
Abstract
Background. Constraint-induced movement therapy (CIMT) is a rehabilitation approach for arm paresis consisting of an intensive schedule of treatment (6 h/d). The high demand of resources for CIMT is a critical issue for its implementation in the Italian health system. Objective. To compare the effects of a reduced-intensity modified CIMT (mCIMT) program that included splinting the unaffected arm for 12 hours daily with the effects of a conventional rehabilitation program for arm paresis in patients with stroke. Methods. Sixty-six participants with hemiparesis (3-24 months poststroke) who could extend the wrist and several fingers at least 10° were randomly assigned to mCIMT or conventional rehabilitation. Each group underwent 10 (2 h/d) treatment sessions (5 d/wk for 2 weeks). Patients were assessed with the Wolf Motor Function Test (WMFT-FA and WMFT-T), the Motor Activity Log (MAL-AOU and MAL-QOM), and the Ashworth Scale before and after treatment and 3 months later. Results. Between-groups analysis showed that the mCIMT group overall had greater improvement than the control group in terms of the WMFT-FA (P = .010), MAL-AOU (P < .001), and MAL-QOM (P < .001). Differences between groups were significant both after treatment (P < .01) and at the 3-month follow-up (P < .01), although 40% of participants did not complete the 3-month assessment. Furthermore, the mCIMT group showed a greater decrease of Ashworth Scale score than the control group at 3 months (P = .021). Conclusion. Two hours of CIMT may be more effective than conventional rehabilitation in improving motor function and use of the paretic arm in patients with chronic stroke.
Keywords
Introduction
Approximately 33% to 66% of patients with arm paresis show minimal recovery of function 6 months after stroke. 1 These patients tend to rely on their unaffected arm to perform activities of daily living (ADLs),2,3 leading to “nonuse” with progressive suppression of movements.3-5 To overcome learned nonuse, Edward Taub et al 3 proposed “constraint-induced movement therapy” (CIMT), which involves intense, functionally oriented task practice with the paretic upper extremity, along with restraint of the less affected upper extremity.3,6 Neurorehabilitation studies have shown that CIMT can increase both motor function and use of the paretic arm of adult patients after stroke3,7-13 and that these improvements parallel changes in activation of the brain sensorimotor network.5,14 One issue of debate in the application of CIMT is the high economic cost because of the great deal of one-to-one therapy (approximately 6 h/d). 11 This issue is particularly relevant in Italy where funding allocated by the health system to rehabilitation is scarce. To overcome this limitation, modified CIMT (mCIMT) protocols may be more feasible.9,11-13,15-19
Studies performed on acute17,20-24 and chronic9,16,18,25-29 patients with stroke have shown that the mCIMT protocols can be effective in improving both use and function of the affected limb. However, studies with a large sample size and follow-up data are required.9,12,13 In addition, the effects of mCIMT on spasticity require clarification.30,31 We hypothesized that a mCIMT program may induce a greater improvement of function and use of the affected arm than a conventional rehabilitation program used for patients with stroke in Italy.
Methods
Study Design
This was a multisite randomized control trial (RCT) promoted by the Italian Society of Neurological Rehabilitation (SIRN) involving 9 clinical sites. A steering committee made up of the main investigator of each of the clinical sites made all the decisions concerning the conduct of the study and decided that the main investigator (NS) was responsible for the randomization procedure. If eligible, patients were allocated to the experimental group (EG) or the control group (CG) by means of an automated randomization system (allocation ratio 1:1). 32 The group allocation was concealed using sealed numbered envelopes that were sent to the clinical hospital where the treatment was delivered. The randomization list was locked in a desk drawer accessible only to the main investigator.
Patients
Inclusion criteria
First-ever ischemic or hemorrhagic stroke (3-24 months poststroke)
Presence of at least 10° of active wrist extension, at least 10° of thumb abduction/extension, and at least 10° of extension at the level of the metacarpophalangeal and interphalangeal joints in at least 2 digits among the II–III–IV–V fingers (these movements had to be repeated 3 times in 1 minute starting from the resting position) 27
Adequate balance while independently standing from a sitting position
Ability to stand for at least 2 minutes without arm support
Passive range of motion (ROM) of at least 90° of shoulder flexion and abduction, 45° of shoulder external rotation, −30° of elbow extension, 45° of forearm supination and pronation (from neutral position), 30° of wrist extension and finger extension to neutral such that no metacarpophalangeal joint had a contracture. 33
Exclusion criteria
Subarachnoid hemorrhage
Age <18 years or >85 years
Mini-Mental State Examination 34 score ≤23/30
Motor Activity Log–amount of use 3 score ≥2.5
Visual analog scale for pain 35 score ≥4 at the affected arm
Participation in other pharmacological or rehabilitation studies during the study period
Treatment of upper limb spasticity (eg, botulinum toxin) in the 3 months prior to the start of the study and/or during its execution
Motricity Index 36 (MI) pinch grip subscore ≤11 or ≥26
All patients were informed of the experimental nature of the study and gave their consent for participation. The study was approved by the Ethics Committee of the IRCCS Santa Lucia, Rome, and subsequently by ethics committees of all sites. The trial was registered in the SIRN clinical trial register (No. 2007/2) and among the scientific research programs of national relevant interest (PRIN) promoted by the Italian Ministry of University and Research (No. 2007MHL4CM).
Treatment Procedures
Prior to the start of the study the steering committee designed the EG (mCIMT) and CG treatment protocols. To ensure uniformity in the delivery of treatment, one therapist from each center was taught the mCIMT treatment protocol and the other was taught the CG protocol.
Participants in both groups received 1-hour, individual treatment sessions as outpatients and 1-hour of household activities 5 days a week (Monday to Friday) for 2 consecutive weeks. In addition, patients in the EG wore a splint on their unaffected arm for at least 12 of their waking hours (Monday to Friday). The splint permitted the unaffected arm to assist in transfers and ambulation (shoulder and elbow movement were permitted), but it prevented use of the hand, forcing the patient to use the affected arm to perform ADLs. Adherence to splint use was controlled by instructing the patient’s caregiver to monitor the patient at least 6 times during waking hours. If the patient was found without a splint, the caregiver recorded the incident in a time log. If 4 of these incidents occurred, the patient was excluded from the study.
The household activities consisted of 30 functional everyday activities (switching on the light, combing one’s hair, etc). The patient, supervised by a caregiver, was required to repeat each activity for approximately 2 minutes, for a total of 1 hour. The caregiver was required to document the start and end time of each therapy session performed at home. The household activities were the same (type of exercises and duration) for both groups. The outpatient treatment was carried out in the morningand the household activities in the afternoon.
Experimental Group Training
Each session consisted of 3 types of activities involving the paretic arm: (a) 10 minutes of passive mobilization of the affected arm joints through full ROM to prevent secondary myoarticular damage and give sensory stimulation, (b) 40 minutes of training based on “repetitive practice” and “shaping,”37,38 and (c) 10 minutes of standard ADLs activities that were challenging and contextually appropriate.27,28
With regard to repetitive practice, a list of fine motor and manipulative gross motor activities that elicit movement behaviors of interest and include a range of functional and play activities were established to engage the patients in active intervention and to sustain attention and motivation. Specific activities were selected by considering (a) joint movements with pronounced deficits, (b) joint movements that the therapist felt had the greatest potential for improvement, and (c) patient’s preference for activities that have similar potential for improving identified movements. The tasks were made progressively more difficult as the patient improved in performance by increasing speed or accuracy, increasing repetition, or creating performance-sensitive adaptations. Task constraints were adapted to allow success and were removed as one’s performance improved. Task performance was recorded, and task-specific structured feedback was provided for encouragement in a consistent manner. Only positive reinforcement was used. Activities belonged to 1 of 6 categories: board games (eg, Connect Four, Hanoi Tower), card games (eg, poker), manipulative games (eg, dominoes), puzzles, arts and crafts (eg, drawing), and gross motor activities (eg, bowling). Each activity was repeated continuously for approximately 10 minutes. An example of repetitive task practice is the popular game “Connect Four” 37 whose motor components involve grasping the disc, appropriately orienting the disc for placement into a slot, bringing the disc to the top of a grid, and releasing the disc into the appropriate slot. Depending on the patient’s motor capabilities and designated target movements, the game was structured differently to grade the difficulty of a specific movement (eg, as the patient improved, discs were placed differently so that picking them up was more difficult).
On the other hand, shaping is an operant conditioning method, in which a behavioral objective is approached in small steps, by progressively increasing difficulty. Therapists altered constraints to grade tasks according to target movements they wanted the patient to achieve. The strategies includeed varying temporal (eg, time required for the task), spatial (eg, location of the object), and accuracy constraints. Only positive feedback was given to the participant who was always rewarded with enthusiastic approval for improvement, and never blamed or punished for failure.6,29
Control Group Training
Each session consisted of 3 types of exercises involving the paretic arm: (a) 20 minutes of passive mobilization and stretching of the affected, 39 (b) 30 minutes of exercises based on active motility tasks, and (c) 10 minutes of standard ADLs activities, as in the EG.27,28
Testing Procedures
At each research center the same examiner, who was blinded with regard to treatment allocation, evaluated patients enrolled in the study. Patients were specifically asked not to wear the mitt at the evaluation session and it was emphasized that they not discuss their treatment. Examiners were requested to inform their research coordinator if they discovered to which group a patient belonged, and they were periodically questioned by the coordinator about this. To standardize the testing procedures, prior to the start of the study, examiners from all participating centers met and received detailed instructions on how to perform all the clinical tests. Furthermore, a video describing the administration of the Wolf Motor Function Test (WMFT) was given to all the centers participating in the study. Before treatment patients were assessed with the Briggs and Nebes’ laterality inventory, 40 the European Stroke Scale 41 (ESS), and the Barthel Index 42 (BI).
At pretreatment, posttreatment, and at 3-month follow-up patients were assessed by means of primary and secondary outcome measures.
Primary Outcomes
Wolf Motor Function Test (WMFT)
43,44 The WMFT consists of 15 timed arm movement tasks plus 2 strength-based tasks (strength tasks were not included in the study). The quality of movement (WMFT-FA) is scored on a 6-point functional ability scale (0 = does not attempt, 5 = normal movement). The summary score for WMFT-FA is the mean of the scores for each item. Test performance (WMFT-T) measures the time required to complete each task (2 minutes maximum). The summary score for WMFT-T is the median. Minimal clinically important difference values (MCID) for WMFT-FA are as follows: 1.0 point for the affected dominant arm and 1.2 points for the affected nondominant side. MCID for WMFT-T = 19.0 seconds. 45
Motor Activity Log (MAL) 3
A semistructured interview used to assess how the affected arm is used spontaneously to accomplish 30 daily activities outside of the clinical setting (ie, feeding, dressing). For each activity the patient has to rate on a 6-point scale how much (amount of use; MAL-AOU) and how well (quality of movement; MAL-QOM) the activity is performed (0 = worst performance, 5 = best performance). MCID for MAL-QOM and MAL-AOU: 1.0 points for the affected dominant arm and 1.1 points for the affected nondominant side. 44
Secondary Outcome
Ashworth Scale (AS) 46
A validated scale that grades the resistance of a relaxed limb to rapid passive stretch in 5 stages (range score 0-4; 0 = no increase in muscle tone, 4 = joint is rigid in flexion or extension). Paretic arm elbow spasticity was evaluated in our study.
Sample Size
The largest CIMT study is the EXCITE randomized controlled trial. 27 Unfortunately, this study did not report the standard deviation for the raw outcome measure values. However, using the mean values of their outcome measures recorded at the end of treatment for the 2 groups (one treated with CIMT vs a control group), and hypothesizing conceivable standard deviations of approximately 25% of these mean values, we computed the sample size needed for our study. Setting the α level at 5% and β level at 80%, we found that a sample size of 62 patients was needed in terms of WMFT-FA, 4 in terms of WMFT-T, 16 in terms of MAL-AOU, and 24 in terms of MAL-QOM. Since 62 was the value for which all the differences resulted in significant values, we chose a sample size of at least 62 patients. Subsequently, we included 66 patients to take into account possible dropouts.
Statistical Analysis
An intention-to-treat analysis was used. The last observation carried forward method was used to handle the missing data, substituting them with the last available value (a complete case analysis, using only the patients with complete data, was also performed to verify the validity of the results). Since our data were normally distributed (after visual and descriptive inspection), we used parametric tests for inferential statistics. Student t test for independent samples was used to test the homogeneity of the groups before the study. A repeated-measure analysis of variance model was carried out by using “Time” as a within-group factor to evaluate within-group changes over time, “Group” as between-group factor to evaluate the main differences between the 2 groups, and the interaction of Time × Group was evaluated to assess the potential differences between groups in terms of changes over time. Post hoc comparisons were carried out by using a 2-tailed Student t test for unpaired data to assess the significance of the differences between groups for each of the 3 assessments (performed before, after treatment, and at 3-month follow-up). The α level for significance was set at .05 for first level of analysis. The Bonferroni correction was used in multiple comparisons (P < .025). 47 Odds ratio was computed between the EG and CG on the number of patients who demonstrated an improvement that exceeded the MCID.
Statistical analysis was carried out using the SPSS for Windows statistical package, version 16.0. The clinical relevance of changes in the primary outcome scores after treatment and at follow-up was evaluated according to the MCID values estimated by Lang et al. 45
Results
Between March 2007 and December 2008, 66 outpatients were randomized in the EG (n = 34) or CG (n = 32; Figure 1). Four patients in the EG and 3 patients in the CG did not receive the allocated intervention and withdrew from the study (Figure 1). Thus, 59 patients received the experimental (n = 30) or control (n = 29) treatment. At follow-up, 13 patients in the EG and 10 patients in the CG withdrew from the study because of medical complications or uncooperativeness (Figure 1). The dropout rate was quite higher than that hypothesized in the study design. No examiners discovered to which group their patients belonged. Patients’ demographic and clinical characteristics are detailed in Table 1.
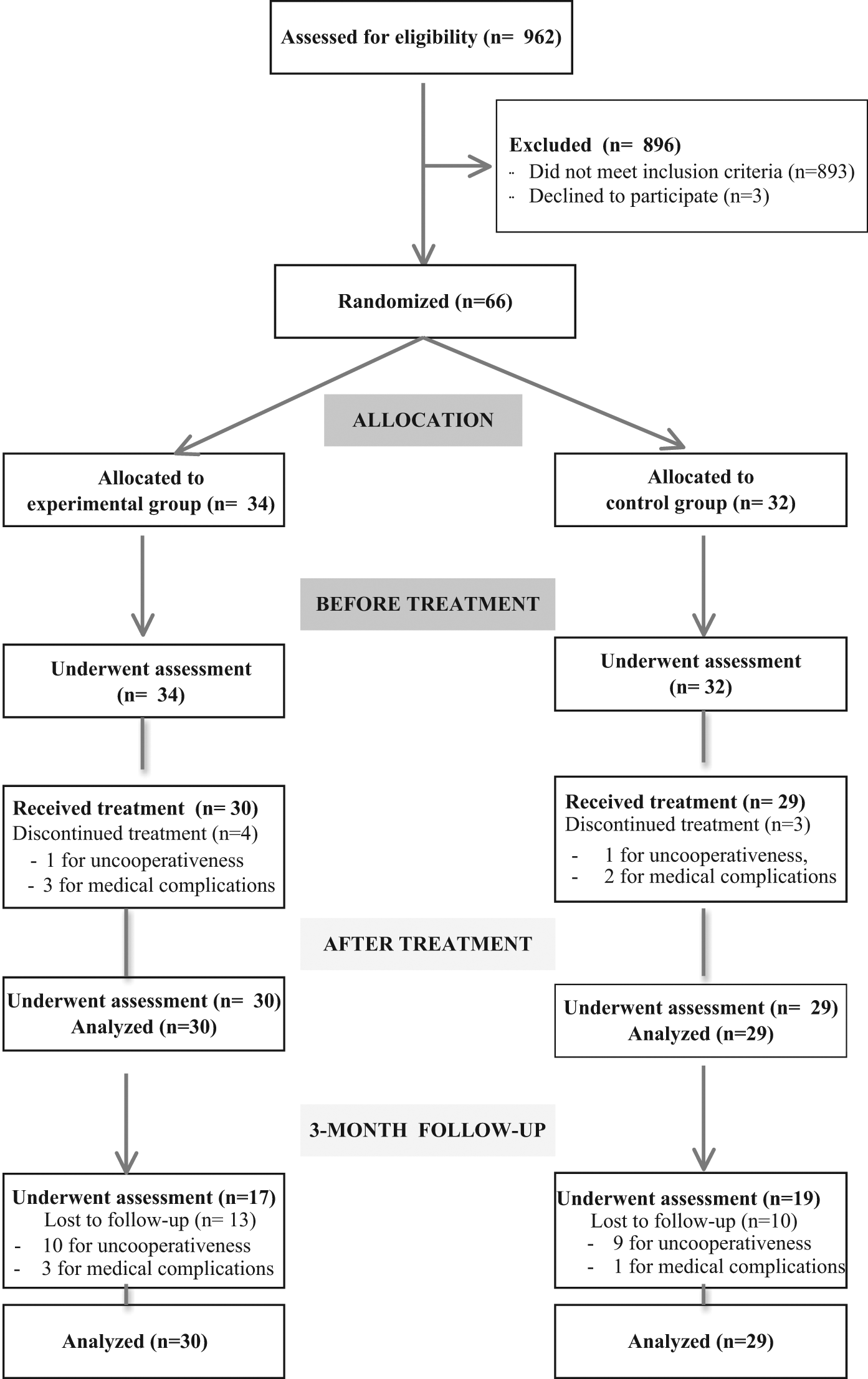
Flow diagram of the study.
Demographic and Clinical Features of the Patient Groups
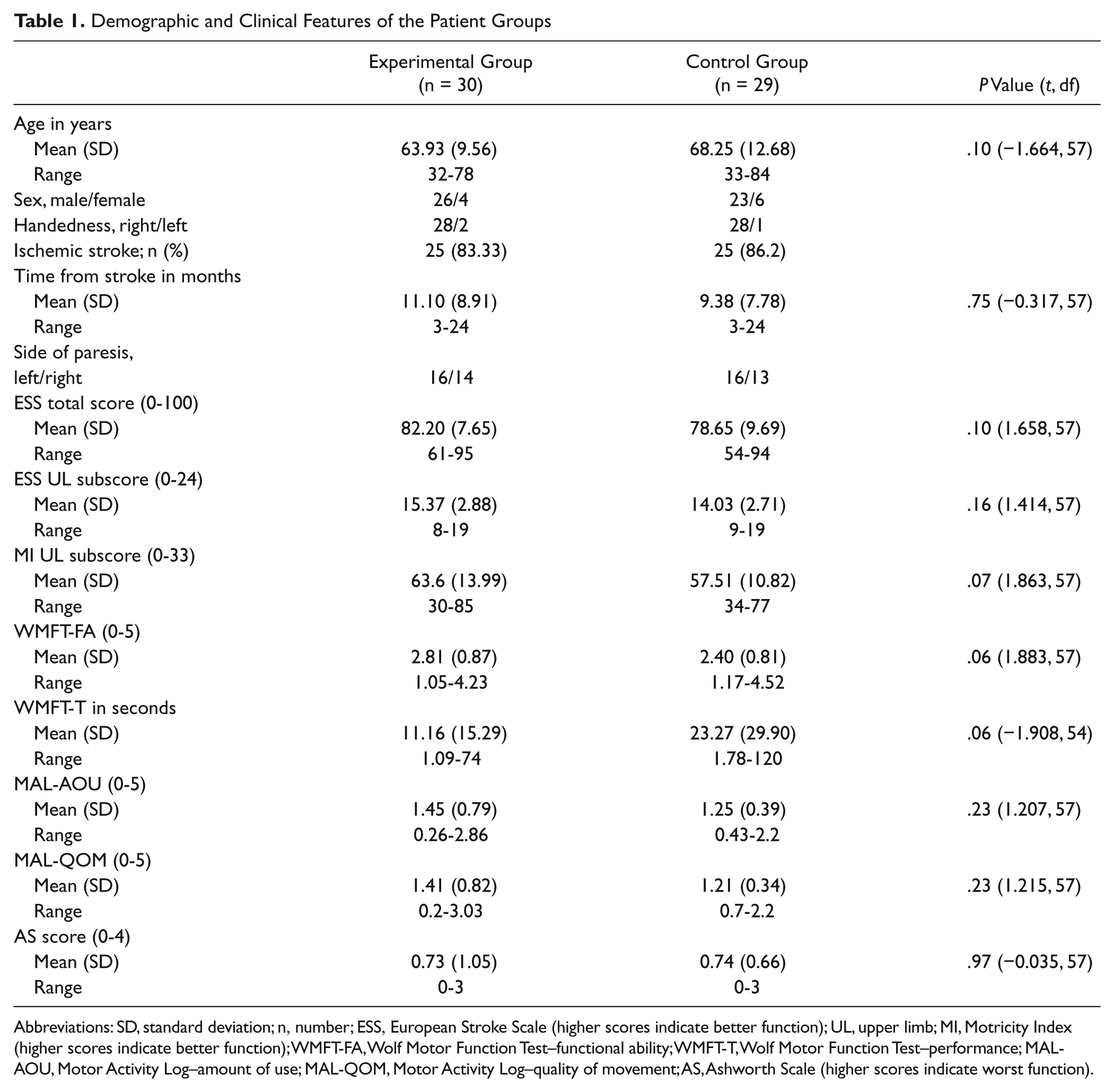
Abbreviations: SD, standard deviation; n, number; ESS, European Stroke Scale (higher scores indicate better function); UL, upper limb; MI, Motricity Index (higher scores indicate better function); WMFT-FA, Wolf Motor Function Test–functional ability; WMFT-T, Wolf Motor Function Test–performance; MAL-AOU, Motor Activity Log–amount of use; MAL-QOM, Motor Activity Log–quality of movement; AS, Ashworth Scale (higher scores indicate worst function).
At the before treatment evaluation, age, education, length of illness, ESS score, ESS upper limb subscore, MI upper limb subscore, MAL-AOU and MAL-QOM scores, and WMFT-FA and WMFT-T were not statistically different between groups (Table 1).
Primary Outcomes
Between-group comparisons showed statistically significant differences for the WMFT-FA (interaction of Time × Group, P = .010), MAL-AOU (P < .001), and MAL-QOM (P < .001). These differences were significant both after treatment (P < .01) and at 3-month follow-up (P < .01).
The interaction of Time × Group was not significant in the WMFT-T probably because of the high standard deviation observed in this parameter Figure 2).
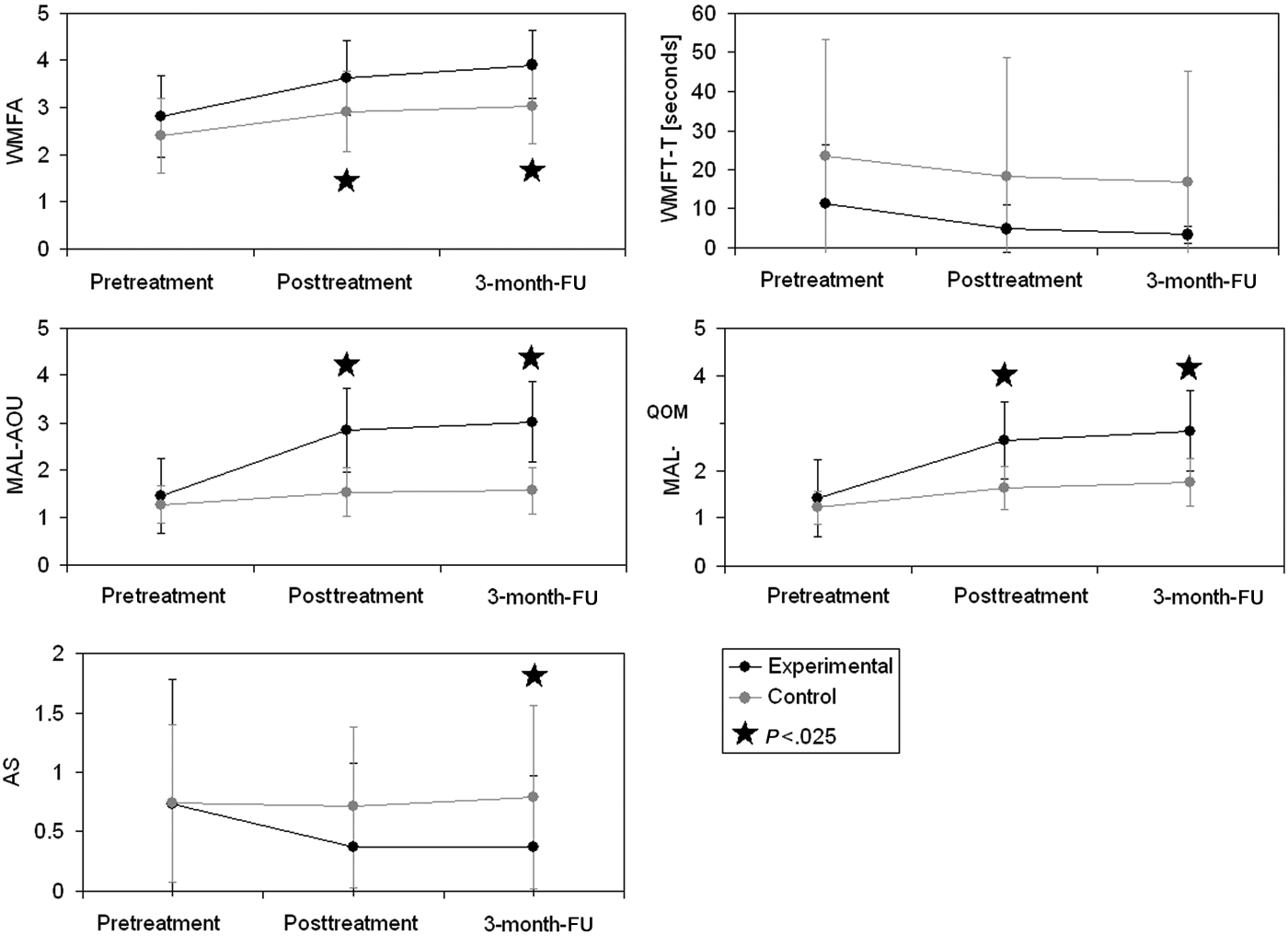
Mean performance and standard errors at primary and secondary outcome measures. Abbreviations: WMFA, Wolf Motor Function Test–functional ability scale; WMFT-T, Wolf Motor Function Test–performance; MAL-AOU, Motor Activity Log–amount of use; MAL-QOM, Motor Activity Log–quality of movement; AS, Ashworth Scale; FU, follow-up.
The standard deviations were similar to that hypothesized during sample size computation for the WMFT-FA and both MAL scores, whereas it was substantially higher than that hypothesized for the WMFT-T. Both groups showed an overall significant improvement in performance on all outcome measures (Table 2 and Figure 2).
Descriptive and Inferential Statistics for All Outcome Measures
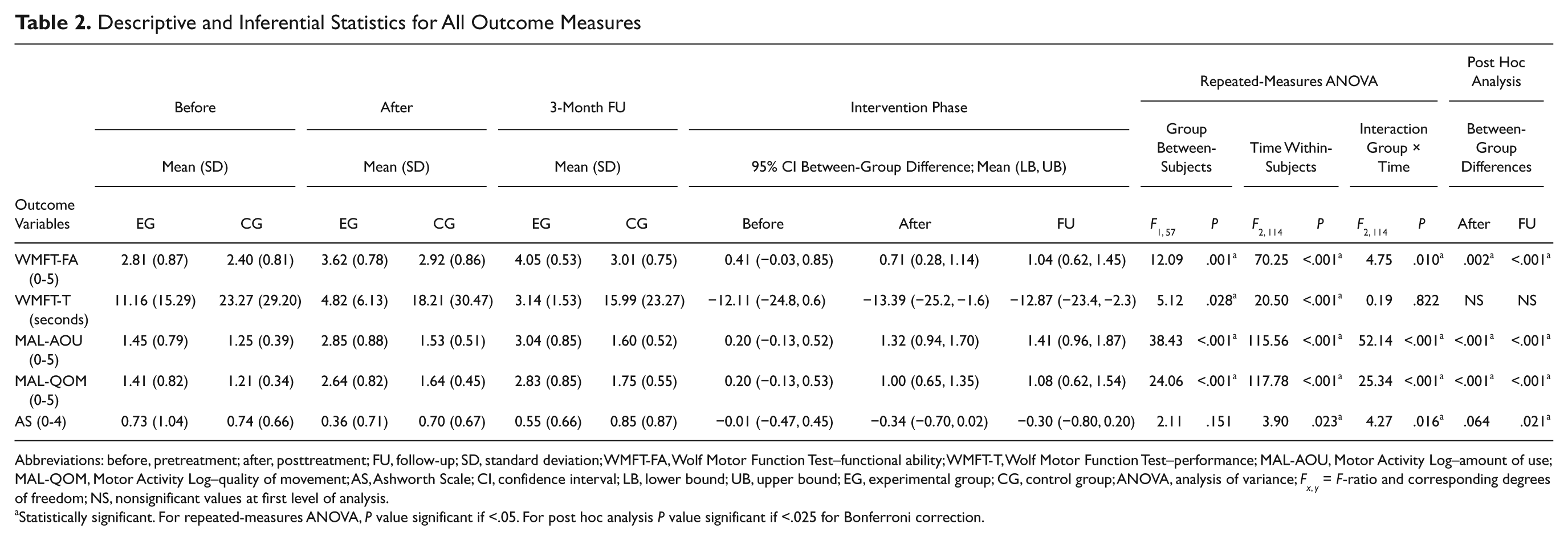
Abbreviations: before, pretreatment; after, posttreatment; FU, follow-up; SD, standard deviation; WMFT-FA, Wolf Motor Function Test–functional ability; WMFT-T, Wolf Motor Function Test–performance; MAL-AOU, Motor Activity Log–amount of use; MAL-QOM, Motor Activity Log–quality of movement; AS, Ashworth Scale; CI, confidence interval; LB, lower bound; UB, upper bound; EG, experimental group; CG, control group; ANOVA, analysis of variance; F x, y = F-ratio and corresponding degrees of freedom; NS, nonsignificant values at first level of analysis.
Statistically significant. For repeated-measures ANOVA, P value significant if <.05. For post hoc analysis P value significant if <.025 for Bonferroni correction.
All results were also confirmed when complete-case analyses were performed.
After the intervention phase the difference found in the EG for WMFT-FA tended to the MCID (0.81 instead of 1.0) whereas at follow-up it was ahead of the estimated score (−1.39). In contrast, the CG did not reach the MCID after the intervention phase or after the follow-up phase. As to WMFT-T, both groups did not achieve the MCID after both the intervention and follow-up phase. With regard to MAL-QOM, the EG achieved the MCID after both the intervention and the follow-up phase, whereas the CG did not reach MCID. Table 3 reports the number of patients who exceeded the threshold defined by MCID with the relevant odds ratios.
Number of Patients Who Exceeded the Minimal Clinically Important Change
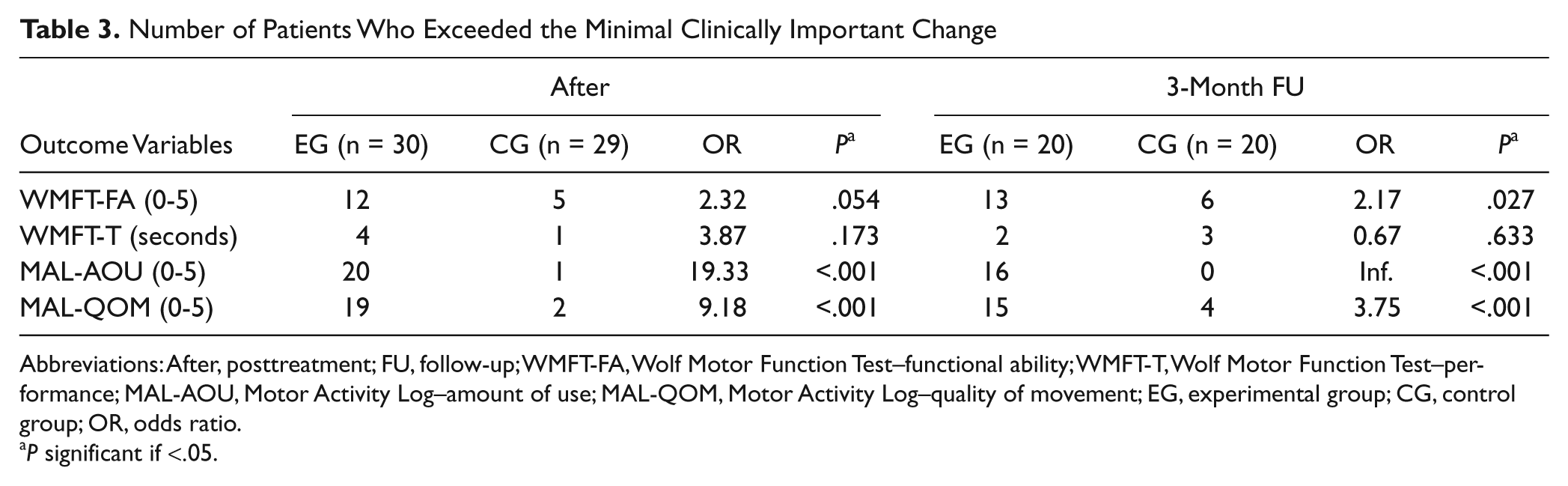
Abbreviations: After, posttreatment; FU, follow-up; WMFT-FA, Wolf Motor Function Test–functional ability; WMFT-T, Wolf Motor Function Test–performance; MAL-AOU, Motor Activity Log–amount of use; MAL-QOM, Motor Activity Log–quality of movement; EG, experimental group; CG, control group; OR, odds ratio.
P significant if <.05.
Secondary Outcomes
Between-groups comparisons showed statistically significant differences in the AS (interaction of Time × Group, P = .016). This difference between groups was significant only at 3-month follow-up (P = .021). However, this significant difference was not found when complete-case analysis was used. The AS revealed a decrease in spasticity in both groups (Table 2).
Discussion
The results of the present study suggested that a mCIMT training program could improve function and use of the affected arm more than a conventional rehabilitation program in outpatients with chronic stroke. In the past 2 decades this field of rehabilitation research has focused mainly on verifying the effects of traditional CIMT protocols.9,21 However, in many countries, the scarce resources allocated to rehabilitation services by health care systems limits the applicability of such an intensive training. Therefore, mCIMT protocols consisting of a reduced restraint time and/or a shortened training period (reduced duration of each single session or reduced sessions frequency) have been put forward.9,11-13,15-19
A Cochrane review taking into account the effects of both types of CIMT protocols (traditional CIMT and mCIMT) showed an overall improvement in arm motor function and use (amount of use and quality of use) as a main outcome. 9 On the contrary, no effect on quality of life was found. Also, this review showed a reduction of the patient’s disability after treatment although it did not persist in the long term. 9 Authors suggested that future studies should include high-quality RCTs with larger sample sizes and that the long-term effect of treatment should be evaluated. 9
A recent systematic review 13 comparing the effects of mCIMT protocol versus traditional rehabilitation included 13 RCTs, involving 278 patients. Results showed that patients receiving mCIMT had higher scores in terms of arm function tests (Fugl-Meyer Assessment and Action Research Arm Test) and on the MAL-AOU and MAL-QOM. The authors concluded that mCIMT could be a feasible alternative intervention for patients with arm dysfunction after a stroke. However, they highlighted that most of the trials included in the review had small sample sizes and that there were shortcomings in the methodological quality in the selected studies. 13 Indeed, some studies did not describe the randomization process and allocation concealment was unclear in most studies, with only a partial use of blinding. 13
An additional study, not included in the previous review, is a large mCIMT RCT performed by Wu et al 18 aimed at comparing the efficacy of distribuited CIMT, bilateral arm training (BAT), and control treatment (CT) mainly based on neurodevelopmental treatment. Sixty-six patients with chronic stroke were randomized to receive mCIMT (n = 22), BAT (n = 22), or CT (n = 22). Each group received treatment for 2 h/d, 5 d/wk for 3 weeks. The mCIMT group used a mitt to restrict the unaffected hand for 6 hours per day and intensively trained the affected arm in functional tasks. Outcome measures included the WMFT, the MAL, and kinematic variables during unilateral and bilateral tasks. After treatment, the mCIMT group had decreased WMFT scores and higher functional ability scores than CT patients. Furthermore, the mCIMT group demonstrated a better performance in the affected arm amount-of-use and quality-of-movement scores (MAL) than the BAT and CT groups. As to kinematic variables, the BAT and mCIMT groups had better performance on movement smoothness than the CT group. However, the BAT group generated greater force at movement initiation than both the mCIMT and CT groups. The study by Wu et al 18 confirms that an mCIMT protocol may be more appropriate to improve functional ability and use of the affected arm compared to BAT or treatment mainly based on neurodevelopmental treatment (CT) or BAT. However, as in many CIMT and mCIMT studies, the lack of a follow-up assessment did not allow the long-term persistence of the superiority of the mCIMT protocol used by Wu et al.
The present study suggests the efficacy of mCIMT protocol, in accordance with the findings of the aforementioned studies. Moreover, it is 1 of the largest 2-arm RCTs to compare the effects of a mCIMT protocol with those of conventional arm rehabilitation in patients with stroke. Furthermore, this research was designed to be one of the few studies that included a follow-up assessment (at 3 months after treatment). Unfortunately, the strength of our results at follow-up was limited by the high dropout rate.
An additional feature of the present study is that the improvement of the EG reached a value higher than the MCID for MAL-scores. 45 Moreover, the odds ratio was greater than 2 for all the primary outcome measures, apart from the WMFT-T, in EG compared with the CG. This means that patients in this study treated with mCIMT were 2 times more likely to experience an improvement that can provide a perceivable benefit in their life in terms of motor and functional abilities than the CG. On the other hand, the time to execute a task was not importantly improved in both groups, without significant differences between them. It is difficult to compare the previous mCIMT studies with the present RCT because of some relevant methodological differences. The first main discrepancy is that the amount of restraining time during waking hours was generally lower compared to our study (5-6 h/d vs 12 h/d in our study). The only exception is the study by Boake et al, 21 where the restraining time was 90% of waking hours. 9 However, in that study patients received an additional hour of daily treatment (3 h/d vs 2 h/d in our study) and were both inpatients and outpatients. A second remarkable difference from previous studies consists of the type of activities used to train the paretic arm. Indeed, activities varied consistently among the studies, ranging from ADL activities, functional tasks, shaping, to proprioceptive muscular facilitation stimulation.9,12
A drawback of the present study is that because of the different types of training performed in the EG and CG (mCIMT vs conventional rehabilitation), neither the specific effects of treatment intensity (2 h/d vs 6 h/d in the traditional CIMT) nor the effect of the restraining procedure per se, could be tested. However, this was not the aim of the present study. Indeed, we intended to compare the effect of a reduced intensity mCIMT program with the effects of a conventional rehabilitation program used in Italy.
The main limitations of this study are the lack of a long-term (6 months and 1 year) follow-up, the high rate of patient dropout at the 3-month follow-up, and the lack of outcome measures of disability. Regarding the dropout rate, it was quite higher than that hypothesized in the study design as some patients did not perform the follow-up evaluation. Indeed, during the intervention phase, the dropout rate was lower because patients and their caregivers were very motivated for rehabilitation. In contrast, they lacked motivation to travel to the rehabilitation center just to perform the clinical evaluation at follow-up. This high dropout rate at follow-up did not allow us to make any meaningful interpretations regarding influence of mCIMT on spasticity, since the last observation carried forward method suggested a significant result but complete-case analyses did not. Further studies are needed to address if mCIMT can modify spasticity differently than conventional rehabilitation.30,31 Another weakness of the present study is the lack of a detailed patient diary to monitor the intensity of the household training. To conclude, the results of the present study suggest that the mCIMT protocol used may be more effective compared with conventional rehabilitation in patients with chronic stroke. Further studies are required to compare the effects of mCIMT programs with traditional CIMT and to investigate the very long-term effects of this rehabilitative procedure.
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.