
Abstract
Postural instability and falls are complex and disabling features of Parkinson’s disease (PD) and respond poorly to anti-Parkinsonian medication. There is an imperative need to evaluate the effectiveness of exercise interventions in enhancing postural stability and decreasing falls in the PD population. The objectives of our study were to determine the effects of exercise training on the enhancement of balance and gait ability and reduction in falls for people with PD and to investigate potential factors contributing to the training effects on balance and gait ability of people with PD. We included 25 randomized control trials of a moderate methodological quality in our meta-analysis. The trials examined the effects of exercise training on balance and gait ability and falls against no intervention and placebo intervention. The results showed positive effects of exercise intervention on enhancing balance and gait performance (Hedges’ g = 0.303 over the short-term in 24 studies and 0.419 over the long-term in 12 studies; P < .05) and reducing the fall rate (rate ratio = 0.485 over the short-term in 4 studies and 0.413 over the long-term in 5 studies; P < .05). The longest follow-up duration was 12 months. There was no evidence that training decreased the number of fallers over the short- or long-term (P > .05). The results of our metaregression and subgroup analysis showed that facility-based training produced greater training effects on improving PD participants’ balance and gait ability (P < .05). The findings support the application of exercise training to improve balance and gait ability and prevent falls in people with PD.
Introduction
Falls are common in people with Parkinson’s disease (PD), with a high incidence rate of 40% to 70%.1,2 Falls are the most problematic feature in people with PD because they can lead to devastating outcomes such as physical injury and negative psychological effects that limit their mobility and ability to perform daily activities. 3 Fall prevention is, therefore, an urgent need for PD patients.
Postural instability is a cardinal symptom of PD and may make it difficult for individuals to perform functional tasks such as transferring and walking,4,5 resulting in poor self-perceived balance confidence 6 and eventually predisposing individuals to falls. 7 Because postural instability responds poorly to anti-Parkinsonian medication, 8 exercise training, a component of physical therapy, has been an important intervention in conjunction with current medical treatments to improve postural stability and reduce falls in individuals with PD. There is an imperative need to evaluate the effectiveness of exercise interventions in these areas.
An increasing number of studies have explored the effects of exercise training for individuals with PD.9-47 They have considered various categories of exercise training such as balance training, walking exercises, muscle strengthening, and stretching exercises. No review study hitherto has shown a reduction in falls, but given the small number of studies available, further work was required to determine if exercises could reduce falls in people with PD.48-51 Furthermore, no meta-analysis has investigated the long-term effects of training, which are more clinically meaningful than its short-term effects because of the progressive nature of PD.
Balance training commonly refers to exercises that challenge one’s control of the body’s center of mass during destabilizing movements and/or decrease the size of one’s base of support. 49 Gait training involves alternating step movements that challenge one’s dynamic control of the body’s center of mass. In our meta-analysis, we focused on exercises with balance and gait training components, with the primary objective being to examine the effects of training on enhancing balance and gait ability and reducing falls over the short- and long-terms. For effects on balance and gait ability, we considered short-term effects as the training effects after treatment completion and long-term effects as the carryover effects of treatment at follow-up intervals (with durations of 4 weeks or greater). Fall data collected during the intervention period and the follow-up period were included, respectively, for the short- and long-term analyses. Our second objective was to explore if the effect sizes in the short- and long-terms were influenced by the features of exercise intervention and the characteristics of individuals with PD.
Methods
Search Criteria
We conducted an extensive search of the literature up to May 8, 2015, using electronic databases, including the CINAHL database, MEDLINE, PubMed, Academic Search Premier via EbscoHost, and Cochrane Library. The keywords used to conduct the literature search were combined with the following English terms: (Physical therapy OR physiotherapy OR rehabilitation OR training OR exercise OR movement) AND Parkin* AND (balance OR postural stability OR gait OR fall). We found other potential studies by examining the reference lists of each identified article.
Study Selection
The studies eligible for this review were randomized controlled trials (including the first phase of crossover trials) for PD individuals, with outcomes related to balance, gait and/or falls. The inclusion criteria for trials were randomized controlled trials that involved experimental group(s) receiving interventions aimed at enhancing balance and gait performance, such as balance, gait, or strengthening exercise, and a control group that did not receive any intervention or just received placebo training that did not include balance, gait, or strengthening exercises (ie, active joint mobility and muscle stretching exercises).
Two investigators (the first and second authors) determined the eligibility of studies by screening the trial titles, abstracts, and full texts. Studies were excluded if they were not randomized controlled trials; if the experimental interventions did not involve any gait, balance, or strengthening exercise; or if the control group had undergone balance, gait, or strengthening exercises for their lower extremities. In addition, studies with low methodological quality, as judged by the Cochrane risk-of-bias tool were excluded from our meta-analysis. 52 All the discrepancies related to trial eligibility were resolved by discussion with a third party (the corresponding author).
Data Extraction and Quality Assessment
The 2 investigators developed a data extraction sheet. The first author extracted all data, and the second author checked their accuracy. The data included population and intervention characteristics; outcomes related to balance, gait, and/or falls; and the methodological quality of the trials evaluated via the Cochrane risk-of-bias tool. The participants’ characteristics included their age, disease severity as measured by the Hoehn and Yahr Staging Scale, medication status during assessment, and fall risk. Participants were classified as having a higher risk of falling if one of the following was indicated in the inclusion criteria: a history of falling in the past 12 months, experiencing freezing of gait in the past month, gait disturbance, postural instability with balance and mobility problems, reduced lower-limb strength, or reduced balance confidence. 53 The gait disturbance included subjective gait disturbance 17 or a score of 1 or 2 on the gait item of the Unified Parkinson’s Disease Rating Scale. 17 The postural instability included an instability during postural transfers, 11 functional reach ≤25 cm, 12 or an inability to achieve the criterion on one of the balance tests in the QuickScreen Clinical Falls Risk Assessments. 12
The intervention characteristics consisted of the percentage of balance and gait training within the total training program, total training hours and duration, training hours per week, amount of supervision given, and training location. 54 The balance training components included exercises that challenged one’s control of the body’s center of mass with destabilizing movements and/or while standing on an unstable or small base of support. The gait training components involved walking exercises over ground or on a treadmill. We calculated the percentage of balance and gait training within the total training program by dividing the time spent in balance and gait training by the duration of each training session when the information was available. Otherwise, we estimated it by dividing the time equally among balance training, gait training, strength training, and other exercises such as stretching and meditation in each training session. All the discrepancies were resolved by discussion with a third party (the corresponding author). In the case of missing and unpublished data, we attempted to contact the authors and successfully obtained information from 4 studies.19,23,24,27
The Cochrane risk-of-bias tool consists of 5 domains, including sequence generation, allocation concealment, blinding, incomplete outcome data, and selective outcome reporting. Each domain comprises 3 outcomes: low, high, and unclear risks of bias. Studies with a low risk of bias in 3 or more domains were suggested as trials of a moderate to high methodological quality and were included in the final meta-analysis. In contrast, studies with a low risk of bias in fewer than 3 domains were judged as trials of a low methodological quality and were excluded.
Quantitative Data Synthesis and Analysis
The outcome measures consisted of balance and gait outcomes and falls. Only one outcome of balance and gait ability in each of those studies was pooled for meta-analysis. We pooled the outcomes that were most frequently used by studies to minimize the heterogeneity and most comprehensive in measuring balance and gait ability.49,55 The final priority order of outcome measures was score on Berg’s Balance Scale, time of Timed Up and Go test, gait velocity of walking test at comfortable or fast speed, score of freezing of gait questionnaire, distance of 2-minyte walk test, time of sit-to-stand, and composite equilibrium score of sensory organization test.
Effect sizes were calculated using Hedges’ g for the balance and gait outcomes, the fall incidence rate ratio, and the fall risk ratio. For each outcome measure of the participants’ balance and gait ability, Hedges’ g of the short-term training effect was calculated by dividing the difference between the changes of the preintervention and postintervention means in the experimental and control groups through the estimated pooled standard deviation of the changes. The pooled standard deviation of the changes was estimated by standard deviation of the changes in the experimental and control groups, with bias corrected from the sample size in each group. For the long-term training effect in the trials with more than one follow-up evaluation, the value at the longest follow-up assessment replaced that at the postintervention assessment.
Fall incidence rate ratio was calculated according to the fall incidence rate in each group or obtained directly from the trials that presented the data. The fall risk ratio was calculated based on the number of persons who fell (fallers) during the study period in each group or obtained directly from the trials that presented the data. In the trials with follow-up periods, the rate and risk ratio values during the trial period after treatment completion were analyzed to explore the long-term fall prevention effects.
To decrease the unit-of-analysis error, 56 if there were multiple intervention groups in one trial, groups with similar intervention characteristics were combined to form a single intervention group to compare with the control group.35,38 The sample size of the single intervention group was the sum of the individual sample sizes of each intervention group. The means and standard deviations of the single-intervention group were calculated based on the individual group data. Intervention groups with different characteristics were considered as different groups and compared separately with the control group. Within one study, the sample size of the control group was divided equally among different intervention groups for comparison.20,22,34,37 The group means and standard deviations remained unchanged. For the crossover studies, only first-phase data were included in the data analysis. 27
Statistical heterogeneity was assessed with the I2 statistics. If there was significant heterogeneity between studies, the random-effects model of meta-analysis was used; otherwise, the fixed-effects model was used to analyze the training effects. 57 Publication bias was evaluated using Egger’s test to determine whether any association existed between the effect and sample sizes. For the effect sizes with significant heterogeneity across studies, univariate metaregression tests were performed to explore the correlations between the participant and intervention characteristics and effect sizes. The Cochrane handbook recommended a minimum of 10 studies to have the robustness of meta-regression; therefore, univariate metaregression was only performed for gait and balance outcomes.56,58 When there was significant correlation, subgroup analyses for each contributing factor was conducted.55,58 For instance, when risk of falling was found to be a significant factor affecting the effect sizes, meta-analyses for studies with participants at higher risk of falling and for those with participants at lower risk of falling were conducted in separate analyses consequently. Regarding the cutoff used for the subgroup analysis, the training location included facility, and community and home-based locations, and these determined the cutoff. The Comprehensive Meta-Analysis software (Version 2, Biostat, Englewood, NJ) was used to perform the meta-analyses, with the level of significance set at P < .05.
Results
Trial Flow and Study Characteristics
A total of 3413 studies were identified by database searches and 7 additional studies were identified by reference checks. Based on the titles and abstracts, 115 studies were selected to determine their eligibility. Finally, 38 articles were included in the qualitative synthesis. A total of 25 studies that had a moderate to high methodological quality were included in the final quantitative synthesis of the meta-analysis (Table 1). Figure 1 shows the flow of information through the review. All eligible studies reported the effects of training on participants’ balance and gait ability, and 8 studies examined the effects of training on outcomes related to falls. Table 2 summarizes the characteristics of the 25 studies.
Cochrane Risk of Bias of 38 Articles Included Into Qualitative Synthesis.
Abbreviations: Y, low risk of bias; N, high risk of bias; UC, unclear risk of bias.
Studies excluded from the quantitative synthesis for meta-analysis because of low methodological quality, with less than 3 domains having low risk of bias.
PRISMA flow diagram showing flow of information through the review.
Characteristics of the 30 Comparisons in 25 Included Trials.
Abbreviations: H&Y, Hoehn and Yahr; SD, standard deviation.
Participants were classified as having a higher risk of falling if one of the following was indicated in the inclusion criteria: a history of falling in the past 12 months, experiencing freezing of gait in the past month, gait disturbance, postural instability with balance and mobility problems, reduced lower-limb strength, or fall-related balance confidence (Canning et al 53 ).
The mean of H&Y was estimated from the Unified Parkinson’s Disease Rating Scale Motor score of 29.5 ± 12.8.
Other exercises: exercises not specifically targeted at enhancing balance and gait performance, such as active joint mobility and muscle stretching exercises.
The percentage of balance and gait training within the total training program was calculated by the time spent in balance and gait training, which was provided in the study.
Effects on Balance and Gait Outcomes
For the short-term effects (the immediate effects after treatment completion) on participants’ balance and gait ability, 1881 participants from the 24 studies were finally included in the data analysis. The fixed-effects model of the meta-analysis was used because there was a low level of heterogeneity in the effect size estimates among the 24 studies with 29 comparisons (I2 = 22%; P > .05). The meta-analysis found statistical significance in favor of the intervention group (P < .001), with a small overall mean effect size (Hedges’ g = 0.303; Figure 2A).
Forest plots from the meta-analyses of effects of exercise training demonstrating estimates of effect size with 95% confidence intervals (CIs): A. Short-term effects on balance and gait abilities. B. Long-term effects on balance and gait abilities. C. Short-term effects on fall rate. D. Long-term effects on fall rate. E. Short-term effects on number of fallers. F. Long-term effects on number of fallers.
For the long-term effects (the carryover effects at follow-up intervals), 941 participants from 12 studies with 13 comparisons were included in the final data analysis. The follow-up period ranged from 4 weeks31,35,38 to 12 months.39,40 There was a moderate level of heterogeneity in the effect size estimates (I2 = 50%; P < .05), and the random-effects model was used in the meta-analysis. The results of the meta-analysis showed statistical significance in favor of the intervention group (P < .001), with a mild overall effect size (Hedges’ g = 0.419; Figure 2B).
Effects on Falls
Among the studies, 8 explored the effects of training on fall prevention along with the outcomes related to the fall rate or number of fallers15,17,23,26,27,31,36,39; 6 studies reported the short-term effects,15,17,23,26,27,31 and 6 studies reported the long-term effects.15,17,23,26,31,36,39 The follow-up periods ranged from 4 weeks to 12 months.
In terms of the fall rate, the estimated effect sizes showed medium heterogeneity over the short- and long-terms (I2 = 62% and 61%, respectively; P < .05). The fall rate showed a significant overall reduction over the short-term (rate ratio = 0.485, P < .05; Figure 2C) and long-term (rate ratio = 0.413, P < .05; Figure 2D). For the number of fallers, the effect sizes demonstrated insignificant heterogeneity over short-and long-terms. The number of fallers did not decrease significantly over the short-term (risk ratio = 0.939, P > .05; Figure 2E) or long-term (risk ratio = 0.787, P > .05; Figure 2F).
The statistical significance in all the outcomes over both the short- and long-terms remained when any 1 trial was removed. There was significant publication bias for the effect sizes of balance and gait outcomes over the short- and long-terms among the included studies (Egger’s tests: P < .05).
Heterogeneity Across Studies and Potential Contributing Factors
The statistical heterogeneity of effects on balance and gait ability showed significance over the long-term (I2 = 50%; P < .05). The effect sizes significantly correlated with the training location during training (P < .05). The subgroup analyses showed that greater long-term training effects on balance and gait outcomes was achieved in participants who received facility-based training (Table 3).
Subgroup Analyses of Effect Sizes Related to Each Contributing Factor.
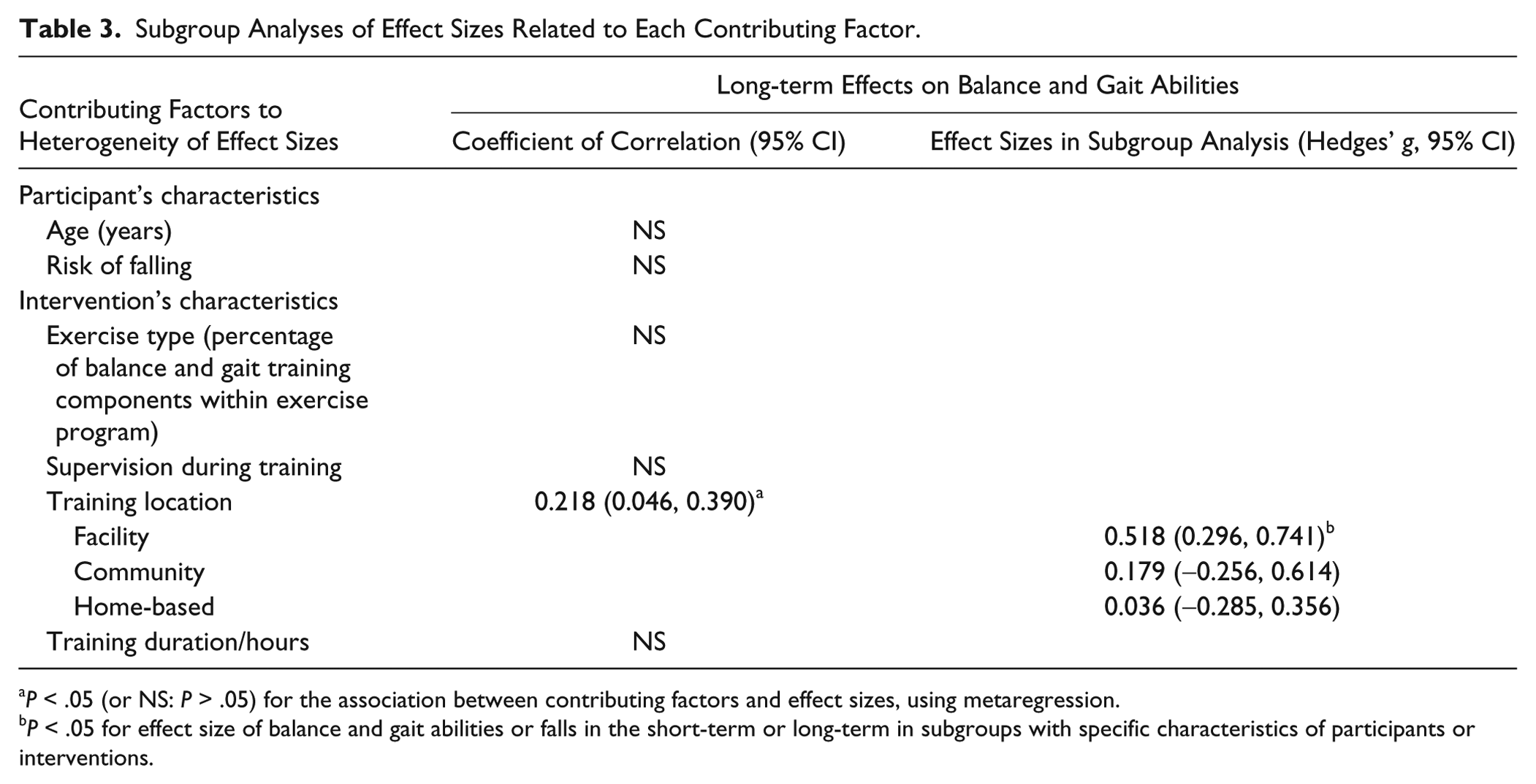
P < .05 (or NS: P > .05) for the association between contributing factors and effect sizes, using metaregression.
P < .05 for effect size of balance and gait abilities or falls in the short-term or long-term in subgroups with specific characteristics of participants or interventions.
Discussion
This is the first review study to report that exercise intervention can improve balance and gait performance over the short- and long-terms in people with PD. For the short-term effects on participants’ balance and gait ability, the overall effect size was positive but small, a finding comparable to 2 meta-analyses in people with PD.48,49 Tomlinson et al 48 reviewed 29 randomized controlled trials and suggested that physiotherapy has short-term benefits in gait speed and balance outcomes. Allen et al 49 analyzed the effects of exercises in 15 randomized and quasirandomized trials and concluded that exercise training improves the performance of balance-related activities in the short-term. Yet our findings provide more convincing evidence for several reasons. First, all the studies we included had a moderate to high methodological quality according to the Cochrane risk-of-bias tool, whereas most studies had low methodological quality in the review by Tomlinson et al, 48 and only fewer than half of the included studies had a moderate to high quality in the study by Allen et al. 49 Second, the short-term effect size heterogeneity among the studies considered in this review was insignificant and much lower than that reported by the previous studies.48,49 Third, we extended previous reviews by reporting positive and moderate long-term treatment effects for balance and gait ability. Despite the variation in follow-up periods (ie, 4 weeks to 12 months), this is the first study to demonstrate the benefits of exercise interventions in the longer term.
In addition to the positive balance and gait outcomes, our meta-analysis is the first to report that exercise training could decrease the fall rates of PD participants by about 60% over both the short- and long-terms. In contrast to fall rate, we found training to have an insignificant effect on the number of fallers, a finding that agrees with that of Allen et al. 49 Our review and that of Allen et al 49 included a small number of studies and with exercise as the only intervention. Previous meta-analyses in older people reporting significant reduction in the number of fallers included a large number of studies,51,59 with exercise intervention alone 59 or with exercise intervention combined with medicine, psychological treatment, education, and so on. 51 It is possible that the small number of included studies or the type of intervention contributed to our insignificant effects on reducing the number of fallers. More studies are needed to investigate the effects of exercise intervention on fall reduction in people with PD.
We further explored factors that contributed to the effect sizes of balance and gait improvement in an attempt to suggest an efficacious exercise training protocol. The subgroup meta-analysis results showed that training at facilities led to more improvement in balance and gait ability over the long-term than the community- and home-based training. Facility-based training, mostly supervised by physical therapists, could have enabled participants to practice the training tasks at their optimal capacity. 49 Therapists in these studies applied motor learning principles such as progression from simple to difficult tasks,23,26,28,31,38 attentional strategies,31,38 and augmented feedback 38 to enhance learning and practice, leading to better retention of the learned balance strategies and reduced fall risk. With respect to the exercise type, there were no significant correlations between the percentage of balance and gait training components and effect sizes of balance and gait ability over the long-term. Strength training was another component and could have a role in enhancing balance and gait performance. 39 Regarding exercise dosage, the training duration of the included trials ranged from 4 to 48 weeks and with a total of 4 to 96 hours. However, there were no significant correlations between the training duration and effect sizes in the long-term balance ability. A few studies instructed participants to perform home exercises during the follow-up period,15,40,44 but only 2 studies reported participants’ compliance with the home exercises.40,44 Thus, the impact of exercise dose and continuous exercises on balance ability and fall reduction is unclear, and more studies are needed in these areas.
Notwithstanding its significant findings, this study has several limitations. First, similar to a previous review, 49 the included trials showed some publication bias for the effect sizes of balance and gait outcomes over the short- and long-terms, probably because a few studies showed a relatively large positive effect size. Second, some of the included studies did not indicate information such as the training durations of the balance and gait components, and we thus had to estimate such information. Standardization of the estimation method was used to minimize its influence on the sources of effect size heterogeneity in the studies we examined. Third, the differences in key participant and intervention characteristics between studies and the heterogeneity in outcome measures could contribute to the effect size heterogeneity. Finally, few of our included studies examined the effects of training on fall outcomes, and the studies that explored long-term effects had different follow-up durations; therefore, the results should be interpreted with caution.
In conclusion, exercise training can improve balance and gait ability in individuals with PD and decrease their fall rates over both the short- and long-terms, which may provide guidance for treatment or for future trials in the PD population. The correlations between effect sizes and the exercise training program characteristics suggest that greater training effects might be contributed by balance and gait training conducted within facilities. These associations should be examined in further studies to determine the optimal fall prevention protocol for individuals with PD.
Footnotes
Acknowledgements
We sincerely thank Dr Stephanie Au-Yeung for her valuable advice.
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.