
Abstract
Objective. To examine the effects of technology-assisted balance and gait training on reducing falls in patients with Parkinson’s disease (PD). Methods. Eligible subjects were randomly allocated to an experimental group given technology-assisted balance and gait training (BAL, n = 26) and an active control group undertaking strengthening exercises (CON, n = 25). The training in each group lasted for 3 months. The number of fallers and fall rate were used as primary outcomes, and single-leg-stance-time, latency of postural response to perturbation, self-selected gait velocity, and stride length as secondary outcomes. Fall incidence was recorded over 15 months after the baseline assessment (Pre). Other tests were performed at Pre, after 3-month intervention (Post3m), at 3 months (Post6m), and 12 months (Post15m) after treatment completion. Results. Forty-five subjects who completed the 3-month training were included in the data analysis. There were fewer fallers in the BAL than in the CON group at Post3m, Post6m, and Post15m (P < .05). In addition, the BAL group had lower fall rate than the CON group at Post3m and Post6m (incidence rate ratio: 0.111-0.188, P < .05), and marginally so at Post15m (incidence rate ratio: 0.407, P = .057). Compared with the CON subjects, the BAL subjects demonstrated greater reduction in the postural response latency and increase in the stride length against baseline at each assessment interval (P < .05), and marginally more increases of single-leg-stance-time at Post3m (P = .064), Post6m (P = .041) and Post15m (P = .087). Conclusions. Our positive findings provide evidence for the clinical use of technology-assisted balance and gait training in reducing falls in people with PD.
Background
Falls are common in patients with Parkinson’s disease (PD). The incidence is as much as 40% to 70%, 1 which is much higher than the incidence observed in neurologically intact older individuals. 2 Falls are the most problematic feature in patients with PD because they can lead to devastating outcomes such as physical injury and negative psychological effects that could consequently limit patients’ mobility and their performance of daily activities. 3 Fall prevention is therefore an urgent requirement for patients with PD.
A recent Cochrane review suggests that exercise training is the most commonly used intervention for fall prevention in elderly people. 4 Exercise training for fall prevention, including balance or gait training,5,6 Tai Chi exercise, 7 and balance combined with stretch and muscle strength training,8,9 have been used in patients with PD. Studies have reported improvements in postural stability after training such as stability limits and functional reach, 7 single balance tasks such as step up-and-down, 5 generic balance performance as measured by the Berg Balance Scale, 6 spatiotemporal gait characteristics,5,7 and self-perceived balance confidence. 6 However the effect of these training programs on fall reduction is inconsistent. Positive effects on reducing future falls have been reported in studies with balance or gait training and Tai Chi exercises,5 -7 but no effect has been reported for programs that combine balance, muscle strengthening, and stretching exercises.8,9 In addition, the longest follow-up period ranged between 1 month, 6 3 months, 7 and 6 months, 8 and thus whether such treatment is effective in reducing fall incidence beyond 6 months is not known. Technology-assisted equipment has been reported to provide preparatory cues10,11 and augmented feedback10,12 to PD patients that could facilitate their motor learning. 13 We designed a balance and gait training program that was assisted by technological devices and collected information on falls for 15 months, including a 3-month intervention and a 12-month follow-up. We aimed to explore the short- and long-term effects of the technology-assisted balance and gait training program on reducing fall incidence in patients with PD. We hypothesized that the technology-assisted balance and gait training would be effective in reducing fall events both in the short term and in the long term.
Method
Subjects
Subjects were recruited from Hong Kong Parkinson’s Disease Association, a patient self-help group, and the Movement Disorders Clinic of a local hospital. The criteria for inclusion consisted of having a diagnosis of idiopathic PD, 14 being stable after taking anti-Parkinsonian medication, having the ability to walk independently for 10 m, and having a Mini-Mental State Examination (MMSE) score of greater than 23. 15 Patients were excluded if they had motor fluctuations and any disorders that would affect balance and locomotion, such as neurological conditions other than PD, uncompensated cardiovascular disease, visual disturbance, or a recent musculoskeletal disorder in the back or the lower limbs (Figure 1). The eligibility criteria were the same during the whole study period. The study was approved by the ethics committees of the university and the hospital concerned. All patients provided written informed consent according to the Declaration of Helsinki. The present study shared the same subject population with the randomized controlled trial reported recently. 10
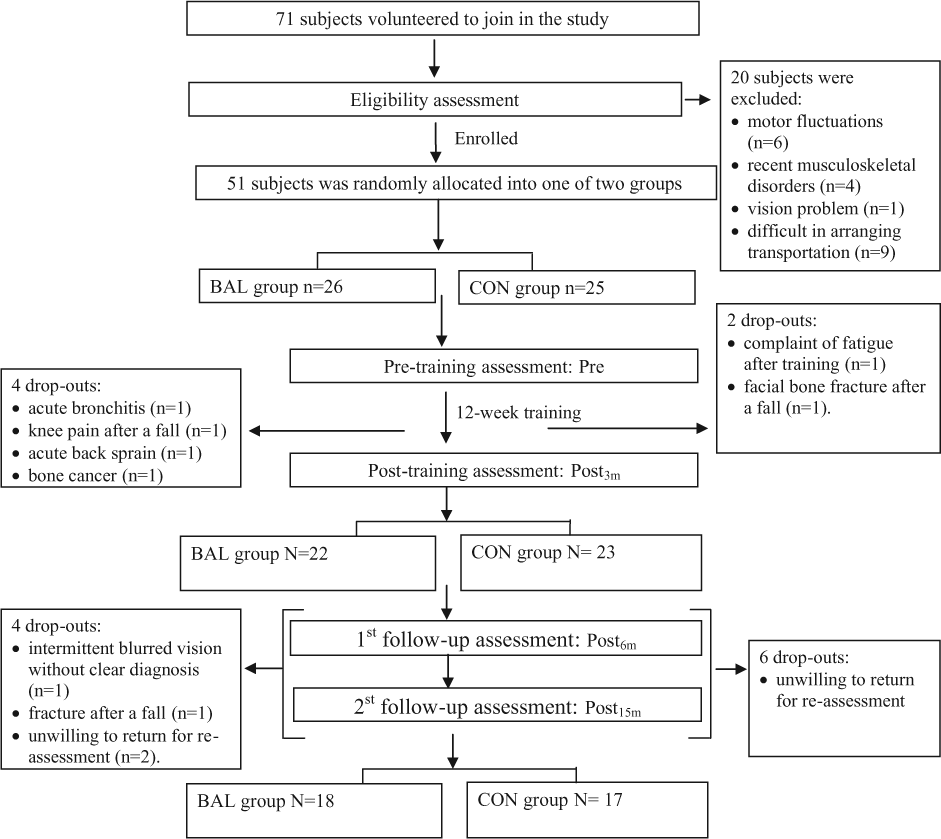
Study design and flow of participants at each stage of the study.
Sample Size Calculation
Based on the findings of Li et al 7 on fall prevention in people with PD, a sample size of 49 was required to detect a reduction of 53% in fall incidence with an assumption of 80% power. We recruited 51 subjects in this study. They were randomly assigned (by drawing lots) to 1 of 2 groups: the experimental group given technology-assisted balance and gait training (BAL, n = 26) or the active control group (CON, n = 25).
Randomization was done by a researcher who was not involved in any other aspect of the study. The result of randomization was given to the research assistant who assigned subjects into their respective training group and who conducted the training. The group assignment was blinded to the tester but not to the subjects. To minimize the possible difference in placebo effects, we used the same manpower allocation, adopted technology-assisted training and equivalent training duration for both BAL and CON groups.
Outcomes
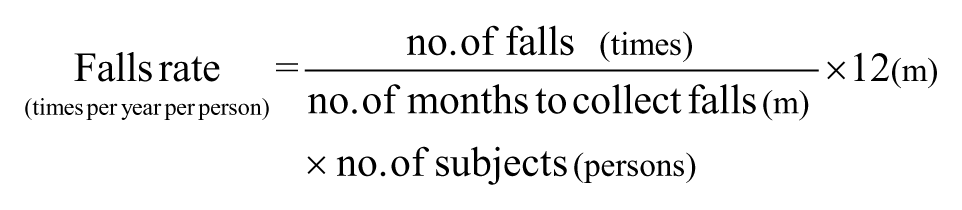
The primary outcomes were the number of fallers, the fall rate, and the time to first fall. Information on the number of falls during the 12 months before recruitment was obtained by patient interview at the baseline assessment. Following the baseline assessment, all the subjects were contacted by phone monthly to record any fall occurrences until the end of the study period or dropout from the study during the 12-week intervention period. A fall is defined as an event during which a subject comes to rest on the ground or at some lower level, not as the result of a major intrinsic event, for example, a syncope, stroke or seizure, or overwhelming hazard. 16 In accordance with the definition of fallers in previous studies related to falls,1,4 persons were classified as fallers if they had one or more falls within their respective follow-up period. The fall rate, indicating the number of falls per year per person, was calculated as the number of falls recorded divided by the number of months spent collecting information on falls and the number of subjects, multiplied by 12. 4
The secondary outcome measures were single-leg-stance (SLS) time17,18 and latency of compensatory postural response to external perturbation with the motor control test (MCT) to reflect the subjects’ balance performance, 19 and self-selected gait velocity and stride length to measure their gait performance. In the SLS test, the subjects were instructed to stand on their more impaired/nondominant leg for as long as possible or until 30 seconds were reached. Reduced SLS time has been found to associate with falls in PD patients. 19 The MCT test was performed using the EquiTest Computerized Dynamic Posturography unit (NeuroCom International Inc, Clackamas, OR) that consists of dual dynamic force plates. 19 The force plates generated a forward translation to move the subjects’ body center of mass in a backward direction relative to their base of support. Backward direction was chosen to simulate the clinical pull test and the postural response to retropulsion because it was more impaired in PD patients. 20 Subjects were instructed to stand on the force plates and to maintain a stable upright posture throughout the test. In response to the translation of the force plates, one compensatory postural response was triggered. The latency of compensatory postural response was the time taken from the onset of force plate translation to the initiation of displacement of the center-of-pressure trajectory detected by the Equitest system. For both the SLS and MCT tests, there was a practice trial followed by 2 test trials, and the mean values were used for data analysis. In the walking test, the subjects were instructed to walk on a 5-m instrumented and computerized GAITRite walkway (CIR Systems Inc, Havertown, PA). There was a practice trial and 3 test trials, and the mean values were used for data analysis. All subjects were tested at the Gait and Balance Laboratory of The Hong Kong Polytechnic University and during their “on” medication state. With standard procedures, all the tests were taken at baseline before the intervention (Pre), immediately after the 3-month treatment (Post3m), at the 3-month follow-up (Post6m) and at the 12-month follow-up (Post15m).
In addition to the outcome measures, demographic data were recorded at the baseline assessment (Pre). These comprised gender, age, body mass index, duration of PD, level of physical activity as determined by a metabolic equivalent (MET) questionnaire, 21 severity and disability level of PD as determined by a modified Hoehn and Yahr (HY) staging score 22 and the Unified Parkinson’s Disease Rating Scale–motor score (UPDRS-III), 23 respectively, and cognitive status as quantified by the MMSE score. 15 The subjects’ anti-Parkinsonian medications were recorded at each assessment interval. The daily levodopa equivalent dose (LED) was calculated according to the LED formulas that were reported previously. 24
Intervention
The patients in both groups (BAL and CON) receiving training for 12 weeks, with 2 phases of 4-week physiotherapist-supervised laboratory-based training at a frequency of 3 sessions per week, separated by 4 weeks of self-supervised home-based training at a frequency of 5 sessions per week. During the laboratory-based training phases, the intervention for each group was conducted by a physiotherapist and a research assistant.
The detail information about the intervention has been presented in our previous article, 10 and in the appendix provided in the Supplementary Material available at http://nnr.sagepub.com/content/by/supplemental-data. In brief, during laboratory-based training phase, balance and gait training for the BAL group consisted of 3 exercise components: volitional stepping and leaning in a standing position, and walking under external perturbation. These exercises aimed to enhance the subjects’ postural control to cope with self-induced and externally triggered perturbations. A computerized dancing system (KSD Technology Co Ltd, Shenzhen, China) was used to perform stepping and leaning exercises with a focus on movement speed and accuracy. The system consisted of dancing software, a computer, a pressure-sensitive carpet, and 2 light-sensitive rods. The subjects stood on the carpet with the light-sensitive rods positioned in the right-forward and left-forward directions and at the longest distance that they could reach without falling. The subjects were instructed to step on a designated area of the carpet or lean their trunk to reach the rod in response to visual cues. A Smart-EquiTest Balance Master (NeuroCom International Inc, Clackamas, NJ) was used to train volitional stepping that focused on speed and amplitude. The training was carried out on a 45 cm × 150 cm pressure-sensitive platform and under the guidance of visual cues (ie, yellow and red cursors) indicating the preset amplitude and the time to step. The subjects were instructed to take a large step rapidly and to stay in the stride–stance position stably in response to a yellow cursor, and then to step back to their original standing position on the appearance of a red cursor. Repetitive stepping was performed in response to these cursors. The subjects had to practice stepping in 4 directions (forward, backward, left, and right) and diagonal stepping to right-forward and left-forward directions, and stepping over an obstacle on progression. Walking under external perturbation was performed on a treadmill and over ground. External perturbation was provided through the sudden start and stop of the treadmill belt or manually by a physiotherapist during walking. The subjects were instructed to take large steps with good stability on the sudden start and stop of the treadmill belt or in response to the manual perturbation during walking. 11 Feedback on the performance accuracy, speed and amplitude was given as a score for the dancing system and the Smart-EquiTest Balance Master, and verbal feedback was given on the treadmill training. The CON group received strength training program that focused on increasing muscle strength of the lower extremities.25 -27 Dynamometers and leg-press machines were used to train the strength of the hip and knee muscles at 60% of one repetition maximum, with 2 sets of 15 repetitions performed in each session. In addition, the subjects performed strengthening exercises with a rowing machine and a cuff weight. The whole laboratory-based training session lasted for 60 minutes in both groups.
During the 4-week home-based training, the training emphases are the same as the laboratory-based phase in each group, postural control in the BAL group and muscle strength in CON group. Home-based training aimed to encourage subjects to practice their learnt exercises and/or postural control strategies during their daily activities and to form an exercise habit. The subjects in the BAL group practised fall-prone activities related to self-induced perturbation, including sit-to-stand and walking and turning in four directions, with an emphasis on movement speed, amplitude and stability. The subjects in CON group performed stepping onto and off a curb and walking training with a cuff weight strapped to their bilateral ankles. Each of the home-based training sessions lasted for 20 minutes.
The durations of each session of laboratory- and home-based training in the BAL group were the same as those of the CON group respectively. Treatment time/session during laboratory- and home-based training phases was recorded by physiotherapists and subjects respectively, for the calculation of exercise compliance.
Statistical Analysis
The data were analyzed with the Statistical Package for Social Sciences (SPSS, version 20.0). Based on the intent-to-treat principle, subjects who completed the postintervention assessment (Post3m) were included in the data analysis. The last observation of all outcome measures except for falls data was carried forward for subjects who dropped out during the follow-up period. Falls information was recorded by monthly phone follow-up throughout the study period for all subjects, including the dropout subjects who did not show up for the follow-up assessments. In terms of the demographic variables, independent t-tests and χ2 tests were used to examine group differences in the quantitative and nominal variables, respectively.
The ratio of fallers to nonfallers was compared using a Pearson χ2 test. For the fall rate after the baseline assessment, a negative binomial regression model was used to determine the between-group difference at each assessment interval. The fall risk ratio and fall incidence rate ratios with the corresponding 95% confidence intervals were calculated. The time to first fall since treatment commencement was analyzed by Kaplan-Meier log rank χ2 test. For balance and gait performance, the mean changes from the baseline values between the BAL and CON groups at each assessment interval were compared using multivariate analysis of variance. The significance level was set at P < .05.
Results
The recruitment was commenced in April 2009 and ended in December 2010 since very few subjects were enrolled then. All assessments were completed at February 2012. There was no difference in the subjects’ characteristics at baseline between the BAL and the CON groups (Table 1). There was comparable daily levodopa equivalent dose at baseline and no difference in the change of dosage at each assessment interval between the BAL and the CON groups (Table 1). The exercise compliance was also comparable between BAL and CON group. During the 3-month intervention period, 6 subjects (12%) dropped out from the study (Figure 1). During the 12-month follow-up period, 10 subjects were unwilling to return for re-assessment, but provided their fall information through the monthly phone follow-up. On the basis of the intent-to-treat rule, the 45 subjects who completed the postintervention assessment (Post3m) were included in the data analysis. There was no group difference between the dropouts and non-dropouts in terms of the subjects’ characteristics, and baseline outcome measures, with the exception that the dropouts had a lower baseline physical activity level (MET = 3.0 ± 1.1) than the non-dropouts (MET = 3.4 ± 0.3, P < .05). No serious harm such as falls and any unintended harms happened during exercise training in both groups.
Subject Characteristics, Medication, and Exercise Compliance Between BAL and CON Groups.
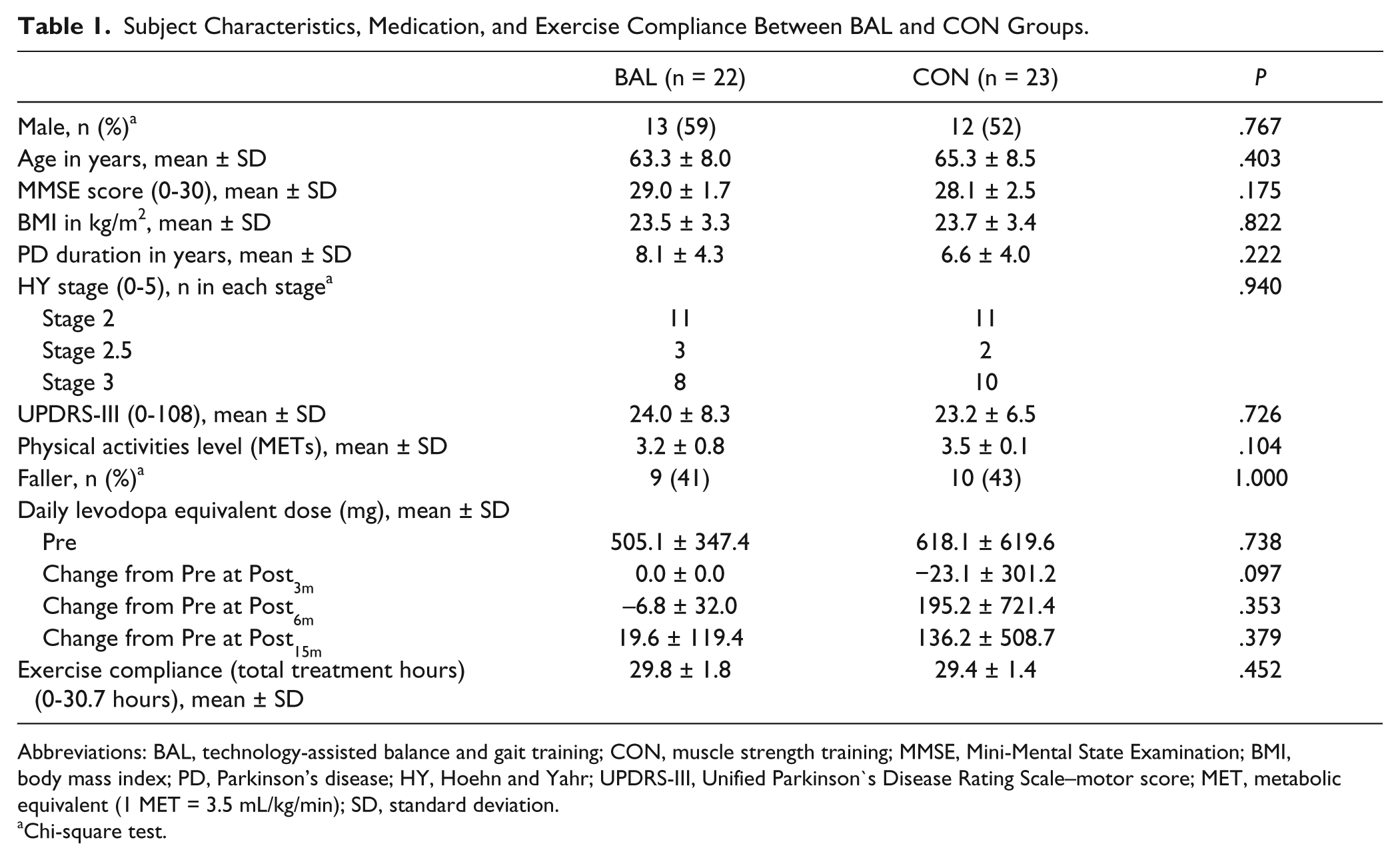
Abbreviations: BAL, technology-assisted balance and gait training; CON, muscle strength training; MMSE, Mini-Mental State Examination; BMI, body mass index; PD, Parkinson’s disease; HY, Hoehn and Yahr; UPDRS-III, Unified Parkinson’s Disease Rating Scale–motor score; MET, metabolic equivalent (1 MET = 3.5 mL/kg/min); SD, standard deviation.
Chi-square test.
Falls
The information on falls was recorded monthly over a period of 12 months after the baseline assessment (Pre). The fall data over 3, 6, and 15 months after treatment commencement were presented, along with the balance and gait outcomes measured at the same intervals (Post3m, Post6m, and Post15m).
Of the 45 subjects, 9 subjects in the BAL group and 10 in the CON group reported falling in the 12 months prior to recruitment (Pre12m). There was no significant between-group difference in the ratio of fallers and nonfallers at Pre12m (risk ratio [RR] = 0.941). However, there were significantly fewer fallers in the BAL than the CON group during study period (RR = 0.190, 0.285, and 0.483, respectively, at Post3m, Post6m, and Post15m, P < .05, Table 2).
Comparisons of Training Effects on Fall Reduction Between BAL and CON Groups.
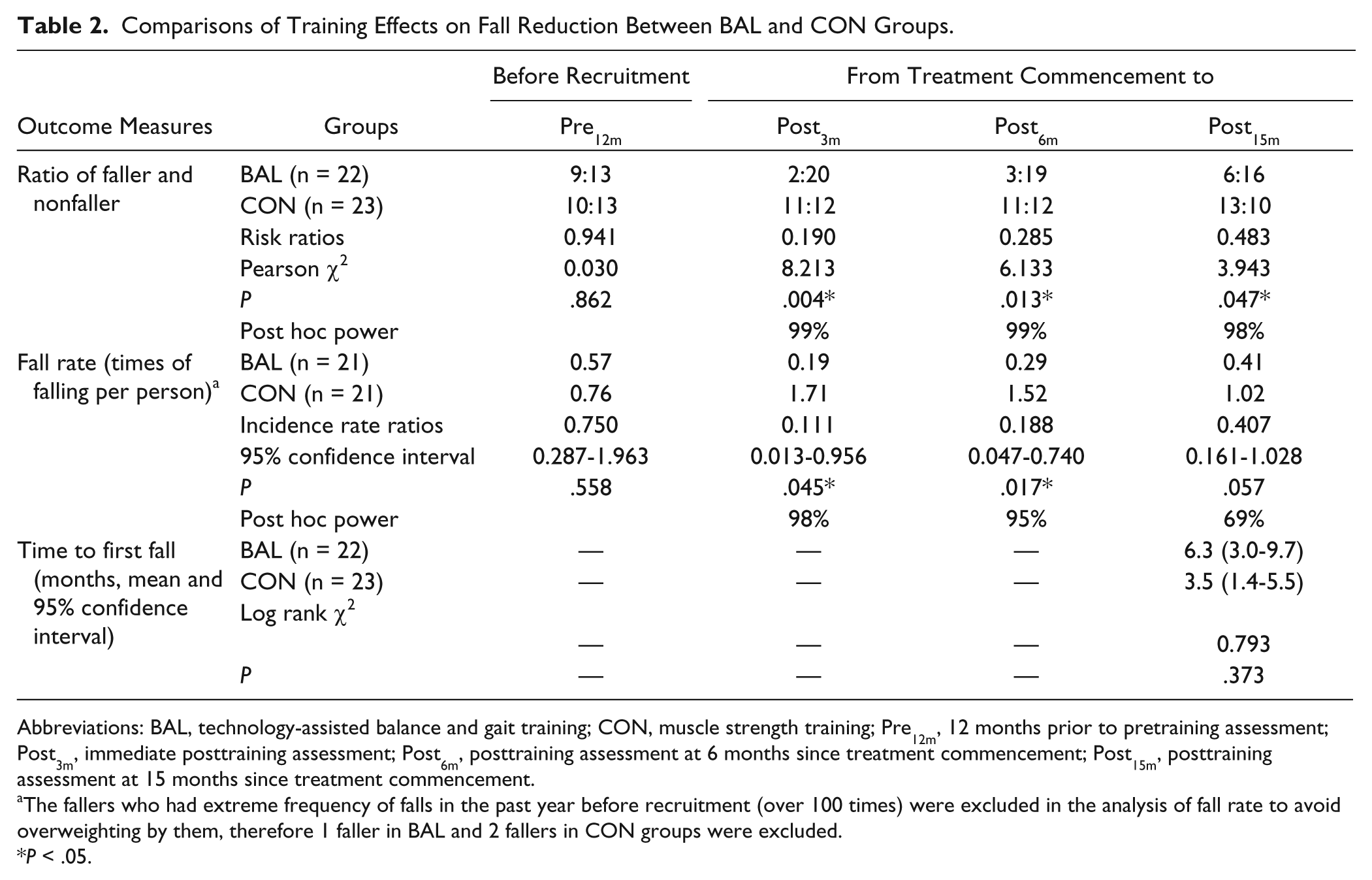
Abbreviations: BAL, technology-assisted balance and gait training; CON, muscle strength training; Pre12m, 12 months prior to pretraining assessment; Post3m, immediate posttraining assessment; Post6m, posttraining assessment at 6 months since treatment commencement; Post15m, posttraining assessment at 15 months since treatment commencement.
The fallers who had extreme frequency of falls in the past year before recruitment (over 100 times) were excluded in the analysis of fall rate to avoid overweighting by them, therefore 1 faller in BAL and 2 fallers in CON groups were excluded.
P < .05.
With respect to the fall rate, 3 self-reported fallers who had fallen over 100 times at Pre12m were not included in the fall rate calculation to avoid overweighting due to the extreme frequency of their falls. 28 Other fallers experienced between 1 and 3 falls in both groups. The fall rate was 0.57 and 0.76 incidences of falling per person per year in the BAL and the CON groups, respectively, at Pre12m, and no between-group difference was detected. After the commencement of treatment, the fall rate decreased in the BAL group but increased in the CON group. Subsequently, the BAL group had a significantly lower fall rate than the CON group at Post3m and Post6m (incidence rate ratios [IRRs] = 0.111-0.188, P < .05), and a marginally lower rate at Post15m (IRR = 0.407, P = .057). Of the 3 fallers with extreme falls, the BAL subject with 2555 falls at Pre12m showed a decreased fall incidence of 735 times at Post15m, and the CON subject with 104 falls at Pre12m showed a decreased fall incidence of 19 times, but another CON subject with 260 falls at Pre12m had an increased fall incidence of 1536 times at Post15m.
During the 15-month follow-up, the first falls occurred earlier in the CON group than the EXP group (CON, 3.5 months; EXP, 6.3 months since treatment commencement). However, the difference did not reach a significant level (Table 2).
Secondary Outcome Measures
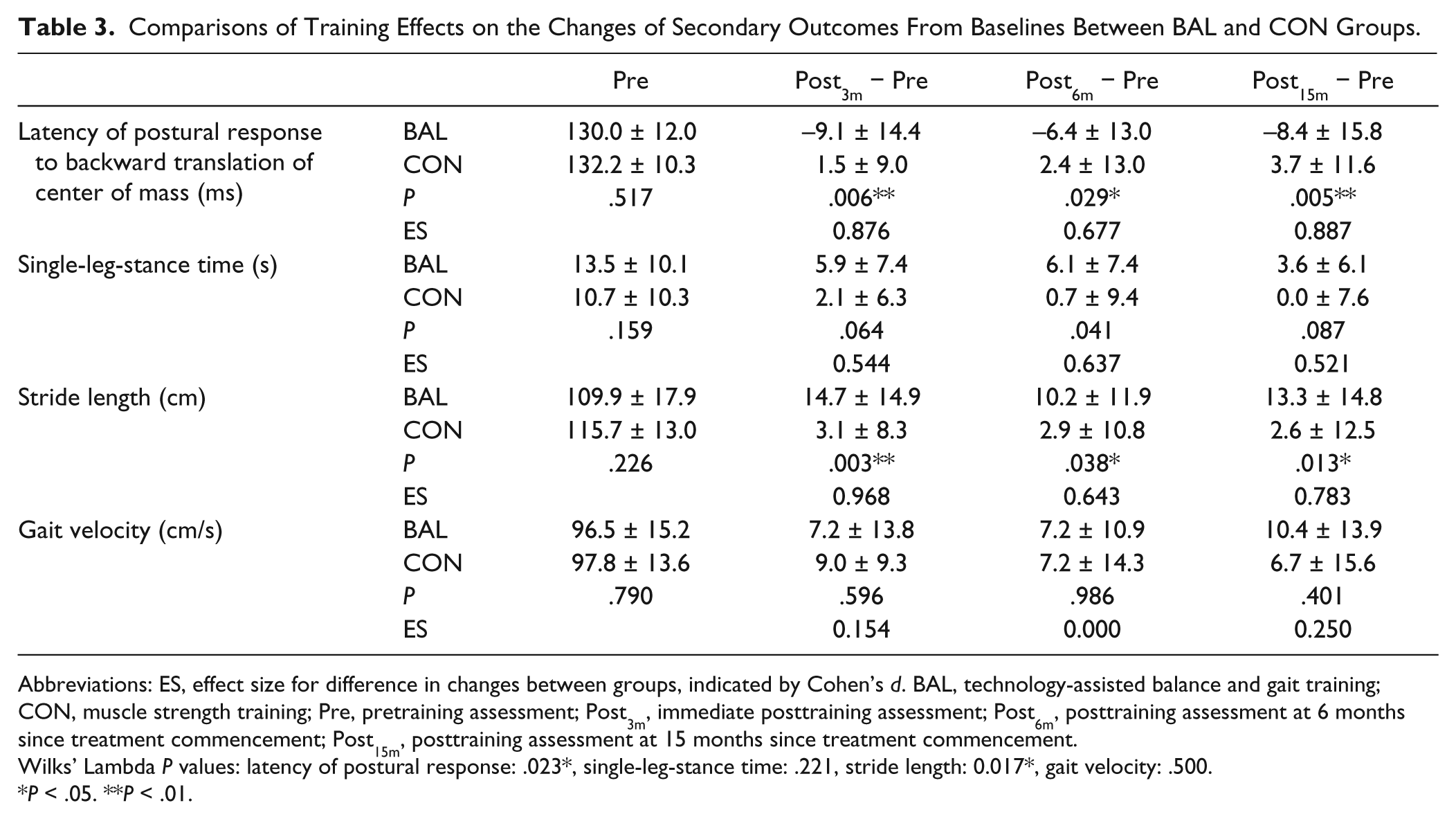
There was no significant between-group difference at baseline in balance and gait performance (Table 3). However, significant between-group differences in changes from the baseline of latency of compensatory postural response to the forward translation of the force plate and stride length were found at each postintervention assessment interval (P < .05). The BAL group showed a greater reduction in the latency of postural response and a more significant increase in stride length than the CON group. Similarly, the BAL group had greater increases in SLS time from baseline than the CON group. The differences were marginally significant at all posttreatment intervals (P = .041-.087). Both subject groups significantly increased their gait velocity after training (BAL by 7.5% to 10.7%, CON by 6.8% to 9.2%, P < .05) but no between-group difference was found in the change of gait velocity at any assessment interval (Table 3).
Comparisons of Training Effects on the Changes of Secondary Outcomes From Baselines Between BAL and CON Groups.
Abbreviations: ES, effect size for difference in changes between groups, indicated by Cohen’s d. BAL, technology-assisted balance and gait training; CON, muscle strength training; Pre, pretraining assessment; Post3m, immediate posttraining assessment; Post6m, posttraining assessment at 6 months since treatment commencement; Post15m, posttraining assessment at 15 months since treatment commencement.
Wilks’ Lambda P values: latency of postural response: .023*, single-leg-stance time: .221, stride length: 0.017*, gait velocity: .500.
P < .05. **P < .01.
Discussion
To the best of our knowledge, this is the first study to show the positive effect of balance and gait training on the reduction of falls in PD patients over a period of 15 months. Balance and Tai Chi training have been reported to significantly reduced the fall rate6,7 and number of fallers 7 at 1-month 6 and 3-month 7 postintervention follow-up. For a progressive disease like PD, the effect of therapy over a longer follow-up period is important. We found that there were significantly fewer fallers in the BAL group up to 15 months after treatment commencement. BAL subjects had a significantly lower fall rate at the Post6m and a marginal reduction in fall rate at Post15m. In addition, balance training appeared to delay the first fall of patients with PD by 3 months when compared with strength training.
Patients with PD have been found to have impaired postural control, including stability limit, 29 anticipatory postural control,30,31 and response to perturbation.20,32 These impairments lead to falls due to self-induced perturbation (eg, when the body leans too far from the base of support during walking or standing, an improperly placed step during walking or gait freezing) 2 and falls that are externally triggered by trips and slips or being pushed or pulled.2,33 The training protocol for the BAL subjects thus focused on enhancing the appropriate shift of body weight through leaning the trunk and increasing the speed and amplitude of volitional stepping in different directions.6,7 In addition, a treadmill was used to enhance foot placement and step length during walking, and speed and amplitude of steps in response to external perturbation. 5 The incorporation of technology-assisted devices such as a dancing mat, balance master, and treadmill into the training protocol provided preparatory cues to enhance the subjects’ attention levels11,34 and to encourage intensive practice to facilitate the motor learning of gait and balance control. 35 PD patients have been found to respond positively to rewards, 36 so the immediate feedback given by the technology-assisted devices after each set of training acted as a reward to motivate the subjects to comply with the training. 12 Esculier et al 12 only used computerized game in their training protocol, whereas we added home-based training to enable patients to transfer their learnt postural control strategies to daily functions. During the home-based training, the subjects could have applied their learnt postural control strategies to perform fall-prone activities such as stepping, walking and reaching.2,33 The ability to perform the fall-prone activities safely suggests that patients’ balance performance and balance confidence could have improved and hence reduce their fall risk. 10 The present study found that the BAL subjects outperformed the CON subjects in terms of the latency of compensatory postural response to perturbation and SLS time over a period of 12 months. A shorter latency of postural response to perturbation results in more timely postural responses to externally induced hits, bumps, trips, or slips.2,34 A longer support-leg standing time may allow patients more time to choose the appropriate postural strategies to maintain an upright posture during self-induced or externally triggered destabilizing tasks. The BAL subjects also increased their stride length significantly more than the CON subjects at treatment completion (Post3m), and the gains were maintained for 12 months after the treatment ended (Post15m). Reduced stride length has been consistently found among individuals with PD, and is a common and debilitating gait problem that may contribute to an increase in the fall risk. 37 It is interesting to note that only the BAL subjects increased their stride length up to 12 months beyond treatment completion. A longer stride length and a faster gait velocity could have increased subjects’ base of support and center-of-mass velocity respectively. Hence these could improve their dynamic postural stability during walking. 38 The enhancement of self-induced and externally triggered postural stability during standing and walking may prevent PD patients from losing their balance and decrease their propensity to fall for a period of up to 12 months after treatment completion. Strength training in the active control group increased gait velocity 27 but had no effect on fall reduction. Since motor learning is context specific, the increase of muscle strength may not have translated to better postural control. 39 Our findings that balance and gait training, rather than strength training, reduce falls in PD patients concur with a recent meta-analytical review of fall prevention programs in elderly people that concluded that only balance training, but not strength training, significantly reduced fall rates. 4
Since the treadmill and balance master are available in most rehabilitation departments, and the dancing mat can be purchased at a low cost, the BAL training protocol can be implemented in the clinic. The combined 12-week laboratory- and home-based training could use less resource than 12-week training in the clinic. Further studies are needed to compare the cost-effectiveness between these 2 modes of training for PD patients.
This study has several limitations. First, the sample size and statistical power were not adequate to detect group differences in the fall rate at Post15m. Second, there was a possible placebo effect since subjects were not blinded to group assignment. We tried to minimize this confounding factor by using technology-assisted training, same manpower allocation and training duration for both BAL and CON groups. Further study that includes a group with placebo control intervention (ie, an intervention that has not been found to reduce falls such as hand dexterity training) could examine a real placebo effect. Third, all of the subjects were community dwelling people with a mild to moderate disease level. Therefore, the results cannot be generalized to patients with advanced-stage PD or those who have been institutionalized. Fourth, we used monthly phone follow-up registration of fall incidence instead of using a fall diary because most of the subjects did not have education beyond the elementary level and some were even illiterate. To minimize the recall bias, we excluded those who had cognitive impairments (MMSE score ≤23). 15 Fifth, the dropout rate of 31% was relatively high, even though it is similar to that in previous interventional studies in older adults with a 12-month follow-up period.28,40,41 Those who dropped out from the study had a lower baseline physical activity level than the non-dropouts, suggesting that subjects with low mobility may find it difficult to retain an interest in participation over the 12-month follow-up period. Although the total dropout rate was relatively high, the reasonable dropout rate of 12% during the intervention period 6 and the high exercise compliance of the BAL subjects (29.8 of 30.7 hours) indicate the excellent adhesion of the intervention and support its feasibility in clinical situations. Sixth, we did not measure muscle strength and could not confirm the effects of strength training program on lower extremities muscle power.
To conclude, the balance and gait training program assisted by technological devices reduced the number of fallers and the fall rate over 15 months compared with the strength training program. The positive findings from this study support the clinical use of balance and gait training for reducing fall events in people with PD.
Footnotes
Acknowledgements
We sincerely thank Professor Christina Hui-Chan and Dr Raymond Chung for their valuable advice.
Authors’ Note
The funders had no role in study design and execution, data analysis, or preparation of the article.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: The study was supported by SK Yee Medical Foundation (5-ZH61) and Hong Kong Parkinson’s Disease Foundation (5-ZH76).
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.