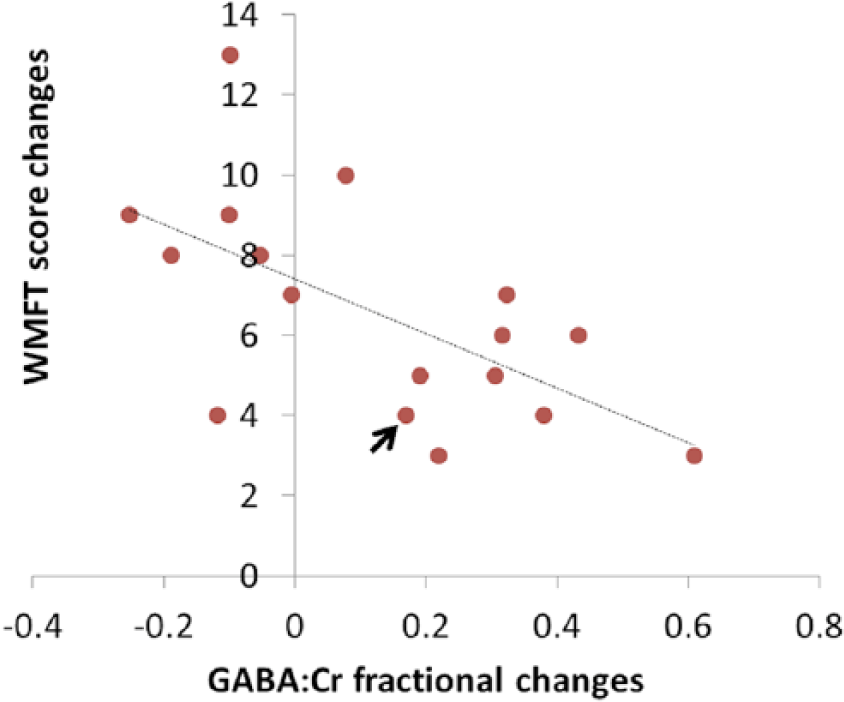
Larger motor improvements (WFMT) were associated with smaller or even negative GABA:Cr fractional changes (R = −0.61, P = .009). Arrow indicating the patient with a lesion in the hand area.
Discussion
We investigated poststroke GABA levels using GABA edited MRS. We found significantly lower GABA levels in patients compared to controls and demonstrated a significant correlation in patients between GABA changes during rehabilitation and motor improvement, indicating a potential role for GABA in poststroke recovery.
Lower GABA Levels Poststroke Compared With Healthy Subjects
Earlier studies using techniques such as paired-pulse TMS6-9 and flumazenil PET10,25 have suggested a decrease in inhibition poststroke. While these techniques are sensitive to changes in GABA receptor levels, our edited MRS approach is a more direct measure of the local concentration of GABA. We found significantly lower GABA:Cr ratios in patients compared to controls, and this difference was also significant after correcting for GM content within the voxel, suggesting that the decrease in GABA in the stroke patients cannot be explained by cortical atrophy alone. We further strengthened this conclusion by expressing GABA levels relative to NAA, a widely accepted neuronal marker, again showing that GABA levels are reduced relative to the neuronal content within the motor cortex. Taken together, the results extend previous studies using TMS and PET by showing decreased cortical GABA levels poststroke.
Prior studies reporting a decrease in GABA activity poststroke have explained the findings in several ways: (a) by a selective loss of GABA neurons during ischemia (primarily PET studies 10 ), (b) by a functional disinhibition that supports motor recovery,6,7 or (c) by the maintenance of the achieved motor function in the chronic stage.8,11 Pharmacological studies have suggested that a decrease in GABAergic activity is directly linked to the maintenance of motor function in the chronic stage after stroke, as GABA agonists can lead to a loss of recovered function after stroke. 11 We find it most likely that the observed decrease in GABA levels in the current study is caused by a functional decrease in inhibition that supports either recovery or maintenance of motor ability (Figure 5A1). Most patients had subcortical lesions, and it therefore appears that selective loss of (cortical) GABAergic neurons is an unlikely source of the lower GABA levels (Figure 5B2).
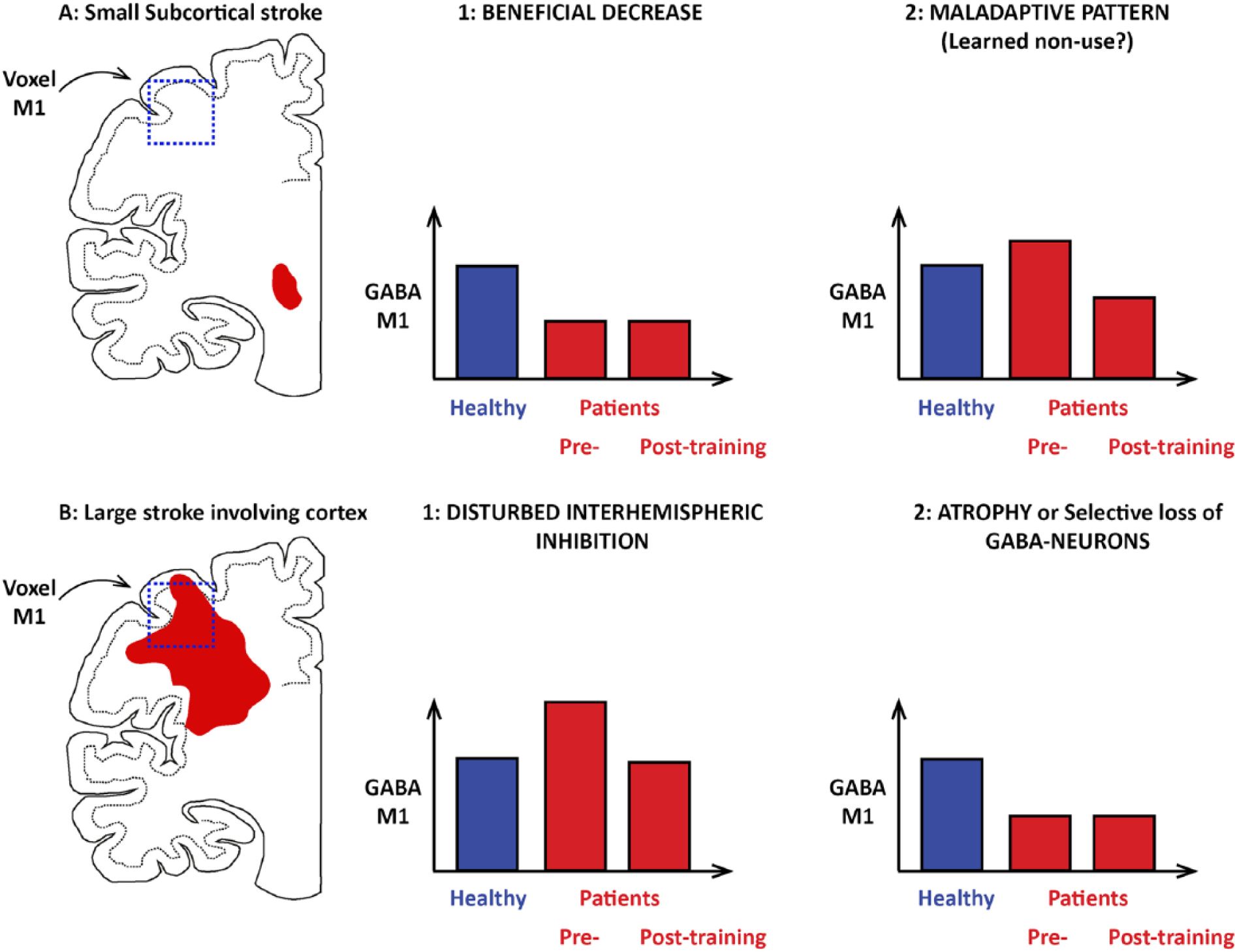
Examples of stroke location and possible changes in M1 GABA (γ-aminobutyric acid) levels after a small subcortical stroke (A) or a large stroke extending into cortex (B). (A1) Beneficial decrease in GABA as a compensatory phenomenon facilitating or maintaining motor recovery. (A2) Maladaptive pattern of GABA increase as a part of a learned nonuse pattern. (B1) Disturbed interhemispheric inhibition leading to a high inhibitory drive from unaffected to affected hemisphere. (B2) Decrease in GABA levels due to loss of GABA neurons in the affected M1 cortex. In case A2 and B1, a training-induced drop in M1 GABA could be associated with a large improvement in motor function after constraint-induced movement therapy (CIMT).
GABA Changes in Relation to Motor Recovery
Consistent with previous studies, we found a significant improvement in motor performance in patients after two weeks of CIMT. 13 In parallel with this improvement in function we observed a tendency for GABA to increase. However, no significant difference could be observed after correcting for the GM fraction within the voxel, suggesting that this increase may be driven by a generalized increase in neuronal activity within the trained motor cortex, rather than a specific change in GABAergic activity. Moreover, no significant changes could be observed when GABA was expressed as a ratio of NAA.
Despite no statistically significant changes in GABA levels between pre- and posttraining across the group as a whole, there was a significant negative correlation between individual changes in GABA and motor improvement, unrelated to changes in GM content, during the 2 weeks of CIMT. These results suggest that a greater decrease in cortical GABA can be linked to motor rehabilitation in the chronic setting, in agreement with findings in animal studies4,26—see also Carmichael. 2 As causality cannot be inferred from the correlation, it is possible that it was the motor improvement that drove down GABA in the patients that improved the most. However, a more likely explanation is that the decrease in GABA activity facilitated motor recovery.
Unlike MRS, TMS has been used to investigate cortical inhibitory activity in stroke patients for more than a decade. Studies using paired-pulse TMS have found evidence for intracortical disinhibition in the affected hemisphere 6 acutely and in the more chronic stage after stroke.7,8 Other TMS studies have investigated the relationship between the lesioned and the intact hemispheres after stroke and found a high task-related interhemispheric inhibitory (IHI) drive from the intact hemisphere, which was associated with poor motor recovery in some patients in the chronic stage after stroke. 27 Based on our current MRS results and the prior TMS literature, we hypothesize that our findings can be explained by patients showing different patterns of GABA modulation prior to and during CIMT (Figure 5). Likely, some patients had maladaptive patterns as disturbed IHI (Figure 5B1) or learned nonuse (Figure 5A2) at baseline. Both disturbed IHI 27 and nonuse (as investigated during limb immobilization28,29) have previously been shown to cause high task-related inhibitory activity. CIMT has been specifically designed to reverse learned nonuse and thus we hypothesize that patients with a pronounced nonuse pattern benefitted the most from training, and that GABA would tend to decrease. Both animal studies 26 and very recent results in stroke patients 30 have indicated that reversal of high cortical GABA levels is associated with clinical improvement.
However, patients with less nonuse and a beneficial decrease in GABA at baseline (Figure 5A1) likely had less of an improvement during CIMT and GABA remained unchanged during the training period. We have previously shown that in a group of well recovered stroke patients inhibitory activity is decreased in motor cortex, but unlike in healthy subjects’ no further decrease was seen in relation to training, possibly because of a lower limit for beneficial GABA decrease. 8 The proposed model would explain the observed association between larger functional improvement and a GABA decrease during CIMT, and the observed trend between high GABA levels at baseline and larger improvement in function. Prior studies have found a high between-subject variation in GABA whereas GABA is rather stable within a subject over time.31-33 The high between-subject variation makes it difficult to use baseline M1 GABA to predict response to therapy, likely explaining why the association between baseline GABA and improvement in WMFT is nonsignificant. It would have been preferable to measure GABA bilaterally so that GABA levels in the affected hemisphere could be expressed as a ratio of GABA in the unaffected hemisphere or in another area as the occipital lobe, thus correcting for the between subject variation. However, the time limitations of our experimental protocol precluded the additional MRS measurement of GABA within the intact hemisphere. A recently developed technique using MRS imaging of GABA 34 could be of potential use in future studies exploring bihemispheric changes in GABA.
Technical Considerations and Study Limitations
Several issues need to be considered when interpreting the results. First, GABA-edited MRS takes advantage of the chemical properties of GABA, so that GABA can be visualized, unlike in standard MRS in which the GABA peak is overlapped by the peaks of other compounds, like the Cr peak at 3 ppm. Unfortunately, the editing pulse used to visualize GABA in MEGA-PRESS is not specific to GABA, thus certain macromolecules will be coedited and resonate at the same frequency as the GABA peak (3.0 ppm). Prior studies have estimated that macromolecules are in fact accounting for between 34% and 46% of the measured signal.35,36 For this reason, GABA measured in this way is occasionally labeled GABA+. Thus, one should consider to what extent our results can be explained by changes in macromolecules instead of GABA (see also Mullins et al 23 ).
Second, our primary outcome was a ratio of GABA to Cr, and thus it should be considered whether the observed differences could be explained by changes in Cr rather than GABA. Decreases in Cr have indeed been reported in the infarcted areas poststroke.37,38 In this study, only one of the participating patients had an infarct located inside the investigated hand area—the others had subcortical lesions (excluding the patient with a lesion in M1 did not change the observed results). Therefore, it is unlikely that there were significant changes in Cr within the investigated hand area. Moreover, a decrease in Cr in patients would lead to higher GABA:Cr ratios, as opposed to what we observed. The advantage of using Cr as a reference compound is that it resonates at the same frequency as does GABA. Compounds resonating at other frequencies (like NAA) will be measured in a slightly different physical location in the brain (for this specific sequence, NAA would be shifted 2.4 mm). This is because of so-called chemical shift displacement. Cr and GABA both resonate at 3 ppm and thus the tissue contributing to the measured signal will be identical in this case.
Third, the stability of GABA measured by MRS is until recently only been investigated up to 1 week. 32 However, we recently demonstrated that GABA:Cr is fairly stable within the occipital lobe of healthy subjects up to 7 months, using the same scanner as in the present study. 33 For this reason, healthy control subjects were only scanned once as we did not expect GABA to change. Furthermore, we find it unlikely that random variation in GABA can explain our results. It is known that GABA tends to decrease with age, 39 and this is why we recruited an age-matched control group. In the present study however, we found no correlation between GABA and age (results not shown).
Cortical GABA levels are affected by a broad range of drugs, including SSRIs. A study on the acute effects of SSRIs found an increase in GABA:Cr ratio in healthy subjects. 40 In depressed patients, it has been shown that GABA:Cr ratios increase after two months of SSRI usage. 41 Therefore, while it is unknown whether SSRIs have different effects in poststroke patients, GABA levels in general are expected to increase, and therefore cannot explain our observed decrease in GABA:Cr. Moreover, the small subgroup of patients not taking antidepressants still showed significantly lower GABA levels than healthy subjects. Consequently, we believe that our results can be interpreted as genuine changes in GABA related to the prior stroke.
From an MRI perspective the current study follows a large cohort of patients undergoing CIMT. However, from a clinical perspective, the cohort may be relatively small, particular in view of the heterogeneity of the studied patient group, which could also be a factor in why we found no significant changes in GABA:Cr or GM per se during CIMT. The study is also limited by the fact that the same therapists are involved in both training patients as well as testing the patients with WMFT. The nonblinded raters might be the reason why we observe a slightly higher average gain in the WMFT (0.4) compared with the EXCITE trial (0.3). 13 Raters were however blinded to the MRS results so the association between WMFT and GABA are not expected to be biased.
Implications
We have shown that GABA levels are reduced 3 to 12 months poststroke. After CIMT rehabilitation, the magnitude of individual patient GABA changes was significantly correlated with the extent of improvement in motor performance: Patients with decreases in GABA after therapy tended to benefit more from rehabilitation. We postulate that this could be caused by interhemispheric disturbances being more pronounced at baseline in patients who benefited the most from training. Such possible bihemispheric changes in GABA after stroke could be explored in future studies, as well as the potential for the use of GABA MRS in selecting patients for neuromodulatory interventions in rehabilitation.
Footnotes
Acknowledgements
The authors thank Kim Mouridsen for useful statistical advice.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This work was supported by the Danish Ministry of Science, Technology and Innovation’s University Investment Grant (MINDLab [902063] to JUB). HJ-B and CJS are supported by the Wellcome Trust and by the National Institute for Health Research (NIHR) Oxford Biomedical Research Centre based at Oxford University Hospitals NHS Trust and University of Oxford.