
Abstract
Background. Patients with neglect ignore or respond slower to contralesional stimuli. Neglect negatively influences independence in activities of daily living (ADL). Prism adaptation (PA) is one of the most frequently studied treatments, yet there is little evidence regarding positive effects on neglect behavior in ADL. Objective. To assess whether PA in the subacute phase ameliorates neglect in situations of varying complexity. Methods. A total of 70 neglect patients admitted for inpatient stroke rehabilitation received either PA or sham adaptation (SA) for 2 weeks, with full access to standard treatment. There were 7 time-dependent measurements (baseline and 1-4, 6, and 14 weeks after start of treatment). The primary outcome was change of neglect as observed during basic ADL with the Catherine Bergego Scale (CBS). Secondary outcomes were changes in performance on a dynamic multitask (ie, the Mobility Assessment Course [MAC]) and a static paper-and-pencil task (ie, a shape cancellation task [SC]). Results. In all, 34 patients received PA and 35 SA. There were significant time-dependent improvements in performance as measured with the CBS, MAC, and SC (all F > 15.57; P < .001). There was no significant difference in magnitude of improvement between groups on the CBS, MAC, and SC (all F < 2.54; P > .113]. Conclusions. No beneficial effects of PA over SA in the subacute phase poststroke were observed, which was comparable for situations of varying complexity. Heterogeneity of the syndrome, time post–stroke onset, and the content of treatment as usual are discussed. Basic knowledge on subtypes and recovery patterns would aid the development of tailored treatment.
Keywords
Introduction
A frequent poststroke disorder in lateralized attention is visuospatial neglect (neglect). Patients with neglect ignore—or respond slower to—contralesional stimuli, without being aware of it.1,2 Of all stroke patients, 20% to 80% show neglect, depending on the moment and task used. 3 Generally, spontaneous recovery occurs within the first 3 months post–stroke onset, but in 40% of neglect patients, the disorder is still present 1 year later. 4 Neglect patients need more help in activities of daily living (ADL) compared with patients without neglect and are less likely to be discharged home.5,6 Adequate treatment of neglect is, therefore, of great importance.
The current neglect treatment is mainly visual scanning training, a compensatory treatment with emphasis on top-down strategies. 7 Its effectivity, however, remains unproven. 8 Additionally, several restorative treatments have been developed, of which prism adaptation (PA) is the most frequently studied (ie, 16 randomized controlled trials [RCTs]).9-24 The PA paradigm was developed by Rossetti et al, 9 and their PA procedure is used in most studies. During PA, patients wear prism glasses that produce an ipsilesional lateral shift of the visual field. Adaptation to this optical shift requires a set of successive visuomotor pointing movements. When the prisms are removed, attention is automatically shifted contralesionally. Of RCTs that included neuropsychological neglect tasks,9,10,12-24 in 60%, PA diminished neglect as measured with at least 1 of these pen-and-paper tasks.9,10,12-15,17,18,24 There is, however, little evidence regarding whether PA diminishes neglect in ADL because paper-and-pencil tasks lack the dynamics and complexity of daily life. 25 Of RCTs that included measures at the level of (basic) ADL,16,17,19,21-23 in only 33% did neglect behavior decrease more after PA compared with no or control treatment.17,19 This inconsistency between results is probably a result of the lack of comparability between studies (eg, treatment procedure, intensity, tasks) or a general lack of methodological quality (eg, small groups [11-43], no right-sided neglect, measures of ADL in only 38% of studies, follow-up measurements in only 25% of studies). In sum, it is uncertain whether PA should be implemented in rehabilitation. The effectiveness of other rehabilitation interventions (eg, limb activation training, optokinetic stimulation, eye patching) also remains unproven. 8 More high-quality (ie, adequate statistical power, randomization, ADL measures, follow-up), pragmatic RCTs in a clinical setting are needed.8,26
We conducted an RCT in which the aforementioned issues were considered. Our primary aim was to determine whether treatment with PA in the subacute phase ameliorated neglect behavior in basic ADL (as measured with the Catherine Bergego Scale [CBS]) to a larger extent compared with sham adaptation (SA). In addition, to eliminate the influence of compensation strategies, we used the Mobility Assessment Course (MAC), a dynamic multitask. 25 Finally, a cancellation task was included, which is a widely used measure for neglect. 27 We included stroke patients with left- and right-sided neglect. Patients with right-sided neglect have not been included in prior trials. Finding a treatment for this group of patients is, however, necessary because consequences of left- versus right-sided neglect in ADL are largely comparable. 28
We included patients in the subacute phase poststroke. A general consideration for early treatment is the plasticity of the brain. Spontaneous neurobiological recovery occurs within all domains and lasts around 90 days.4,29 The main part of recovery during this critical period is likely driven by spontaneous recovery, and the effects of rehabilitation interventions are much smaller. They may, however, improve or extend the duration of neuroplasticity.29-31 A more specific consideration is that patients with neglect ignore one side of their body or space in the acute phase poststroke and learn not to use this side of the body or hemifield. Early treatment might minimize this learned nonuse, and larger effects of PA could potentially be obtained. 13
Methods
Research Design
A single-center, randomized, double-blind (ie, regarding the primary outcome), parallel-group study with an allocation ratio of 1:1 (ie, an equal number of patients was allocated to each group) was conducted (for the trial protocol, see Ten Brink et al 32 ). A rehabilitation physician was consulted by the investigator regarding the inclusion and exclusion criteria (see below). Patients gave written informed consent. The nurses, physical therapist, and occupational therapist who filled in the CBS were blinded to the treatment conditions. The investigator (AFTB) who treated and tested the patients regarding the secondary outcomes was not blinded to the treatment because she had to put on the goggles. If possible, tests were computerized to increase objectivity. Patients could not be (completely) blinded to the treatment because they had to wear the goggles. However, patients were not explicitly told which treatment they received, and none of them expressed any awareness of assigned condition (after informal enquiry). Patients were tested at baseline and after 1, 2, 3, 4, 6, and 14 weeks from the start of treatment. The MAC was assessed at baseline and after 2, 4, and 14 weeks.
The study was conducted according to the principles of the Declaration of Helsinki (64th WMA General Assembly; October; Fortaleza, Brazil) and in accordance with the Medical Research Involving Human Subjects Act (WMO). The study was approved by the Medical Ethical Committee of the University Medical Centre Utrecht.
Participants
Stroke patients with a clinical diagnosed symptomatic stroke (first or recurrent, ischemic, or intracerebral hemorrhagic lesion) admitted consecutively to De Hoogstraat Rehabilitation Centre in Utrecht, the Netherlands, were considered for inclusion. Patients had to be aged between 18 and 85 years and have sufficient comprehension and communication skills. Patients were not included in case of interfering psychiatric disorders or substance abuse, when they were physically or mentally unable to participate, or when the expected discharge was <3 weeks.
Neglect Screening
All patients were screened for neglect per usual care within the first 2 weeks after admission. Patients could enroll when they showed neglect on the shape cancellation task (SC), line bisection, or CBS (see subsection “Primary outcome”; a CBS score of ≥6 was used as a threshold for neglect 33 ). The SC (see subsection “Static task—SC”) and line bisection were administered on a computer monitor. 34 The line bisection task consisted of 3 horizontal lines (22° long, 0.2° thick1) that were presented at upper right, at lower left, and in the horizontal and vertical center. The stimulus presentation was approximately 19° wide and 5.7° high1. Patients had to mark the midpoint.
The thresholds for neglect were based on the mean plus 3 SDs of 28 healthy individuals. 34 The SC omission difference score ranged from 0 to 1.05, resulting in a threshold of ≥2. The line bisection deviations ranged from −0.77 to 0.81°, −0.85 to 0.48° and −0.89 to 0.42°** for the 3 lines, respectively. A deviation outside normal range on ≥2 lines was used as a threshold.
Apparatus
The treatment and the SC were administered using a 22-inch interactive WACOM (PL2200) tablet screen (1920 × 1080), with a screen size of 477.64 × 268.11 mm. 35 The tablet screen was oriented horizontally and slightly tilted (angle of 18 degrees) with an adjustable stand. Patients had to respond to stimuli by drawing on or pointing at the screen with a digital stylus. DiagnoseIS (developed by Metrisquare, Netherlands) was used to program the SC. The tablet was controlled by a laptop (Samsung NP300E5A-S01NL).
Intervention
The PA procedure was adapted from Rossetti et al. 9 Patients wore a pair of goggles fitted with wide-field point-to-point prismatic lenses, inducing an ipsilesional optical shift of 10° (PA) or goggles with plain lenses (SA). Exposure consisted of ±100 fast pointing movements to 3 stimuli (red, yellow, blue) presented on a horizontal axis at a distance of ±65 cm. 35 The left and right stimuli were located 10° away from the body midline. The investigator indicated which stimulus was the target. A board was held under the chin to prevent viewing of the hand at its starting position but allowing an unobstructed view of the targets and terminal errors. The coordinates of the touch responses were recorded.
Immediately after ending the adaptation phase (either PA or SA), the after effect of adaptation was measured. The goggles were removed, and patients were instructed to look at the central visual target. After a few seconds, patients had to point to the central target with closed eyes to prevent online adjustment of the pointing movement resulting from visual feedback. For successful PA, a contralesional shift of ±3 cm from the target was required. For patients in the PA group, the procedure was repeated once with ±50 pointing movements when the aftereffect was <3 cm.*
The treatment was performed in the rehabilitation center once a day, each working day, for 2 weeks in addition to usual care. Usual care differed per patient and contained ±4 to 6 therapies (eg, physical, occupational, speech; 30-60 minutes) per working day. Neglect treatment consisted of psychoeducation and visual scanning training (ie, search tasks and reading), 1 hour per week, 1 to 6 weeks (3 on average). In addition, during the other therapies and during ALD, patients were occasionally stimulated to attend their neglected side.
Randomization
Before the start of the study, the investigator put 70 printed cards with the treatment condition (35 PA and 35 SA) in envelopes. After completion of the baseline assessment, the investigator opened an envelope and allocated the patient based on the treatment written on the card.
Primary Outcome
The CBS is an observation scale for neglect behavior in ADL.33,36 Neglect severity was scored for each of 10 items on a scale of 0 (no neglect) to 3 (severe neglect) by a nurse, physical therapist, and occupational therapist. Items that were impossible to score (eg, because patients were unable to independently perform the activity or the situation was not observed) were considered invalid and were not included in the total score. For the first 4 items, the score provided by the nurse was used; for the last 6 items, the average score of the 3 disciplines was used. The total score was the sum of the (weighted) item scores, divided by the number of valid items, multiplied by 10 (resulting in a total score ranging from 0 to 30).33,36 In case 5 or fewer items were observed, the total score was considered not reliable and therefore a missing value.
Secondary Outcomes
Dynamic Task: MAC
Patients were instructed to walk or navigate their wheelchair independently at a leisurely pace through a corridor, without stopping or turning back (see Ten Brink et al 25 for a detailed description). Meanwhile, patients had to point out targets (12 per side, yellow, 10 × 10 cm). It was emphasized that there was no time limit, and finding all targets was the main goal. Task assessment lasted approximately 5 minutes. The asymmetry score was computed as the absolute difference between the number of omissions, left versus right.
Static Task: SC
The SC consisted of 54 small targets, 52 large distractors, and 23 words and letters. 35 Patients were instructed to cancel all targets. No time limit was given. The absolute difference in the number of omissions between the left and right sides of the stimulus field (asymmetry score) was computed.
Patient Characteristics
We reviewed the patient’s medical record and captured demographic (age, gender) and stroke-related characteristics (date stroke, stroke history, stroke type, lesion side). Global cognitive functioning was screened with either the Mini-Mental State Examination (MMSE) 37 or the Montreal Cognitive Assessment (MoCA). 38 We converted MMSE scores into MoCA scores to create a single, pooled MoCA score ([1.124 × MMSE] − 8.165). 39 Quality of communication was determined with the Stichting Afasie Nederland test, 40 an observation scale for language communication. Muscle strength was measured by the Motricity Index, a short task to assess the loss of strength in the arm and leg. 41 Independence in ADL was assessed using the Barthel Index. 42 Independence in walking was evaluated with the Functional Ambulation Categories. 43
Data Analyses
Power
An effect size of 0.70 SDs was used to estimate the necessary sample size. To identify a difference with a power of 80% and α of .05 (2-sided), 35 patients per group (70 patients in total) were required for sufficient statistical power. 32
Demographic and Stroke-Related Characteristics
Nonparametric Mann-Whitney and χ2 tests were used to compare demographic and stroke-related characteristics between groups. Baseline neglect variables were compared with a t-test when data were normally distributed and with a Mann-Whitney test when data were not normally distributed.
Outcome Analyses
The analyses were conducted by the available-case, intention-to-treat method; that is, all data were included in the analysis, and the data were analyzed with all patients remaining in the treatment group to which they were initially randomized. A linear mixed-effects model analysis was performed in IBM SPSS Statistics (version 23) 44 for each outcome measure separately. We choose this approach because it is appropriate for repeated measures in a heterogeneous group; the variable time is treated as a continuous measure (which is an advantage because intervals differed between measurements); patients with missing data are included; and covariates can be introduced. 45 The linear mixed-effects model used a heterogeneous first-order autoregressive covariance structure and included a random intercept for each patient. Missing data were handled by a maximum likelihood algorithm under the assumption that the missingness was random. The predictors of theoretical interest were the effects of time and group and the interaction between time and group. These predictors were included in the basic model. The quadratic relation of time, baseline score, number of days poststroke, gender, and age were introduced as potential covariates (fixed effects). This was regardless of whether or not these variables differed between groups, to enhance the fit of the model. To statistically compare the fit of each new model with the old model, the change in −2 log-likelihood (χ2Change = −2LLold – [−2LLnew]) was assessed in light of the number of additional parameters (dfChange = kOld − kNew). 46 The coefficients of the best-performing model were reported (thus, the included covariates could differ between final models, depending on their significance). Significance was set toP = .05.
Secondary analyes were performed in subgroups of patients with right-sided brain damage and moderate to severe neglect on the given task (resulting in different subgroups per task) to compare current results with prior studies and to correct for possible ceiling effects in the outcome measures. Moderate to severe neglect was defined as a CBS baseline score of ≥7, 16 MAC asymmetry score of ≥3, 25 and SC asymmetry score of ≥4. 24 Finally, analyses were repeated with the size of the absolute aftereffect (average of all sessions) as factor, instead of group.
Results
Patient Characteristics
Recruitment to the trial was carried out from November 2013 to November 2016; the final follow-up measurement took place in March 2017. A total of 581 stroke patients were admitted to the rehabilitation wards during the period of recruitment (Figure 1). A total of 70 were included in the study, among whom 1 patient quit during the baseline measurement and was neither randomized nor treated. Two patients in the PA group did not complete the treatment as a result of illness or early discharge (both after 5 sessions).
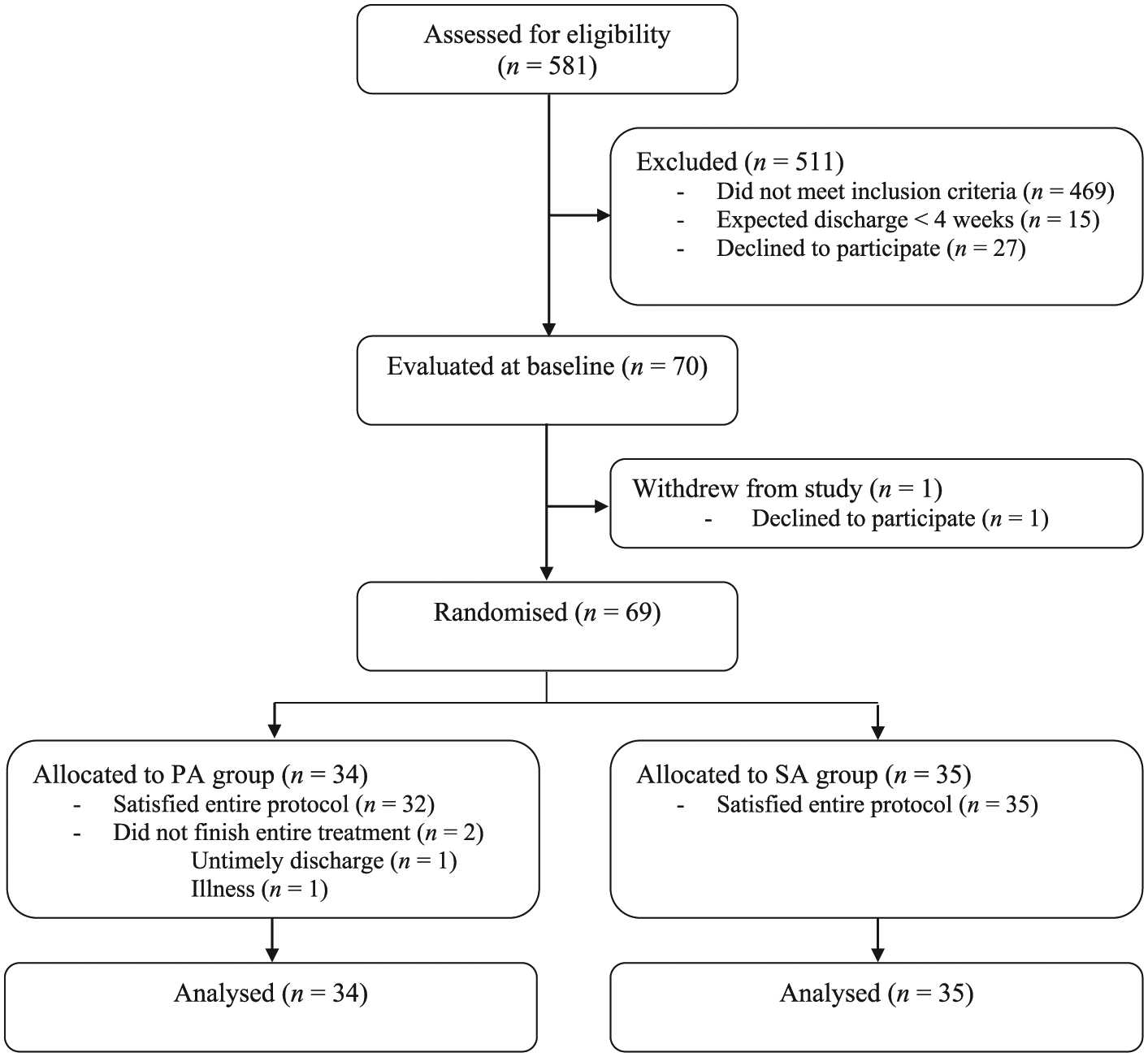
Participant flow through the study.
The groups were comparable with respect to patient characteristics (Table 1; see Supplementary Table 1 for characteristics of patients with right brain damage). Because patients could be included based on abnormal performance on one of neglect tasks (Supplementary Table 2), not all patients showed neglect on all outcome measures when they entered the trial. SC scores at baseline were not normally distributed, so a nonparametric test was used. Overall, scores on neglect measures at baseline were comparable between groups. Raw mean scores for separate patient groups (ie, overall group, right-sided lesions, and left-sided lesions) are depicted in Table 2. Within the right-sided lesions group, patients in the SA group obtained higher baseline CBS scores compared with patients in the SA group.
Median (IQR) Demographic and Stroke-Related Characteristics at Admission, and Mean (SD) Neglect Variables at Baseline, Split Per Group. a
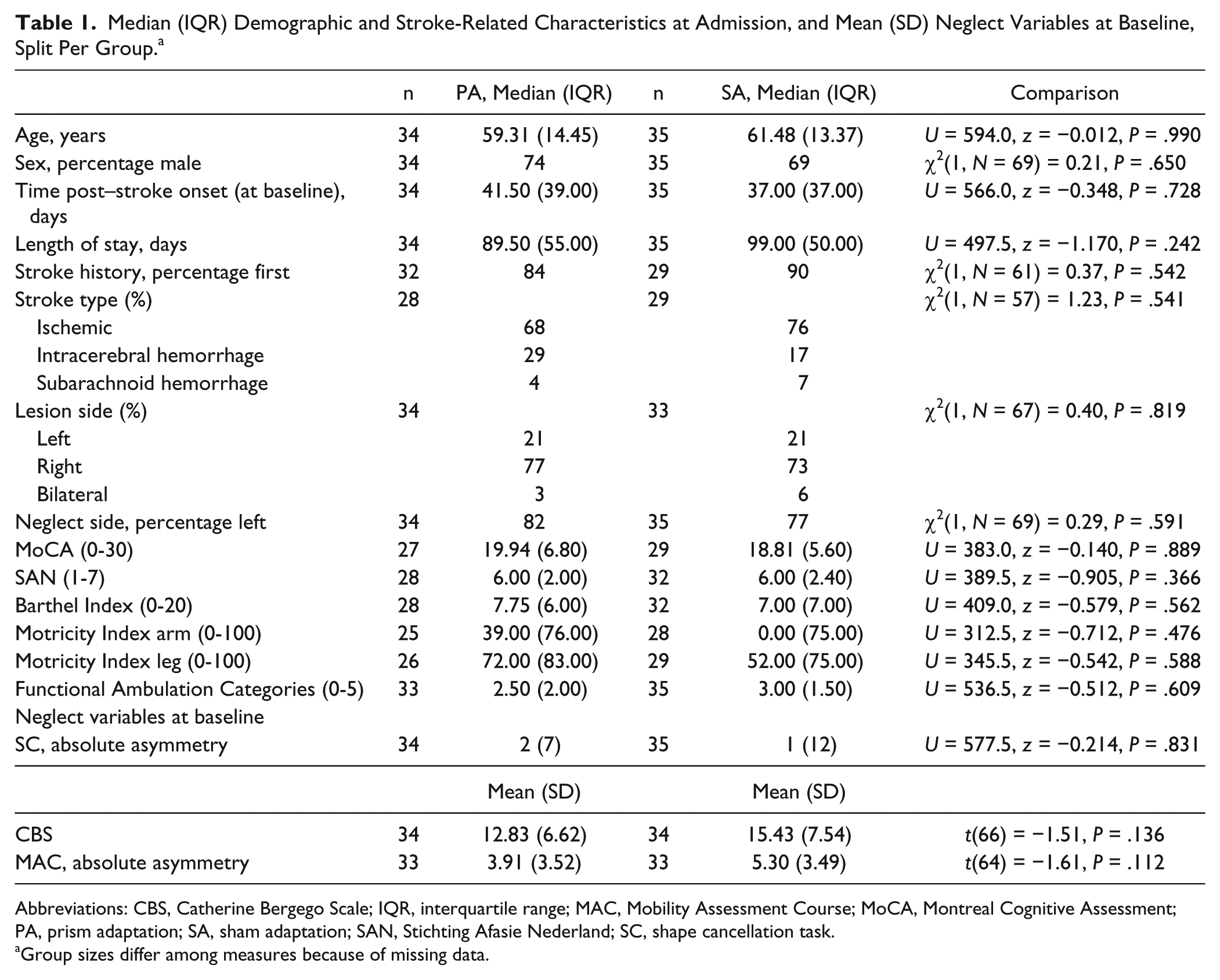
Abbreviations: CBS, Catherine Bergego Scale; IQR, interquartile range; MAC, Mobility Assessment Course; MoCA, Montreal Cognitive Assessment; PA, prism adaptation; SA, sham adaptation; SAN, Stichting Afasie Nederland; SC, shape cancellation task.
Group sizes differ among measures because of missing data.
Mean (SD) Neglect Scores Per Week, Split for Experimental Group and Lesion Side. a
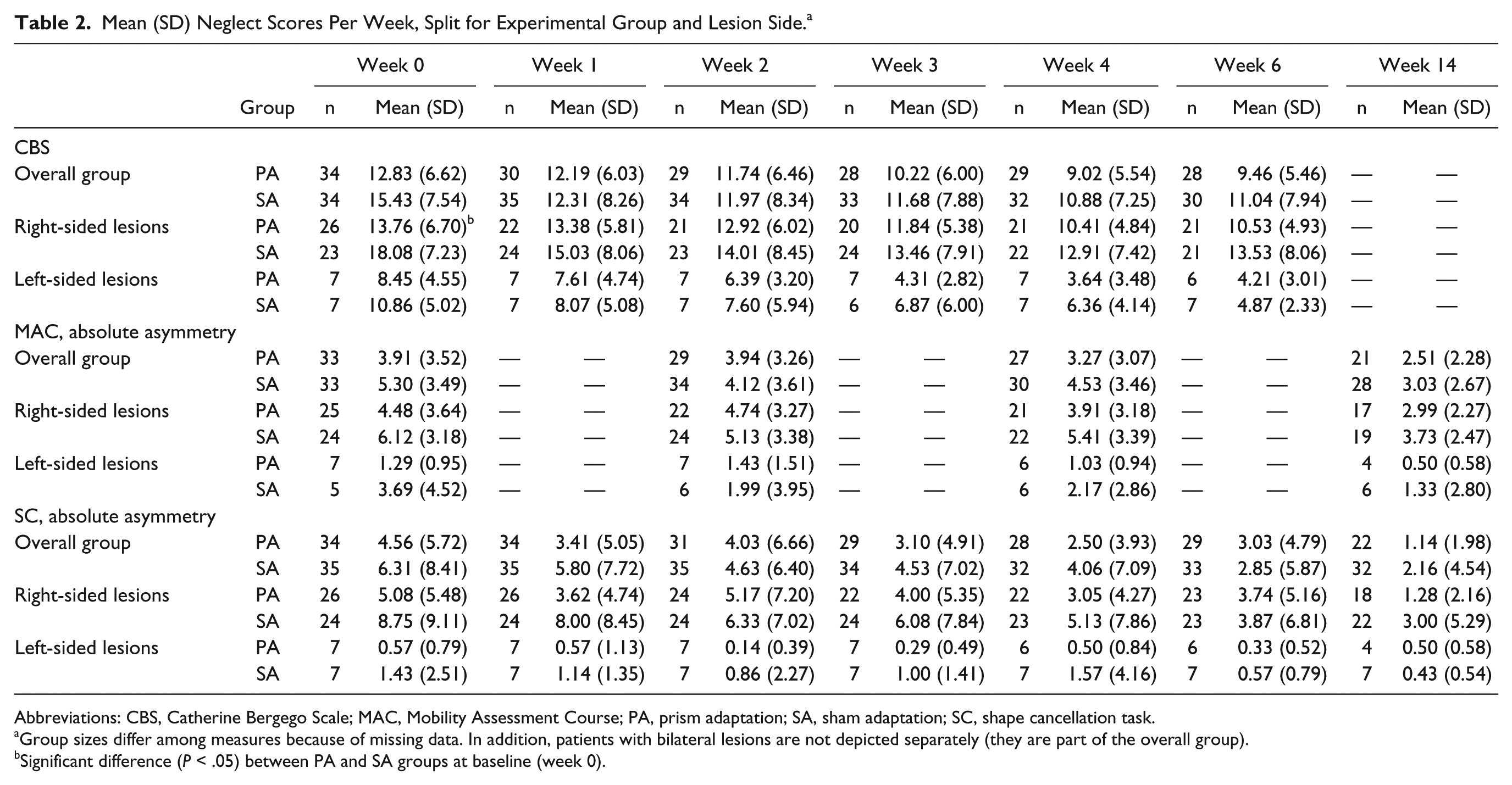
Abbreviations: CBS, Catherine Bergego Scale; MAC, Mobility Assessment Course; PA, prism adaptation; SA, sham adaptation; SC, shape cancellation task.
Group sizes differ among measures because of missing data. In addition, patients with bilateral lesions are not depicted separately (they are part of the overall group).
Significant difference (P < .05) between PA and SA groups at baseline (week 0).
Primary Outcome: Influence of PA on Basic ADL
CBS scores could not be obtained after 14 weeks because most patients were discharged home. The final model included baseline score, days poststroke, and gender as confounders (Table 3). Overall, CBS scores improved over time [F(1, 239) = 38.90; P < .001]. There was no main effect of experimental condition [F(1, 148) = 2.54; P = .113], indicating that the effects of PA and SA on the CBS scores were comparable. Additionally, no interaction effect [F(1, 239) = 2.28; P = .133] was observed, indicating that the pattern of improvement through time was comparable for PA and SA (Figure 2).
Fixed-Effect Predictors and Covariates for Predicting the CBS Total Score Across Weeks 1 to 6 (n = 69).
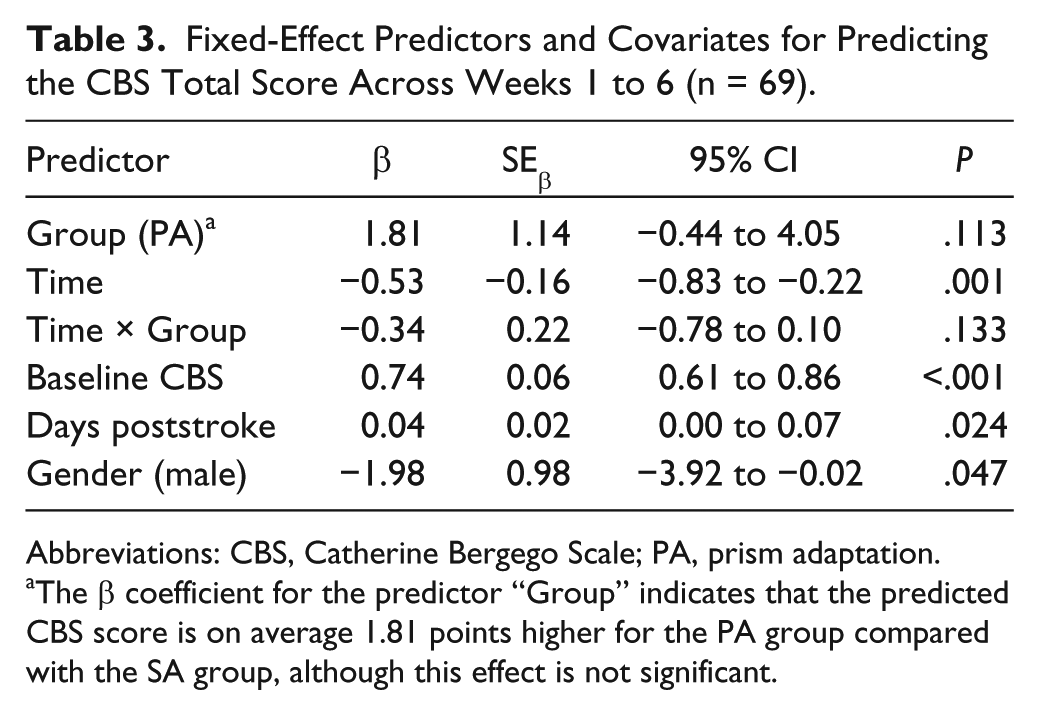
Abbreviations: CBS, Catherine Bergego Scale; PA, prism adaptation.
The β coefficient for the predictor “Group” indicates that the predicted CBS score is on average 1.81 points higher for the PA group compared with the SA group, although this effect is not significant.
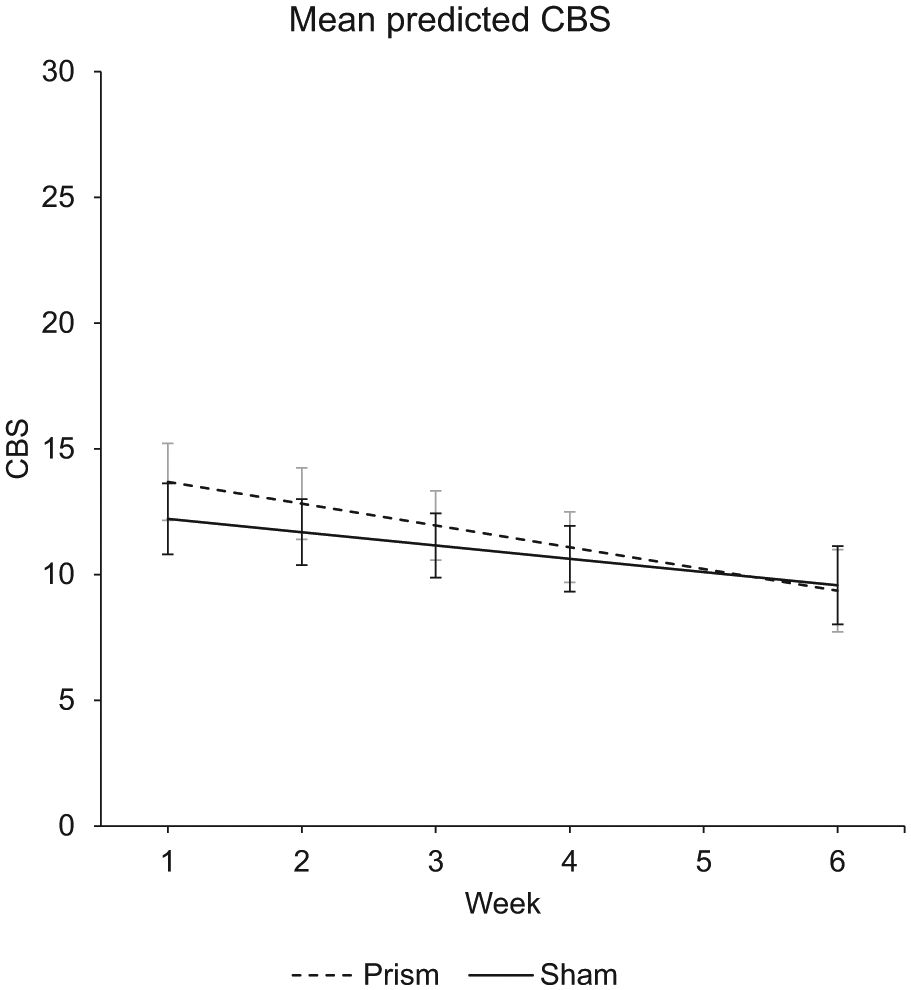
The average model-predicted CBS scores and CIs across assessment sessions for each group: PA (dashed line) and SA (solid line). The assessment session in week 1 occurred after 1 week of treatment, and the assessment session in week 2 occurred after 2 weeks of treatment. Lower scores indicate less severe neglect. Note that scores were corrected for the confounders in the model, including the baseline CBS score. The linear mixed-effects model analysis takes into account the underlying model of the data, correcting for covariates (eg, baseline score and days poststroke) and missing data; therefore, reporting these data points are preferred over observed means.
Subanalyses for patients with right-sided brain damage and moderate to severe neglect (n = 21 in the PA group, n = 21 in the SA group), with aftereffect as factor, resulted in similar findings (Supplementary Tables 3 and 4).
Secondary Outcomes: Influence of PA on Lateralized Attention
The final model for the MAC included the confounder baseline score (Table 4). Overall, patients improved over time with regard to MAC scores [F(1, 110) = 17.53; P < .001]. No effect of experimental condition was found [F(1, 129) = 0.70; P = .406], indicating that the effects of PA and SA on the MAC scores were comparable. In addition, no interaction effect was seen [F(1, 110) = 0.04; P = .851], indicating that the pattern of improvement on MAC scores through time was comparable between groups. Comparable results were obtained when analyses were performed for patients with right-sided brain damage and moderate to severe neglect (n = 15 in the PA group, n = 20 in the SA group) and with aftereffect as factor (Supplementary Tables 5 and 6).
Fixed-Effect Predictors and Covariates for Predicting the MAC Asymmetry Score Across Assessment in Weeks 2, 4, and 14 (n = 69).
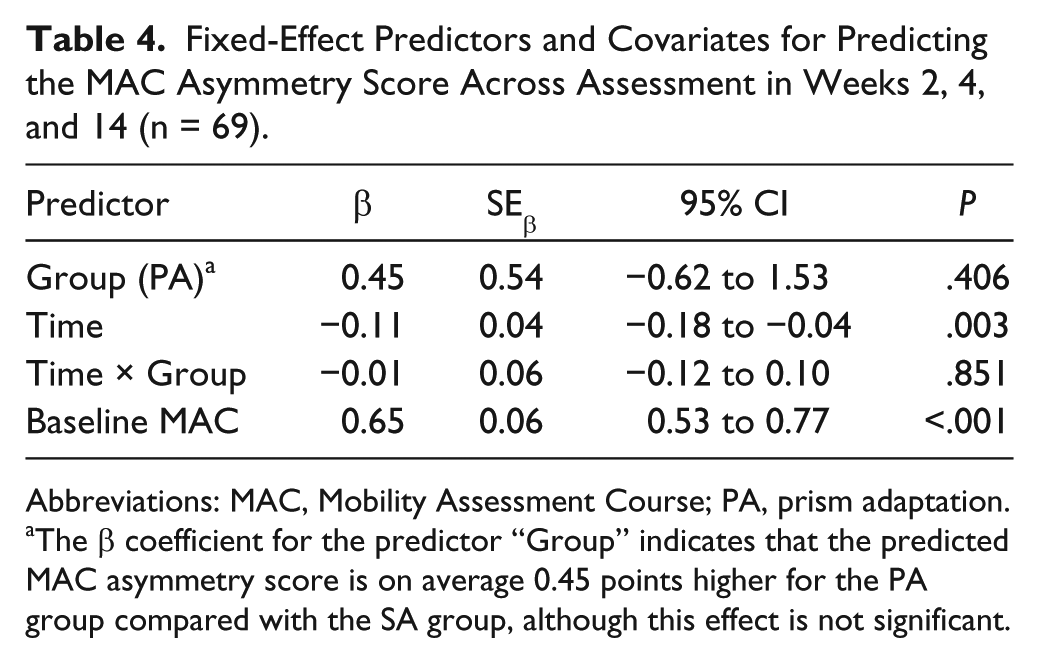
Abbreviations: MAC, Mobility Assessment Course; PA, prism adaptation.
The β coefficient for the predictor “Group” indicates that the predicted MAC asymmetry score is on average 0.45 points higher for the PA group compared with the SA group, although this effect is not significant.
The final model for the SC included the confounder baseline score (Table 5). Overall, scores on the SC improved over time [F(1, 311) = 15.57; P < .001]. There was no effect of group [F(1, 105) = 0.19; P = .661], indicating that SC scores did not differ between patients who received PA compared with SA. Furthermore, no interaction effect was seen [F(1, 311) = 3.65; P = .057], indicating that PA and SA had no differential effects on the pattern of improvement. Similar results were found when analyses were performed for patients with right-sided brain damage and moderate to severe neglect (n = 12 in the PA group, n = 14 in the SA group) and with aftereffect as factor (Supplementary Tables 7 and 8).
Fixed-Effect Predictors and Covariates for Predicting the SC Asymmetry Score Across Weeks 1 to 14 (n = 69).
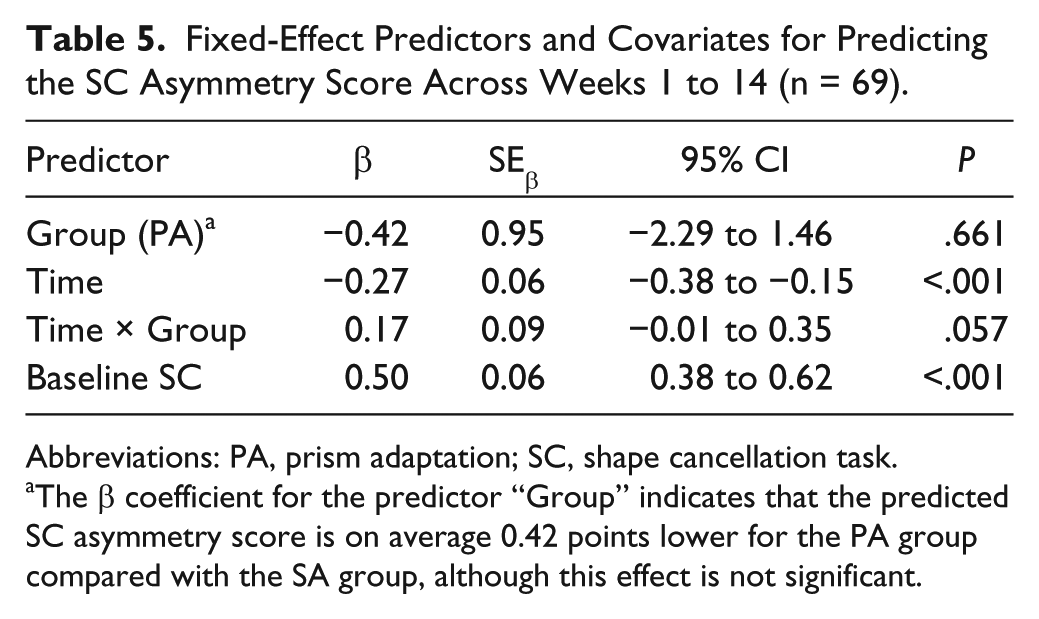
Abbreviations: PA, prism adaptation; SC, shape cancellation task.
The β coefficient for the predictor “Group” indicates that the predicted SC asymmetry score is on average 0.42 points lower for the PA group compared with the SA group, although this effect is not significant.
Discussion
In the current study, 69 stroke patients received 10 sessions of either PA or SA during their admission for inpatient rehabilitation. We measured neglect behavior in situations of varying complexity. Overall, a time-dependent improvement of neglect behavior was observed on all measures (ie, CBS, MAC, and SC), but no differences were found between PA and SA groups. Comparable results were found when we subsequently performed subanalyses including only patients with moderate to severe neglect and right hemisphere lesions or with aftereffect as a factor.
How do these results relate to earlier findings? We evaluated 5 RCTs (of which 2 are recent)22,24 that were comparable to ours regarding the time post–stroke onset (1-2 months on average), intensity of the treatment (4 to 20 sessions), and inclusion of a control group (SA).13,16,19,22,24 Only 2 of these used the CBS to measure neglect behavior in ADL. In these studies, no beneficial effects of PA over SA were reported.16,19 These results should, however, be interpreted with caution because it was estimated by Turton et al 16 that inclusion of at least 32 patients in total is necessary to observe clinically relevant treatment effects on the CBS, which was not the case in these studies. In our study—with a larger sample of patients (n = 69)—however, no treatment effects were found either. Two prior studies used the Functional Independence Measure. Here, long-term positive effects of PA were seen in 1 study (for mild neglect only), 19 but not in another. 22 Although all early studies (including ours) reported improvement in basic ADL over time, it is uncertain to what extent this change is related to an actual improvement of the core deficit in neglect: lateralized inattention. Because only basic activities are observed with the CBS and FIM, improvement could relate to the use of compensatory strategies, especially because many of these basic activities are practiced daily during inpatient rehabilitation. In all 5 studies, the lateralized attention deficit was also measured with (different) neuropsychological neglect tasks. In general (with the exception of positive findings on a few tasks), no beneficial effects of PA were found directly after treatment16,19 or during follow-up compared with SA.13,16,19,22,24 With cancellation tasks, in which no time limit is provided, compensation strategies are quite easily incorporated. Results on dynamic multitasks in a daily life environment, such as the MAC in our RCT, have not been reported yet. Visual search while moving (MAC) is not used in daily routines, such as basic ADL, and it is more dynamic in nature compared with neuropsychological tests. 25 Nevertheless, no difference was seen between groups on MAC performance in the current study. Because it is a fairly new test, it remains to be seen to what extent this task is insensitive to compensation strategies or leaves less room for compensation. In sum, in most early-onset RCTs, few beneficial effects of PA over SA are reported. This is in sharp contrast to the RCTs in the later and/or chronic phase, in which positive effects of PA compared with SA (or no treatment) were reported on at least 1 outcome measure in all studies9-11,14,17,18 but one. 20 Note that this is a rough comparison because studies differed regarding treatment characteristics, such as intensity. However, looking at studies with low (1 session in total)9,11,47 versus high (5 sessions per week)16,20 intensity does not suggest that a higher intensity results in better outcome.
It has been argued that SA (the control treatment) is a form of visuomotor training and could, therefore, also diminish neglect. 18 The SA procedure requires the patient to plan and perform a series of movements toward stimuli in the ipsilesional and contralesional fields. Half of the movements (ie, toward contralesional stimuli) might train the orientation of the sensorimotor system toward the neglected side. The study of Serino et al, 14 however, indicated that patients wearing sham goggles improved only a little, whereas their performance on neuropsychological tests greatly improved when they subsequently received PA. In several other studies, no improvement was found in the SA group, whereas the PA group improved.9,11,17 It seems, therefore, more likely that other factors led to recovery of patients receiving SA.
Timing of treatment, therefore, seems to be the crucial factor for significant beneficial effects of PA. In the first 3 months poststroke, a neglect patient group is more heterogeneous compared with a later stage. There are 2 important mechanisms that may enhance the heterogeneity: first, spontaneous neurobiological recovery in the first 3 months post–stroke onset is variable between patients.4,48 About half of patients with neglect in the first week poststroke do not show neglect as measured with a cancellation task 12 weeks later. 4 Second, treatment responsiveness on the existing multidisciplinary rehabilitation program could differ between patients. In particular, the visual scanning training may have the largest impact on the use of compensation strategies to avoid impairment during (simple) activities in daily living resulting from the lateralized attention deficit (see above). In the chronic phase, therefore, the group is more homogeneous compared with the early phase because quick-recovering patients are not included.
Evaluating intervention effects (of PA or other interventions) for neglect on a group level in such a heterogeneous group might not be the most appropriate approach. Future studies should focus on tracing factors that determine individual differences between patients (eg, data-driven [cluster] analyses) and, hence, patterns of recovery at the subgroup level (eg, van Mierlo et al 49 ). Subsequently, the choice of treatment could be based on this knowledge (several examples exist in the literature on drug treatment 50 ). Such studies are needed in rehabilitation research too because data-driven analyses allow the generation of new hypotheses. This is necessary because the current approach has not resulted in evidence—or evidence only to a limited extent—on beneficial effects of neglect treatment in the subacute phase post–stroke onset.
Alternatively, a theory-driven approach could be used to diminish heterogeneity of the syndrome when the focus of the study is aimed at specific subtypes of neglect, such as region-specific neglect,34,51 or distinctions between perceptual awareness versus neglect in action planning and execution.26,52 In addition, patients who are likely to benefit from PA could be differentiated based on brain properties. Lesion data or data regarding brain networks could be used in both a theory-driven approach, because different neglect subtypes likely have a different neuroanatomical bases, as well as in a data-driven approach, based on patterns of recovery in patients with different lesion locations.12,53-55 For example, lesions in the cerebellum 54 or (wide) lesions in the occipital lobe 12 seem to limit the effect of PA. Notwithstanding the theoretical importance of such distinctions, analyzing smaller subgroups was currently not feasible statistically. Future trials should include measures that allow differentiation between such subtypes and/or lesion sites to reveal which patients benefit from the studied treatment.
Finally, because neglect is a multifaceted disorder, the best treatment might involve combinations of different therapeutic techniques.56,57 A review study regarding this topic concluded that combined treatments led to larger beneficial effects compared with individual treatments (the phase of treatment was not specified). 47 However, more basic knowledge on the best timing of neglect treatment and individual recovery patterns is needed first to aid the development of evidence-based tailored treatment.
Strengths and Limitations
A large number of neglect patients were included, and almost no patient dropped out during treatment or was lost to follow-up. This can be considered a strength because the treatment should eventually be integrated within the current rehabilitation program. This was the first study in which patients with right-sided neglect after left hemisphere lesions were included. The strength of the study (ie, all neglect patients in the subacute phase were included) is, however, at the same time a limitation because the heterogeneity of the group could have prevented us from finding (subtle) effects of PA. Patients were tested only for neglect; thus, visual field defects were not detected. Positive effects of PA on neglect in patients with comorbid hemianopia, however, have been reported. 13 In addition, because patients were randomized, we did not expect comorbid visual field defects to affect our results.
An important drawback of a study that is performed as part of an existing rehabilitation program is the lack of control regarding other treatments. In the current rehabilitation center, neglect treatment consisted of 1 hour of visual scanning training per week, in combination with efforts made by the complete team during every day, throughout the admission (eg, physical and occupational therapists as well as nursing staff trying to enhance attention for the neglected side). The intensity of the usual care might, therefore, differ between individual patients, depending on the severity of neglect and treatment sessions (physical, occupational, etc) per day. At the group level, however, estimations are that the groups received largely comparable amounts of neglect training and feedback on a daily basis.
A final limitation is the difference between SA and PA groups at baseline for patients with right-sided lesions. Patients in the SA group obtained higher CBS scores (indicating more severe neglect) compared with patients in the PA group. SA patients had, therefore, more potential for rehabilitation, which could, possibly, have affected our results. To minimize this effect, we have corrected for the baseline score in our models.
Conclusions
No time-dependent beneficial effects were found in a large sample of neglect patients after PA compared with SA in the subacute phase poststroke. Possibly, PA is no effective treatment for neglect in the subacute phase. It could, however, also relate to the heterogeneity of the neglect syndrome, enhanced by neurobiological recovery or standard treatment effects. To conclude, we found no evidence that PA should replace the current treatment for neglect in the subacute phase poststroke.
Footnotes
Acknowledgements
We would like to thank all patients who participated in this study and the nurses, occupational therapists, and physical therapists who observed the patients throughout the study.
Authors’ Note
Trial registration Number: NTR3278.
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: Funded by the Revalidatiefonds (R2012134) and Netherlands Organization for Scientific Research (NWO; 451-10-013). The Revalidatiefonds approved the design of the study. NWO and the Revalidatiefonds have no other role regarding the data or manuscript.
*
In the PA group, 12 patients obtained an aftereffect of less than 3 cm in >50% of sessions (despite the 50 additional pointing movements). In the SA group, 1 patient pointed more than 3 cm next to the target in >50% of sessions.
**
Degrees (°) depict visual degrees.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.