
Abstract
Background. Unilateral spatial neglect (USN) is a visual-perceptual disorder that entails the inability to perceive and integrate stimuli on one side of the body, resulting in the neglect of one side of the body. Stroke patients with USN present with extensive functional disability and duration of therapy input. Objective. To determine the effect of saccadic eye movement training with visual scanning exercises (VSEs) integrated with task-specific activities on USN poststroke. Methods. A matched-pair randomized control trial was conducted. Subjects were matched according to their functional activity level and allocated to either a control (n = 12) or an experimental group (n = 12). All patients received task-specific activities for a 4-week intervention period. The experimental group received saccadic eye movement training with VSE integrated with task specific activities as an “add on” intervention. Assessments were conducted weekly over the intervention period. Results. Statistical significant difference was noted on the King-Devick Test (P = .021), Star Cancellation Test (P = .016), and Barthel Index (P = .004). Conclusion. Intensive saccadic eye movement training with VSE integrated with task-specific activities has a significant effect on USN in patients poststroke. Results of this study are supported by findings from previously reviewed literature in the sense that the effect of saccadic eye movement training with VSE as an intervention approach has a significant effect on the visual perceptual processing of participants with USN poststroke. The significant improved visual perceptual processing translate to significantly better visual function and ability to perform activities of daily living following the stroke.
Introduction
Unilateral spatial neglect (USN) is a complex and multifaceted disorder. 1 Patients with USN following a stroke may present with sensory neglect that is defined as the impaired ability to respond to sensory stimuli such as visual, auditory, tactile, and olfactory input from the contralesional hemispace. 1 Regardless of the side of the stroke, 2 sensory neglect is rarely observed in isolation and may present in combination with motor, language, and cognitive dysfunctions. Motor neglect in addition to sensory neglect may result in nonuse or decreased use of the contralesional extremities during functional activities in the home, work, community, and recreational environment.1,3-6
Unilateral spatial neglect has a negative influence on functional recovery and is associated with poor functional outcome following a stroke.1,3,4,5,7,8-14 Every year approximately 3 to 5 million patients suffer from neglect following a stroke, placing a substantial burden on the country’s health system 1 and the limited number of rehabilitation therapists in both the public and the private sector in South Africa. Incidence of USN may continue to increase as result of the aging of the general population and the effect of the high number of patients with human immunodeficiency Virus (HIV) and acquired immunodeficiency syndrome (AIDS) contribute to an increased number of patients who sustain a stroke.15-18
The increased incidence of stroke and USN 1 in especially the younger population emphasizes the importance of effective and evidence-based rehabilitation, including the management of USN. Various earlier treatment techniques for USN included visual scanning therapy, optokinetic stimulation, neck muscle vibration, caloric and galvanic vestibular, and prism adaptation. 1 A number of new novel treatment options for USN were introduced in the past 2 decades, for example, visuomotor feedback training, 19 combination of visual scanning therapy and functional electrical stimulation, 20 functional electrical stimulation, 21 and interactive virtual environment training. 22 Despite the significant number of new and novel treatment techniques in the treatment of USN, currently there are no evidence-based recommendations that could assist a rehabilitation therapist to select the best treatment or combination of techniques that is most advantageous in rehabilitation of a stroke patient with USN. 1
Unilateral spatial neglect is the most disruptive impairment of visual scanning, with fewer eye movements observed to one side of body or extrapersonal space during the performance of an activity. With careful observation of a patient’s activity, the fovea of the eye does not appear to be directed to gather information from one side of the body or extrapersonal space. Visual scanning using saccadic eye movements occurs on only one side of the midline within the unaffected side of the body with limited or absent spontaneous eye movements or head movements past the midline into the affected space.14,23 Despite the important role that vision plays in a person’s functional ability, a lack of evidence in the literature on the integration of visual scanning exercises (VSEs) as part of and integrated with physiotherapy was identified. This observation of the lack of evidence and the lack of integration of saccadic eye movement training with VSEs during task-specific activities urged the researcher to investigate the effect of VSEs integrated with physiotherapy in patients who present with USN poststroke.
Methods
The study design entailed a matched-pair randomized control trial 24 conducted between October 2009 and February 2011 at a Government Rehabilitation Centre (GRC) in Pretoria, South Africa. Ethical approval to conduct this study was granted by the Ethics Committee of the Faculty of Health Sciences at the University of Pretoria, South Africa (S33/2009). Research funding to conduct the study was obtained from the Medical Research Council of South Africa.
Participants
Participants between the ages of 19 and 74 years who had been admitted to the GRC for rehabilitation following a clinical ischemic or hemorrhagic cerebral vascular incident within 1 and 3 weeks poststroke were recruited to participate in the trial. Participants were selected from a large age range to include younger participants who presented with a stroke due to HIV and AIDS.25,26 Participants were excluded from the study if they (a) scored less than 7 on the Mini-Mental State Examination and presented with a Glasgow coma scale score of less than 14, 26 (b) had a history of an organic disorder or major psychiatric problems and/or (c) were included in other pharmacological or rehabilitation intervention studies,25-27 and (d) had another comorbid condition, musculoskeletal or neuromuscular disability such as cancer or amputation, which would have prevented participation over a period of 4 weeks.25-27 Written informed consent was obtained from the participants who met the inclusion criteria and who were willing to participate in the study.
Sample Size
Twenty-four participants with USN following a cerebral vascular incident who were admitted to the GRC were recruited to participate in the study. The sample size of 24 participants was based on the calculation to detect a 1 standard deviation difference with 80% power using analysis of covariance (ANCOVA).
Matching
Participants who met the inclusion criteria of the study were screened on the basis of their functional activity level as measured on the Stroke Activity Scale (SAS) by an independent assessor directly after they had been admitted to the GRC. Participants were matched and allocated on the basis of their scores on the SAS to ensure that participants in the 2 groups were comparable with regard to their level of functional activity. The first participant who was eligible for participation in the study was allocated to group 1 (experimental group). Participants who matched a previous participant’s score on the SAS were automatically placed in the second group (control group). If a participant had a score that did not match another participant’s SAS score, the participant was randomly allocated to either group 1 or group 2 using a formula on a Microsoft Excel program to randomly allocate participants.
The allocation process was repeated until 12 participants had been allocated to each group. The participants from group 1 and group 2 were blinded to the group they were assigned to. 27 The 2 groups of 12 participants in each group did not make provision for dropout of participants in the study. If a participant dropped out of the study for any reason, another participant was recruited to replace him or her during the 4 weeks of the study. No statistical difference was noted between the groups at baseline (P = .24). Based on the interpretation of the SAS, the motor function of participants from group 1 and group 2 was similar at the beginning of the intervention period. It can be concluded that the 2 groups were comparable to each other regarding motor function and level of functional activity prior to intervention.
Research Process
After the demographical information was obtained, participants in both groups were assessed in terms of their functional ability based on the framework of the International Classification of Functioning, Disability and Health. 28 Within this disability framework, the participants were assessed on the levels of body impairment and functional activity by using the selected clinical assessment tools and outcome measures. Assessment at baseline was conducted immediately after the participants had been allocated to groups 1 and 2. Their baseline measurements on the selected outcome measures were completed before commencement of the intervention.
Intervention
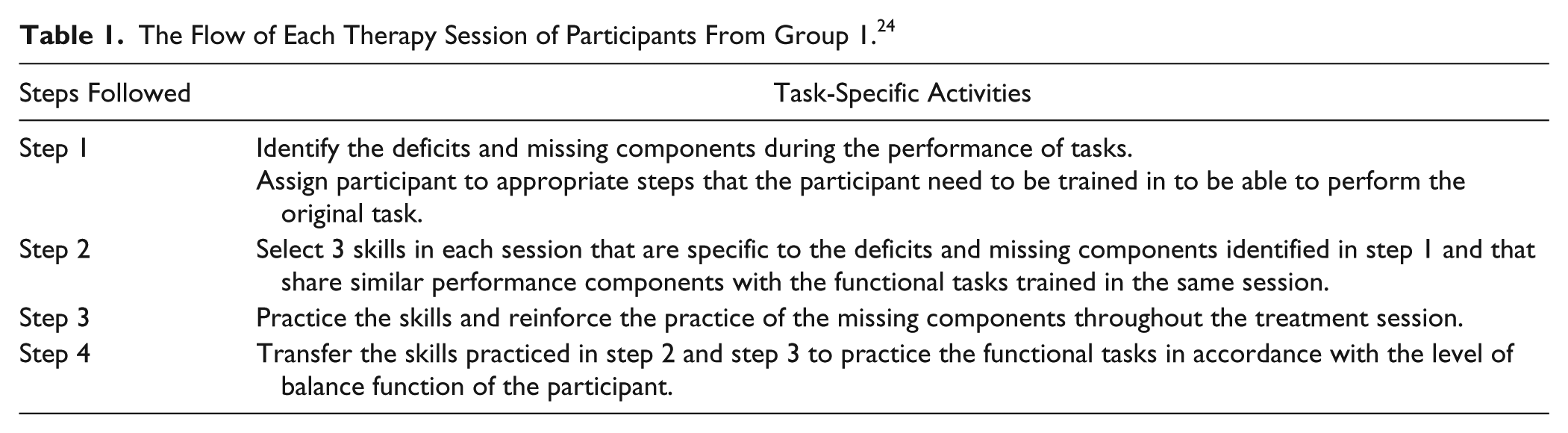
The intervention period commenced directly after the baseline assessment and continued for 5 days per week for 4 consecutive weeks. The intervention period consisted of 4 weeks because this is the average period of time participants spend in the GRC for poststroke rehabilitation. Group 1 received saccadic eye movement training with visual scanning exercises integrated with task-specific activities and group 2 received task-specific activities only. Only the guideline of the interventions is given because the principles were adapted to each participant’s functional ability. The flow of each therapy session is presented in Table 1. 24 The VSEs integrated with task-specific activities consisted of dual-task activities, which require the ability to allocate information-processing resources between 2 tasks and to maintain sufficient attention on the visual scanning task during the dual-task performance.29,30 The guideline of the VSEs integrated with task-specific activities and the principles of progression of these exercises are presented in Table 2.
The Flow of Each Therapy Session of Participants From Group 1. 24
Guide of the Principles of Visual Scanning Exercises Integrated With Task-Specific Activities and the Principles of Progression of These Exercises.

The average duration of physiotherapy sessions was approximately 45 minutes. Time spent on report writing, advice given to participants, family, or caregivers, and discussions with other members of the multidisciplinary team were not included in these 45 minutes. Because rehabilitation requires a multidisciplinary team approach, the participants’ treatment by other members of the rehabilitation team (namely, the occupational therapist, the speech-and-language therapist, and the social worker) continued as usual at the GRC.
Control of Bias in the Research Process
A qualified physiotherapist from the principal investigator’s practice treated participants in group 1 and one physiotherapist from the GRC treated participants in group 2. The principal investigator orientated and trained the 2 physiotherapists in the task-specific treatment approach to rehabilitation of participants who had sustained a stroke and who suffered from USN poststroke to ensure that there was no difference in the application of the poststroke task-specific treatment approach between the 2 physiotherapists.
Orientation and in-service training of the 2 physiotherapists took place prior to the commencement of the trial. The participants in groups 1 and 2 were treated in separate venues to control blinding of the participants throughout the study. The 2 physiotherapists who treated the participants in groups 1 and 2 based their treatment on a client-centered task-based approach to rehabilitation. The client-centered task-based approach to rehabilitation entails the facilitation of active participation and the responsibility of the participants and their caregivers in the rehabilitation process. 31
To ensure reliability of the research data, a skilled assessor who was blinded to the groups conducted all the assessments of the participants in the trial. The independent assessor conducted the assessment of the participants on day 1, day 8, day 15, day 22, and day 28. All the outcome measures used in this study, namely the King-Devick Test,14,23,32,33 Star Cancellation Test, 34 and Barthel Index (BI),35,36 are internationally recognized and validated. This ensured the reliability of the data. The results of this study may therefore be compared with those of similar studies where the same methods or outcome measures were implemented.
Assessment Instruments
In this study, the International Classification of Functioning, Disability and Health was used as the model of disablement within which participants were assessed and treated. 28 Assessments of visual scanning and oculomotor function on impairment level were carried out using 2 selected outcome measures namely the King-Devick Test14,23,32,33 and the Star Cancellation Test 34 The King-Devick Test is a useful tool for the assessment of residual oculomotor functions in participants poststroke.14,32 The test is an indicator of oculomotor visual performance for eye movements during reading and assesses residual oculomotor functions in the clinical setting.14,32 The test is quick, easy to score, and can be administered by all members of the rehabilitation team. The test can be repeated without affecting the reliability and validity of the measure because learning is not likely to play a role in the outcome of the test.
No statistical difference was noted on the King-Devick Subtest 1 (P = .82), King-Devick Subtest 2 (P = .57), and King-Devick Subtest 3 (P = .15) at baseline between group 1 and group 2. Interpretation of the subtests’ scores at baseline indicates that the 2 groups were comparable with regard to their residual oculomotor function at the beginning of the study.
The Star Cancellation Test 34 was selected to assess the effect of the interventions on participants’ USN. The implication of the Star Cancellation score at baseline is that the level of USN in the near extrapersonal space observed in both groups was fairly similar (P = .06) prior to the intervention. Participants in both groups therefore presented with comparable level of USN at the beginning of the trial. The Star Cancellation Test presents with excellent validity, sensitivity and test–retest reliability (intraclass correlation coefficient = 0.89). 14 The test can be repeated without influencing the reliability and validity of the measure.
Assessments of functional activity level were carried out with the use of BI35,36 to assess whether visual scanning exercises integrated with task-specific activities (group 1) had a greater influence on functional activities than task-specific activities alone (group 2). The BI35,36 assesses the performance of 10 common activities of daily living (ADLs) regarding feeding, bathing, grooming, dressing, bowel control, bladder control, toileting, chair transfer, ambulation, and stair climbing, as well as the patient’s dependence (on assistance) to perform these activities. No statistical difference was found in the level of functional ability and dependence on assistance during ADLs between the groups at baseline (P = .54).
Data Analysis
For descriptive purposes it was assumed that given the small number of participants in each group, all data were nonnormally distributed. Results are therefore described with medians and 25th and 75th percentiles. For comparison purposes, Mann–Whitney U tests were carried out without adjustment for multiple comparisons. For comparing outcomes at week 4, adjusting for baseline values, as well as the fact that subjects were matched, a mixed model rank ANCOVA analysis was used where the week 4 and baselines values were ranked and the ranked values used in the regression analyses. P values ≤.05 were regarded as statistically significant. All analyses were done in R 2.14.2.
Results
The course of the study is displayed in Figure 1. The demographic data of participants from group 1 and group 2 are displayed in Table 3. No statistical difference regarding the (a) demographic data, (b) residential areas, (c) access to basic services, and (d) level of education between the groups was found at baseline. On the basis of these results, it can be concluded that the 2 groups were comparable to each other regarding age, gender, race, affected side poststroke, and dominant side prior to the stroke at the beginning of the study. It can also be concluded that the 2 groups were comparable to each other regarding home environment, socioeconomic status, and level of education at the beginning of the study and the demographic profile was, therefore, not expected to have any influence on the outcome of the interventions on the dependent variables. The obtaining of comprehensive sociodemographic information was important to the researchers such as access to a caregiver and environmental system because a difference in resources and support may influence the outcome of the intervention and the ability to sustain the progress made during the rehabilitation period. 8
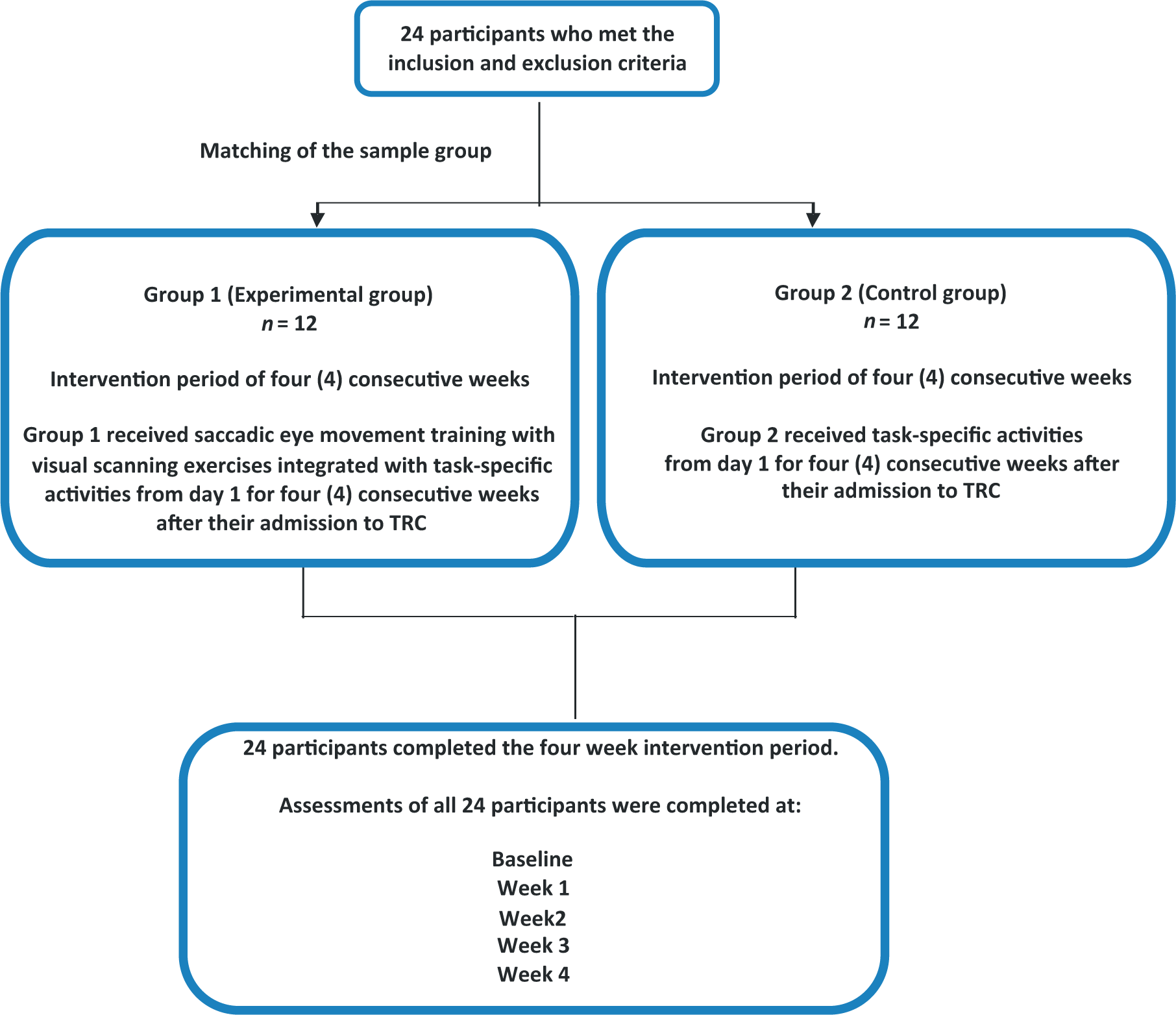
The course of the study.
The Demographic Data of Participants From Group 1 (n = 12) and Group 2 (n =12).
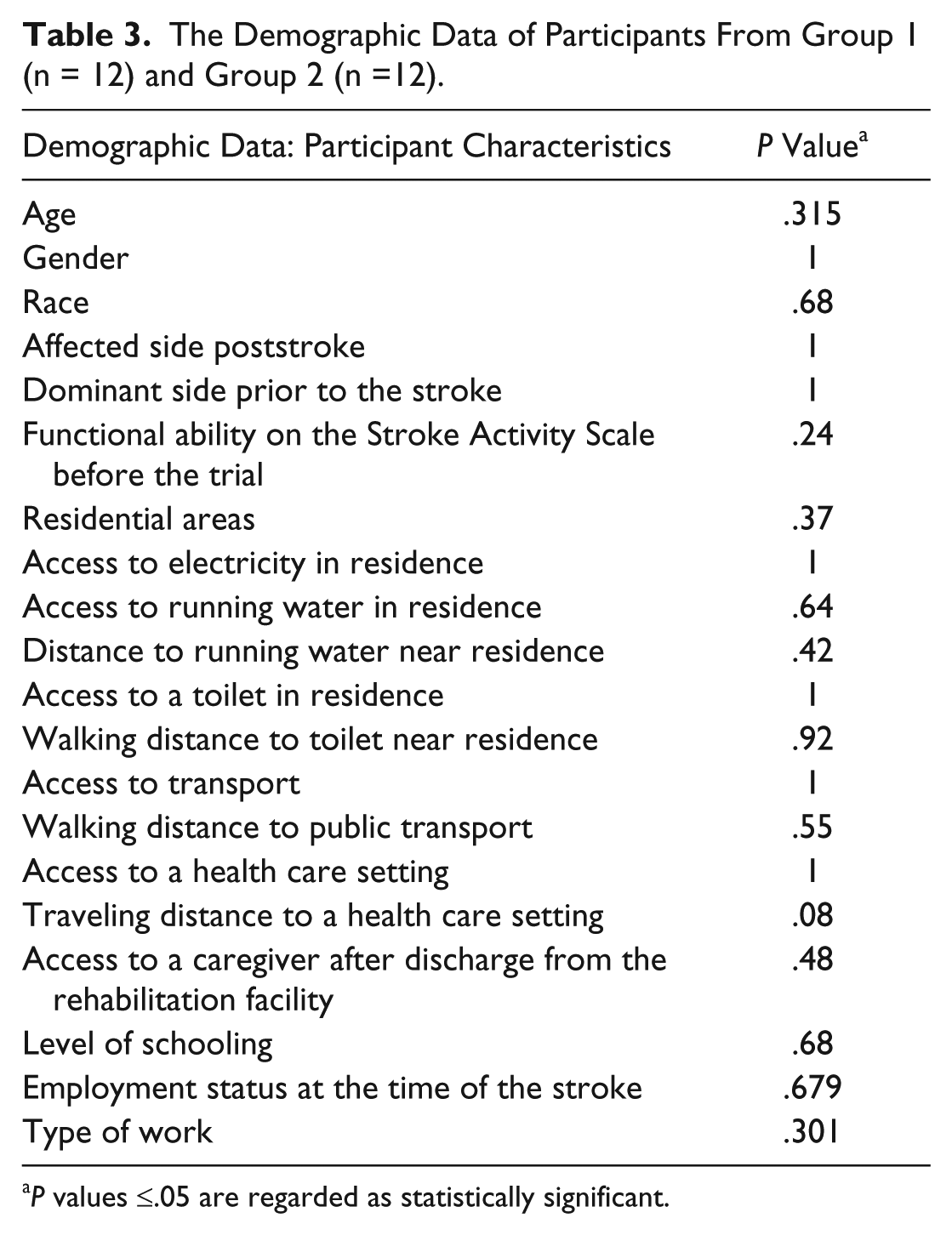
P values ≤.05 are regarded as statistically significant.
King-Devick Test to Assess the Effect of the Interventions on Participants’ Oculomotor Function
For descriptive purposes, it was assumed that given the limited number of participants in each group, all data were nonnormally distributed. Group 1 and group 2 are therefore described by means of medians and 25th and 75th percentiles in Figures 2 to 4. For comparisons between groups at weekly assessments, Mann–Whitney U tests were done without adjustment for multiple comparisons. No statistical difference was noted on the King-Devick Subtest 1 (P = .82), King-Devick Subtest 2 (P = .57), and King-Devick Subtest 3 (P = .15) at baseline between group 1 and group 2. The implications of the King-Devick Subtest 1, King-Devick Subtest 2, and King-Devick Subtest 3 scores at baseline are that the residual oculomotor function in participants from group 1 and group 2 was similar at the beginning of the study. Based on the interpretation of the King-Devick Subtests 1, 2, and 3 scores, participants in both groups suffered from poor oculomotor function and impairment of the visual efficiency processes, specifically slow saccadic eye movements, at the beginning of the study.
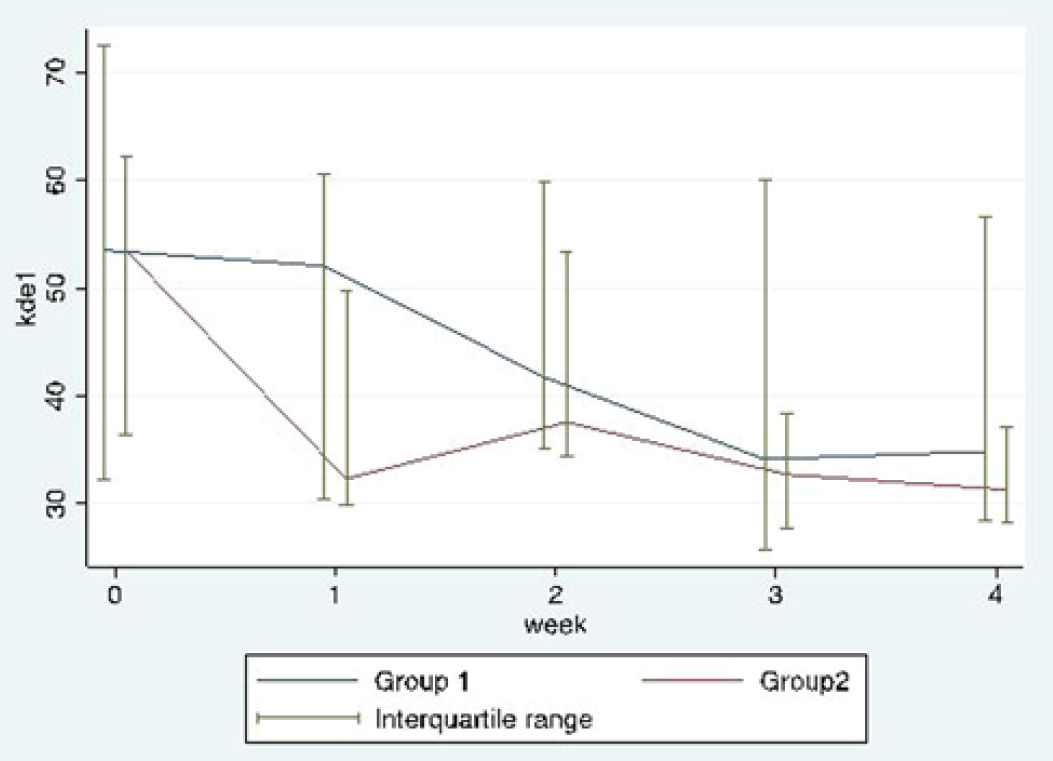
Median and interquartile range of the King-Devick Test–Subtest 1 over the 4-week intervention period for group 1 and group 2.
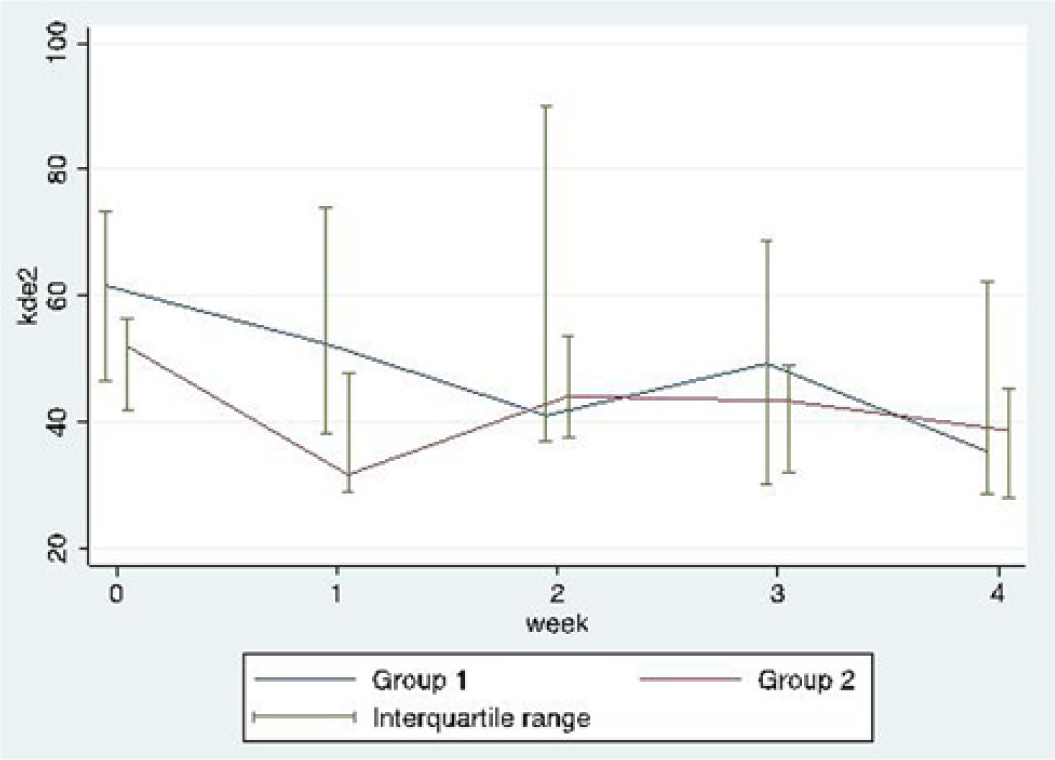
Median and interquartile range of the King-Devick Test–Subtest 2 over the 4-week intervention period for group 1 and group 2.
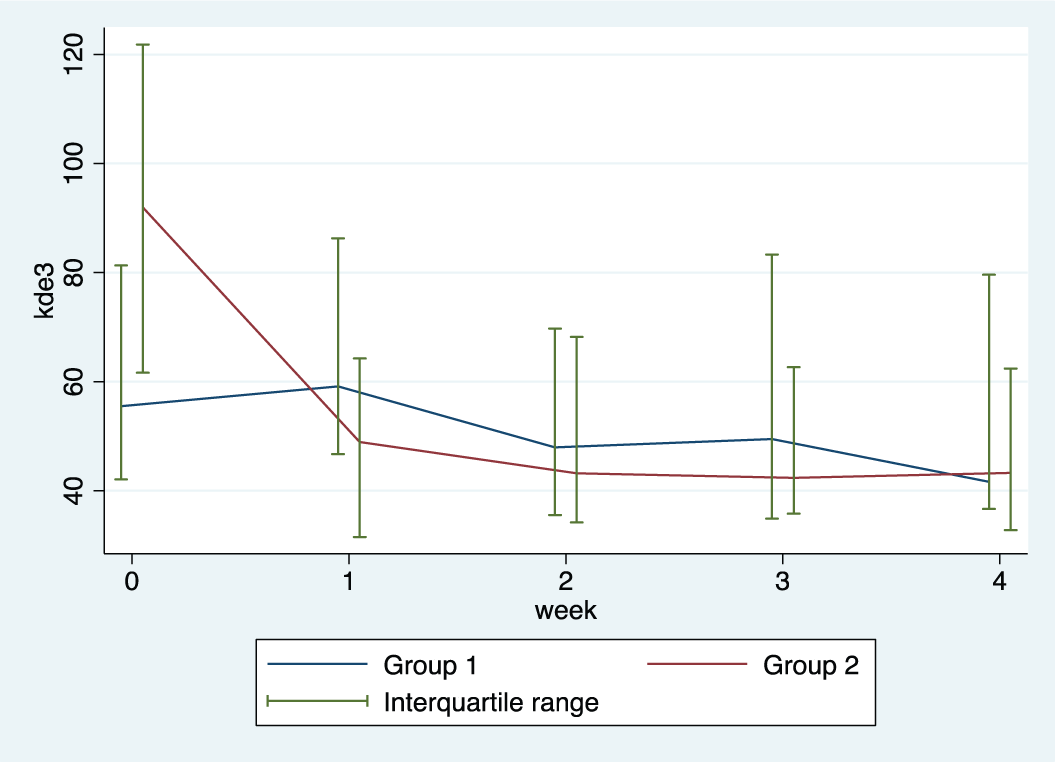
Median and interquartile range of the King-Devick Test–Subtest 3 over the 4-week intervention period for group 1 and group 2.
Impairment of the oculomotor function and visual efficiency processes, specifically slow saccadic eye movements, in participants from group 1 and group 2 improved over the 4-week intervention period. To compare outcomes at week 4, the mixed-model rank ANCOVA analysis was used (adjusting for matching and baseline values). Week 4 and baseline values were ranked and the ranked values were used in the regression analysis. Thus, comparing ranks of both groups after the 4-week intervention period and adjusting for matching and baseline values, the King-Devick Subtest 1 (P = .45) and King-Devick Subtest 2 (P = .76) scores at week 4 were not significantly different for the 2 groups.
Comparing ranks of both groups after the 4-week intervention period and adjusting for matching and baseline values, the King-Devick Subtest 3 score at week 4 was statistically significantly better in participants from group 1 compared with those from group 2 (P = .02). The oculomotor strategies and visual efficiency processes, specifically the saccadic eye movements required to complete the King-Devick Subtest 3, were significantly better in participants from group 1 compared with those from group 2 (P = .0211). The implication is that participants from group 1 presented with better oculomotor function, visual efficiency processes, and saccadic eye movements compared with participants from group 2 postintervention. The King-Devick Subtest 3 is the most advanced subtest of the King-Devick Test in the sense that the King-Devick Subtest 3 requires larger saccadic eye movements and visual search strategies than King-Devick Subtests 1 and 2. It is interesting to note that the difference in the 2 groups presented only in the more difficult test, which displays a higher level of oculomotor function, visual efficiency processes, and saccadic eye movements and not in the easier King Devick Subtests 1 and 2.
Star Cancellation Test to Assess the Effect of the Interventions on Participants’ Unilateral Spatial Neglect
A near statistical difference was noted on the Star Cancellation Test at baseline where group 2 was slightly higher than group 1 (P = .06). The implication of the Star Cancellation Test score at baseline is that the level of USN in the near extrapersonal space observed in participants from group 2 was slightly better than in participants from group 1 prior to the intervention (see Figure 5).
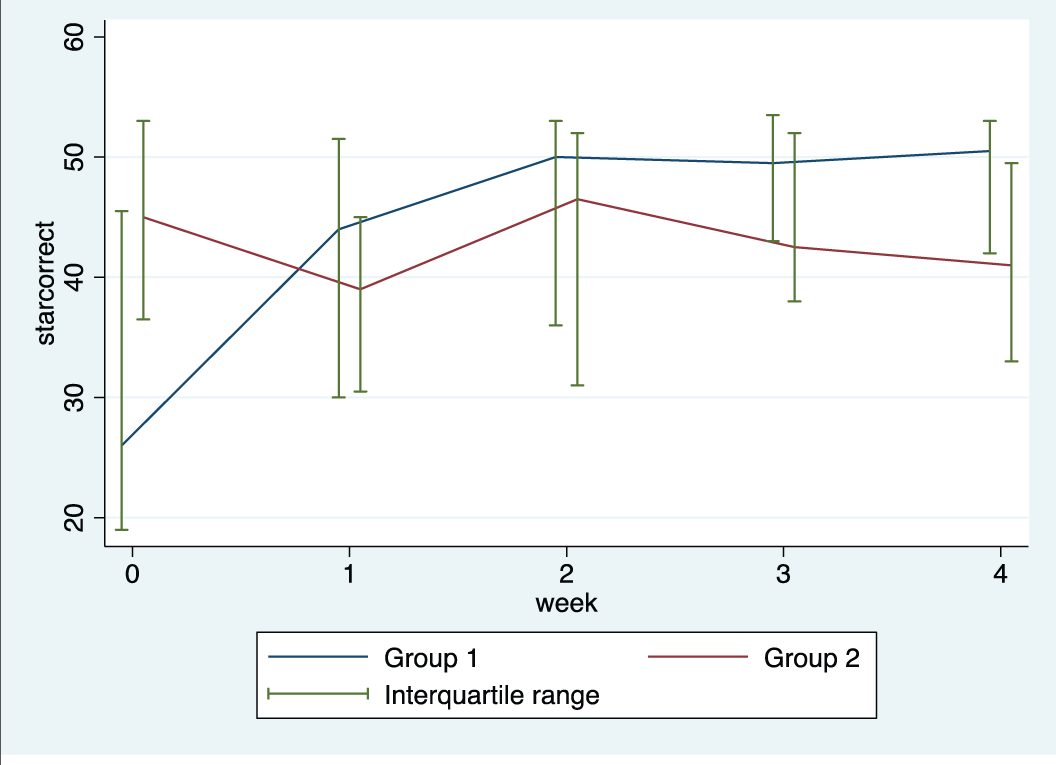
Median and interquartile range of the Star Cancellation Test over the 4-week intervention period.
The number of “cancelled” stars by participants in group 1 increased over the intervention period of 4 weeks. Based on the interpretation of the Star Cancellation Test, the USN in the near extrapersonal environment noted in participants from group 1 improved over the 4-week intervention period. To compare outcomes at week 4 and adjusting for baseline values, the mixed-model rank ANCOVA analysis was used. The baseline values and week 4 were ranked and the ranked values were used in the regression analysis. Comparing the difference in ranks of stars “cancelled” after adjusting for matching and baseline values, participants from group 1 were statistically significantly (P = .02) better than participants from group 2. The number of “cancelled” stars by participants from group 2 decreased over the intervention period of 4 weeks. According to the interpretation of the Star Cancellation Test, the USN noted in participants from group 2 at baseline worsened over the 4-week intervention period.
Barthel Index to Assess the Effect of the Interventions on Participants’ Functional Ability
The BI score at baseline was fairly similar in group 1 and group 2. No statistical difference was found between the groups at baseline (P = .54). Based on the interpretation, the BI score at baseline of participants in group 1 and group 2 was an indication of severe dependence in the performance of ADLs at the beginning of the intervention period. Prior to the intervention, the levels of dependence in participants from group 1 and group 2 were fairly equal (see Figure 6).
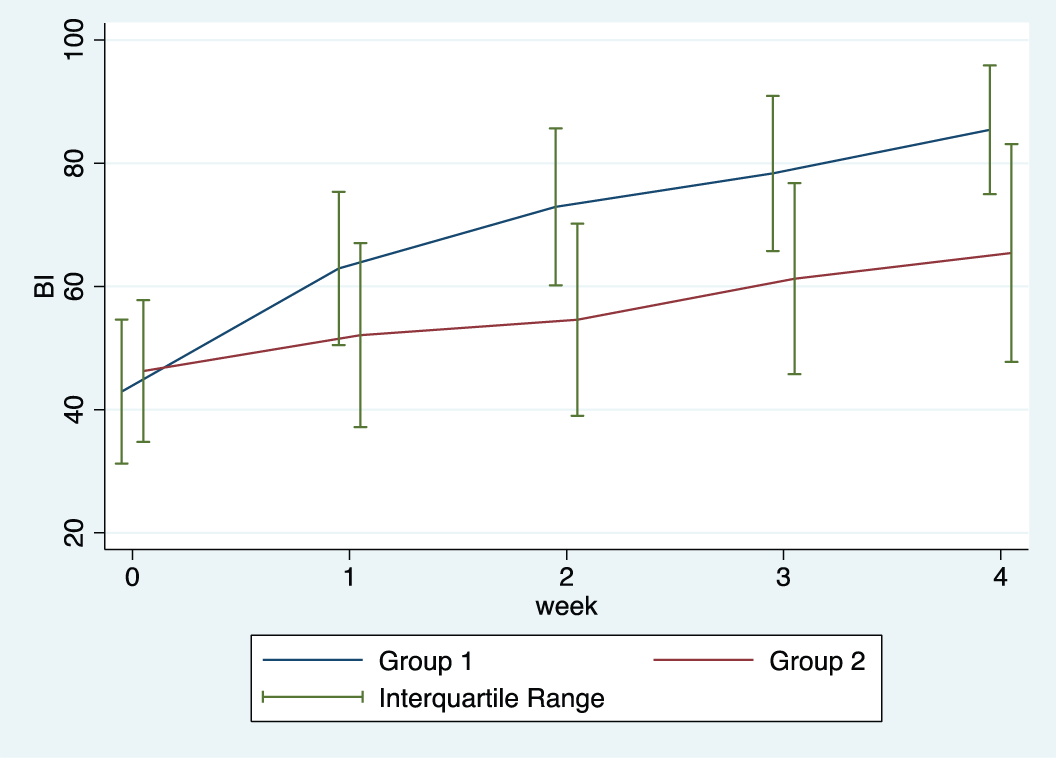
Median and interquartile range of the Barthel Index of participants from group 1 and group 2 over the 4-week intervention period.
The BI score of participants in group 1 increased to a large extent over the 4-week intervention period, indicating that the level of dependence of participants in group 1 had decreased over the 4-week intervention period to a “moderate” level of dependence. Participants from group 1’s level of functional performance in ADLs improved statistically significant over the intervention period.
The BI score of participants in group 2 increased minimally over the 4-week intervention period. The interpretation of the BI postintervention implies that participants from group 2 continued to present with a severe dependence in the performance of ADLs. A statistically significant difference (P = .04) was noted when the functional improvement between the 2 groups after the intervention period was compared with the mixed-model rank ANCOVA analysis (adjusting for matching and baseline values). Week 4 and baseline values were ranked and the ranked values were used in the regression analysis. Comparing the difference in ranks adjusted for matching and baseline values was also statistically significant (P = .004) between group 1 and group 2 after the 4-week intervention period. Participants from group 1 presented with a higher level of functional performance in ADLs compared with participants from group 2 after the intervention period.
Figure 7 demonstrates the individual profiles of the BI of participants from group 1 and group 2 over the 4-week intervention period. One participant from group 1 and one participant from group 2’s BI score at baseline implied a total dependence in the performance of functional activities prior to the intervention period. At baseline, 8 participants from each group presented with a BI score that indicated a severe dependence in the performance of ADLs at the beginning of the intervention period. Three participants from group 1 and 3 participants from group 2 presented with a “moderate” level of dependence at baseline. No participants from either group required minimal assistance with the completion of ADL preintervention. No participants from either group could independently perform ADLs at the beginning of the study.
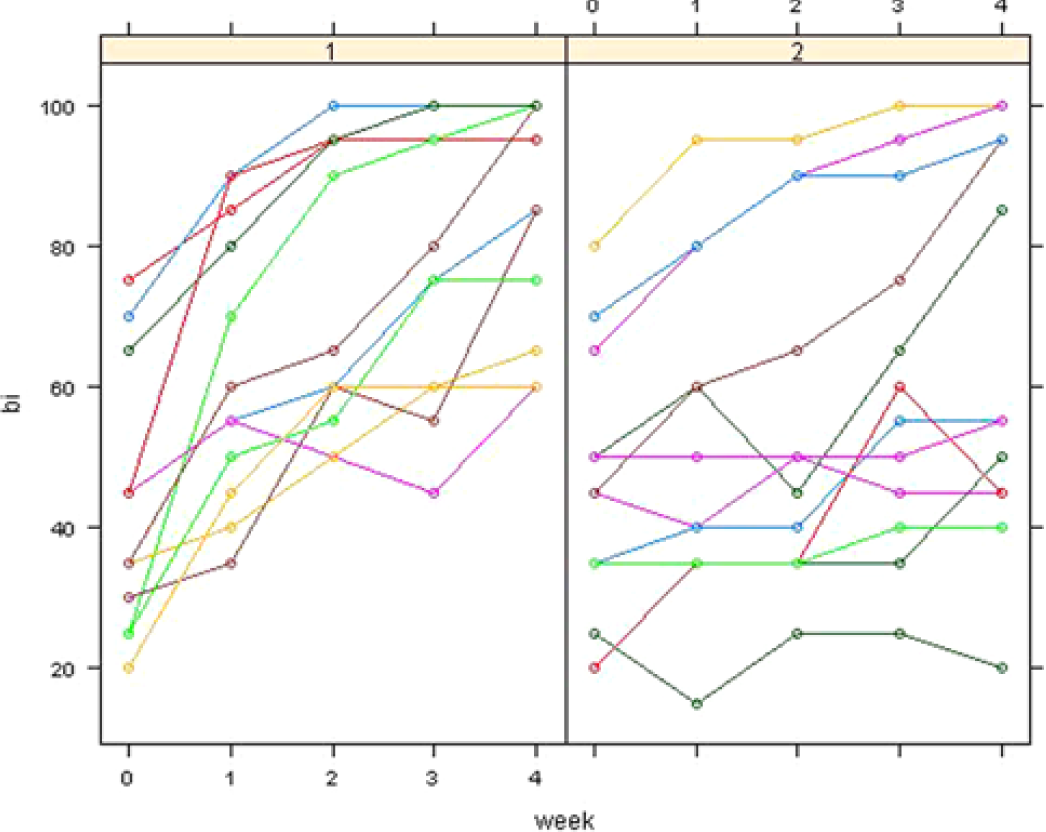
The individual profiles of the Barthel Index (BI) of participants from group 1 and group 2 over the 4-week intervention period.
After the 4-week intervention period, one participant from group 2 continued to be totally dependent in the performance of ADLs. Participants with a level of severe independence in the performance of ADLs at baseline decreased from 8 participants in each group, respectively, to 2 participants in group 1, compared with 6 participants in group 2 at week 4. Four participants from group 1 and 1 participant from group 2 presented with a “moderate” level of dependence after the intervention period. Participants that required only minimal assistance in the performance of ADLs increased from 0 participants at baseline to 1 participant in group 1 and 2 participants from group 2 postintervention. Five participants from group 1 compared with 2 participants from group 2 were independent in the performance of functional activities at the end of the intervention period.
Discussion
Based on the interpretation of the weekly King-Devick Test, specifically the King-Devick Subtest 3, participants in groups 1 and 2 presented with decreased oculomotor strategies and visual efficiency processes at baseline. After the 4-week intervention period, participants in group 1 presented with improved (a) oculomotor function and (b) oculomotor visual performance during reading as assessed on the King-Devick Subtest 3 compared with participants in group 2 postintervention.
The presence of decreased oculomotor function, visual efficiency processes and saccadic eye movements are associated with USN and visual perceptual dysfunction.3,4,38 The interpretation of the Star Cancellation Test demonstrates that the USN noted at baseline in the participants in group 2 was better than in participants in group 1. The participants from group 1 demonstrated a significant improvement in the USN over the 4-week intervention period. The USN noted in participants from group 2 at baseline increased over the 4-week intervention period. Participants from group 2 continued to present with USN in the near extrapersonal space postintervention. After the 4-week intervention period, participants in group 1 presented with (a) decreased USN and (b) improved visual perceptual processing as assessed by the Star Cancellation Test compared with participants in group 2. Participants in group 2 presented with an increased USN and poor visual perceptual processing compared with the participants from group 1 after the 4-week intervention period.
These results confirm findings from other studies that show that the presence of decreased oculomotor function, visual efficiency processes, and saccadic eye movements are associated with USN and visual perceptual dysfunction, which leads to substantial functional disability during daily life activities.3,4,38 Perceptual impairments, specifically USN, are a significant cause of disability following a stroke and can adversely affect a patient’s ability to safely and efficiently mobilize in and around the house as well as at work and in the community. Visual perceptual impairment also affects the patient’s ability to perform most tasks in the work environment, reading and enjoyment of many recreational activities and, as such severely affect a stroke survivor’s overall quality of life. 37
From the literature it is clear that the functional activities that theoretically should improve when USN and visual perceptual processing improve are (a) personal hygiene and self-care activities, (b) dressing, (c) eating, (d) kitchen activities, (e) walking up and down stairs, (f) walking over uneven surfaces, (g) walking through an aisle, (h) communication, (i) finding objects, (j) writing, (k) reading, (l) driving, (m) recreational activities and hobbies, and (n) social interactions. The result of the change in USN and oculomotor function was compared to the functional activities tested on the BI. The activities that were included in the BI correspond with the activities listed above from the literature.
The increased USN noted in participants in group 2 was associated with poor oculomotor function, decreased visual efficiency processes, slow saccadic eye movements and a severe dependence in the performance of ADLs after the intervention period. The improved USN and perceptual processing noted in participants in group 1 were associated with a significantly improved oculomotor function, visual efficiency processes, saccadic eye movements, and a higher level of functional performance in ADL compared with participants from group 2 after the 4-week intervention period.
Conclusions
The results of this study are supported by findings from previously published literature: (a) Individuals’ ability to move effectively and efficiently in their environment is affected by the successful interaction between the individual’s perceptual systems that precedes the motor response and determines the success or failure of the motor action and task completion within a particular environment. (b) Individuals with visual impairment and decreased oculomotor visual performance caused by a stroke may present with visual perceptual deficits—specifically USN—affecting their movement and their functional outcome. (c) The effect of saccadic eye movement training with visual scanning exercises as an intervention has a significant effect on the visual perceptual processing of participants that present with USN poststroke. (d) The significantly improved USN and perceptual processing poststroke translated to significantly better visual function and ability to perform the visually guided ADLs following the stroke. (e) Intensive saccadic eye movement training can decrease USN in patients poststroke, as well as re-train and enhance a patient’s visual perceptual processing with associated improvements in functional ability.
Footnotes
Acknowledgements
We thank the Medical Research Council of South Africa for the grant received to conduct the study. Thank you to all the research assistants for their assistance and commitment throughout the study. Without them, the study would not have been possible. Thank you to Mrs Barbara English for the language editing of the research article.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: Research funding to conduct the study was obtained from the Medical Research Council of South Africa.