
Abstract
Background. Spatial neglect is a debilitating disorder for which there is no agreed on course of rehabilitation. The lack of consensus on treatment may result from systematic differences in the syndrome's characteristics, with spatial cognitive deficits potentially affecting perceptual-attentional “Where” or motor-intentional “Aiming” spatial processing. Heterogeneity of response to treatment might be explained by different treatment impacts on these dissociated deficits: prism adaptation, for example, might reduce Aiming deficits without affecting Where spatial deficits. Objective. Here, we tested the hypothesis that classifying patients by their profile of Where-versus-Aiming spatial deficit would predict response to prism adaptation and specifically that patients with Aiming bias would have better recovery than those with isolated Where bias. Methods. We classified the spatial errors of 24 subacute right stroke survivors with left spatial neglect as (1) isolated Where bias, (2) isolated Aiming bias, or (3) both. Participants then completed 2 weeks of prism adaptation treatment. They also completed the Behavioral Inattention Test and Catherine Bergego Scale (CBS) tests of neglect recovery weekly for 6 weeks. Results. As hypothesized, participants with only Aiming deficits improved on the CBS, whereas those with only Where deficits did not improve. Participants with both deficits demonstrated intermediate improvement. Conclusion. These results support behavioral classification of spatial neglect patients as a potential valuable tool for assigning targeted, effective early rehabilitation.
Keywords
Introduction
Spatial neglect is a debilitating cognitive disorder in which impaired contralesional response, reporting, or action causes functional disability. 1 Stroke survivors with neglect experience longer hospitalizations and poorer rehabilitation outcomes.2,3 Although treatment may reduce neglect severity,3,4 there is no consensus as yet on the best clinical standards for rehabilitation to restore daily life function. 5
Studies of neglect treatment might yield conflicting findings regarding its efficacy because treatments may differently affect distinct brain-based spatial processing systems. 6 Because neglect may result from deficits in one or more brain-behavior systems supporting different stages of spatial-cognitive information processing,1,7 considering its taxonomy should be an early step in designing treatment trials. Both group assignment and outcome measures must be designed to be sensitive to differences in neglect subtypes. We are unaware of any spatial neglect treatment trials designed to take deficit profiles into account: this may have reduced the ability of prior neglect studies to detect treatment effects.
Classification of spatial neglect deficits is based on analyzing abnormal spatial behaviors and can be laboratory based, but it is also relevant to examination at the bedside.1,7 Impairment of input-related stages of information processing may lead to deficits in the spatial distribution of attention and perception, affecting stimulus encoding: These are Where spatial deficits. They include difficulty with contralesional perceptual awareness, difficulty focusing or disengaging spatial attention, and a reduced capacity to allocate perceptual resources across the entire spatial field.8-10 Impairment at output-related stages disturbs spatial action planning and execution.1,7,11,12 These are motor-intentional, or Aiming, deficits, which can potentially affect the limbs, body, and eyes. 11 They include impairment of movement of the contralesional body (limb akinesia); impairment in the gain, duration, or force of movements in contralesional space referenced to body center (hemispatial hypokinesia); and impairment of contralesionally directed movements performed in either the contralesional or ipsilesional space (directional hypokinesia).
Prism adaptation is a promising spatial neglect treatment reported to exert long-lasting benefits that generalize beyond the laboratory to self-care, navigation, and other functional tasks.13-18 Nevertheless, not all efficacy studies reported that neglect improved with prism treatment.19,20 Even in responsive patients, prism adaptation therapy (PAT) may not ameliorate all neglect symptoms: this may be related to a specific effect of PAT on Aiming, but not Where, bias.6,18,21 Using a computerized line bisection task that separately quantifies Where and Aiming spatial biases, 22 we demonstrated that 5 participants with left neglect experienced an improvement in Aiming bias after 2 sessions of PAT, with no reliable change in Where bias. 18 This specific effect of prism adaptation on Aiming bias was also observed in a large group of neurologically healthy individuals. 21
The current study addressed a major block in translation of prism adaptation to the clinical setting. We asked whether classifying patients by their spatial deficit profile (Where vs Aiming) predicted improvement following PAT. Neglect patients completed a computerized line bisection task for assessing their Where and Aiming spatial biases prior to 2 weeks of PAT, allowing for classification based on their baseline deficit. The Behavioral Inattention Test (BIT) 23 and the Catherine Bergego Scale (CBS)24,25 were administered weekly thereafter for a total of 6 follow-up assessments. Because prism adaptation may specifically target Aiming bias in neglect,18,21 we hypothesized that participants with Aiming deficits would show greater improvement than those with isolated Where deficits.
Methods
The study was approved by the institutional review boards of the Kessler Foundation and Seton Hall University.
Participants
A consecutive sample of 24 right-brain-damaged persons with stroke was recruited from inpatient rehabilitation hospitals. The participants (17 men; 7 women; aged 30 to 90 years, all premorbidly right-handed) were screened for neglect and hemianopia 6 to 47 days poststroke (see Neglect Assessment). Patients demonstrating rightward error on the computerized line bisection task and presenting with spatial neglect (BIT ≤ 129 or CBS > 1) were included. Patients more than 60 days poststroke, with left-hemisphere lesions, a prior history of neurological or psychiatric conditions, or uncorrected ocular disorders were excluded. Patients with leftward line bisection error were also excluded because these errors suggest ipsilesional neglect, which may be associated with different clinical and recovery characteristics.26,27
Participants received PAT once daily for 10 days, using the procedure described in Chen et al. 28 Each PAT session lasted 15 to 20 minutes.
Computerized Line Bisection: Where and Aiming Bias Assessment
Participants performed computerized line bisection prior to PAT. Sitting at a computer monitor, they bisected 32 horizontal lines (subtending 23.6° of visual angle) under normal and reversed viewing conditions. Lines appeared centrally, one at a time, and participants clicked on the line’s center using a wireless mouse. A participant’s direct view of the hand was prevented by a cardboard shelf. Thus, they needed to watch the monitor for visual feedback. Under normal viewing, the cursor on the monitor moved in the same direction as the mouse. Under reversed conditions, visual feedback was left-right reversed, such that rightward movements of the mouse resulted in leftward movements of the cursor and vice versa. This task has demonstrated research utility and construct validity to assess Where and Aiming bias in neglect patients10,18 and healthy controls.22,29 Participants’ line bisection error across 16 normal and reversed trials was averaged and fractionated into Where and Aiming components (mm equivalents) as follows10,18,21,22,29:


Neglect Assessment
Neglect was assessed with the BIT 23 and CBS (via the Kessler Foundation-Neglect Assessment Process) 25 at study entry (screening, session 1), reassessed just prior to PAT (baseline, session 2), and then weekly thereafter for 5 weeks, for a total of 6 postscreening assessments. The BIT-Conventional is a paper-and-pencil test consisting of 6 subtests: line crossing, letter cancellation, star cancellation, figure/shape copying, line bisection, and representational drawing (higher scores indicate better function). 23 The CBS assesses neglect-specific functional impairment (eg, dressing the left side of the body and eating from the left side of a plate). 24 It was completed by occupational therapists, blinded to the purpose of the study and trained for reliability by our research staff, who rated participants’ performances for left-sided stimuli and actions (10 items, scored on a 0 to 3 scale, with 0 indicating no neglect and 3 indicating severe neglect). 25 Lower scores indicate better function.
Data Analysis
As recently emphasized, 30 a major translational block for valid neglect treatment research is the widespread use of statistical techniques that are inappropriate for analyzing longitudinal trajectories of improvement in heterogeneous subject groups for whom there is high within-subject intracorrelation of dependent measures. To avoid this pitfall, participants’ recovery trajectories were analyzed with mixed linear modeling (MLM) using STATA/IC 12.1. 31 The primary analytical goal was to determine whether classifying patients on the basis of Where and Aiming biases predicted neglect improvement following PAT (ie, sessions 2 through 7). Thus, participants were coded as to whether they had a rightward Where bias (Where bias greater than zero) and whether they had a rightward Aiming bias. Participants’ bias type was then categorized: isolated Where bias (n = 7), isolated Aiming Bias (n = 5), or both Where and Aiming biases (n = 12). Group equivalence was tested prior to treatment with nonparametric Kruskal-Wallis tests on the screening characteristics.
Estimating Spontaneous Recovery Rate
The analyses took into account the possible confounding effects of spontaneous recovery using an estimate of each participant’s spontaneous recovery rate between the screening (session 1) and baseline (session 2) assessments. Session 1 occurred within 48 hours of participants’ consenting and Session 2 just prior to PAT, with an average of 15 days between (SD = 6.02). Separate spontaneous recovery rates on the BIT and CBS were calculated for each participant:
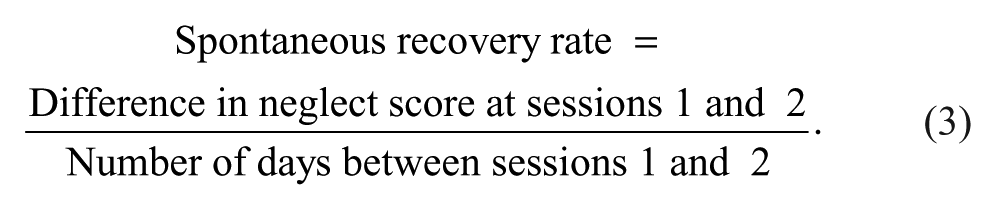
Higher values on this measure indicate greater per-day improvement between sessions 1 and 2.
MLM Analyses
The MLM used an unstructured covariance structure and maximum likelihood estimation, and it included participants’ random intercepts and slopes. 32 The F distribution with between-within denominator degrees of freedom was used to assess the significance of fixed-effects parameters.30,33
The predictors of theoretical interest were the effects of bias type and the bias type by session interaction. The covariates were participants’ spontaneous recovery rate and its interaction with assessment session (2 through 7). Preliminary analyses identified potential additional covariates by separately testing the ability of age, gender, days poststroke, lesion volume, and baseline deficit (as assessed at screening) to predict the CBS and BIT on their own. Variables that acted as significant predictors when entered on their own were introduced as potential covariates.
We predicted that participants with Aiming bias would experience more improvement. Thus, the Aiming-only and Aiming + Where groups were expected to improve more than the Where-only group (ie, a bias type by assessment session interaction). If this interaction were observed, planned orthogonal contrasts of the linear recovery trajectories would specifically test the hypothesis: one contrast comparing the 2 groups with Aiming bias with the Where-only group and a second comparing the Aiming-only with the Aiming + Where group.
Lesion Mapping
Participants underwent standard clinical radiological exams (MRI and/or CT). Lesions were evaluated by selecting brain scans showing the greatest lesion extent. Lesion borders were manually mapped from clinical scans onto transverse brain images in MRIcro and then transposed to the standard brain template using a combination of MRIcro and Montreal Neurological Institute space. 34 A “double-strain” lesion mapping was performed. 34 Three technicians, blinded to patients’ behavioral classifications, manually mapped out individual lesions, followed by conferencing with an independent neurologist to ensure accuracy. Finally, 2-dimensional MRIcro maps were transformed to 3-dimensional maps (voxel of interest format) using MRIcron. Lesion location was identified using an anatomical checklist, and lesion volume (voxels) was calculated from the lesion map. The normalized lesion images were used for subsequent group overlap in MRIcro. 35
Results
See Table 1 for participant characteristics at screening and Figures 1 to 3 for their lesion maps. The groups differed in average age, with Where-only older than both Aiming-only (P = .019) and Aiming + Where (P = .018) participants, who did not differ (P = .752). The groups also differed in their Aiming and Where bias, as expected.
Median Participant Characteristics at Screening as a Function of Bias Type. a
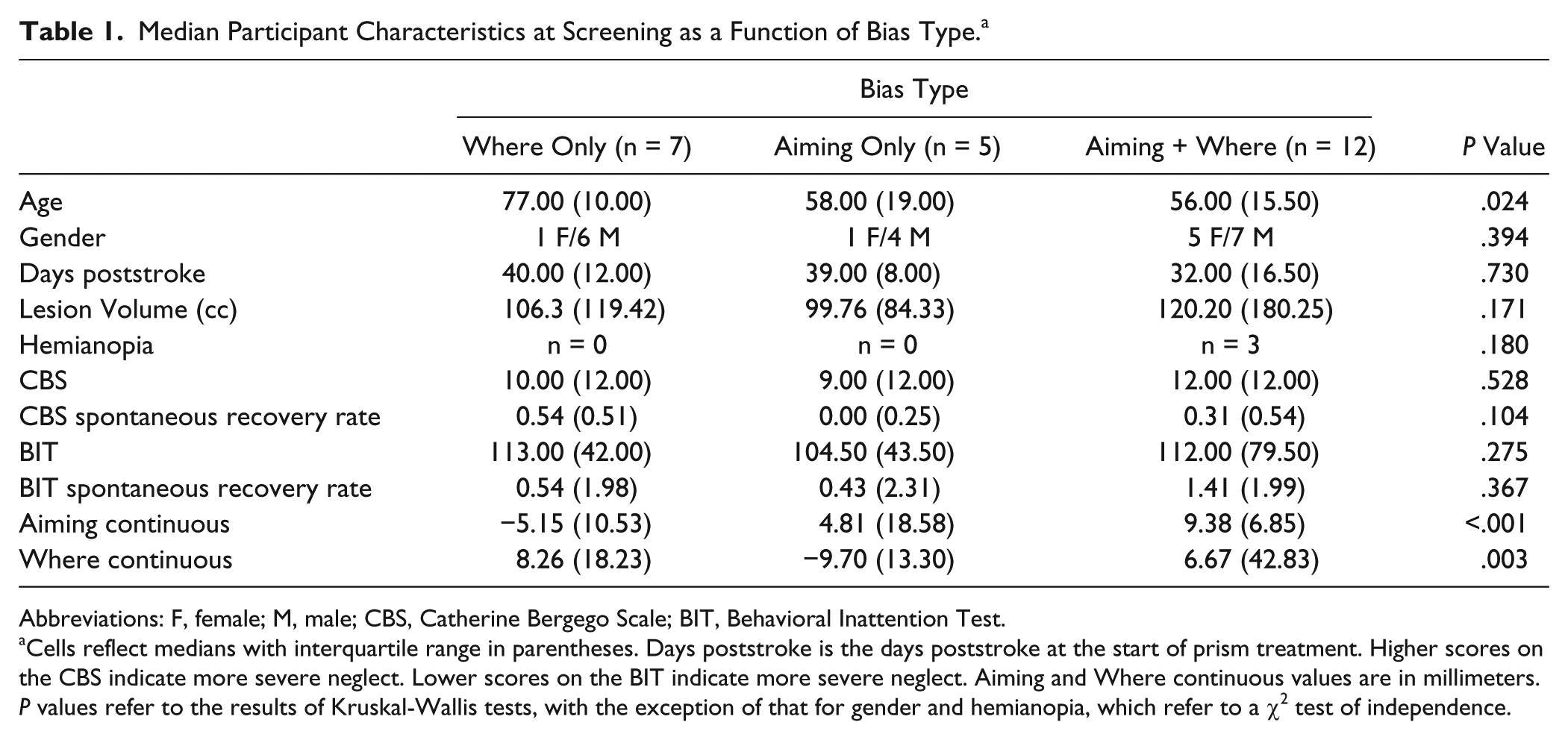
Abbreviations: F, female; M, male; CBS, Catherine Bergego Scale; BIT, Behavioral Inattention Test.
Cells reflect medians with interquartile range in parentheses. Days poststroke is the days poststroke at the start of prism treatment. Higher scores on the CBS indicate more severe neglect. Lower scores on the BIT indicate more severe neglect. Aiming and Where continuous values are in millimeters. P values refer to the results of Kruskal-Wallis tests, with the exception of that for gender and hemianopia, which refer to a χ2 test of independence.
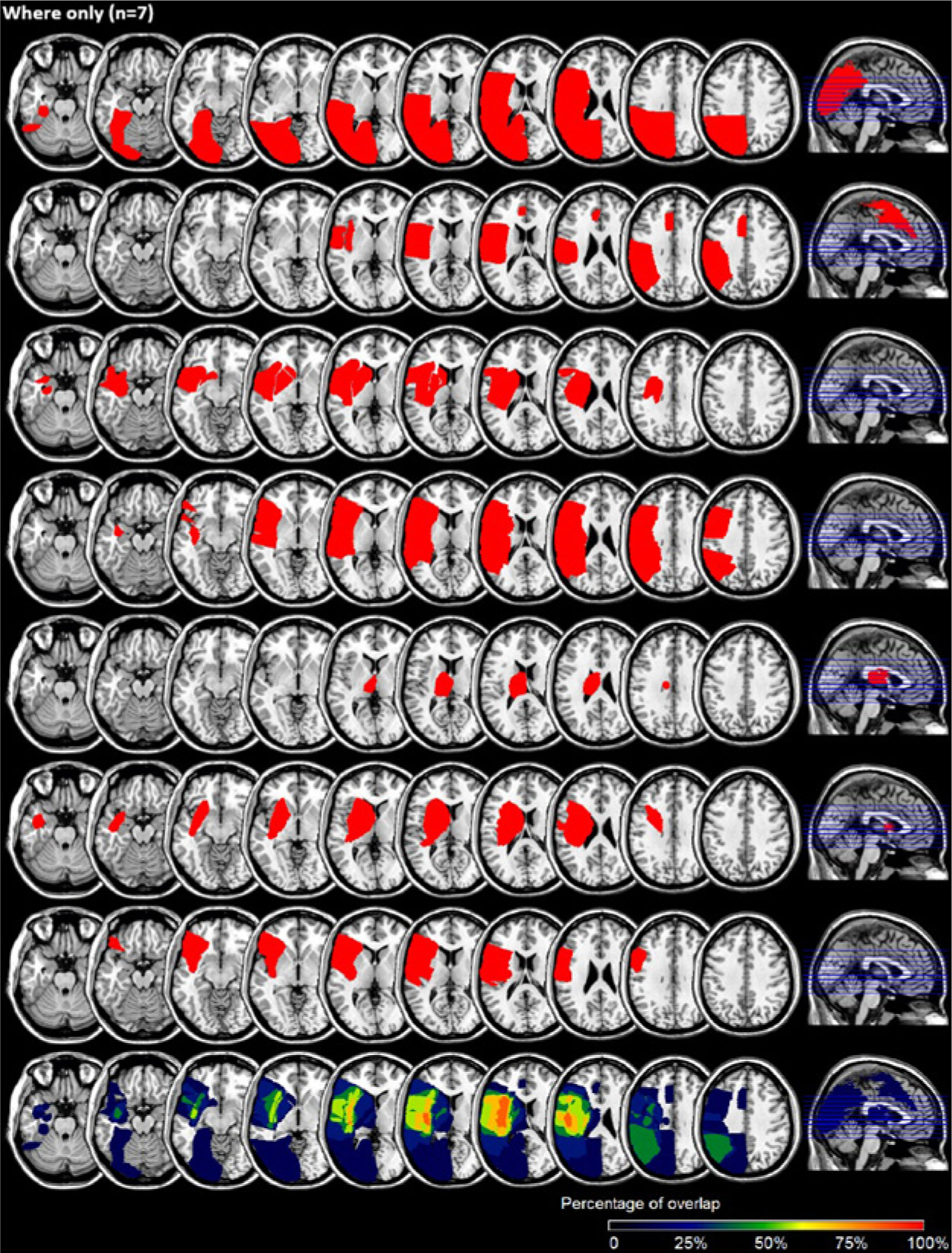
Individual lesions (rows 1-7) and group overlap (row 8) for Where-only participants (n = 7).
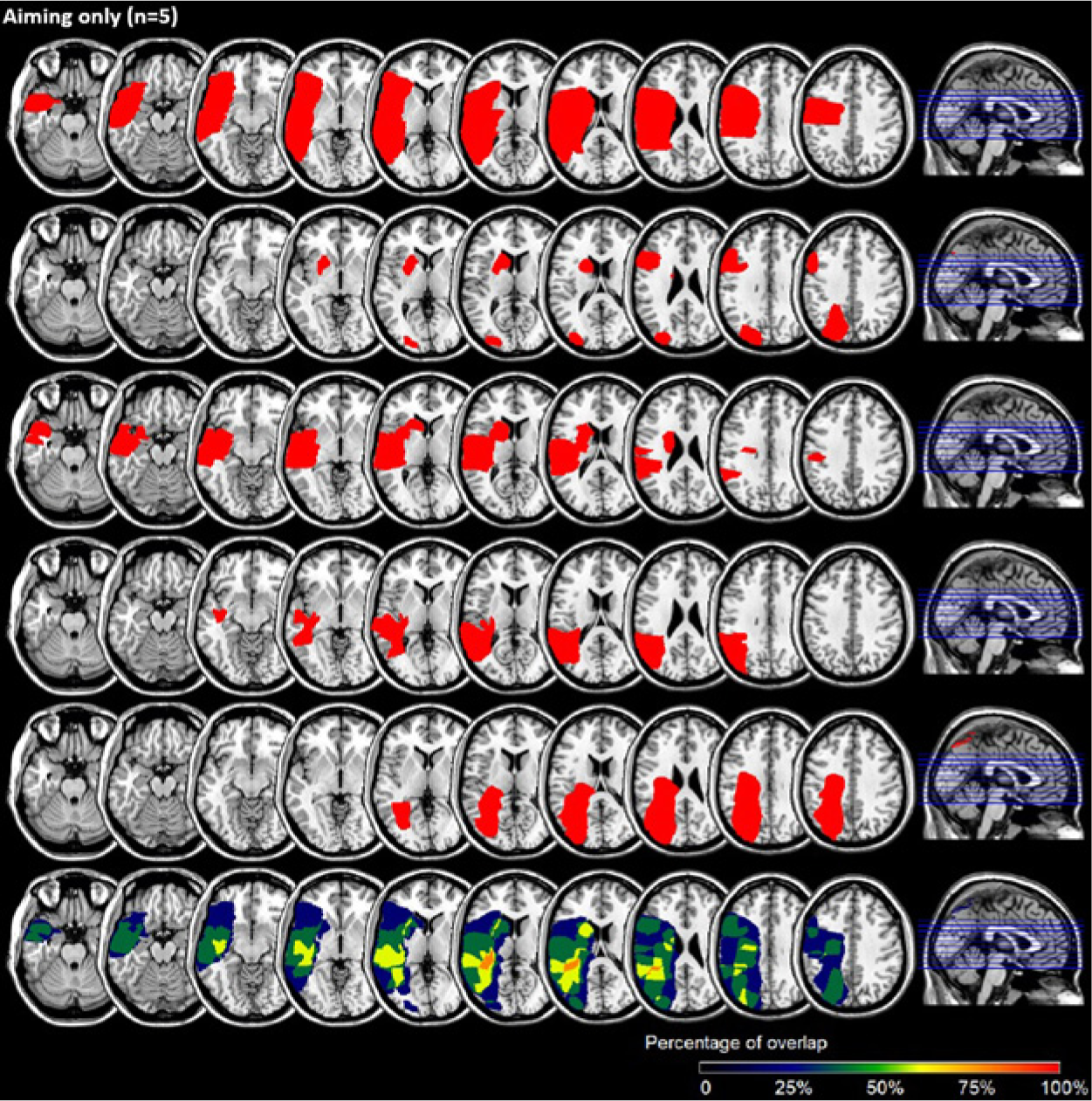
Individual lesions (rows 1-5) and group overlap (row 6) for Aiming-only participants (n = 5).
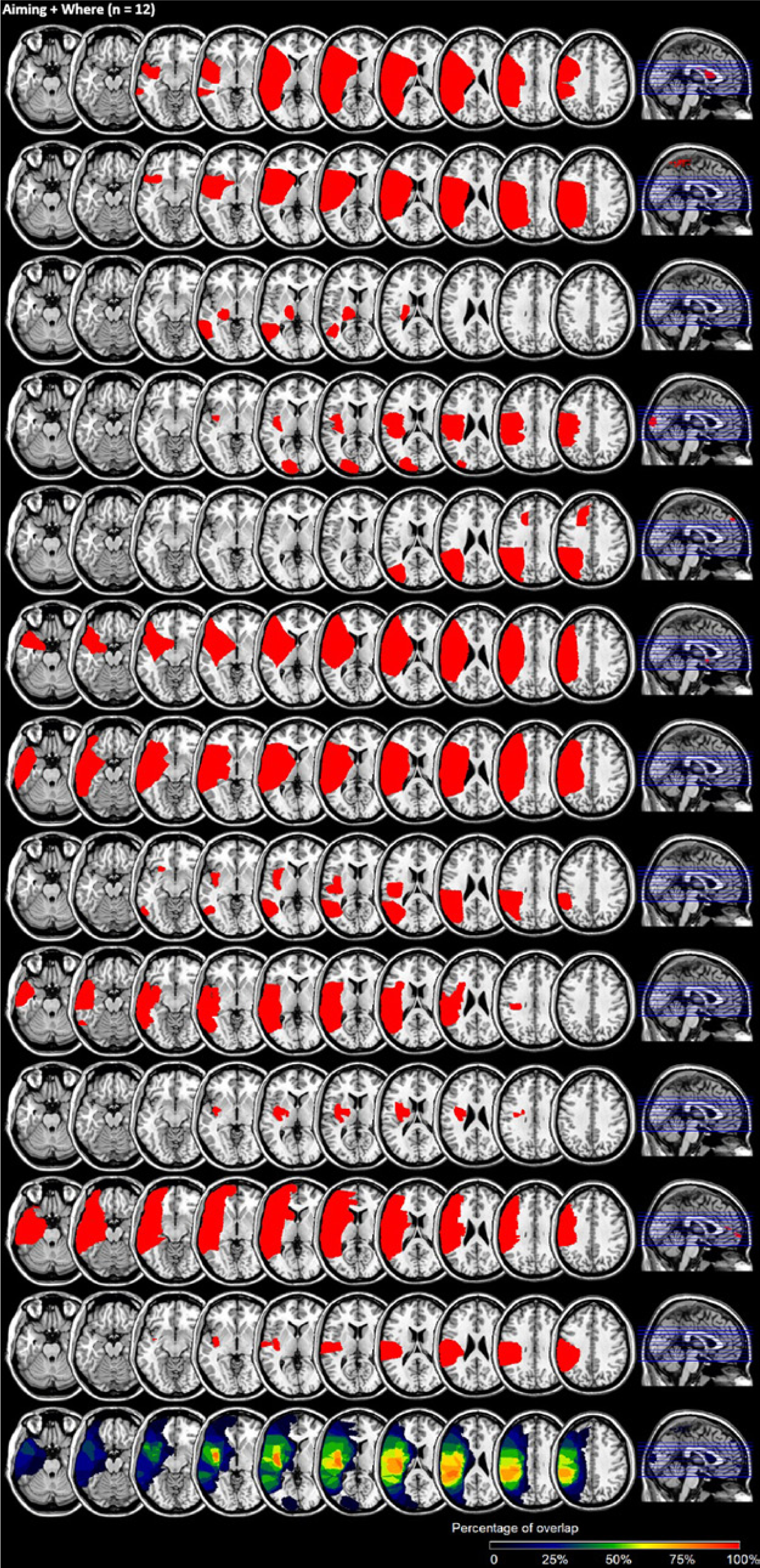
Individual lesions (rows 1-12) and group overlap (row 13) for Aiming + Where participants (n = 12).
MLM Predicting CBS
CBS scores were positively skewed and nonnormal (joint test of normality in skewness and kurtosis: χ2(2) = 0.33; P < .009. Taking the square-root transform improved the distribution’s shape: χ2(2) = 2.79; P = .248. Therefore, all analyses were performed with the square-root transformed CBS. For ease of interpretation, figures reflect CBS scores transformed back into their original scale.
CBS scores showed high within-subject correlation across sessions (intraclass correlation coefficient [ICC] = 0.67). The preliminary MLM analyses to identify potential covariates revealed that both age (P = .008) and baseline CBS (P < .001) predicted average CBS performance across assessment sessions 2 through 7, whereas gender (P = .630), days poststroke (P = .539), and lesion volume (P = .171) did not. Thus, age and baseline deficit were entered as covariates into the main analysis. Additionally, because residual diagnostics revealed heteroskedasticity among the different bias types, the MLM used a residual covariance structure that allowed different variances for each bias type. 33
Results of the analysis are depicted in Table 2. Consistent with our hypothesis, there was an interaction between bias type and session (Figure 4). Planned contrasts showed that the Aiming-only and Aiming + Where participants differed significantly from the Where-only participants (z = −2.60; P = .009) but not from each other (z = −1.02; P = .306). Aiming-only participants had the steepest linear recovery (β = −0.56; b = −0.41; standard error [SE] = 0.17; confidence interval [CI] = −0.73, −0.08; z = −2.44; P = .015), whereas Where-only participants had a slope that did not differ from zero (β = −0.11; b = −0.08; SE = 0.17; CI = −0.42, 0.24; z = −0.52; P = .516). Participants with Aiming + Where bias had an intermediate slope (β = −0.41; b = −0.30; SE = 0.16; CI = −0.61, 0.01; z = −1.89; P = .058). These results support our hypothesis: participants with a rightward Aiming bias showed greater improvement with PAT.
Fixed-Effect Predictors and Covariates for Predicting the Square-Root Transformed CBS Across Assessment Sessions 2 Through 7. a
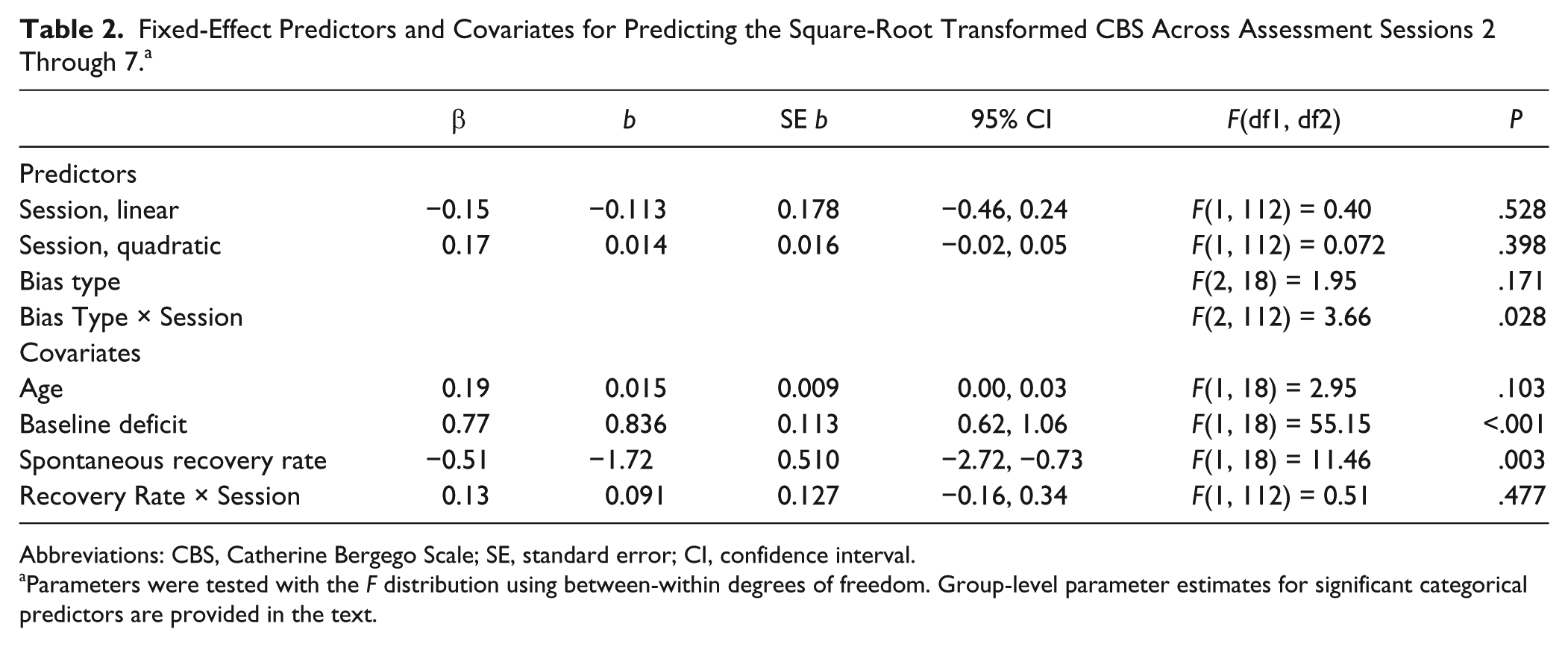
Abbreviations: CBS, Catherine Bergego Scale; SE, standard error; CI, confidence interval.
Parameters were tested with the F distribution using between-within degrees of freedom. Group-level parameter estimates for significant categorical predictors are provided in the text.
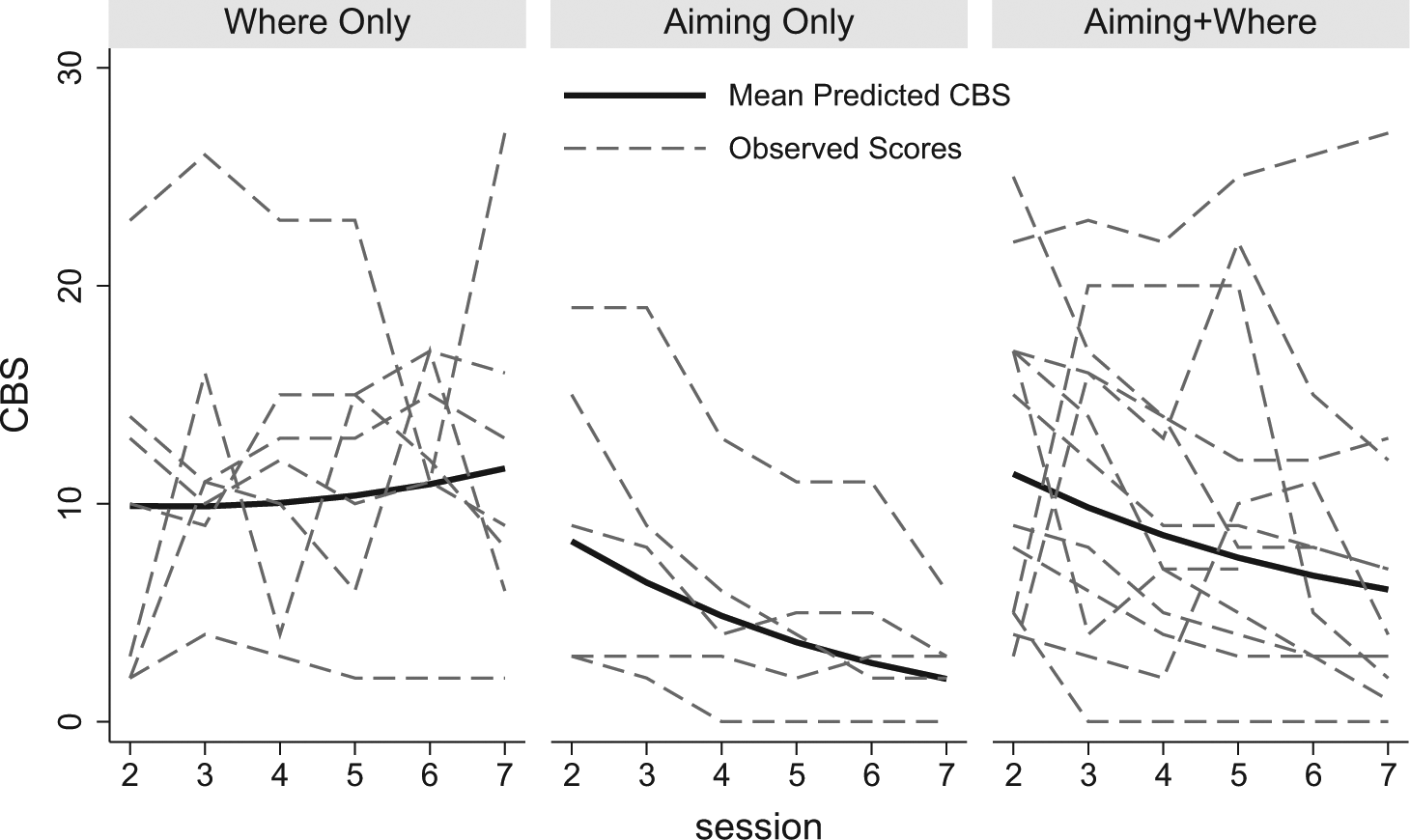
Participants’ observed CBS scores (dashed lines) and average model predicted CBS scores (thick, solid lines) across assessment sessions for each of the 3 bias types: 1 week separated each session. Assessment session 2 occurred just prior to prism treatment; 1 week of prism treatment occurred between sessions 2 and 3 and another between sessions 3 and 4. Lower scores indicate better performance (less severe neglect).
There were also main effects of baseline CBS and spontaneous recovery rate on the average CBS score across all sessions (Table 2). Participants with poorer CBS scores at screening tended to have poorer CBS scores averaged over sessions 2 through 7. Participants with greater recovery before PAT tended overall to have better CBS scores across assessments 2 to 7. The lack of significant interaction between spontaneous recovery rate and session indicates that spontaneous recovery, as assessed prior to the treatment, did not predict change after PAT.
Alternate Explanations for CBS Improvement
Although the a priori criterion for inclusion of potential covariates was that they independently predict CBS over assessment sessions, post hoc analyses were performed to exclude the alternate explanations that potential group differences in age or lesion volume accounted for the differential improvement among the bias types. An MLM with the effects of age, bias type, session, and the bias type by session and age by session interactions revealed a nonsignificant age by session interaction (P = .508) but significant bias type by session interaction (P = .050), with slopes for each bias type similar to those in the main analysis. Thus, the differential improvement among the bias types cannot be attributed to age-related changes: Age did not predict improvement across assessments, but controlling for age-related improvements, bias type continued to predict improvement across the assessments.
A similar MLM tested for the effects of lesion volume. The lesion volume by session interaction did not reach significance (P = .133), but the bias type by session interaction did (P = .003), with slopes for each bias type similar to those observed in the main analysis. Thus, the differential improvement observed for the bias types cannot be attributed to lesion-volume-related improvements in CBS scores.
MLM Predicting BIT
Preliminary analyses revealed that BIT scores were significantly nonnormal (joint test of normality in skewness and kurtosis: χ2(2) = 16.34; P < .001). No transformation improved the shape of the distribution. Therefore, analyses of the BIT used bootstrapped estimates of the SEs. A limitation of this method is that it does not allow for modeling of random slopes (only random intercepts).
As with the CBS, there was high within-subject correlation of BIT scores (ICC = 0.91). Preliminary MLM analyses to identify potential covariates identified only baseline BIT as a significant predictor of averaged BIT performance (P < .001), whereas gender (P = .355), days poststroke (P = .082), lesion volume (P = .597), and age (P = .142) were not. Although age did not significantly predict BIT scores on its own, because of baseline age differences, it was included as a covariate in the main analysis.
Contrary to the hypothesis, bias type failed to predict differences in linear improvement across assessment sessions on the BIT (P = .551 for the bias type by session interaction). However, there was a significant linear effect of session (β = 0.50; b = 10.029; SE = 3.96; P < .001), indicating that, as a group, participants’ BIT scores improved after PAT. There was also a trend on the quadratic effect of session (β = −0.35; b = −0.767; SE = 0.390; P < .10). Similar to the CBS, there were effects of baseline status and spontaneous recovery rate. Participants with better screening BIT scores had better BIT throughout (β = 0.90; b = 0.856; SE = 0.098; P < .001). Likewise, participants with better spontaneous recovery between sessions 1 and 2 had higher scores across the assessment sessions (β = 0.44; b = 9.532; SE = 1.852; P < .001). Furthermore, spontaneous recovery in BIT did not predict change across sessions 2 through 7 (β = 0.03; b = 0.127; SE = 0.263; P = .567).
Discussion
Sorting patients from neglect treatment studies into groups based on their specific neglect characteristics may be useful for predicting treatment response. 6 Here, we predicted that patients with Aiming deficits would experience greater recovery after PAT than those with isolated Where deficits. Participants’ performance on the CBS is consistent with this hypothesis: Participants with Aiming bias had steeper recovery trajectories than did those without Aiming bias. Furthermore, participants with isolated Where spatial deficits failed to show improvements. These results are consistent with prior work demonstrating that PAT improved Aiming, but not Where, spatial dysfunction. 18
Whereas Where and Aiming spatial biases predicted different patterns of recovery on the CBS, they did not do so for the BIT, a paper-and-pencil test of neglect. It is possible that the CBS may be more sensitive to detect neglect (and neglect improvement), especially body-based, motor-exploratory, or functional deficits, as compared with paper-and-pencil tests.24,36 Consistent with this argument, the quadratic component on assessment session approached significance for the BIT, but not CBS. This pattern suggests that those with Aiming deficits were still improving on the CBS, but that participants’ improvement on the BIT was plateauing. In their Cochrane review, Bowen and Lincoln 37 contended that evaluating functional outcomes may be critical in determining neglect treatment value, a view consistent with our results.
The data underscore the importance of finding a match between cognitive mechanisms targeted by a treatment and patients’ cognitive impairments. However, classifying patients requires an assessment that identifies specific information-processing deficits. Thus, the findings here support substituting modality-specific cognitive assessment for the generic, composite cognitive screening tools, typically used in many health outcome studies. 38 Such classification may be important for identifying not only which patients will respond positively to a treatment but also may help clarify the negative impact of treatment for subgroups of patients: Treatments improving function in one brain-behavior system may simultaneously adversely affect other neuroanatomical systems.10,20
Neural Mechanisms
Where and Aiming spatial deficits may be supported by dissociable neuroanatomical systems. Heilman and colleagues39-41 first proposed an Aiming, motor-intentional set of neglect deficits critically linked to lesions affecting the frontal cortex and subcortical regions. Subsequent reports partially supported an association between motor-intentional impairment and damage to anterior dorsolateral prefrontal and subcortical sites.41-46 However, Aiming motor-intentional deficits were also reported in association with parietal and temporal cortical lesions.47-49 Similarly, although Where perceptual-attentional impairment was frequently associated with damage to the posterior parietal or temporal cortical regions,42-44,50 this form of impairment has also been associated with more anterior lesions. 49
The small sample size within the groups of the current study precluded systematic analysis of the lesion-behavior associations. Nonetheless, Figures 1 through 3 illustrate that even within groups showing similar behavioral deficits, there was much variety in the lesion locations. Where and Aiming function are each likely supported by a network of interacting brain areas.51-53 Damage in any one of the component areas of the network may result in Where or Aiming deficits. Previously, we demonstrated a complex association: frontal lobe lesions that spared medial temporal sites, including the basal ganglia, predicted better PAT response in spatial neglect. 28 That study did not analyze participants’ patterns of spatial deficits but suggests that analyzing both lesioned and spared regions may be necessary to understand neuroanatomical PAT response predictors. Ideally, future research should include larger groups of patients having a range of representative lesions to assess neuroanatomical-behavioral correlations.
Conclusions
The results of this study suggest that patients with spatial neglect and Aiming spatial biases may experience the most benefit from treatment with PAT. PAT may be ineffective in improving function for patients with isolated perceptual-attentional Where bias. Although neglect severity and lesion location also mediate response to prism adaptation,4,28,54 these factors are commonly considered when designing clinical trial research investigating rehabilitations for these patients. However, because other neglect treatments also target specific spatial neglect deficits, 10 classifying deficits using modality-specific measures may be an important part of any trial intending to obtain the most valid, applicable, and valuable results for neglect care. Aiming spatial neglect also adversely affects motor function and self-care measures. Thus, in the future it may be appropriate for biological stroke treatment trials enrolling diverse patient groups to consider stratification of patients (or balancing of treatment and control groups) based on initial classification of spatial processing deficits.
Footnotes
Acknowledgements
The authors thank Jenny Masmela, Dr Uri Adler, Naureen Zaidi, Bibai Ren, Julia Martin, and Jodi Feriod for assistance with patient recruiting and the collection, scoring, and maintenance of data. The authors thank Priyanka Shah, Daniela Sacchetti, and Karuna Poddar for assistance with lesion mapping.
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This work was funded by the Kessler Foundation, the National Institutes of Health, and the Department of Education/National Institute of Disability and Rehabilitation Research (K02 NS 047099, R01 NS 055808, K24 HD062647, H133 G120203 PI: Barrett). Study contents do not necessarily represent the policy of the Department of Education, and one should not assume endorsement by the federal government. Drs Chen and Goedert received partial salary and Dr Boston consulting fees from the NIH R01 grant supporting the study. Dr Barrett received partial salary from the NIH R01 grant that supported the study and received unrelated research funds from Pfizer/Eisai and the Wallerstein Foundation for Geriatric Improvement.