
Abstract
Background. Although most mirror therapy studies have shown improved motor performance in stroke patients, the optimal mirror training protocol still remains unclear. Objective. To study the relative contribution of a mirror in training a reaching task and of unilateral and bimanual training with a mirror. Methods. A total of 93 stroke patients at least 6 months poststroke were instructed to perform a reaching task as fast and as fluently as possible. They performed 70 practice trials after being randomly allocated to 1 of 5 experimental groups: training with (1) the paretic arm with direct view (Paretic-No Mirror), (2) the nonparetic arm with direct view (Nonparetic-No Mirror), (3) the nonparetic arm with mirror reflection (Nonparetic Mirror), (4) both sides and with a nontransparent screen preventing visual control of paretic side (Bilateral-Screen), and (5) both sides with mirror reflection of the nonparetic arm (Bilateral-Mirror). As baseline and follow-up, patients performed 6 trials using only their paretic side. Primary outcome measure was the movement time. Results. We found the largest intervention effect in the Paretic-No Mirror condition. However, the Nonparetic-Mirror condition was not significantly different from the Paretic-No Mirror condition, while the Unaffected-No Mirror condition had significantly less improvement than the Paretic-No Mirror condition. In addition, movement time improved significantly less in the bimanual conditions and there was no difference between both bimanual conditions or between both mirror conditions. Conclusion. The present study confirms that using a mirror reflection can facilitate motor learning. In this task, bimanual movement using mirror training was less effective than unilateral training.
Introduction
It has been reported that 55% to 75% of stroke survivors suffer from a paretic arm. 1 Intensive, task-specific training programs have been shown to improve motor function, even in patients in the chronic phase of stroke, 2 but are generally time consuming and expensive. Mirror therapy, originally designed by Ramachandran et al 3 to alleviate phantom limb pain, is a cheap and promising intervention that has been shown to improve upper limb function in acute, 4 subacute 5 and chronic stroke patients. 6
Although most studies on mirror therapy have shown improved motor performance in their participants, the quantum of improvements has been relatively small, not always reaching clinical significance.4,6 In addition, there are differences between studies in how mirror therapy is performed. Among others, differences exist in whether the paretic hand behind the mirror is instructed to move as much as possible bimanually with the uninvolved hand in front of the mirror. In most mirror therapy studies in stroke patients, participants are instructed to practice bimanually, moving affected and unaffected limbs together. This provides a direct motor training paradigm, related to the known effects of bimanual training programs. 7 The added value of mirror therapy in this form of training is that the mirror replaces feedback on movement of the affected side by a form of “virtual feedback” that creates the illusion that the paretic side moves with a normal movement pattern. However, from the relatively small number of trials and the lack of a direct comparison of different types of mirror training, the most optimal training is presently unclear.
While from a motor learning perspective it may be most effective to instruct patients to move the paretic side behind the mirror as much as possible, it could be argued that the strength of the mirror illusion decreases as a result of paretic side movement, as it causes an incongruence between task performance and visual feedback. In addition, movement of the paretic arm behind the mirror may increase proprioceptive feedback of the arm behind the mirror, which then may partly disrupt the visual illusion. This would suggest that movement of the arm behind the mirror is not beneficial or even detrimental. In addition, if movement of the hand behind the mirror is not necessary to obtain a motor learning effect, it would indicate the added value of using mirror therapy in severely affected patients without any residual paretic arm function, for whom there are very few therapeutic options currently available.
The aim of the present study was to gain insight in the relative contribution of a mirror in exercising a reaching task and in the differences in unilateral and bimanual exercises when training such a reaching task with and without a mirror. To realize this, we used a short-term motor learning task, which allowed us to compare several conditions in an effective, controlled manner. The aim was not to create a clinically meaningfully change in hand function, but to show differences in learning due to the different learning conditions. In all conditions, the task was to perform a reaching movement to a target from a standardized position as quickly as possible. We had stroke patients train this task under the following experimental conditions: (1) task performance with affected hand and direct view of affected side (Affected-Only condition), (2) task performance with the unaffected side and direct view of the unaffected side (Unaffected-No Mirror), (3) task performance with the unaffected side and mirror reflection of unaffected side as if the affected side is also moving (Unaffected-Mirror), (4) task performance with both sides and a screen between arms preventing view of affected side (Bimanual-No Mirror), and (5) task performance with both sides and mirror reflection of the unaffected side as if the affected side is moving similarly (Bimanual-Mirror).
Methods
Participants
Patients were recruited from Rijndam Rehabilitation Centre, Rotterdam; Rehabilitation Centre Blixembosch, Eindhoven; and Rehabilitation Centre Leijpark, Tilburg, all located in the Netherlands. After contacting 252 outpatients (hospitalized between January 1998 and August 2010), 103 patients were enrolled. Inclusion criteria were knowledge of the Dutch language, at least 6 months poststroke, home dwelling status, and a Brunnstrom score for the upper extremity between III and VI. 8 The 6 stages of the Brunnstrom score range from (I) flaccidity to (VI) full-range voluntary extension and individual finger movements although less accurate than on the opposite side. Patients with neglect, comorbidity that influenced upper extremity usage, or a history of multiple strokes were excluded from participation.
Sample Size
The sample size was calculated on data from a study of Cirstea and Levin, 9 on which our experimental paradigm was based. Assuming a standard deviation of 0.20s, we calculated that 12 patients in each group would be sufficient to have an 80% chance of detecting a statistically significant difference in improvements of 0.25s between any 2 groups. To increase the power, we aimed for a total of 20 patients in each group.
Clinical Assessment
Before the start of the experiment, motor ability of the participants was evaluated with the Fugl-Meyer Assessment (FMA).10,11 The upper extremity part of the FMA examines voluntary movements and the ability to execute upper limb movements outside of synergies. It consists of 9 components: reflexes, flexor synergy, extensor synergy, movement-combining synergies, out of synergy movement, normal reflex activity, wrist, hand, and coordination speed. The FMA assessment scores range from 0 to 66, with higher scores indicating better motor recovery.
Experimental Procedure
Our experimental paradigm was based on a study of Cirstea and Levin. 9 Participants had to perform a simple motor task consisting of a pointing movement with the index finger. Participants had to move their index finger from a target located next to their chair toward a target located in front of them (Figure 1). The distance and height of the end target was adjusted according to the length and ability to extend the arm for each subject. The target was placed such that, at the end of the pointing movement, the finger just did not make contact with the target. A sound indicated the start of the trial, and patients were instructed to maintain their finger at the final position until a second sound indicated the end of the trial. Patients were instructed to move as fast and as fluently as possible toward the target.
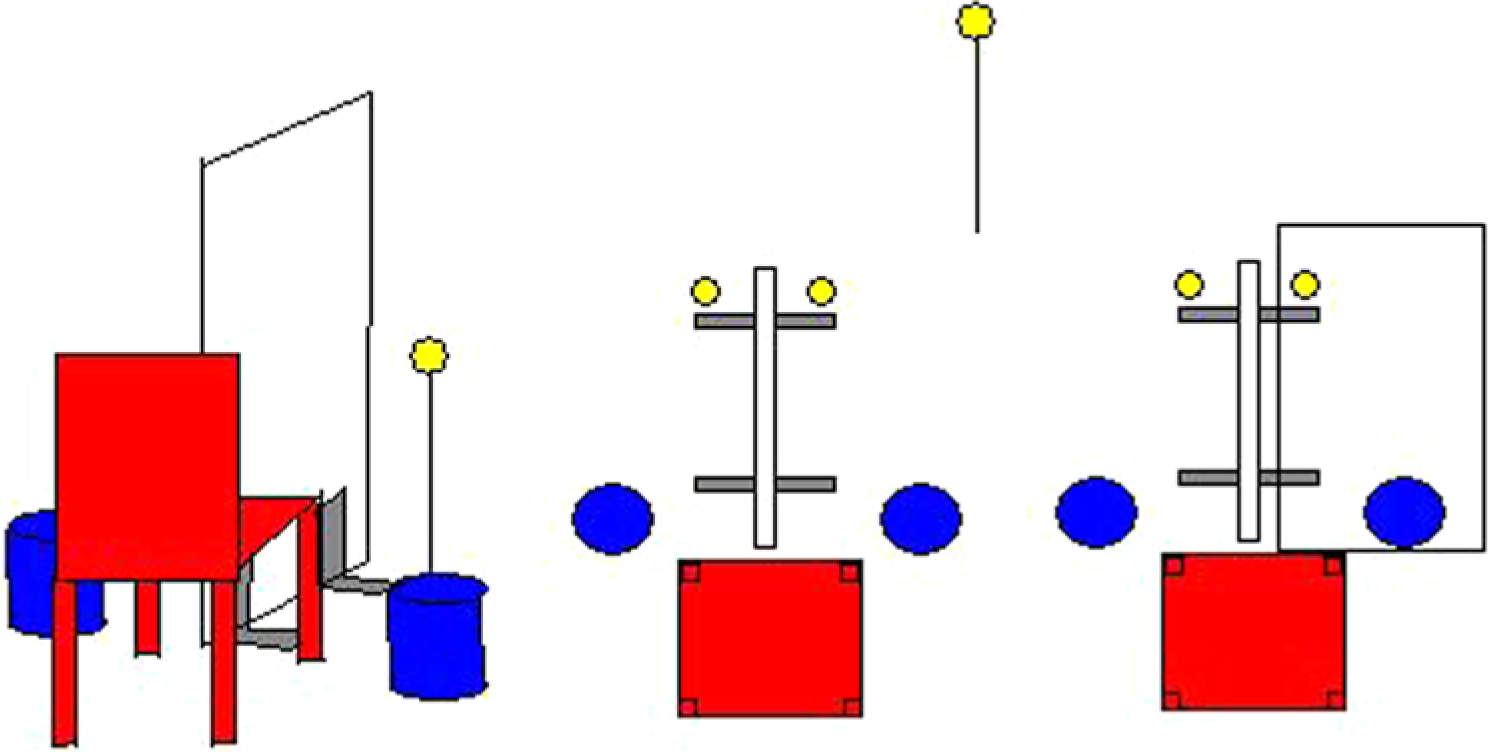
Experimental setup. Side view and top view representation of the measurement setup. The participants had to move their index finger from a target located next to their chair (blue cylinder in the picture) toward a target located in front of them (yellow circle). The distance and height of the end target was adjusted according to the length and ability to extend the arm for each subject. The target was placed such that, at the end of the pointing movement, the finger just did not make contact with the target. During the measurements of baseline and follow-up performance, subjects moved only the involved hand. Based on the experimental condition, a mirror could be placed between both hands.
All participants began with performing the pointing task with their affected side and with direct vision. A total of 6 trials served as baseline measurements. After these first 6 trials, patients were allocated to 1 of the 5 experimental groups (see below), and practiced the task 70 times under the allocated experimental condition. After the practice period, they again performed 6 trials using only their affected side with direct vision, which served as follow-up measurement.
Experimental Conditions
Participants were randomly assigned to 1 of the 5 experimental conditions. To minimize possible confounding effects of motor ability and age, we stratified participants into groups based on age (older or younger than 55 years) and motor function (Fugl-Meyer score smaller or greater than 50). In this way, we created 4 strata, which were all randomized separately into the experimental groups. The random allocation was based on a computer-generated random code using blocks of 20 patients and using sealed envelopes.
The experimental conditions were as follows: (1) task performance with affected hand, direct view of affected side (Affected-Only), (2) task performance with unaffected side, direct view of unaffected side (Unaffected-No Mirror), (3) task performance with unaffected side, mirror reflection of unaffected side as if the affected side was also moving (Unaffected-Mirror), (4) task performance with both sides, screen between arms preventing view of affected side (Bimanual-No Mirror), and (5) task performance with both sides, mirror reflection of unaffected side as if the affected side was moving exactly similar as the unaffected side (Bimanual-Mirror).
Data Acquisition and Analysis
Kinematic data from the arm and trunk were recorded with a 3-dimensional optical tracking system (Qualisys, Gothenburg, Sweden). Reflecting markers were placed on the index (tip), the wrist (head of the ulna), the elbow (lateral epicondyle), the shoulders (ipsilateral and contralateral acromion processes), and the trunk (top of the sternum). Movements were recorded for 3 to 5 seconds at 240Hz. Based on the recordings, 3-dimensional position profiles were created with Qualisys Track Manager (1.5.1.x).
Outcome Measures
Following Cirstea and Levin, 9 the primary outcome measure of the present study was the movement time of the reaching task since this was also the primary out. As secondary outcome measures, we determined reaction time, peak movement velocity, number of peaks in the velocity profile as a measure of the smoothness of the trajectory, and the precision of reaching the target.
From the 6 baseline and follow-up recordings, we omitted the first trial, regarding this as a learning trial. To calculate the outcome measures, first, raw X–Y–Z position data were preprocessed using a smoothing filter with a cutoff frequency of 8 Hz. The velocity of the index finger was than obtained by differentiating x, y, and z marker positions. The beginning and the end of the movement were defined using the model of Schot et al, 12 wherein multiple sources of information are selected to define start and endpoints. For the present study, we used the distance from the target, the velocity in forward (y) direction and the time since movement as predictors in the model. We used a 2-step approach, wherein we first low-pass filtered the signal at a very low frequency (2 Hz), then defined the endpoint in that signal, and then selected the exact end of the movement.
Movement time was defined as the time between start and end of the movement. Reaction time was defined as the time between the start signal and the start of the movement. Peak velocity was defined as the highest value in the velocity scalar, as calculated from the filtered x–y–z velocities. Movement precision was defined as the smallest difference between the tip of the index and the target position and smoothness was defined as the number of peaks in the filtered velocity signal.
Statistical Analysis
For each task and parameter, individual mean values and coefficients of variation for the 5 baseline and follow-up trials were calculated and used for group analysis. We omitted the first trial of the 6 baseline and follow-up trials. A linear mixed-model analysis was used to test for differences in the intervention effect (the differences between baseline and follow-up) between the different conditions. In this mixed-model approach, we included a random effect for the slope (change in measure between baseline and follow-up) and for the baseline value per patients.
The condition, time (difference baseline and follow-up), and the interaction between condition and time were used as fixed effects. The linear mixed-model compared condition 1 (Affected-Only) with each of the other 4 conditions. In addition, we compared condition 2 (Unaffected-NoMirror) with condition 3 (Unaffected-Mirror) and we compared condition 4 (Bimanual-NoMirror) with condition 5 (Bimanual-Mirror) since these pairs were composed of similar conditions except for the mirror effect. Furthermore, we compared the 2 mirror conditions (Unaffected-Mirror plus Bimanual-Mirror) and with the 2 no-mirror conditions (Unaffected-No Mirror and Bimanual-No Mirror) as well as both mirror conditions (Unaffected-Mirror and Bimanual-Mirror). All statistical analyses were performed using SAS and a P < .05 was considered statistically significant.
Results
A total of 103 patients participated in this study. Although initially found eligible for the study, we found that 10 patients were not able to sufficiently concentrate throughout the high number of reaching movement or became too fatigued (see Figure 2). Table 1 shows the patient characteristics of all 5 experimental groups. While we found relatively large differences in the time since stroke between groups, we did not find a significant correlation (r = .151, P = .155) between this variable and the primary outcome measure (the change in movement time between baseline and follow-up). Therefore, we did not further correct for these differences between groups.
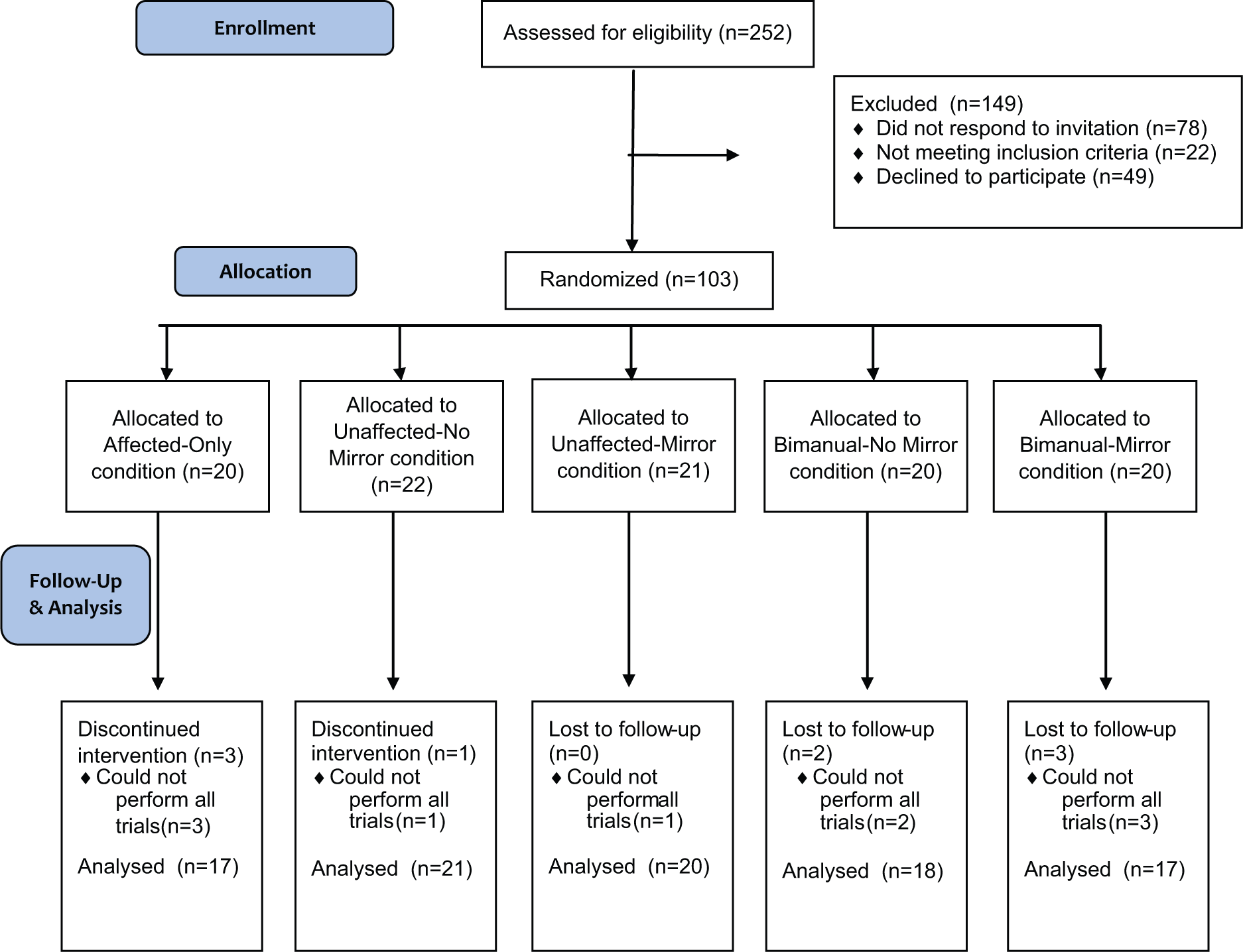
Consort flow diagram describing the study procedures and distribution of the patients over the different groups.
Patients’ Characteristics. a
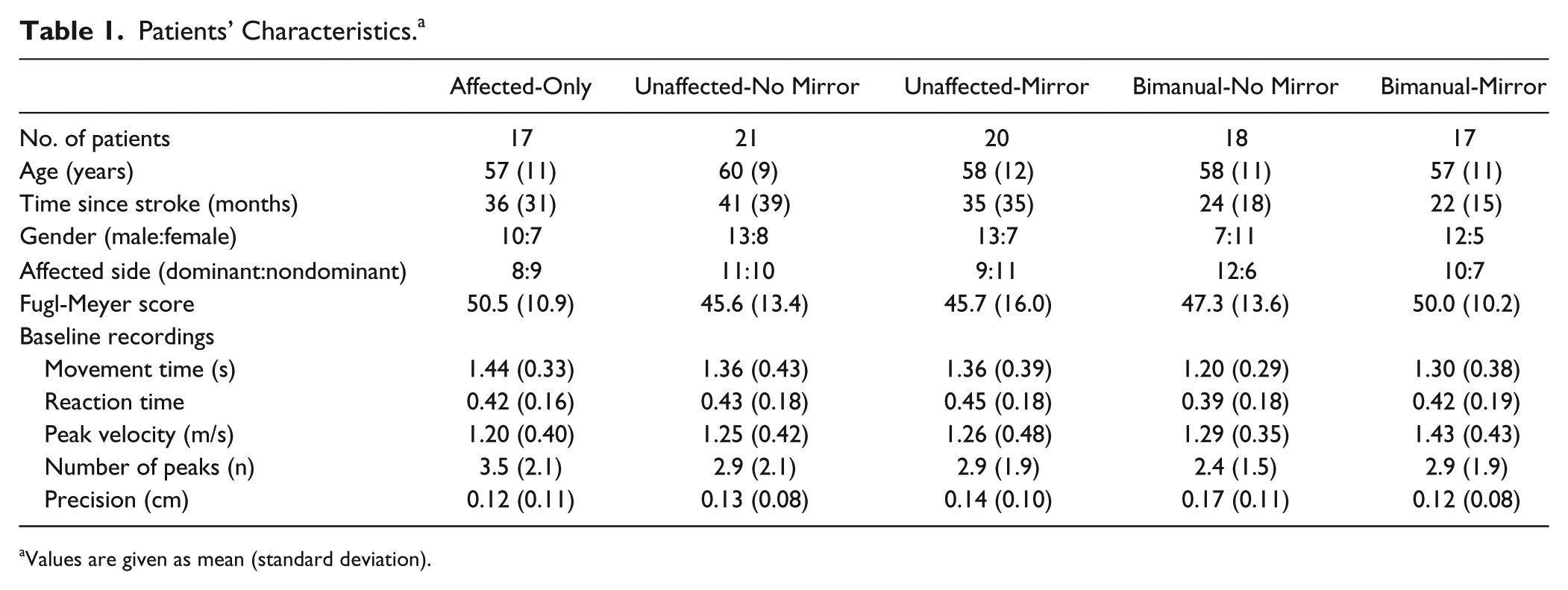
Values are given as mean (standard deviation).
Figure 3 shows the results of the primary outcome measure movement time before and after the 70 practice trials time in each of the 5 different conditions. We found an overall time effect between the baseline and follow-up measurements (P < .0001), indicating that the groups significantly improved following the reaching exercises. The largest improvement in movement time was seen in the Affected-Only condition. The improvement in the Unaffected-No Mirror condition and the Bimanual-Mirror conditions were significantly smaller than the Affected-Only condition, and the Bimanual-No Mirror condition approached statistical significance. In contrast, the improvements in the Unaffected-Mirror condition were not significantly different from the Affected-Only condition. When comparing the mirror conditions with the no mirror conditions, we found a trend toward a significantly larger improvement in the Unaffected-Mirror condition versus the Unaffected-No Mirror conditions (P = .078) while both Bimanual conditions were not significantly different (P = .621). Finally, the comparison of the combined Mirror conditions (Unaffected-Mirror plus Bimanual-Mirror) versus the combined no-mirror condition (Unaffected-No Mirror plus Unaffected-Bimanual) was not significantly different (P = .102) and nor was the comparison between the unimanual mirror condition (Unaffected-Mirror) and the bimanual mirror condition (Bimanual-Mirror, P = .334).
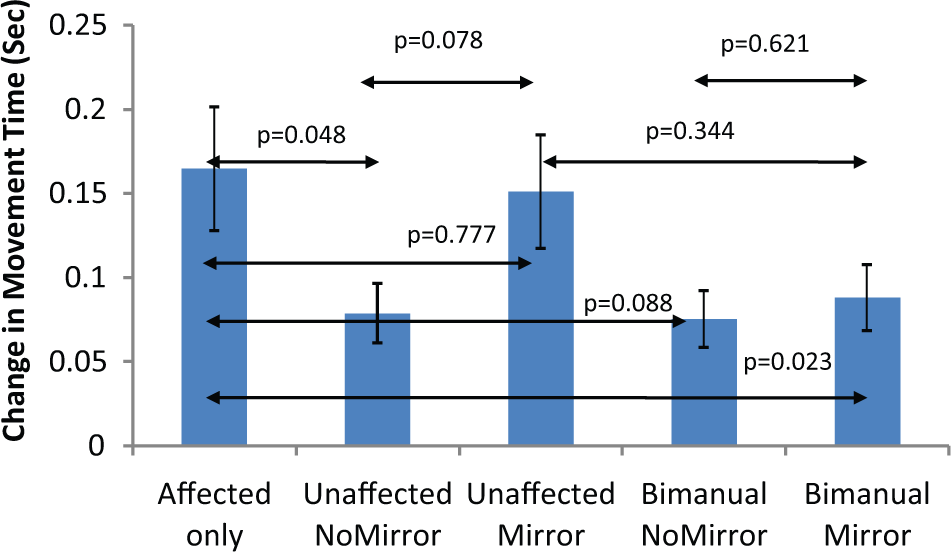
Movement time. Mean (standard error of the mean) change scores in movement time during the five different conditions. The P values indicate the difference in change scores between the Affected-Only condition with each of the other 4 conditions. In addition, P values are shown between both Unaffected conditions and both Bimanual conditions.
The changes between baseline and follow-up measurement for the secondary outcome measures are shown in Table 2. We found no general time-effect between the baseline and follow-up measurements for the reaction time and the movement precision, while we did find significant effects for the peak velocity and the number of peaks. When comparing the change scores of the Affected-Only condition and the other 4 conditions, we found overall no significant differences except for the peak velocity, where both bimanual conditions (Bimanual-No Mirror and Bimanual-Mirror) showed significantly less improvement in peak velocity than the Affected-Only condition.
Secondary Outcome Measures. a
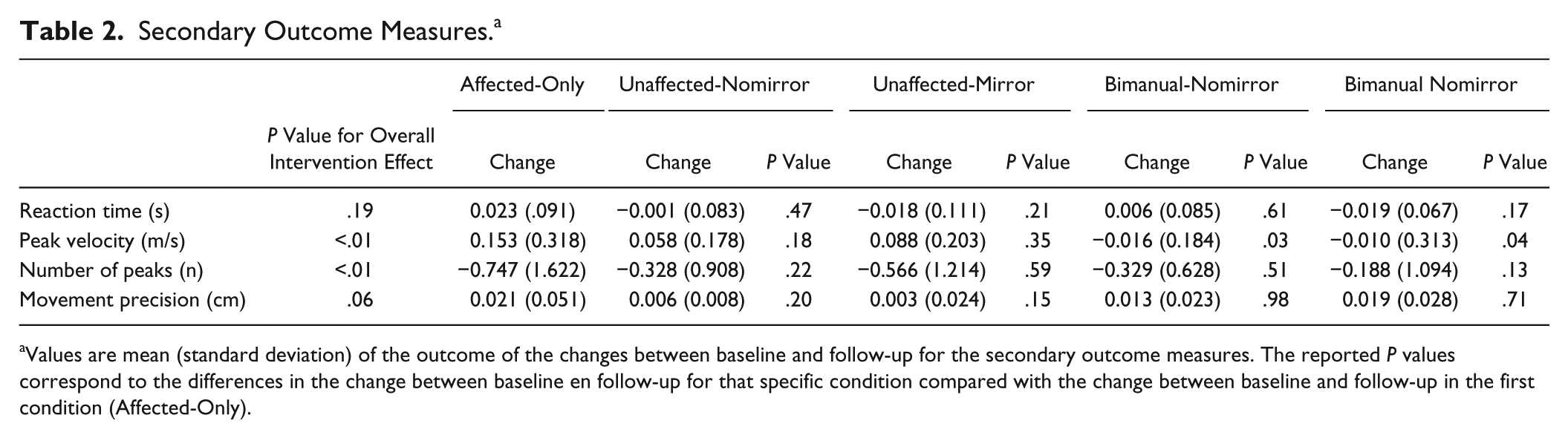
Values are mean (standard deviation) of the outcome of the changes between baseline and follow-up for the secondary outcome measures. The reported P values correspond to the differences in the change between baseline en follow-up for that specific condition compared with the change between baseline and follow-up in the first condition (Affected-Only).
Discussion
The aim of the present study was to gain insight in the relative contribution of a mirror in performing a reaching task and in the differences in unilateral and bimanual exercises when training such a reaching task with and without a mirror. We found a significant overall intervention effect on the primary outcome measure of movement time, indicating a learning effect in the primary outcome measure after 70 training movements. When comparing the conditions, we found the largest intervention effect in the Affected-Only condition in which only the involved hand was trained. However, the condition where the patients only trained the uninvolved hand while using a mirror (Unaffected-Mirror) was not significantly different from the Affected-Only condition, while the Unaffected-No Mirror condition had significantly less improvement than the Affected-Only condition. In addition, improvement in movement time was significantly smaller in the Bimanual-Mirror condition, while there was a trend that the improvement in the Bimanual-No Mirror condition was also significantly smaller than the Affected-Only condition.
To our knowledge, this is the first study to compare a number of different mirror and no-mirror training conditions in stroke. Previous studies on mirror therapy in stroke were mainly case series13,14) or randomized controlled trials.4-6 The randomized controlled trials all compared the effects of several weeks of mirror training on functional outcome measures such as the Fugl-Meyer score and the Functional Independence Measure scores. These trials differed in how the mirror training was performed and in the type of training of the control group. In the first mirror therapy study on stroke patients, Altschuler et al 15 compared mirror training with the same training but using a plastic sheet between both hands. Training was bimanual in the sense that patients were instructed to move as well as possible with the involved hand. Similar instructions were given in the trials by Michielsen et al 6 and Dohle et al, 4 both comparing a mirror group with a control group that performed similar exercises without a mirror. Yavuzer et al 5 also used bimanual movements. However, in this study, the control group used the nonreflective side of mirror. In healthy controls, Hamzei et al 16 compared 4 days of 20-minute training between a mirror and a no-mirror group, with the contralateral arm stationary. Finally, Sütbeyaz et al 17 also used the non-reflective side of the mirror in the control group but instructed patients to only move the unaffected leg.
Our finding that training with a mirror increases motor learning is in line with a large number of clinical studies as well as 2 recent studies on healthy participants (Hamzei et al 16 and Nojima et al 18 ). However, since most of the clinical studies used bimanual training in both groups and since all of these studies report small but significantly better results in the mirror group compared to the control group, it may be surprising that in the present study the training effects of the bimanual training were relatively small and that there was no significant difference between the Bimanual-No Mirror and the Bimanual-Mirror conditions. A reason why the training effects in these conditions were relatively small might be that these conditions were more tiresome for the affected arm of the patients than both Unaffected-Only conditions. In the 2 unaffected-only conditions (Unaffected-Mirror and Unaffected-No Mirror), subjects performed only affected arm movements during the baseline and follow-up measurements, while in the bimanual conditions subjects performed 70 bilateral movements.
It should be noted that the performance of the simple reaching movement in the present study is not clinically relevant in itself and that the short training session may not have long-lasting effects of motor capacity. In addition, the short training may only lead to a motor learning effect for this specific task en may not indicate improvement of motor control of the paretic arm, which would require much longer training. However, the aim of this study was not to establish the clinical application of specific mirror therapy training schemes, but to compare different training schemes within a single study. This approach is in line with the recent study of Hamzei et al, 16 showing significant differences more improvement in motor tasks of moving pegs and marbles in a mirror group compared with a control group in 2 groups of 13 subjects using a training load of only 20 minutes per day for 4 days. Similarly, Nojima et al 18 trained a rotation movement of a ball 10 sessions of 30 seconds and found significantly larger increase in the number or rotations in a mirror group compared with a control group. The similar outcomes of these 2 studies with our study indicate that simple motor tasks can be used to study differences in motor learning in an efficient way. This may guide further development of training schemes that can be tested in future randomized controlled trials.
The present study has a number of limitations. One limitation, as already mentioned earlier, was that fatigue of the involved hand may have been different between conditions. While this may have influenced some of the conditions, it did not influence the direct comparison between the mirror and no-mirror conditions (Unaffected-No Mirror vs Unaffected-Mirror and Bimanual-No Mirror vs Bimanual-Mirror). A second limitation was that the number of patients per group was relatively small. The power analyses of our study was based on a findings by Cirstea and Levin, 9 showing a 0.25s improvement in the Affected-Only condition, which was comparable with the present study (0.19s improvement). Although a number of trends that did not reach statistical significance, we did find a significant difference in the primary outcome measure, indicating sufficient power for these comparisons. Finally, in this study, we did not study the underlying mechanisms of the differences between the conditions. An increasing number of studies focus on the neural neuronal correlates of mirror therapy and observational learning,16,19-22 relating the effects to, among others, the mirror neuron system that is known to be activated when observing reaching movements.
Conclusions
In summary, the present study confirms that using a mirror reflection can facilitate motor learning as confirmed by the relatively large effect of the mirror when moving only the unaffected hand. However, at the same time, the present data indicate that mirror training alone is not more effective than directly training the involved hand. Taken together, our data suggest that mirror therapy may be effective in specific situations, such as where the patient is not yet able to move the affected hand or where the affected hand is easily fatiguing. For patients with a better functioning of the affected arm, it may be more effective to combine mirror training with training of only the affected arm or with other training regimens such as constraint-induced movement therapy.
Footnotes
Authors’ Note
Ruud W. Selles and Marian E. Michielsen contributed equally to this study.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.