
Abstract
Background. No treatment for auditory neglect and no randomized controlled trial evaluating smooth pursuit eye movement therapy (SPT) for multimodal neglect are available. Objective. To compare the effects of SPT and visual scanning therapy (VST) on auditory and visual neglect in chronic stroke patients with neglect. Methods. A randomized, prospective trial was conducted. Fifty patients with left auditory and visual neglect were randomly assigned. Twenty-four patients completed SPT therapy and 21 patients VST. Five patients (4 VST, 1 SPT) were lost. Each group received 1-hour sessions of neglect therapy for 5 consecutive days totaling 5 hours. Outcome measures in visual neglect (digit cancellation, visuoperceptual- and motor line bisection, paragraph reading) and auditory neglect (auditory midline) were assessed twice before therapy, thereafter, and at 2-week follow-up. The SPT group practiced smooth pursuit eye movements while tracking stimuli moving leftward. The VST group systematically scanned the same but static stimuli. Both groups were divided into subgroups, and effects were separately investigated for mild and severe neglect. Results. Both groups did not differ before therapy in clinical/demographic variables or neglect severity (auditory/visual). After treatment, the SPT group showed significant and lasting improvements in all visual measures and normal performance in the auditory midline. Neither visual nor auditory neglect impairments changed significantly after VST. Moreover, the treatment effect sizes (Cohen’s d) were considerably higher for visual and auditory neglect after SPT versus VST, both for mild and severe neglect. Conclusions. Repetitive contralesional, smooth pursuit training induces superior, multimodal therapeutic effects in mild and severe neglect.
Introduction
Spatial neglect is a challenging and complex disorder. 1 Typically, it is characterized by an inability to respond to sensory stimuli (visual, auditory, tactile, olfactory) in the contralesional hemispace of a neurological patient. 1 Despite spontaneous recovery, approximately a third of all neglect patients present chronic neglect 1 year after stroke with major impairments in attention and perception. 2 Moreover, associated awareness deficits impair recovery 3 and interfere with treatment of hemiparesis. 4 Nevertheless, the past decade has seen substantial advances in neglect therapy, with studies showing that optokinetic stimulation (OKS) with pursuit eye movements,5-7 attention training,8,9 visuomotor feedback, 10 neck-proprioceptive training, 11 prism adaptation, 12 and transcranial magnetic stimulation13,14 all effectively reduce visual neglect. However, few randomized controlled trials (RCTs) are available,15,16 and the results of such trials do not necessarily confirm therapeutic effects of some interventions, such as prism adaptation. 17 In addition, no established treatment is available for auditory neglect, which is surprising given its frequency. 18 Only recently have researchers begun to investigate potential treatments for auditory neglect.19,20
Recent studies using OKS with smooth pursuit eye movement training (SPT) via moving displays to the contralesional side showed substantial and lasting improvements in visuospatial5,6,21 and tactile neglect. 7 These positive effects may result from the fact that pursuit eye movements are easier for subacute neglect patients than saccadic eye movements to the neglected hemispace. 22 Moreover, this type of stimulation activates multiple cortical and subcortical regions in healthy subjects (temporoparietal cortex, basal ganglia, brain stem, cerebellum23-25), some of which are involved in eye movements and gaze shifts. Primate studies 26 found largely congruent and overlapping receptive fields of neurons in the monkey’s ventral intraparietal cortex. Crucially, these neurons have been shown to have bimodal properties by responding to visual and auditory spatial stimuli, thereby enabling the audiovisual integration of information into a modality invariant representation of external space. Accordingly, right temporoparietal lesions frequently cause visual and auditory neglect. 19 Recently, we showed a rapid but transient normalization of the subjective auditory midline in neglect patients after 20 minutes of SPT, persisting several hours poststimulation. 19 Moreover, 20 sessions of SPT induced lasting recovery from visual and auditory neglect in 3 patients. 19 In the present RCT, we attempted to clarify 2 issues: (a) Does repetitive SPT of 5 treatment sessions reduce visual and auditory neglect to a significantly greater extent than 5 sessions of standard visual scanning therapy (VST)? (b) Do these improvements remain stable for at least 2 weeks posttreatment?
Methods
Participants
Fifty stroke patients with left-sided neglect (time postlesion ≥ 1 month) were consecutively recruited provided they met the following inclusion criteria: right-hemispheric stroke with no previous history of cerebrovascular disease; signs of left neglect in at least 3 out of the 5 used visual neglect tests (perceptual/motor line bisection, single/double digit cancellation, paragraph reading; for description see Assessment, below, results in Table 1) and in the auditory midline test; no psychiatric disorder and no peripheral hearing deficit. In addition, only patients who were able to sit in a wheelchair for 50 minutes were selected. Finally a minimum stay in the clinic for 6 weeks was required to complete the study protocol. Sensorimotor disturbances were assessed by a neurologist, and visual fields were mapped perimetrically. 27 All subjects had at least 9 years of education and a corrected visual acuity of at least 0.70 (20/30 Snellen equivalent) for the near viewing distance (0.4 m). In total, 45 patients completed the study including the follow-up phase (Table 1). Five patients (4 VST group, 1 SPT group) were discharged before completing the study because health insurance providers declined further funding of the patients’ hospitalization.
Demographic/Clinical Data and Assessment Scores for Both Groups at Pretreatment 1 (Baseline 1) a .
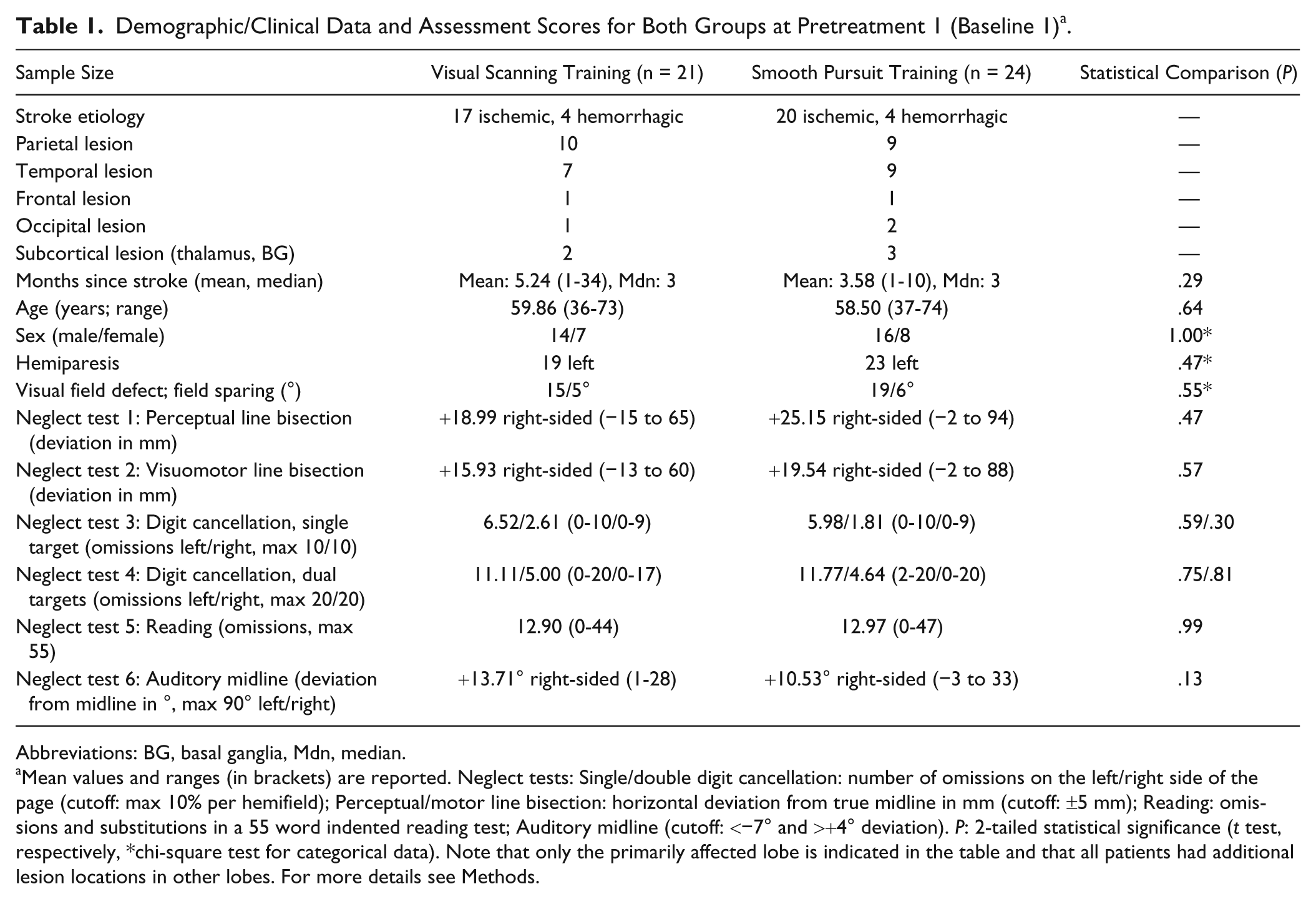
Abbreviations: BG, basal ganglia, Mdn, median.
Mean values and ranges (in brackets) are reported. Neglect tests: Single/double digit cancellation: number of omissions on the left/right side of the page (cutoff: max 10% per hemifield); Perceptual/motor line bisection: horizontal deviation from true midline in mm (cutoff: ±5 mm); Reading: omissions and substitutions in a 55 word indented reading test; Auditory midline (cutoff: <−7° and >+4° deviation). P: 2-tailed statistical significance (t test, respectively, *chi-square test for categorical data). Note that only the primarily affected lobe is indicated in the table and that all patients had additional lesion locations in other lobes. For more details see Methods.
Study Design
Patients were allocated randomly to a treatment group by a person not involved in the study who drew cards from a sealed envelope after baseline 2. Every patient was examined in a single subject baseline design with a treatment-free interval of 2 weeks before treatment and an identical follow-up period of 2 weeks after treatment ended. Four assessments were carried out: 2 pretests resulting in 1 averaged baseline before treatment, a posttest, and a follow-up 2 weeks after the posttest. The treatment started immediately after the second pretest (Baseline) and consisted of five 50-minute sessions, held over a period of 7 to 9 days. Apart from this treatment all patients received standard occupational therapy and physiotherapy, but no other neglect or attentional training. Informed consent according to the Declaration of Helsinki II was obtained from all participants, and the study was approved by the local ethics committee (Bavarian Medical Association). Figure 1 summarizes the patient recruitment and retention.
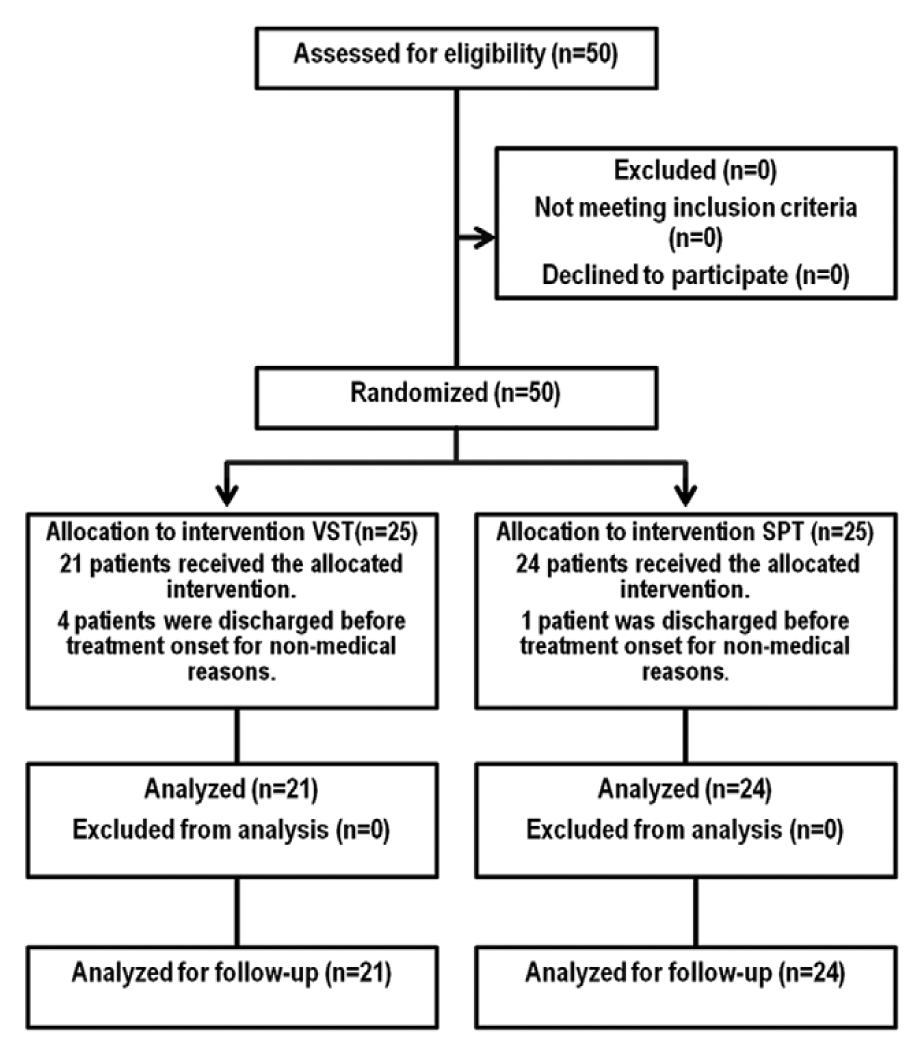
Flow chart of recruitment and retention.
Assessment and Outcome Measures
Cancellation
Patients were instructed to cancel with a pen in their right hand, all target digits (eg, all 20 number “8” items) distributed randomly among 200 single distractor digits ranging from “0” to “9” and presented on a 29 × 21 cm white piece of paper in front of the patient. This cancellation task was administered 3 times with a different target item at each measurement date. The number of omissions in the left and right hemifields was counted (maximum 10 per hemispace and task) and added across all 3 tasks resulting in a maximum of 30 omissions for each hemifield. In a more demanding dual cancellation version, 2 types of target digits (ie, all “1” and “9” numbers) had to be cancelled on 3 different sheets of paper that were identical to those in the single cancellation task (maximum 20 targets per hemispace). Cancellation tasks are reliable during repeated testing. 28 Moreover, dual cancellation tasks increase attentional load, produce more omissions, and are therefore more sensitive. 29
Paragraph reading
Indented reading texts are highly sensitive for neglect in daily life 30 and were included to examine treatment transfer to a nontrained but important activity of daily living. Twenty parallel versions of a paragraph reading test were used. 31 Fifty-five words were arranged in 6 double-spaced lines with irregularly indented margins on both sides. Each text was printed in Arial 12 point font on a 25 cm × 9 cm sheet of paper. Five texts were presented successively in each session. The mean number of omissions across the 5 reading tests was calculated.
Line bisection
Two versions were used. In the perceptual version (10 trials) a 24 × 1 cm yellow horizontal bar against black background was presented centrally on a PC screen at a distance of 0.4 m from the patient. On the right side of the bar a small vertical black slit was visible (2 × 10 mm) that had to be positioned in the center of the bar. The objective center of the bar was aligned with the patient’s body sagittal plane. The examiner moved the slit by key-press on the keyboard based on the patient’s verbal feedback into the subjective midline position. In the motor version (3 trials) a 200 mm long and 5 mm wide black horizontal line was presented centrally on a 29 × 21 cm large white sheet of paper. The patient was instructed to bisect the line with the right hand using a pencil. The purpose of both tasks was to assess the possible transfer of treatment effects into perceptual and motor domains of visual neglect.
Auditory tests
The peripheral hearing functions in all patients were screened with a Philips HP 8741/31 pure-tone audiometer in a sound-shielded room. Hearing sensitivity (loss in dB) was within normal limits and showed no significant difference between the 2 ears and both treatment groups (all Ps >.05). Auditory neglect was assessed with the auditory subjective midline test (details and normative values 19 ). Subjects listened to sound stimuli (3 seconds of white noise, sound pressure level: 75 dB) sequentially presented over headphones (AKG K240), with a spatial resolution of 5° in front space. The starting position was pseudo-randomized between the 2 hemispaces to control for any bias. The subject’s head rested on a head/chinrest while viewing a red central fixation spot (0.5°, 30 Lux). Subjects indicated whether the sound came from the left, right, or directly from their subjective midline position. Following each “left” or “right” response a new stimulus located 5° more toward the opposite direction of the perceived sound position was presented. This adjustment procedure was repeated until the subject indicated that the sound represented his subjective midline. Each session consisted of 20 trials with an equal number of 10 starting positions per hemispace. 19
Treatments
SPT stimuli were presented on a 17-in. PC monitor (eccentricity: 44.8° horizontal, 34.8° vertical, refresh rate 75 Hz) in a distance of 0.4 m from the patient. The patients were instructed to look at computer-generated random displays of 30 to 70 dots (of all colors, size: 2° to 4°) on a dark background, all moving coherently toward the left, contralesional hemispace with a speed varying from 2.6° to 11.2°/s. Movement speed and the number of stimuli on the display changed from trial to trial to keep patients alert. Subjects were encouraged to make smooth pursuit movements toward the direction of the motion and return with their eyes to the ipsilesional side of the screen each time they reached the (contralesional) border of the screen. Eye movements were monitored by the therapist for the duration of the session from the side. No head movements were allowed and controlled by the therapist. Patients in the VST group received treatment using the same setup, device, and stimuli as for SPT. However, all visual stimuli were displayed stationary. Patients were instructed to scan the array systematically (horizontally, vertically) by starting on the top left corner and ending at the bottom right of the screen. Patients searched for specific target symbols on the display (ie, all red circles). Scanning strategies were repeatedly explained to the patients and the timing of treatment and breaks was identical to the SPT group. Patients were encouraged repeatedly to make (saccadic) eye movements to the left side. No head movements were allowed. Each SPT/VST therapy session consisted of 4 runs of 10 minutes duration, with short breaks (2 minutes) between these runs. Thus, the only crucial difference between the 2 treatments was in the moving versus stationary presentation of the visual stimuli, and in the type of eye movements exacted from the patient (voluntary saccades during VST vs pursuit eye movements and saccades during SPT).
Statistical Analysis
A series of mixed ANOVAs was carried out with Treatment (SPT vs VST) as between-group factor and Measurement Point (Baseline 1, Baseline 2, Posttest, Follow-up) as within-group factor. The chosen α level of .05 was Bonferroni-corrected for multiple comparisons (t tests). Additionally, both treatment groups were split into moderately versus severely impaired subgroups, and effects sizes in these subgroups were computed.
Results
Demographic Comparison of the 2 Treatment Groups at Treatment Onset
The 2 neglect groups did not differ significantly with respect to sex (χ2 = 0.00, P = 1.00), frequency of visual field defects (χ2 = 0.36, P = .55), presence of paresis (χ2 = 0.52, P = .47), age (t[43] = −0.48, P = .64), or time since lesion (t[43] = −1.08, P = .29). The clinical and demographic data are shown in Table 1.
Group Comparisons at Baseline
Separate univariate ANOVAs with the factors Group (VST and SPT) and Time (first and second baseline) were performed for each task to rule out spontaneous remission, repetition, or unspecific training effects between the 2 baselines as well as preexisting group differences. There were no significant main effects of Group in any of the measured variables (largest F[1, 43] = 2.45, P = .124 [Auditory Midline] and no significant Group × Time interactions [largest F[1, 43] = 2.05, P = .16 [Reading Omissions]). Therefore, the pretreatment performances of the SPT and the VST groups can be assumed to be comparable. A (marginally) significantly deteriorated second baseline compared to the first was found for the Dual Cancellation Test with less targets detected on the left side of the array (F[1, 43] = 4.01, P = .052). All main effects of Time were not significant either (largest F(1, 43) = 1.10, P = .30 [Reading Omissions]). These results indicate neither significant improvements from the first to the second baseline (indicative of spontaneous remissions) nor significant differences between the 2 experimental groups, nor significant Group × Time interactions. Based on these findings, all subsequent analyses ware carried out using data that were collapsed across both baseline measures.
Treatment Comparisons
Separate 2 × 3 ANOVAs with the factors Group (SPT and VST) and Time (pooled baseline, posttest, follow-up) were carried out for reading omissions, deviations in perceptual and motor line bisection, and the auditory midline task. The omissions in the Single and Double Cancellation tasks were analyzed using 2 × 2 × 3 ANOVAs with the factors Group (SPT and VST), Side (left or right sided omissions), and Time (pooled baseline, posttreatment, and follow-up). Greenhouse–Geisser corrections were performed if the sphericity assumption had been violated.
Auditory Midline
There were significant main effects of Time (F[2, 86] = 7.22, P = .001) and Group (F[1, 43] = 25.10, P = .001) as well as a significant Group × Time interaction (F[2, 86] = 6.29, P = .003). A further simple main effect analysis revealed a significant effect for SPT (F[2, 42] = 15.31, P < .001, η2p = 0.422) but not for VST (F[2, 42] = 0.08, P = .919, η2p = 0.004). Paired comparisons showed a significant reduction of the rightward deviation in the auditory midline after SPT from baseline to posttest (mean difference = 8.45, P < .001) and from baseline to follow-up (mean difference = 7.75, P < .001; Figure 2A), but no difference from posttest to follow-up (P > .05).
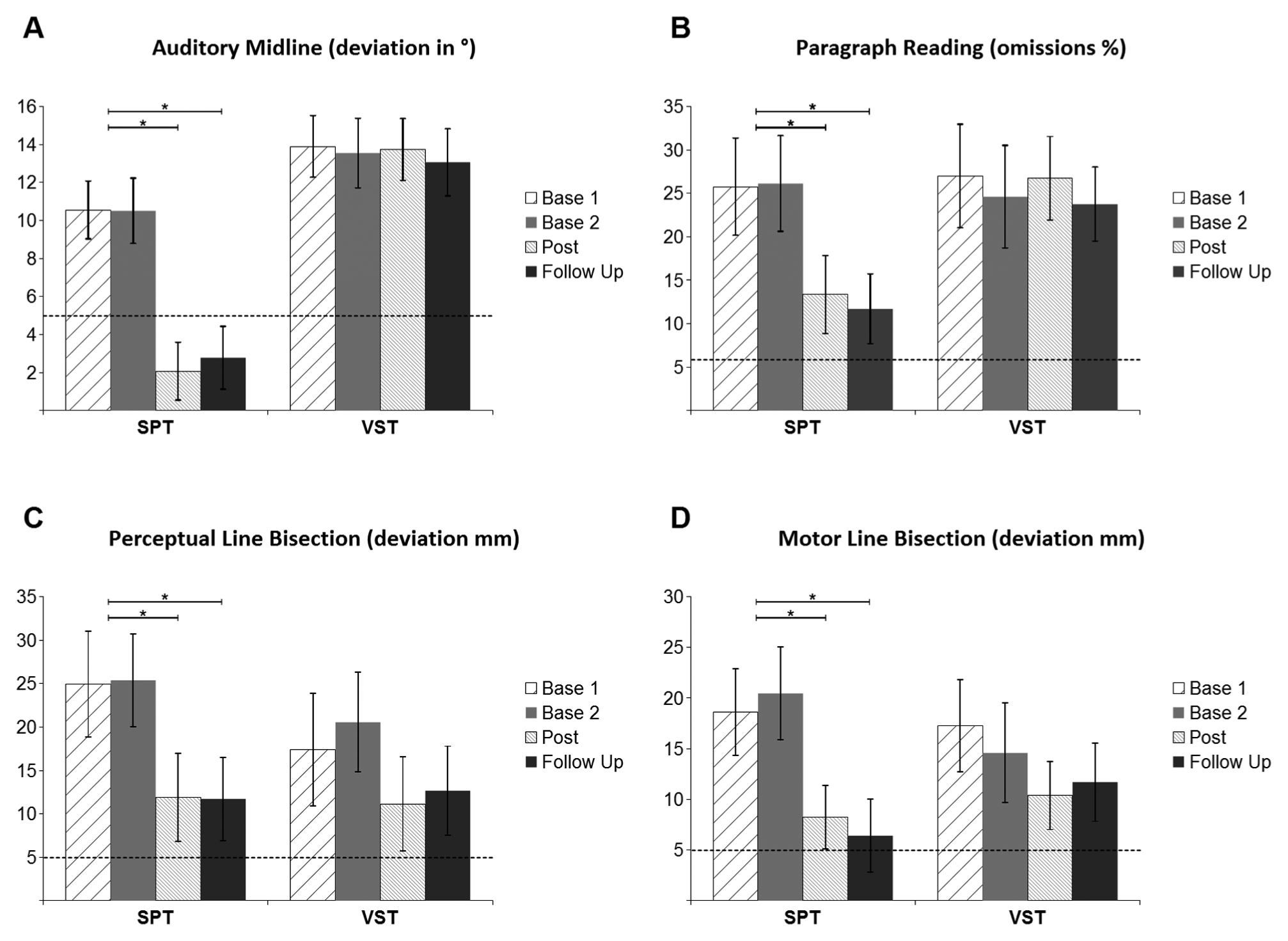
Effects of smooth pursuit training (SPT) and visual scanning training (VST) on the auditory midline task (A), paragraph reading (B), perceptual line bisection error (C), and motor line bisection error (D).
Paragraph Reading
The ANOVA yielded a significant main effect of Time (F[1.58, 68.16] = 14.41, P < .001) as well as a significant Group × Time interaction (F[1.58, 68.16] = 11.37, P = .052). There was no significant effect of Group (F[1, 43] = 1.60, P = .213). The main effect analysis was significant for SPT (F[2, 42] = 22.20, P < .001, η2p = 0.515), but not VST (F[2, 42] = 1.27, P = .30, η2p = 0.057). Paired comparisons revealed a significant reduction of omissions after SPT from baseline to posttest (mean difference = 6.30, P < .001) and to follow-up (mean difference = 7.12, P < .001; Figure 2B). Posttest and follow-up measures did not differ significantly (P > .05).
Perceptual Line Bisection
There was a significant main effect of Time (F[1.39, 59.88] = 10.47, P = .001) but no significant effect of Group (F[1, 43] = 0.09, P = .77), nor a significant Group × Time interaction (F[1.39, 59.88] = 1.04, P = .34) were found. The main effect analysis was significant for SPT (F[2, 42] = 5.90, P = .006, η2p = 0.219) but not for VST (F[2, 42] = 1.47, P = .24, η2p = 0.065). Paired comparisons revealed a significant reduction of the rightward deviation after SPT from baseline to posttest (mean difference = 13.27, P = .009) and to follow-up (mean difference = 13.42, P = .004; Figure 2C), while posttest and follow-up were not different (P > .05).
Motor Line Bisection
For motor line bisection there was a significant main effect of Time (F[2, 86] = 11.37, P ≤ .001). There was neither a significant Group effect (F[1, 43] = 0.69, P = .79) nor a significant Time × Group interaction (F[2, 86] = 2.38, P = .10). A simple main effect analysis was significant for SPT (F[2, 42] =8.07, P = .001, η2p = 0.278) but not for VST (F[2, 42] = 1.37, P = .26, η2p = 0.061). Paired comparisons revealed a significant reduction of the rightward deviation after SPT from baseline to posttest (mean difference = 11.29, P = .002) and to follow-up (mean difference = 13.12, P = .001; Figure 2D), while posttest and follow-up did not differ (P > .05).
Single Digit Cancellation
For the single digit cancellation task, a 3 × 2 × 2 ANOVA revealed significant main effects for Time (F[2, 86] = 14.37, P < .001), Side (F[1, 43] = 90.09, P < .001), and Group (F[1, 43] = 5.22, P = .027) as well as significant Group × Time (F[2, 86] = 5.91, P = .004) and Side × Time (F[2, 86] = 6.23, P = .003) interactions. The Group × Side (F[1, 43] = 0.96, P = .33) and the Group × Side × Time interactions (F[2, 86] = 2.16, P = .12) were not significant. A simple main effect analysis was performed to examine the effects of the different treatments separately. These analyses revealed significant effects for the SPT treatment on the left side (F[2, 42] = 19.47, P < .001, η2p = 0.481) and on the right side (F[2, 42] = 6.23, P = .004, η2p = 0.229) of the Single Number Cancellation task. Paired comparisons yielded a significant reduction of left-sided (mean difference = 2.78, P < .001) and a nonsignificant trend for a reduction of right-sided (mean difference = 0.90, P = .081) omissions after SPT from baseline to posttest. Both comparisons between baseline and follow-up were significant as well (left-sided: mean difference = 2.94, P < .001; right-sided: mean difference = 1.02, P = .003). No significant change was observed between posttest and follow-up (left/right side P > .05). There was no significant simple main effect after VST, neither for left-sided (F[2, 42] = 1.02, P = .37, η2p = 0.046) nor for right-sided (F[2, 42] = 0.30, P = .74, η2p = 0.014) omissions (Figure 3A and B).
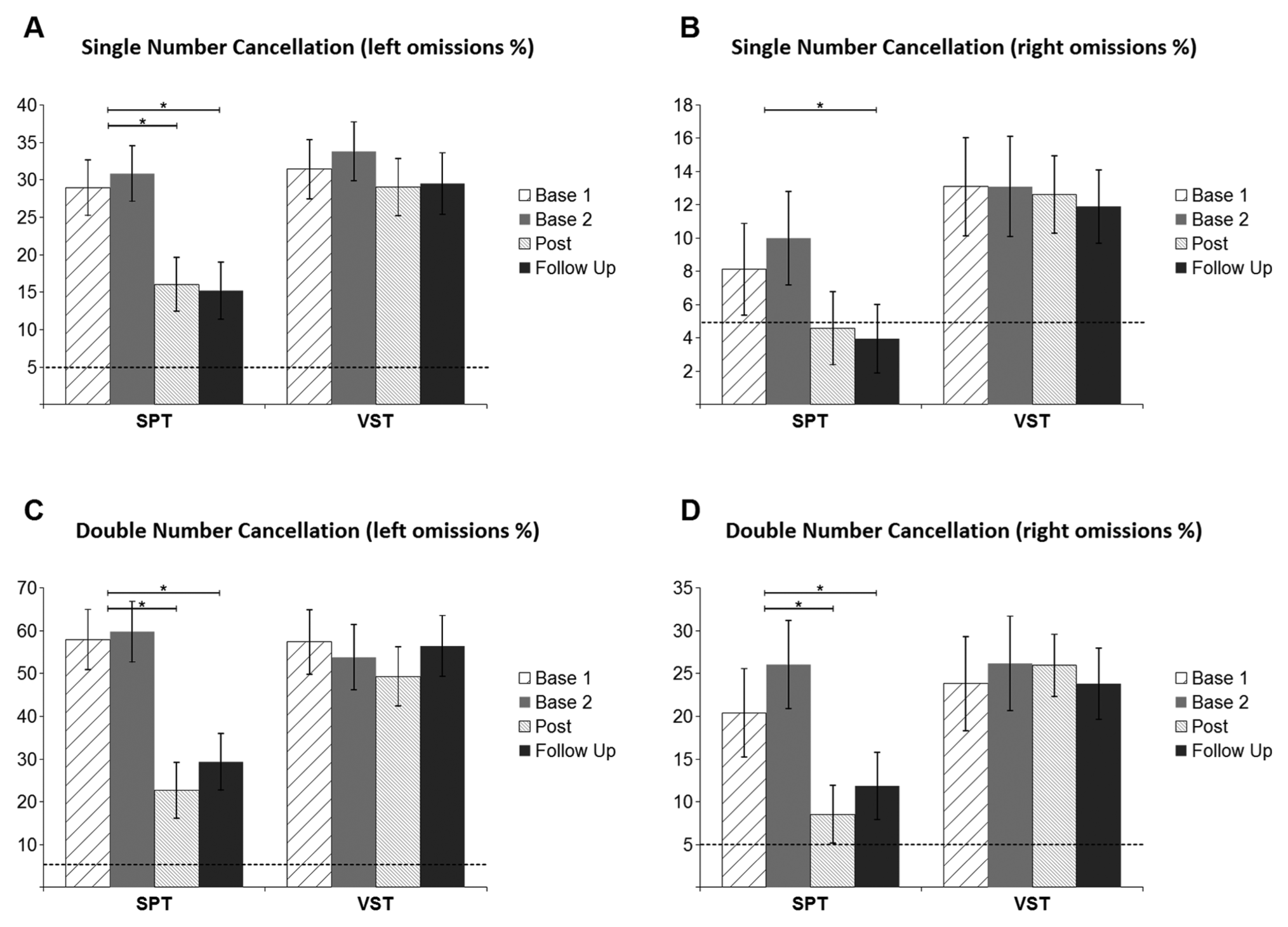
Effects of SPT and VST on the percentage of left-sided (A; contralesional) and right-sided (B; ipsilesional) omissions in single digit cancellation during 2 baseline measurements (Base 1, Base 2), after treatment (Post) and at follow-up. Analogue results for dual digit cancellation are shown for left-sided (C) and right-sided (D) omissions, respectively.
Double Digit Cancellation
For double digit cancellation, a 3 × 2 × 2 ANOVA revealed significant main effects for Time (F[1.53, 65.79] = 22.07, P < .001), Side (F[1, 43] = 69.03, P < .001), Group (F[1, 43] = 4.08, P = .050), and significant Group × Time (F[1.53, 65,79] = 16.22, P < .001), Side × Time (F[1.76, 75.55] = 7.08, P = .002), and Group × Side × Time interactions (F[1.76, 75.55] = 3.66, P = .036). The Group × Side interaction (F[1, 43] = 1.08, P = .30) was not significant. A simple main effect analysis revealed significant effects for the SPT treatment on the left side (F[2, 42] = 24.04, P < .001, η2p = 0.537) and on the right side of the array (F[2, 42] = 7.39, P = .002, η2p = 0.260). Paired comparisons revealed a significant reduction of left-sided (mean difference = 7.23, P < .001) and right-sided (mean difference = 2.94, P = .001) omissions after SPT from baseline to posttest. Both comparisons between baseline and follow-up were also significant (left-sided: mean difference = 5.90, P < .001; right-sided: mean difference = 2.27, P = .007). No significant change was observed between posttest and follow-up (left/right side P > .05).
Again, there was no significant simple main effect for VST observable, neither for left-sided (F[2, 42] = 2.34, P = .11, η2p = 0.10) nor for right-sided (F[2, 42] = 0.280, P = .76, η2p = 0.013) omissions (Figure 3C and D).
Comparison of Effect Sizes for Subgroups With Mild Versus Severe Neglect
To compare whether the efficacy of the treatments was modulated by the severity of neglect, the groups were divided by median split into mild or severe neglect for each dependent variable. Cohen’s d was computed for the posttreatment and the follow-up measurements as compared to the pooled baselines before treatment, separately for all split dependent variables. Effect sizes were considerably higher for SPT than VST therapy, both in the visual and auditory modalities, and for both severity subgroups. Importantly, all effects of SPT remained stable at follow-up (Figure 4).
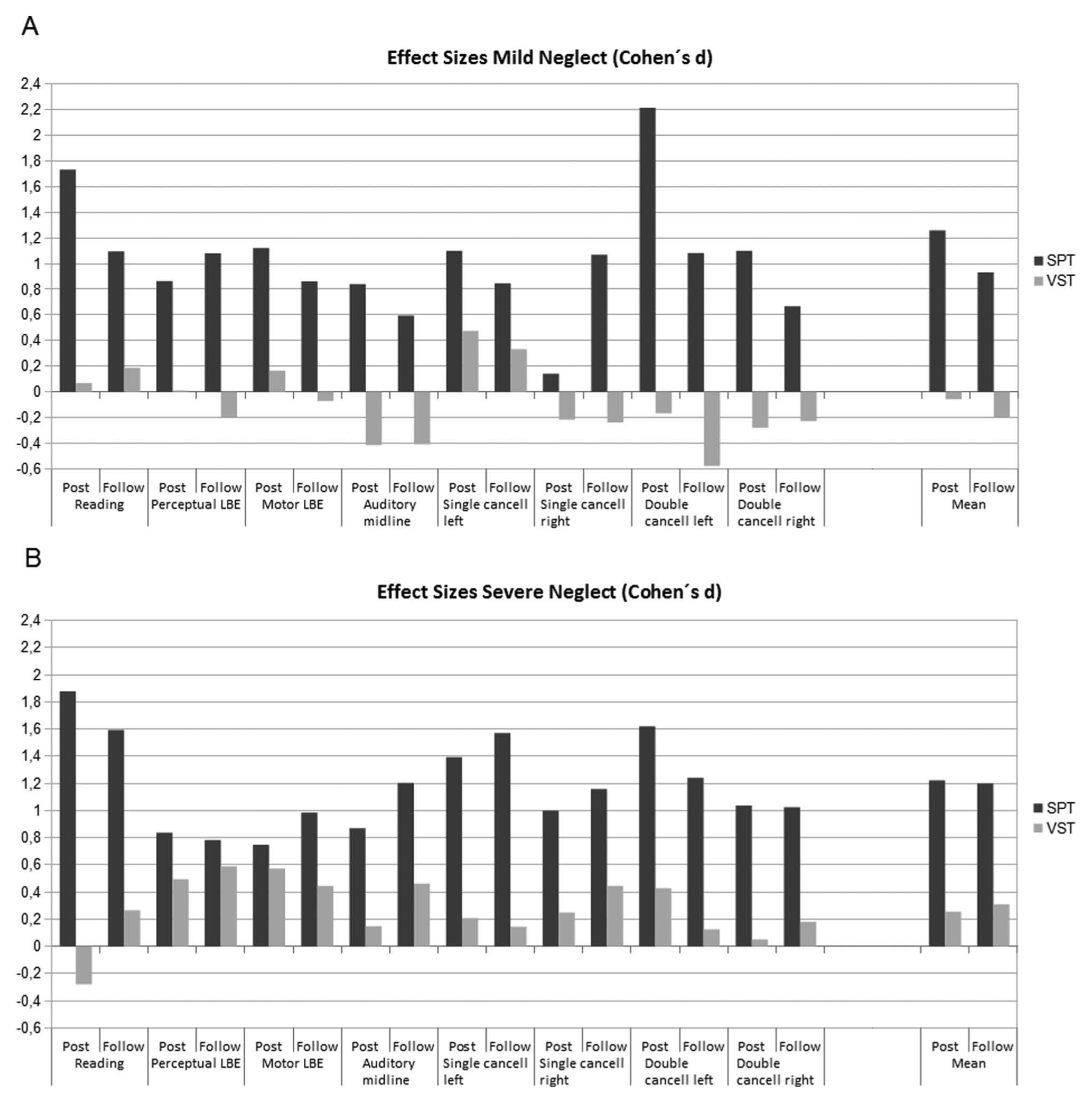
Mean effect sizes (Cohen’s d) for the treatments and their stability in visual and auditory outcome measures, separately for mild versus severe neglect in the 2 treatment groups (VST = grey bars vs SPT = black bars). Negative bars indicate (nonsignificant) worsening of the performance.
Discussion
This first RCT of pure SPT showed widespread therapeutic effects on visual neglect, which generalized across perceptual and visuomotor tasks. Importantly, SPT also reduced auditory neglect. Immediate transfer of SPT to daily life tasks was observed for the paragraph reading test although reading was not trained. Interestingly, the improvements were strongest (Figure 3C and D) in the dual cancellation task, which may indicate improved attentional resources after SPT. In terms of efficacy, SPT was clearly more effective within this short treatment duration (5 hours) than conventional VST. Importantly, all effects of SPT remained stable at follow-up (Figure 4). Moreover, comparable treatment effects were obtained for moderately and severely impaired patients. By and large, these results concur with previous studies using similar methods for visual and tactile neglect,5-7,19,21 and show for the first time that SPT significantly improves one component of auditory neglect: the auditory midline.
Functional imaging studies suggest a widespread activation of a cortico-subcortical network during OKS inducing smooth pursuit eye movements in healthy participants,24,32 and hemianopia. 33 This network includes the occipitotemporal, parietal, insular and occipital cortex, basal ganglia, cerebellum, and the brain stem.23,24,32 Moreover, this network is involved in gaze and attentional shifts,23-25 which were explicit features of SPT. SPT may thus have improved neglect by recalibrating egocentric spatial orientation, 34 thus correcting the pathological, ipsilesional neglect bias into a more symmetrical midline position, and facilitating attention shifts to the neglected side. 35 Additionally, SPT may have activated the vestibulo-ocular system via optokinetic nystagmus. The cross-modal effect is probably related to multimodal space representations. 36 The parietal cortex is involved in visual/auditory space representations 26 and auditory-spatial attention shifts. 37 It also contains a modality-independent priority map, which is believed to be involved in spatial neglect.38,39 Visual motion may induce stronger treatment effects because of dynamic features contained in moving displays eliciting smooth pursuit 40 and the multiple brain regions involved in visual motion processing. 41
A few limitations of our study should be mentioned: First, graphical overlays of MRI-lesion scans were not available, and functional outcome measures were not included. VST is the most often evaluated treatment for visuospatial neglect in neurorehabilitation. 15 Unfortunately, VST has several shortcomings such as no effect on nonvisual neglect (haptic 11 ; auditory: current study), and the large number of necessary treatment sessions (20-40). 34 Moreover, no RCT is available documenting long-term efficacy of VST on functional disability. Therefore, more time- and modality-effective therapies are required to accelerate behavioral recovery from visual neglect, and also from auditory neglect, body-related neglect,42,43 and extinction phenomena. 44 SPT is one such candidate because it acts multimodally, quickly, and is easily applicable.
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.