
Abstract
Background. Constraint-induced movement therapy (CIMT) has proven effective in increasing functional use of the affected arm in patients with chronic stroke. The mechanism of CIMT is not well understood. Objective. To demonstrate, in a proof-of-concept study, the feasibility of using kinematic measures in conjunction with clinical outcome measures to better understand the mechanism of recovery in chronic stroke patients with mild to moderate motor impairments who undergo CIMT. Methods. A total of 10 patients with chronic stroke were enrolled in a modified CIMT protocol over 2 weeks. Treatment response was assessed with the Action Research Arm Test (ARAT), the Upper-Extremity Fugl-Meyer score (FM-UE), and kinematic analysis of visually guided arm and wrist movements. All assessments were performed twice before the therapeutic intervention and once afterward. Results. There was a clinically meaningful improvement in ARAT from the second pre-CIMT session to the post-CIMT session compared with the change between the 2 pre-CIMT sessions. In contrast, FM-UE and kinematic measures showed no meaningful improvements. Conclusions. Functional improvement in the affected arm after CIMT in patients with chronic stroke appears to be mediated through compensatory strategies rather than a decrease in impairment or return to more normal motor control. We suggest that future large-scale studies of new interventions for neurorehabilitation track performance using kinematic analyses as well as clinical scales.
Introduction
Stroke occurs in approximately 795 000 Americans a year and is the leading cause of adult disability. 1 Between 30% and 66% of patients are left with limited arm function 6 months after stroke. 2 There is clearly a need for interventions that can improve arm function beyond what is regained through spontaneous recovery and conventional rehabilitation. Constraint-induced movement therapy (CIMT) has emerged as a promising intervention in subacute3,4 and chronic5,6 stroke. In CIMT, the unaffected arm is restrained for a majority of waking hours while the affected arm undergoes task-based practice. 7 The mechanisms underlying the functional improvement seen with CIMT are not well understood at either the neural or the behavioral level.8,9 Are patients regaining more normal control of their affected arm after CIMT, or are they learning to use compensatory strategies?
The distinction between motor recovery and compensation is often not addressed in rehabilitation studies.10,11 We define motor recovery as the reemergence of movement kinematics similar to those of healthy age-matched controls, resulting from a decrease in impairment, whereas compensation involves the use of the unaffected limb or alternative muscle groups on the affected side to accomplish a task. For example, with hemiparesis patients may engage excessive truncal or scapular movement while reaching12,13 or use alternative grasp strategies 14 to pick up objects. A concern that has been raised is that emphasis on the use of compensatory strategies to achieve immediate functional gains may be detrimental to long-term motor recovery,13,15,16 although this has not been systematically examined.
Most studies of CIMT have used self-reported questionnaires or functional scales that are unable to distinguish between improvements resulting from motor recovery and those attributable to compensation. 17 The primary outcome measures in the largest randomized controlled trial of CIMT to date were a patient questionnaire (Motor Activity Log) and a functional arm test (Wolf Motor Function Test) involving timed and strength tasks. 4 A few studies have also investigated the effect of CIMT on tests of arm impairment in chronic stroke patients, most commonly using the Upper-Extremity Fugl-Meyer Assessment (FM-UE), with variable results.5,18-22 Mean changes in FM-UE scores in these studies ranged from 3 to 19, with the larger changes occurring with lower-intensity, longer-duration treatment protocols.20,21 Limitations of the FM-UE as an impairment assessment tool include a ceiling effect in patients with mild deficits and its 3-graded scale, which may limit its responsiveness to change. 23 Kinematic analysis can provide objective, quantitative, fine-grained measures of arm motor impairment after stroke, 24 with the ability to detect and quantify even subtle differences in movement patterns, which is crucial for a mechanistic understanding of this increasingly popular therapy.
The few studies that have assessed kinematics before and after CIMT17,18,25,26 have shown reduced reaction time, 18 reduced movement duration,17,18,26 increased smoothness, 26 reduced path length, 18 and reduced trajectory variability.17,26 Massie et al 17 found that patients used more shoulder abduction to reach after CIMT, which suggests that some of the functional improvements seen with CIMT may be a result of compensatory strategies rather than reacquisition of normal motor control. These prior kinematic studies characterized unrestrained 3-dimensional movements and so did not test patients’ abilities to perform tasks under conditions that do not allow the use of compensatory strategies. Indeed, patients may continue to use compensatory habits despite a degree of neural recovery that would actually allow for a more normal movement pattern if they were to attempt it. 27 Therefore, we argue that patients’ level of impairment should be tested on a constrained kinematic task designed to preclude the use of compensation.
In the current study, compensatory strategies were minimized in the kinematic tasks through the use of constraints, with the aim of capturing measures reflecting “true” impairment. For example, the arm task used in the current study required planar reaching movements (hand, elbow, and shoulder had to be level), with participants seated in a setup that limited trunk and shoulder movement (Figure 1). When reaching movements are planar, there is only a single joint angle solution pair at the elbow and shoulder for a given end point. Thus, in our tasks, patients could not use compensatory strategies that take advantage of the multiple degrees of freedom available when performing 3-dimensional reaching movements. That is to say, we tested for impairment in a system that does not have redundancy that can be exploited by compensation.14,28 Our tasks were relatively simple movements designed to test an elementary level of motor control in the proximal arm and wrist and can be considered the arm and wrist analogues of quantitative tests of finger individuation. 29 That these tasks capture an elementary level of multijoint limb control is supported by the observation that healthy participants are able to perform them making movements with straight trajectories and high end-point accuracy 30 with minimal practice despite having little experience with planar reaching or isolated visually guided wrist movements in everyday activities. 31 Previous kinematic studies in patients with hemiparesis have shown deficits in trajectory and end-point control, with increased initial directional error, 32 path curvature, 33 end-point error, 34 and segmentation.33,35 These are the 4 kinematic outcome measures that we used in the current study to assay for reductions in arm impairment.
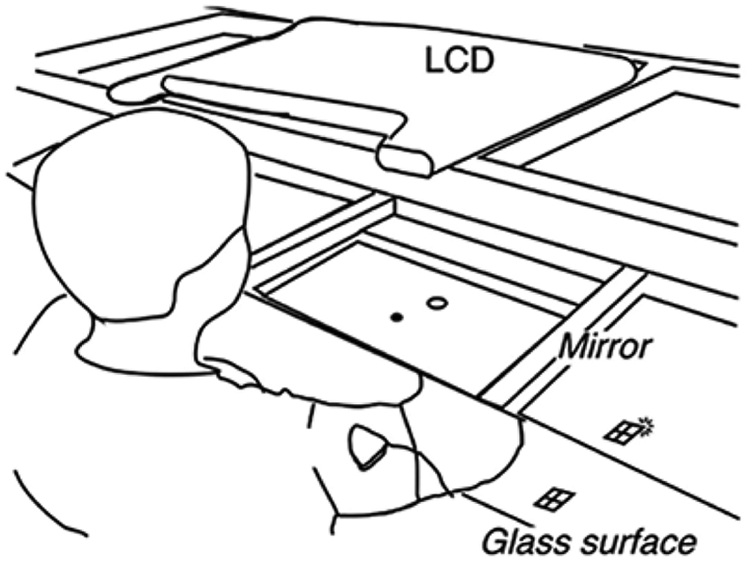
Setup for the arm reaching task: participants were seated with the shoulder, elbow, and hand aligned in the same plane, and the their trunk was secured between the table and chair to limit truncal displacement. The wrist, hand, and fingers were immobilized with a splint, thus confining movements to the shoulder and elbow, and the forearm was supported on an air-sled system, which removed friction. Participants viewed a mirror that reflected an LCD display, and the arm was obscured from view
A recent meta-analysis found a graded effect of modified CIMT, with the largest effects on arm function (measured by the Action Research Arm Test [ARAT]), significant but smaller effects on arm impairment (measured by the FM-UE), and improvements in some kinematic variables but not others. 36 However, no single study has compared improvements at all 3 levels, as was done in the current study, in which patients with chronic stroke participated in a modified CIMT program and were evaluated with clinical scales of motor function and impairment as well as with kinematic analysis of arm and wrist movements. We hypothesized here that the main effect of CIMT is to promote functional use of the affected arm primarily through compensatory strategies and not through a reduction in impairment (ie, motor recovery), given the task-oriented nature of the training intervention and findings of a prior study 17 of CIMT. Therefore, we predicted that we would see the greatest improvements in the ARAT and more modest, if any, improvements in the FM-UE and in kinematic variables.
Methods
Study Participants
A total of 10 patients with chronic stroke were recruited from a local rehabilitation hospital and outpatient neurological practices between May 2005 and February 2007. Participants met the following inclusion criteria: (1) ischemic or hemorrhagic stroke at least 6 months prior to enrollment, (2) motor deficit involving 1 arm with the ability to perform at least 20° wrist extension and 10° finger extension, (3) significant unaffected hand use for activities of daily living, and (4) ARAT score <50 in the affected arm. Inclusion criteria (2) and (3) are similar to those used in previous studies of CIMT that demonstrated functional motor improvements, 4 and we required patients to have a demonstrable deficit on the ARAT to avoid a potential ceiling effect. Patients were excluded if they had only ataxia or sensory symptoms, were unable to give informed consent or were unable to participate in training because of aphasia or cognitive impairment, had significant pain or musculoskeletal problems that would interfere with intensive training, or were receiving ongoing physical therapy for the arm. All participants signed a written consent form that was approved by the local institutional human research review board.
Intervention
All patients completed 2 weeks of CIMT at home under the supervision of a licensed physical therapist, with a goal of 4 hours a day for 10 consecutive weekdays. This was a modified version of the original CIMT protocol, which consisted of 6 hours of therapy a day for 10 consecutive weekdays. 4 Therapy sessions began with active range of motion and/or stretching exercises, then proceeded to task-based activities that were individualized based on the patient’s goals and interests. Activities included folding clothes, eating, writing, throwing a ball, and playing games (eg, chess and Jenga). Task difficulty was adjusted for individual patients to be sufficiently challenging as determined by the therapist, and shaping techniques were incorporated, with increasing task difficulty over successive sessions. Verbal feedback was provided to participants during task practice. The time spent in each activity ranged from 1 to 15 minutes, depending on the patient’s level of interest and endurance. The total activity time was recorded for each session by the therapist. Participants were also encouraged to wear the mitt on their unaffected hand outside of therapy and reported their compliance.
Study Design
Clinical and kinematic assessments were performed at 3 time points: (1) 3 weeks prior to therapy, (2) 1 week prior to therapy, and (3) within 2 weeks after completion of therapy. Two assessments were performed prior to the CIMT intervention to reduce the impact of improvements caused by practice effects, particularly in our kinematic tasks.
Clinical Outcome Measures
All clinical assessments were performed by a single physical therapist blinded to the patients’ performance during therapy. The primary clinical outcome measures were the ARAT 37 and the FM-UE scale, 38 which have been shown to have good reliability, validity, and responsiveness to motor change in patients with chronic stroke.23,39-41
The ARAT is an instrument that tests arm function and consists of 19 items in 4 domains: grasp, grip, pinch, and gross movement. Each domain contains items arranged into hierarchical order of difficulty such that success at the most difficult item of a specific subclass assumes success for all items lower in the hierarchy of the same class. Each item is scored on a 4-point ordinal scale (0 = cannot perform, 1 = performs test partially, 2 = completes test but takes abnormally long time or has great difficulty, and 3 = performs test normally), with a maximum score of 57. The ARAT is a functional measure with limited ability to discriminate between “normal” movements and the use of compensatory strategies. 10
Arm impairment was assessed using the FM-UE. The FM-UE is scored using a 3-point ordinal scale (0 = cannot perform, 1 = can perform partially, 2 = can perform fully) on 22 items in 4 sections: arm, wrist, hand, and coordination, for a maximum score of 66. This test specifies that all limb subcomponents move in a qualitatively normal manner for a normal performance score to be given. We further subdivided the FM-UE into proximal (first 18 items, maximum score 36), wrist (next 5 items, maximum score 10), hand (next 7 items, maximum score 14), and coordination (last 3 items, maximum score 6).
Kinematics: Arm Reaching Task
Participants moved a cursor by making reaching movements over a glass-surface table (Figure 1). Hand position, calibrated to the position of the fingertip, was monitored using a Flock of Birds (Ascension Technology, Burlington, VT) magnetic movement recording system at a frequency of 120 Hz. The experimental computer converted this information online into hand, elbow, and shoulder positions using custom routines in RealBasic (Real Software, Austin, TX). The computer used real-time hand position information to control the visual display and to provide visual feedback.
The target set consisted of 8 radially arrayed circles with a 1-cm radius, 45° apart, 8 cm from a center start circle. Each trial began after the participant held the cursor inside the start circle for 750 ms. Participants were instructed to make straight, out-and-back movements with a sharp reversal within the target, when they were ready to move after the target appeared. To ensure that movements were made quickly and to ensure consistency between trials and sessions, the black cursor froze at its position at 200 ms, and the reversal point was indicated by a white square. 42 This time requirement also allowed us to focus on deficits in patients’ feed-forward control by minimizing online corrections. Participants were given 1 or 2 practice runs of 88 movements for each arm to become familiar with the task. They completed 2 experimental runs, each comprising 11 cycles of 8 targets presented in random order, for each arm.
Kinematics: Wrist Pointing Task
Participants sat in a chair with their forearm placed in a rigid splint that maintained the elbow at a 90° angle and the forearm midway between pronation and supination. The participant’s hand was lightly taped in a fist, and a 1.5-cm spherical reflective marker was attached over the index finger’s first interphalangeal joint. The hand was hidden from view. Participants were instructed to make pointing movements through combinations of abduction-adduction and flexion-extension movements around the wrist, so as to point the marker at targets projected onto a vertical computer screen. The position of the marker was monitored using a Qualysis ProReflex video camera (model MCU 240; Qualisys, Gothenburg, Sweden) equipped with an infrared strobe coupled to a video digitizer, which recorded the marker’s position in the vertical plane at a frequency of 100 Hz.
The target set for the wrist task consisted of 4 radially arrayed circles, separated by 90°, at a distance, which required a 2-cm movement of the infrared marker. Similarly to the arm reaching task, participants were instructed to make out and back movements, placing both the cursor, which froze after 100 ms, and a white reversal square in the center of the target. They completed 1 familiarization run and 2 experimental runs for each wrist, which consisted of 22 cycles of 4 targets presented in random order.
Analysis of Kinematics
We analyzed hand and wrist position data using custom routines within the IGOR analysis software package (Wavemetrics, Lake Oswego, OR). Position time series were low-pass filtered (Butterworth filter) at 8 Hz for the arm task and 14 Hz for the wrist task and differentiated to yield tangential velocity and acceleration.
The first velocity peak above a threshold (10 cm/s for the arm and 5 cm/s for the wrist) was identified for each trial. These thresholds were chosen to exclude small movements made by some participants who had difficulty stabilizing their hand within the start circle. The start of the movement was defined as either the point at which the velocity crossed 1 cm/s or the first velocity minimum prior to the first velocity peak, whichever was later. The end point of the outward movement was defined as the reversal point—that is, the point where distance from the origin stopped increasing. The movements were further divided into submovements based on their acceleration profiles. The first submovement was defined as the movement up until the first zero crossing of acceleration from negative to positive. 43 Each subsequent submovement was defined as the movement between zero crossings of acceleration from negative to positive.
We calculated the following variables for the outward movement: (1) movement time; (2) peak velocity; (3) absolute initial directional error, which is the angle between the vector from start position to target and the vector from start position to cursor position at 120 ms after movement start; (4) path curvature, the unsigned area between hand path and the shortest possible path (a straight line joining the start and end points of the movement), divided by the area of a semicircle with the shortest possible path as its diameter; (5) systematic error, the distance between the average end-point position and target center; (6) end-point variance, the determinant of the covariance matrix of the end points corrected for the number of observations and averaged across targets; and (7) number of submovements.
The following kinds of trials were excluded: anticipatory movements, movements that did not reach 30% of the distance to the target, movements without reversals, and spatial outliers (in which the movement direction was >90° from the target direction). Anticipatory movements were defined as those with reaction times less than 200 ms, based on the fastest reaction times seen in a similar task when healthy participants were instructed to move “as soon as possible.” 44
Statistical Analysis
All statistical analyses were performed on average group data. One-tailed, paired t tests were performed using Excel (Microsoft, Redmond, WA) on the differences between the change from session 1 to 2 (Δ1) and the change from session 2 to 3 (Δ2). We chose to compare the changes in values in order to minimize the possible confound of task practice on our measures across sessions and chose 1-tailed tests because our hypotheses were based on improvements in our clinical and kinematic variables.
We performed post hoc power analyses to assess the false-negative rate for each of our comparisons. Meaningful effect size was chosen as 10% of the maximum possible score for the clinical measures.23,41 The study was powered at 0.83 for ARAT, 0.86 for FM total, 0.78 for FM arm, and 0.52 for FM wrist. For the kinematic measures, we used 50% of the patients’ mean deficit (the difference between the patients’ affected side and values obtained for elderly controls in an ongoing study). The magnitude of improvement in our kinematic tasks that would be associated with a clinically meaningful reduction in impairment is not known, but we presumed that significant recovery would be accompanied by a larger percentage improvement in the more sensitive 45 and responsive 46 kinematic measures compared with the clinical scales. For the arm kinematic measures, the study was powered at 0.55 for path curvature, 0.65 for initial directional error, 0.48 for systematic error, 0.45 for end-point variance, and 0.48 for number of submovements. For wrist movements, the study was powered at 0.51 for path curvature, 0.99 for initial directional error, 0.88 for systematic error, 0.96 for end-point variance, and 0.55 for number of submovements.
Results
A total of 10 patients with chronic stroke participated in the study, but 1 patient was excluded from the analysis because he did not meet inclusion criteria. Table 1 summarizes patient demographics and stroke location. The mean age of patients was 70 years, and mean time elapsed since stroke was 34.3 months (range = 10-162 months). Of the 9 patients, 7 had ischemic strokes, 5 involved the dominant hemisphere, and lesions included both cortical and subcortical areas. For the study intervention, patients spent on average 2.45 hours practicing activities (range = 1.84-2.89 hours) with the therapist each day. By self-report, they spent an average of 61 min/d (range = 0-251 min/d) wearing the mitt outside of therapy. However, 5 of the patients did not wear the mitt at all outside of therapy because of safety concerns. No adverse events were reported during the study.
Patient Demographics and Clinical Characteristics
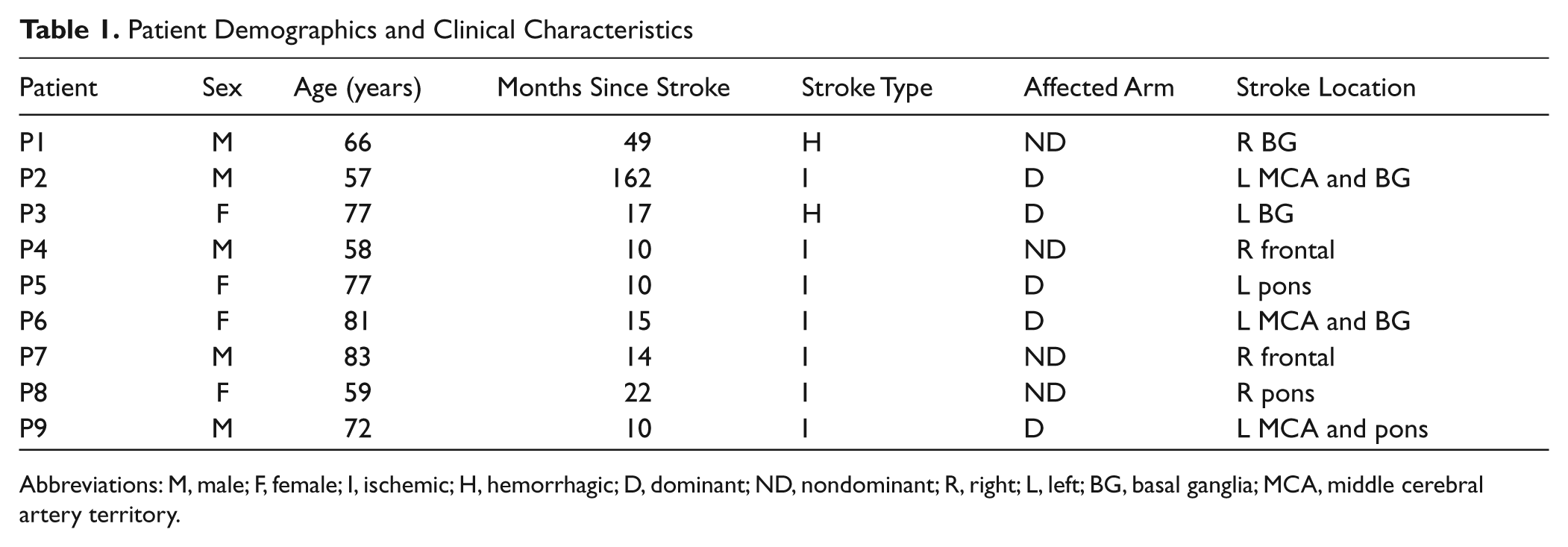
Abbreviations: M, male; F, female; I, ischemic; H, hemorrhagic; D, dominant; ND, nondominant; R, right; L, left; BG, basal ganglia; MCA, middle cerebral artery territory.
Clinical Outcomes
At baseline, patients were moderately affected, with a mean ARAT score of 31.3 and mean total FM-UE score of 44.3 (Table 2). Clinical outcome measures are summarized in Figure 2. Arm function as measured by the ARAT improved significantly more after CIMT than between the 2 pre-CIMT sessions (−0.8 vs 5.4, P = .004). Δ2 was also significantly larger than Δ1 for the total FM-UE (−0.9 vs 4.1, P = .018), FM wrist score (-0.2 vs 0.9, P = .027), and FM coordination score (−0.2 vs 0.9, P = .014) but not for the FM arm (−0.4 vs 1.4, P = .087) or FM hand (−0.1 vs 0.9, P = .148).
Patient Baseline Clinical Assessments
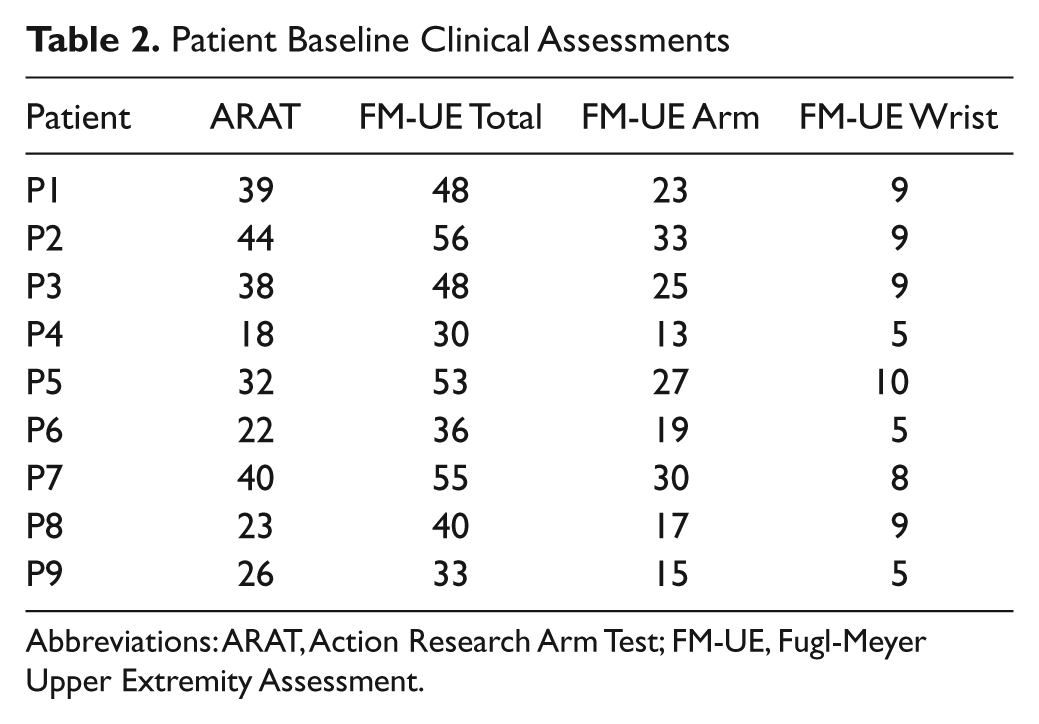
Abbreviations: ARAT, Action Research Arm Test; FM-UE, Fugl-Meyer Upper Extremity Assessment.
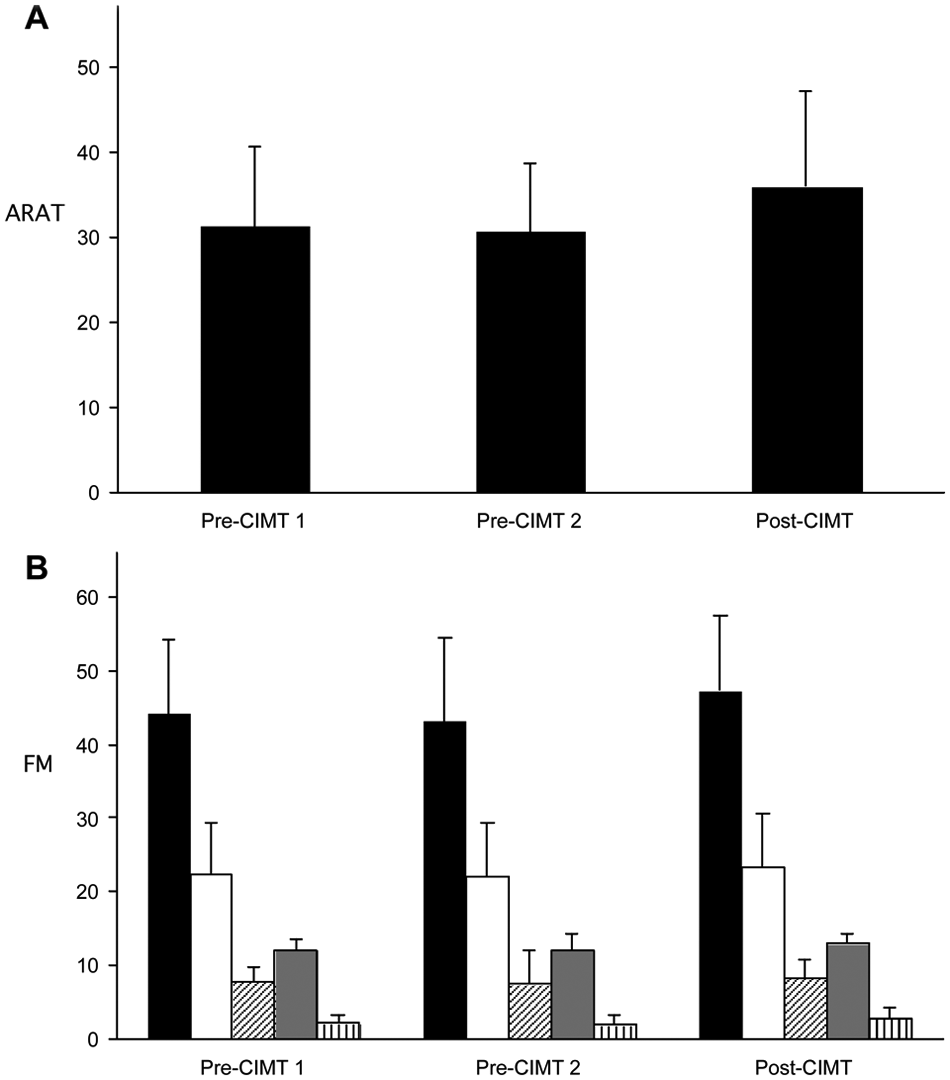
Mean scores on the (A) ARAT and (B) FM-UE for each session, with error bars representing SD. For (B), total FM-UE (in black) is further subdivided into proximal arm (white), wrist (oblique stripes), hand (gray), and coordination (vertical stripes)
Arm Kinematics
Hand trajectories for the arm reaching task in a healthy control and a patient are shown in Figures 3A to 3C. There was no significant improvement from Δ1 to Δ2 for the percentage of rejected moves, movement times, or peak velocities. Kinematic outcomes are shown in Figure 4. There were no significant improvements from Δ1 and Δ2 for path curvature, initial directional error, systematic error, or variable error.
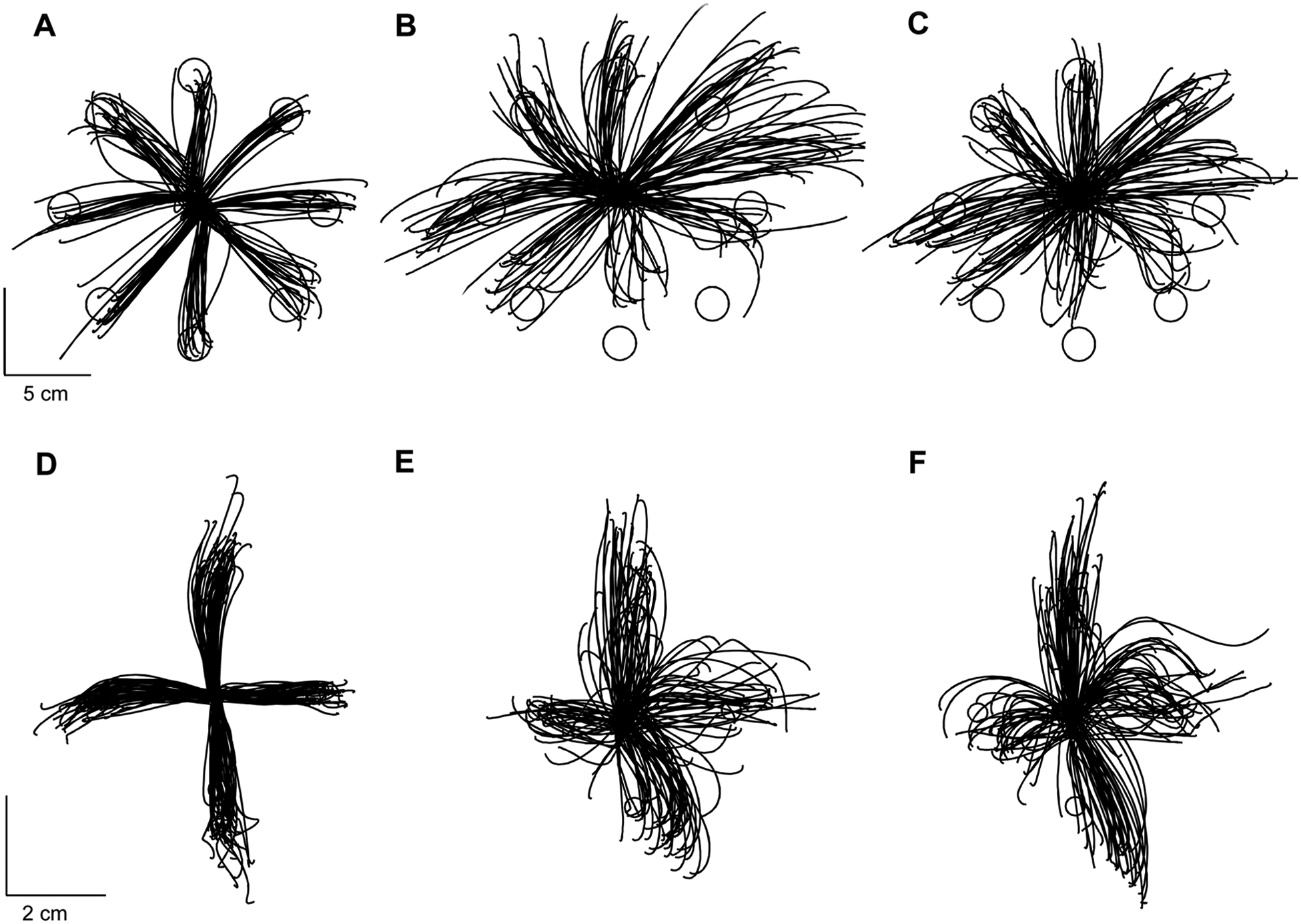
Trajectories for randomly selected participants performing the arm reaching and wrist pointing tasks: (A) control, dominant arm; (B) patient, affected arm, pre-CIMT 2; (C) patient, affected arm, post-CIMT; (D) control subject, dominant wrist; (E) patient, affected wrist, pre-CIMT 2; and (F) patient, affected wrist, post-CIMT 2. Trajectories of healthy controls are presented for illustrative purposes
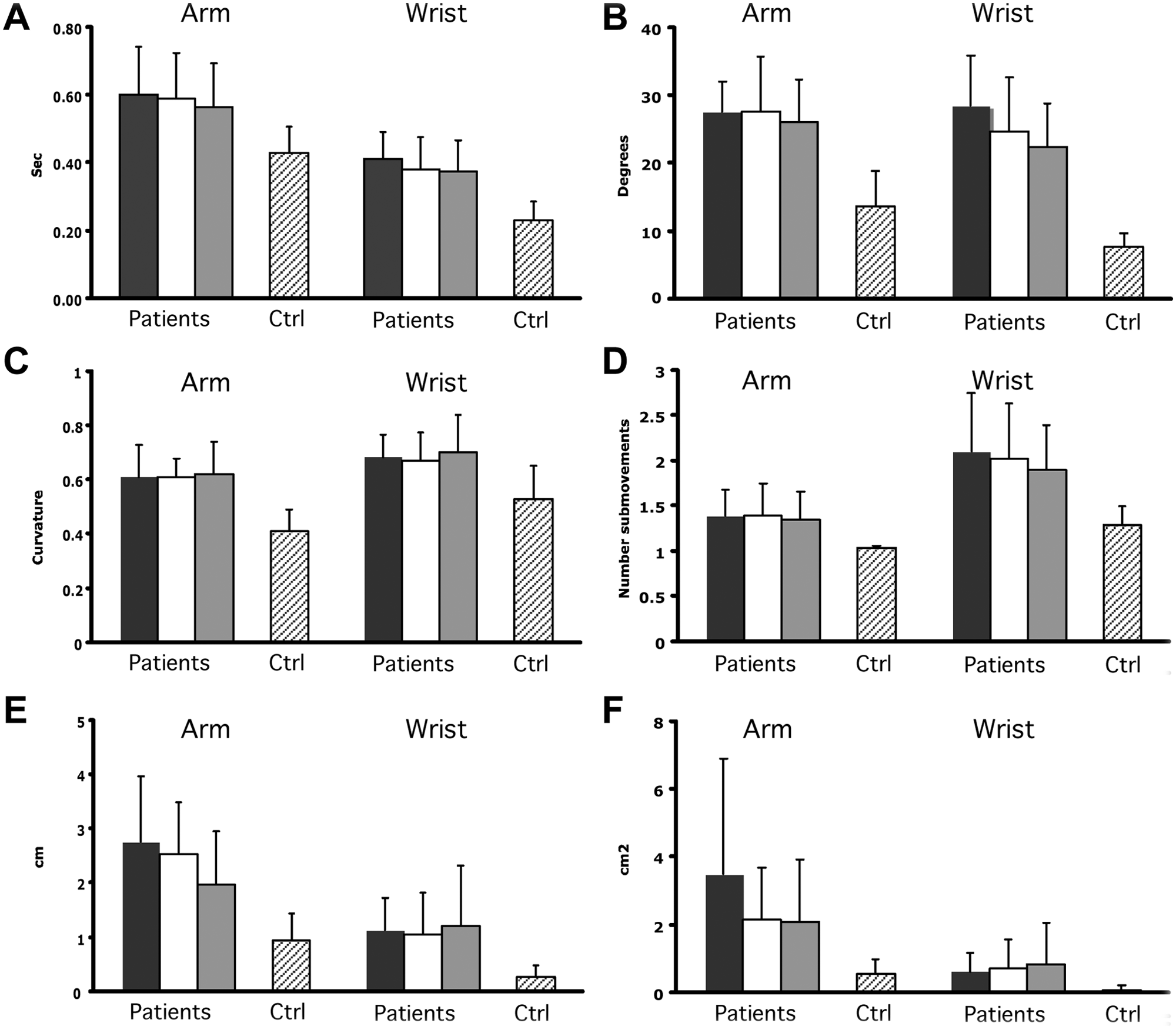
Kinematic outcomes for (A) movement time, (B) initial directional error, (C) path curvature, (D) number of submovements, (E) systematic error, and (F) variable error in the arm and wrist tasks. Scores for each session are shown: 1 (black), 2 (white), and 3 (gray). Performance of elderly controls in a separate study are shown to the right. Values are mean with error bars depicting standard deviation
Wrist Kinematics
Trajectories for the wrist pointing task in a healthy control and patient are shown in Figures 3D to 3F. There were no significant improvements from Δ1 to Δ2 for the percentage of rejected moves, movement times, or peak velocities. There were also no significant improvements from Δ1 to Δ2 for path curvature, initial directional error, systematic error, or variable error in the affected wrist (Figure 4).
Discussion
Improvements in function can result from a reduction in impairment, the use of compensatory strategies at a fixed level of impairment, or a combination of both.10,11,16,47 The objective of this study was to use clinical and kinematic assessments of upper-extremity movements to better understand the contributions of compensation and recovery to the functional improvements seen after CIMT in patients with chronic stroke. We found statistically significant improvements in arm function and a statistically significant but very small reduction in impairment after CIMT. Assuming a 10% change in these scales to be clinically meaningful,23,41 we conclude that the CIMT intervention resulted in an improvement in arm function that was close to reaching clinical relevance (9.5%) but no meaningful improvement in overall arm impairment (6.2%). Our results are consistent with the findings of a recent meta-analysis of modified CIMT. 36
The magnitude of functional arm improvement seen in our study was somewhat smaller compared with those in other studies of modified CIMT protocols in patients with chronic stroke that used similar assessments of arm function and found differences ranging from 7 to 10 in ARAT after CIMT.19,20 These studies used a modified CIMT protocol with shorter sessions of CIMT but over a longer period of time. The modified CIMT protocol in our study was similar to the original CIMT protocol used in the EXCITE trial 4 but with 4 h/d of therapy, rather than 6 h/d, for 10 consecutive weekdays, and our patients wore the mitt outside therapy for only an average of 61 min/d. The optimal dosing for CIMT is still not well established, 17 but it is likely that the patients in our study were relatively underdosed. We should stress, however, that we were interested in the weighting of compensation versus true recovery for a given amount of therapy. It is possible that a more prolonged or more intensive CIMT intervention program would have resulted in greater gains in function accompanied by reduction in impairment, but it is also possible that further gains at the functional level via compensation would not be accompanied by reductions in impairment.
We chose the FM-UE and constrained pointing tasks with the arm and wrist as our measures of arm impairment. The FM-UE is one of the most widely used measures of motor impairment after stroke 23 and has been used as a primary outcome measure to evaluate the effect of upper-extremity rehabilitative techniques. Previous studies of CIMT in patients with chronic stroke have found variable effects on FM-UE scores.5,18-22 Page et al 21 found significant changes in ARAT scores without corresponding changes in FM-UE scores and speculated that their results were a result of the greater reliance of the ARAT on distal upper-extremity function, which may be emphasized more heavily than the proximal arm in activities practiced during CIMT. In our study, we found small improvements in the overall FM-UE score, with increases distributed across all subsections, although some of these were not statistically significant. Therefore, it is unlikely that the more substantial changes in ARAT than in FM-UE scores after CIMT were a result of greater effects on the distal limb.
Detailed movement analysis in nonhuman animals48,49 and humans13,16 has been used to differentiate functional gains resulting from compensation from those indicating recovery. The arm reaching and wrist pointing tasks in this study were designed to minimize compensatory strategies by restricting degrees of freedom available to the patient to accomplish the task. Constrained tasks such as these, although not routinely used in everyday activities, are valuable assays of impairment and motor control of the arm, analogous in our view to the finger individuation index that has been developed for the hand. 29 Healthy individuals make accurate straight planar reaching movements within a few trials when they first encounter the reaching task,30,50 which indicates that it is not a task that needs to be learned—it is easy if baseline motor control is intact.
It is interesting to note that we found a small increase in FM-UE total without significant changes in our kinematic variables, even though both are measures of impairment. The increase in FM-UE may reflect coarse improvements in impairment that are not sufficient to induce improvements in fine motor control of the arm and wrist required for visually guided prehension. Indeed, the magnitude of change in FM-UE is small and not likely to be functionally relevant, as evidenced by studies of robotic rehabilitation that have elicited comparable changes in FM-UE scores without an effect on arm function or activities of daily living. 51 If this interpretation is correct, it implies that CIMT causes functional improvements in parallel with, but unrelated to, smaller reductions in impairment.
One potential objection to the apparent dissociation between function and impairment might be that CIMT resulted in task-specific improvements in motor control that did not generalize to our novel kinematic tasks. It is important to emphasize that we consider our kinematic tests assays for rudimentary baseline motor control rather than specialized tasks per se. Healthy individuals can perform planar reaches and make wrist pointing movements with no need for extended practice because these tasks probe for basic motor control capacities that healthy individuals already have. We consider it highly unlikely that these individuals could recover more normal control in more ecological and challenging everyday tasks but fail to generalize to our more basic kinematic tests. This would be akin to saying that a patient could become better at typing without showing any improvement on a finger individuation index. 52 In the specific case of planar reaching, such a view would imply that patients could show improved control of 3-dimensional arm movements but not of 2-dimensional arm movements. Again, we consider this highly unlikely, especially as it has been shown that when the effects of gravity are removed, patients with stroke greatly increase the range of their 2-dimensional planar movements, 53 which implies that patients find control easier when the gravitational challenge of 3-dimensional movements is removed. Nevertheless, an interesting future direction would be to combine kinematic assessments of constrained and free movements to quantify both impairment and the compensatory mechanisms contributing to functional gains. We also recognize this study’s small sample size and lack of power to detect changes in some of our kinematic variables. With regard to the issue of power, however, it should be emphasized that some measures were adequately powered and that none of these showed improvement. One of the points of this study is to encourage the use of kinematic measures in future larger-scale studies.
Our interpretation of the current data is that CIMT induces task-specific compensatory strategies through practice in the chronic stage of stroke despite an invariant impairment level. CIMT could have a qualitatively different effect if applied very early after stroke if larger reductions in impairment than expected from spontaneous recovery occurred. 54 Then, patients would not resort to compensatory strategies. Although early CIMT did not show a benefit in 1 trial, impairment was not assessed. 55
Our study and others demonstrate the feasibility of using kinematic analysis to obtain more detailed, objective measures of movement patterns and motor performance in studies of novel neurorehabilitative interventions.56-58 Analysis at the kinematic level will provide us with the ability to differentiate between functional gains achieved through compensation versus those achieved through true recovery of motor control. 45 At the current time, conventional therapy has largely focused on teaching compensatory strategies, with a goal of achieving early functional independence. As mentioned above, early focus on compensation may limit long-term recovery.13,14,16 Even in the acute stroke period, patients may learn not to use or explore more normal movements with the affected limb because of habitual reliance on compensatory strategies and thus miss out on a time window of plasticity within which true recovery could be maximized 11 . Detailed kinematic assessments of the kind used here could contribute to a better understanding of the interactions between spontaneous recovery, the development of compensatory behaviors, and rehabilitation and their relative contributions to long-term outcome.16,59
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: The work was supported by the following grants: National Institutes of Health Grant Number K02-NS048099 and the Suellen Jones Saunders Memorial Fund.