
Abstract
Background. Off-the-shelf activity-promoting video games (AVGs) are proposed as a tool for promoting regular physical activity among individuals poststroke. Objective. To characterize the energy expenditure (EE), exercise intensity, and energy metabolism of individuals poststroke, while playing AVGs in different positions, from different consoles, and to compare the performance with comfortable walking and with able-bodied individuals. Methods. Eleven poststroke and 8 able-bodied participants played in standing Wii-Boxing Xbox-Boxing, Wii-Run and Penguin, and also Wii-Boxing in sitting. EE (expressed as metabolic equivalents [METs]); exercise intensity (expressed as %predicted maximal heart rate [HR]), rate of perceived exertion (RPE), and respiratory exchange ratio (RER) were used to characterize the games. Results. Participants’ poststroke EE ranged from 1.81 ± 0.74 to 3.46 ± 1.3 METs and was lower compared with able-bodied participants for Xbox-Boxing (P = .001), Wii-Boxing in standing (P = .01), Run (P < .001), and Penguin (P = .001). Participants’ poststroke exercise intensity ranged from 49.8 ± 9.3 to 64.7 ± 9.3 %predicted maximal HR and was lower compared with able-bodied participants for Xbox-Boxing (P = .007) and Run (P = .005). For participants poststroke, EE of walking at a comfortable did not differ from boxing games in standing or Run. For able-bodied participants only, the EE for Xbox-Boxing was higher than Wii-Boxing (6.5 ± 2.6 vs 4.4 ± 1.1, P = .02). EE was higher in standing versus sitting for poststroke (P = .04) and able-bodied (P = .03) participants. There were no significant group differences for RPEs. RER of playing in sitting approached anaerobic metabolism. Conclusions. Playing upper extremity (ie, Boxing) or mobility (ie, Run) AVGs in standing resulted in moderate EE and intensity for participants poststroke. EE was lower for poststroke than for able-bodied participants.
Introduction
Community-dwelling individuals poststroke are prone to a sedentary lifestyle,1-3 with poor maintenance of long-term physical activity (PA).2,4 The American Heart Association and the American College of Sports Medicine recommend low to moderate intensity PA to promote health and vigorous PA for cardiovascular fitness.5-7 Given that the levels of PA among individuals poststroke in the chronic phase rarely meet these criteria, activity-promoting video game (AVG) technologies may provide a worthwhile alternative for promoting PA. These technologies offer the potential of enhancing adherence, 8 while being low cost, easy to operate, and widely available. 9
Off-the-shelf AVG consoles, such as Microsoft-Xbox with the Kinect sensor and the Nintendo-Wii with their accompanying games, including Kinect-Sports, Wii Fit, and Wii Sports, enable individuals to simulate sports and experience a variety of physical activities. Although the games were originally designed for recreation, they have also been explored for their potential health benefits, both in healthy and neurological populations.10-18 Playing AVGs has been shown to enhance body movement and energy expenditure (EE) in healthy individuals.13,19-22 The intensity of exercise while playing Wii games has been shown to range from light to moderate levels.12,19,20,23 These findings of activity promotion in healthy people may also have relevance to individuals poststroke.
A few studies have described the use of AVGs for the rehabilitation of individuals poststroke.17,24-27 These studies focused on the feasibility of using the games and primarily employed upper extremity (UE) games. Although the findings are limited by the small sample sizes, they indicate that AVGs are feasible for use by individuals poststroke with moderate motor impairment in the subacute and chronic phases.
The energy characteristics of the games when played by individuals poststroke have been reported in only one study. 28 Hurkmans et al 28 found that the EE of individuals poststroke while playing Wii-Sports Boxing and Tennis was consistent with exercise at a moderate intensity. The study, however, was limited to these 2 UE games played on one gaming console (Wii). Understanding the energy characteristics of a variety of games that have different task demands and use different consoles is a required first step in the implementation of AVGs for health promotion in individuals poststroke.
Thus, the aim of the present study was to characterize the EE, exercise intensity, and energy metabolism of exercise in individuals poststroke while playing AVGs and to compare their performance with that of able-bodied individuals and in reference to their comfortable walking (Walking-c). Specifically, we explored variables that can potentially modify EE during game play by evaluating games of different categories (UE, mobility, and balance), playing on different consoles (Xbox+ Kinect, and Wii), and in different positions (standing and sitting). We hypothesized that the participants poststroke would exercise at a moderate intensity when playing the games, and at a lower intensity than the able-bodied participants. We also hypothesized that the EE of the same game would not vary between the consoles and would be higher when playing in a standing versus a sitting position.
Methods
Participants
Eleven poststroke and 8 able-bodied individuals participated in this study. Participants poststroke were recruited from community stroke support groups and by word of mouth and able-bodied participants were recruited from our institution by word of mouth and study flyer advertisement. An a priori power calculation to detect difference of 2 metabolic equivalents (METs) between the groups indicated that at least 8 individuals should be included in each group. Determinants for the calculation were standard deviation = 1 for both groups,20,28 α = .01 one-tail, and power = .85.
The inclusion criteria for the individuals poststroke were as follows: age range from 25 to 75 years, onset of stroke greater than 6 months prior to study recruitment, and ability to walk 50 feet without the assistance of another person, using either a walking device or a brace. The exclusion criteria for both the poststroke and the able-bodied individuals were as follows: any medical condition other than the stroke that affected their walking; a history of severe heart disease, myocardial infarction, valve replacement, coronary artery bypass surgery, severe lung disease, or uncontrolled diabetes. All participants poststroke were cleared to participate in the study by their primary physician. The study protocol was approved by the institutional review board, and participants signed a written informed consent.
Characterization of Participants
Prior to game familiarization, participants’ height and weight were measured using a wall-mounted body meter (Seca 206, Hamburg, Germany) and a digital scale (Contek wcs8). In addition, characteristics of Walking-c, including speed, distance, EE and metabolic cost, were measured over 6 minutes of walking. 29 Participants sat for 10 minutes and were then instructed to “walk at your usual comfortable speed” 30 back and forth over a 25-m walkway for 6 minutes. For participants poststroke, level of motor impairment was evaluated using the motor section for the upper and lower extremities of the Fugl-Meyer assessment. 31
Console and Game Selection
Figure 1 shows the games played using the 2 gaming consoles and the positions during the games. We selected the Xbox with the Kinect sensor and the Wii consoles since both are commercially available and widely used. 9 The Xbox Boxing, Wii-Sports Boxing, and Wii Fit Run and Penguin games were selected on the basis of their task requirements 32 and predicted energy demands. 20 The boxing game requires bilateral UE movements, the Run game requires stepping and balance, and the Penguin game requires dynamic standing balance. The boxing game was played in standing, using both the Xbox console + Kinect sensor (KBox) and the Wii console (WBox), and in sitting using the Wii console (WBox Sit).
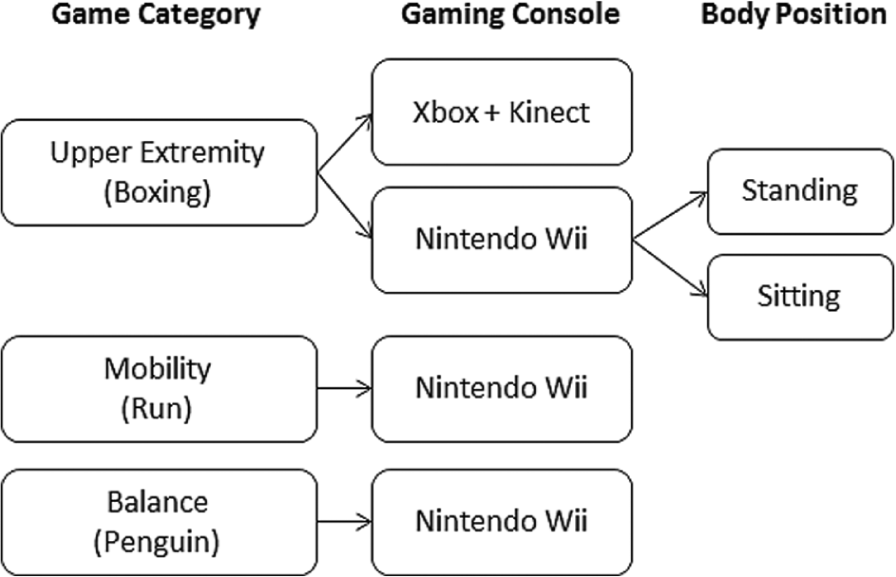
Block diagram showing the games played using the 2 gaming consoles and the 2 positions during the games.
Playing the Games
The study consisted of 1 session for game familiarization and 3 sessions for game testing, which were separated by at least 2 days. Participants were instructed to avoid eating or drinking for 2 hours and caffeine consumption for 12 hours prior to each session. During the familiarization session, the participants played each game for 10 to 15 minutes. By the end of the session, all the participants reported feeling comfortable with playing the games. At the beginning of each testing session, participants sat still with their eyes closed in a quiet, dimly lit room for 10 minutes. Activities were then performed for 8 to 10 minutes each, with 8 to 10 minutes of rest in between. Games were repeatedly loaded so as to achieve 8 to 10 minutes of continuous activity. During the testing sessions, the participants also performed three standard daily motor activities. Data for these activities are not reported here. The number and order of the games within each session were fixed and designed to ensure that the activity with the expected lowest energy demand was played first and the activity with the expected highest energy demand was played last. The order of the sessions was counterbalanced.
Measurements of Outcome Variables
Metabolic measures, including oxygen consumption and the respiratory exchange ratio (RER) of Walking-c, rest, and gaming, were collected using the breath-by-breath measurement technique with a portable telemetric gas analysis system (COSMED K4b 2 , COSMED, Rome, Italy). 33 The system was calibrated before each session according to the manufacturer’s instructions. Heart rate (HR) was continuously measured using a Polar HR monitor (Polar Electro, Kempele, Finland). Rate of perceived exertion (RPE) was recorded at the middle and at the end of each gaming period, using Borg’s RPE scale of 6 to 20.34-35 Participants’ feeling of enjoyment while playing the games was evaluated by the question “Did you enjoy the game?” (adapted from the Short Feedback Questionnaire) 36 and rated on a scale of 1 (not at all) to 5 (a lot).
Data Analysis
Games were characterized by MET (representing EE and exercise intensity), percentage of predicted maximal HR (HR%pred.max, representing exercise intensity), RER (representing energy metabolism), and level of enjoyment.
Values of the outcome variables were extracted for data analyses from the last 4 minutes of the Walking-c and the last 5 minutes of each gaming period after visual inspection for
Metabolic equivalent values were calculated by dividing the mean
HR%pred.max was used to describe exercise intensity, as it is a relative measure that accounts for individual factors, such as age. 5 Predicted maximal HR was calculated by the Tanaka formula (HRmax(pred.) = 208 – (0.7 × age)). 40 For participants who took beta-blockers, it was calculated by the formula (HRmax(pred.)(adjusted) = 164 − (0.7 × age)), which accounts for the effect of beta-blockers. 41
Energy metabolism was evaluated using the RER, which is an indicator of the energy system (ie, aerobic or anaerobic) employed during the activity.
The MET of rest while sitting and the gross metabolic cost of walking were calculated and used for the characterization of participants. Two minutes from the first rest period of each session were selected to represent steady state resting
Statistical Analysis
Statistical analyses were performed using nonparametric tests to account for the small sample size.
To test the hypotheses that EE and exercise intensity of AVGs would be lower for participants poststroke, Mann–Whitney U between-group tests were performed for each outcome variable and game separately. Within-group differences in EE and exercise intensity between games and Walking-c were determined using the Wilcoxon signed-rank test. All analyses were performed assuming a one-tail test, and α = .01, which was adjusted for multiple comparisons.
Interaction effects between game and group for the analyses of console and position were assessed using 2 separate repeated-measure analyses of variance, with game as the within-variable and group as the between-variable (α = .05). To determine if position and console affected EE, comparisons of the MET values for KBox versus WBox and WBox versus WBox Sit were performed for each group separately, using Wilcoxon signed-rank tests with 2 tails and 1 tail, respectively (α = .05).
Between-group analysis of the RER values yielded no differences, and thus the effect of game category on RER was tested on the combined data of both groups by using a t test (n = 19, α = .01, multiple comparisons correction). Statistical analyses were performed with SPSS, version 18 (IBM SPSS Inc, Chicago, IL).
Results
Participants
Characteristics of the participants are presented in Table 1. Groups were similar in mean age and body mass index. Walking-c speed, distance, and metabolic cost were significantly different between groups (z = −3.3, P < .01; z = −2.6, P = .01; and z = −2.3, P = 0.02, respectively).
Characteristics of the Participants.
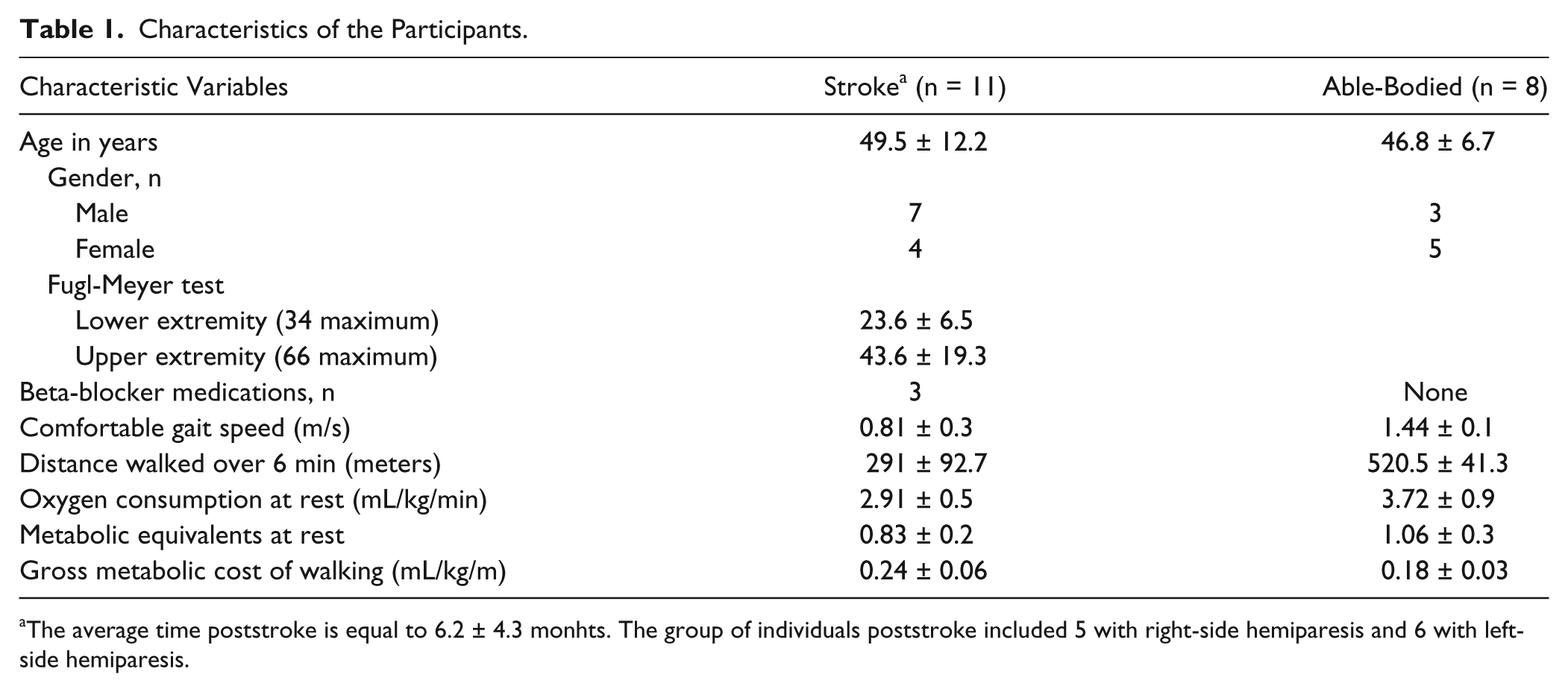
The average time poststroke is equal to 6.2 ± 4.3 monhts. The group of individuals poststroke included 5 with right-side hemiparesis and 6 with left-side hemiparesis.
Playing the Games
All the participants completed all the testing sessions successfully and were engaged in competent game play. During the boxing game, one participant poststroke was not able to hold the controller with the affected hand and instead had it attached to his hand with a strap. During the Run game, the participants poststroke stepped in place, whereas the able-bodied participants either ran or stepped in place.
Poststroke participants’ scores for enjoyment ranged from “enjoyed” to “enjoyed a lot,” with the Run game having the lowest score (4.0 ± 0.3) and KBox having the highest score (4.9 ± 0.1). Able-bodied participants’ scores ranged from “enjoyed” for all boxing games (4.2 ± 1.2 for Kbox and Wbox and 4.2 ± 1.0 for WBox Sit) to “somewhat enjoyed” for Run (3.0 ± 1.0).
Energy Expenditure and Exercise Intensity
The METs and HR%pred.max for each game and Walking-c are summarized in Figures 2 and 3. The METs and HR%pred.max of the participants poststroke were significantly lower than those of the able-bodied participants during KBox (METs: z = −3, P = .001 and HR%pred.max: z = −2.5, P = .007) and Run (METs: z = −3.5, P < .001 and HR%pred.max: z = −2.7, P = .005). MET values were also significantly lower for WBox (z = −2.2, P = .01) and Penguin (z = −2.6, P = .001), but not the HR%pred.max values. No significant differences in RPE were found between the groups. However, patterns of a higher rating by the able-bodied participants during the UE games and a higher rating by the participants poststroke during the balance and mobility games were observed (see Figure 4).
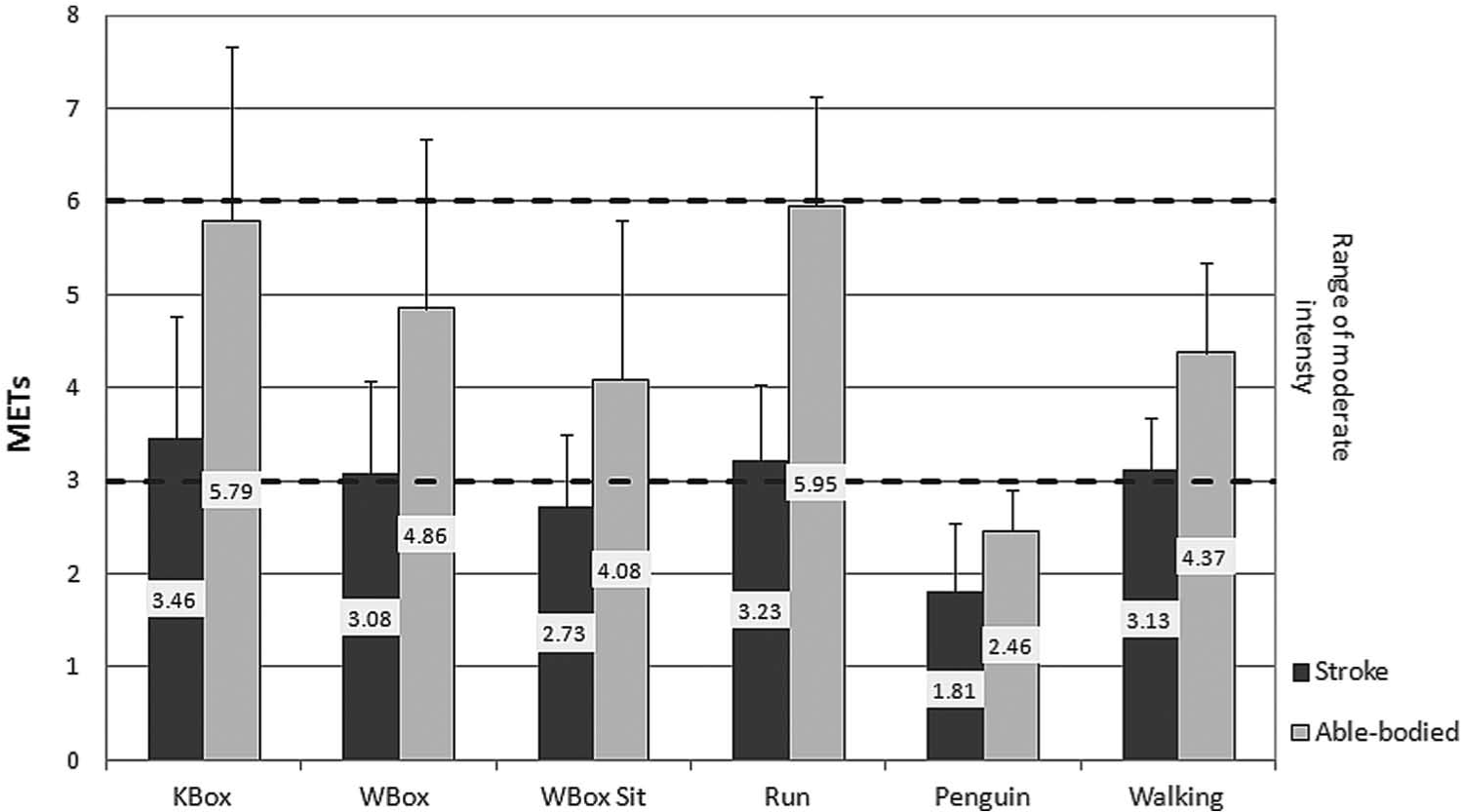
Metabolic equivalents (METs) for Xbox Kinect Boxing (KBox), Wii Boxing (WBox), Wii Boxing in sitting (WBox Sit), Run, Penguin, and walking at a comfortable speed (Walking). Data are presented as mean ± standard deviation. Horizontal lines indicate the range of moderate intensity, as described by the American College of Sports Medicine.
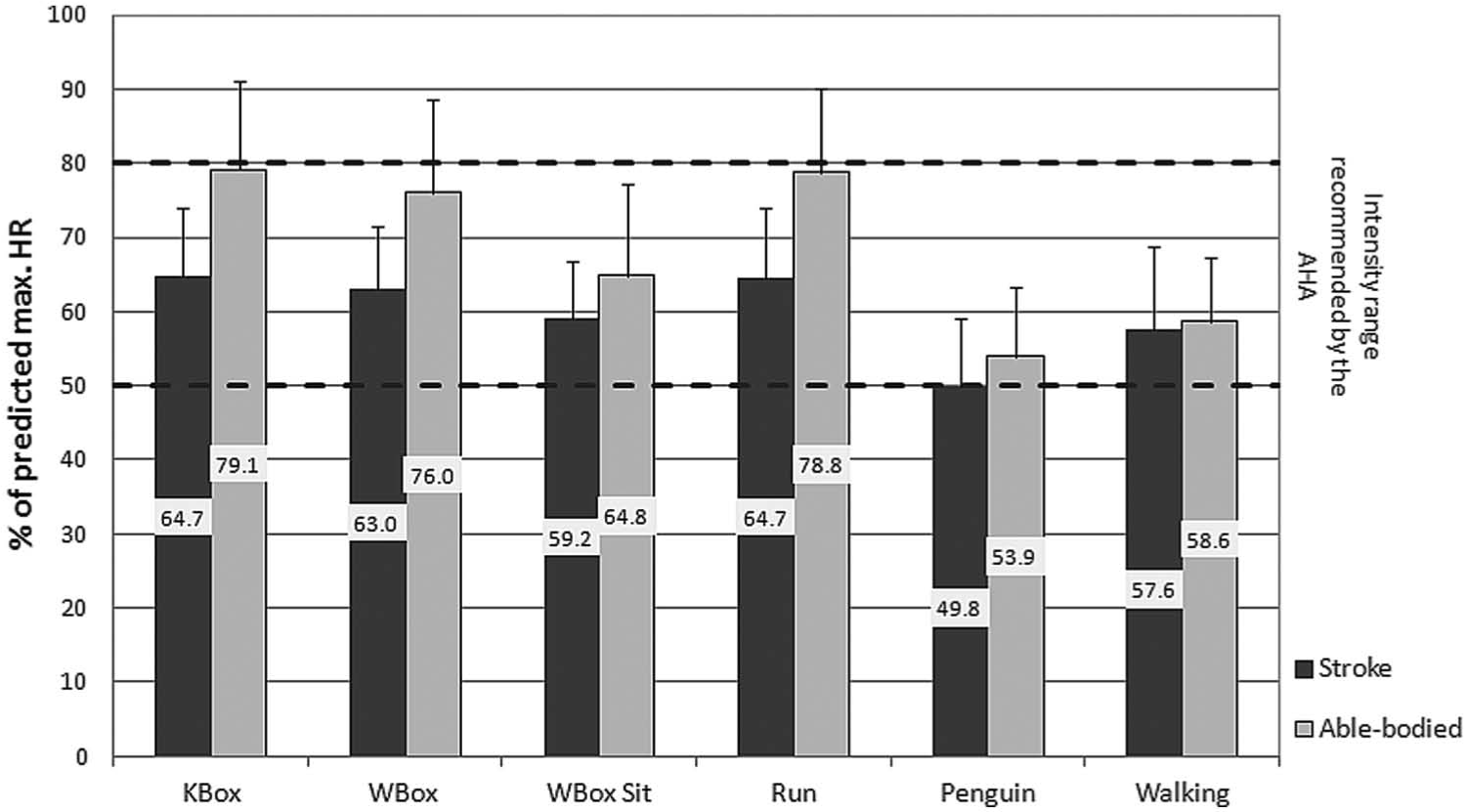
Percentage of predicted maximal heart rate (HR) during Xbox Kinect Boxing (KBox), Wii Boxing (WBox), Wii Boxing in sitting (WBox Sit), Run, Penguin, and walking at a comfortable speed (Walking). Data are presented as mean ± standard deviation. Horizontal lines indicate the recommended intensity range of physical activity for individuals poststroke, as described by the American Heart Association.
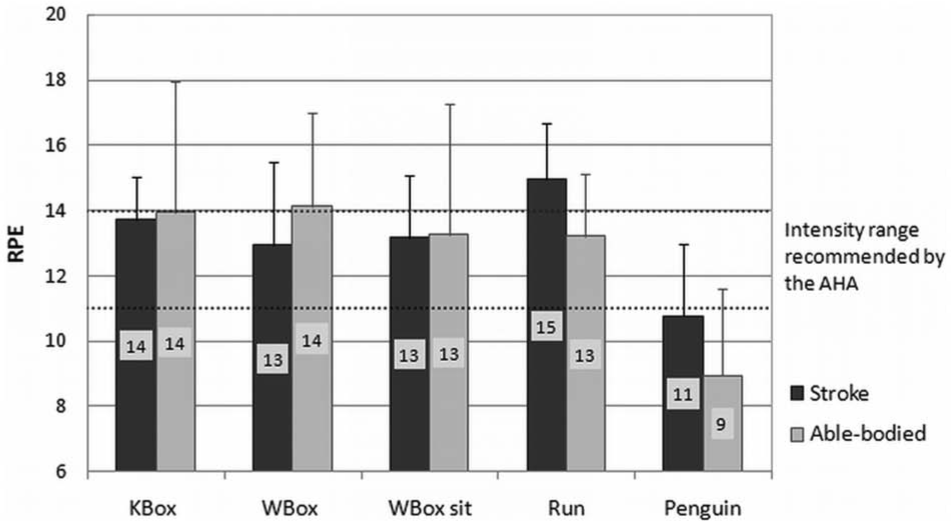
Rate of perceived exertion (RPE) during Xbox Kinect Boxing (KBox), Wii Boxing (WBox), Wii Boxing in sitting (WBox Sit), Run, and Penguin. Data are presented as mean ± standard deviation. Horizontal lines indicate the recommended intensity range of physical activity for individuals poststroke, as described by the American Heart Association (AHA).
For participants poststroke, the only significant differences found in the MET values between the Walking-c and gaming activities were higher METs for Walking-c than for Penguin (METs: z = −2.9, P = .003) and for WBox Sit (z = −2.8, P = .006). The only significant difference found in HR%pred.max values between Walking-c and gaming activities was higher HR%pred.max for Walking-c than for Penguin (z = −2.9, P = .002). For able-bodied participants, EE and HR%pred.max for Walking-c were significantly lower than for Run (z = −2.4, P = .01), and MET for Walking-c was significantly higher than for Penguin (z = −2.4, P = .01).
Energy Metabolism
The RER values for all participants were highest for WBox Sit, followed by KBox, WBox, Run, and Penguin (0.97 ± 0.03 and 1.02 ± 0.03; 0.94 ± 0.02 and 0.99 ± 0.04; 0.93 ± 0.03 and 0.96 ± 0.03; 0.91 ± 0.02 and 0.93 ± 0.02; 0.8 ± 0.03 and 0.84 ± 0.02, respectively). WBox Sit had significantly higher RER values than WBox (1.00 ± 0.02 vs 0.94 ± 0.02, t = −3.2, P = .005) and Run (1.00 ± 0.02 vs 0.92 ± 0.02, t = 3.1, P = .007).
Comparison Between Gaming Consoles and Body Positions
The interaction between group and game was not significant, and there was a significant main effect for both group and console. METs for KBox were significantly higher than for WBox for the able-bodied participants (z = −2.4, P = .02), but not for the participants poststroke (see Figure 5A). The MET values for WBox in standing were significantly higher relative to sitting for both the poststroke (z = −1.7, P = .04) and the able-bodied (z = −1.9, P = .03) participants (see Figure 5B).
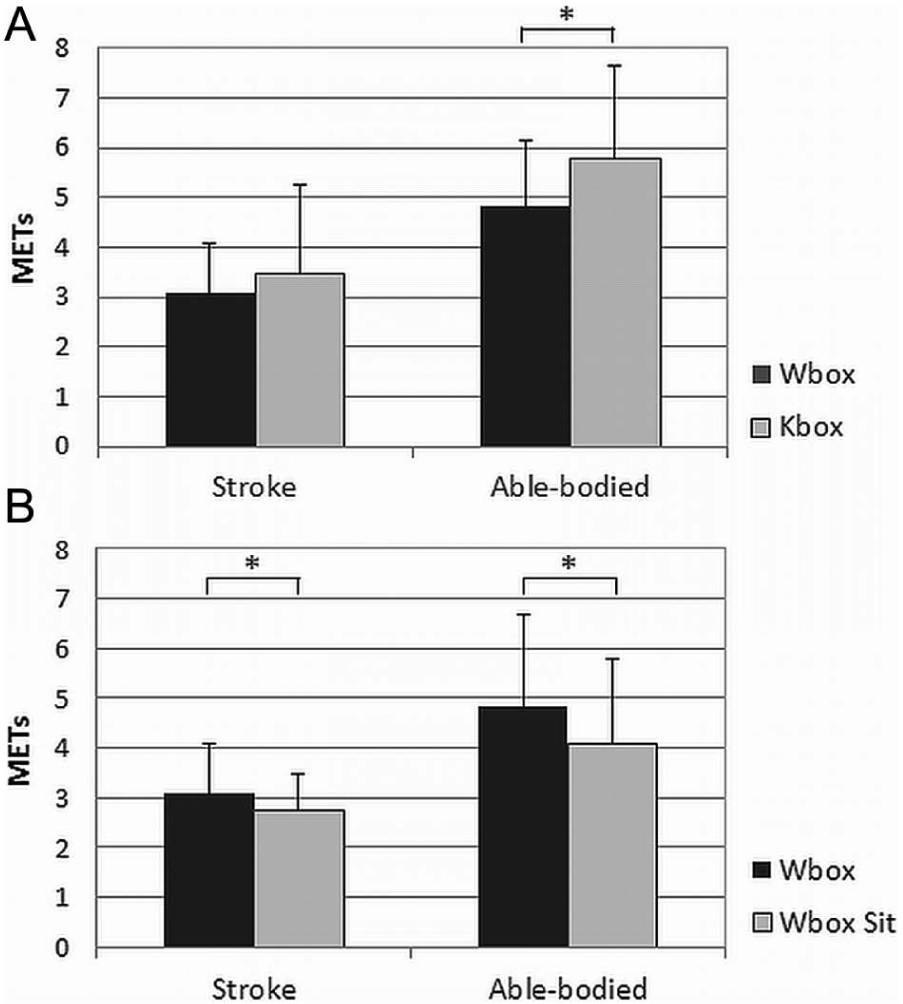
Comparison of metabolic equivalents (METs) of (A) Wii Boxing (Wbox) versus Xbox Kinect Boxing (Kbox) in standing and (B) Wii Boxing (Wbox) versus Wii Boxing in sitting (B). Data are presented as mean ± standard deviation.
Discussion
To the best of our knowledge, this is the first study to compare the EE and exercise intensity of poststroke and able-bodied individuals, as well as to measure their performance while playing on 2 different consoles and in 2 different positions. We found that the individuals poststroke who had a moderately severe motor impairment 43 and were unlimited community ambulators 44 played UE and mobility AVGs at the lower end of moderate EE and intensity, regardless of the console they used, and that this intensity was significantly lower than that of the able-bodied individuals. Furthermore, playing in sitting demonstrated lower EE as compared with standing.
Energy Expenditure and Exercise Intensity of the Participants Poststroke
Recommendations on the level of PA required for the accrual of health benefits suggest that healthy deconditioned or poststroke individuals should be engaged in activity at a moderate MET level (3.0-5.9) or a percentage of maximal HR greater than 50%.5,6 We found that playing AVGs met the recommendation but only at the range’s lower end. Similar EE findings were recently reported for WBox. 28 The Penguin game, as expected, 20 demonstrated a light EE. In addition to increasing EE, our participants reported that they enjoyed the game playing. All boxing activities approached anaerobic metabolism, whereas Run and Penguin demonstrated aerobic metabolism. These findings are in accordance with reports on the potential of off-the-shelf AVGs to promote health and an active lifestyle for sedentary or deconditioned individuals.10,19,22,45
As hypothesized, the participants poststroke played the games at a lower EE and intensity than the able-bodied participants. This finding is in line with a recent report on older adults playing AVGs at a lower EE than healthy young adults. 38 It is also noteworthy that the difference in EE across activities was smaller for the participants poststroke than for the able-bodied participants (1.65 METs vs 3.43 METs). Similarly, the HR response to activities was confined to a narrower range for the poststroke participants (49.8 ± 9.3 to 64.7 ± 9.3 HR%pred.max) than for the able-bodied participants (79 ± 12 to 53.9 ± 9.3 HR%pred.max).
Both their lower EE and the narrower range of EE and intensity across games with different task requirements may be explained in part by neuromuscular impairments, such as decreased muscle endurance, muscle weakness, and impaired balance, which may compromise motor performance during the game, interfere with vigorous play, and obstruct higher EE. The participants poststroke in our study had a total Fugl-Meyer assessment score of 67, and although they were fully engaged in the game play, their motor performance during gaming was different from that of the able-bodied controls (eg, walking vs running and boxing with mainly 1 hand vs 2 hands). In addition, their metabolic cost of walking was higher than able-bodied participants and within the reported range for individuals poststroke,29,46,47 indicating inefficient and uncoordinated body movements.
It has previously been shown that stroke-related impairments limit the ability of individuals poststroke to achieve their maximal aerobic effort. 48 Studies investigating comfortable and fast walking of individuals poststroke support the assumption that their ability to challenge the aerobic system is limited by neuromuscular impairments that prevent them from modifying their motor performance and increasing their EE. For example, Jonkers et al 49 found that the ability to increase walking speed was impaired for individuals with greater mobility limitations. They associated this finding with muscle weakness, which prevented participants from changing their walking pattern and generating higher speeds.
We found that boxing games, specifically when played in sitting, had RER values that approached anaerobic metabolism and were higher relative to mobility activities. For healthy individuals, UE exercises were demonstrated to be more metabolically taxing than lower extremity exercises when performed at similar intensities and were associated with higher lactate concentration. 50 The authors suggested that UE exercises used smaller muscle groups and a relatively lower number of glycolytic motor units for generating the movements. Their explanations may provide support for our RER findings, since playing boxing in a sitting position almost exclusively involves the UE musculature, whereas playing boxing in a standing position involves some activity of the larger lower extremity muscle groups, and playing Run and Penguin requires mainly larger muscle groups.
Subjective perceptions of exertion were similar for poststroke and able-bodied participants, even though the actual EE was lower for participants poststroke. It is possible that participants post-troke reported disproportionally high RPE because of lower exercise capacity, resulting in the participants working at a greater percentage of their maximal exercise capacity. In addition, the higher ratings might represent an overestimation of exercise effort. Previous report showed an overestimation of exercise effort by individuals poststroke, based on RPE. 51 The researchers related this overestimation to stroke-related impairments as well as to physiological, pharmacological, and psychological factors.
The cognitive load of game play might also influence the reports of perceived exertion. Playing the games involves different cognitive processes, such as comprehension of the task, attention, and the processing of multisensory inputs. Therefore, individuals poststroke might experience the output of higher cognitive effort relative to able-bodied individuals and may be reporting both on physical and cognitive effort. In the absence of specific cognitive assessment, this suggestion should be considered speculative and merits further investigation.
Comparison Between Consoles and Body Positions
Higher EE was demonstrated by the able-bodied participants while playing KBox as compared with WBox, whereas no difference in EE between the consoles was found for the participants poststroke. Similarly, no differences in EE between the consoles were reported for older adults in other study. 38 The difference in EE for the able-bodied participants may be explained by the motion capture and translation features of the consoles. In the Wii, where the virtual figure on the screen is manipulated by acceleration of the handheld remote, the users might learn to achieve the game goal with limited body movements. In contrast, with the Xbox Kinect, where the movements of the virtual figure in the game are sensitive to the actual movement of body parts, the users may try to increase their body movements in order to achieve the game goal, which in turn will require more energy. The lack of difference in energy demands between consoles for the participants poststroke is in accordance with the overall findings of their narrower range of EE.
Game play in standing showed higher EE for both groups. This finding was expected, given that playing in a standing position involves the activity of larger muscle groups. However, it is in contrast with Taylor et al, 38 who reported no difference in EE between game play in standing and sitting for the WBox game among older adults. These contradictory findings might be explained by an overall lower EE in the older adults study. In addition participants in our study had more time for practicing the games in a familiarization session, which might have afforded them the skill to differentiate between positions.
Clinical Implications
The findings reported here have some clinical implications for the application of AVGs to promoting PA among individuals poststroke. They suggest that both upper and lower extremity games can promote PA at the lower end of moderate intensity. Furthermore, the combination of games from different categories and played in different positions might enable continuous activity, while avoiding the metabolic endpoint of anaerobic metabolism. Attention should be paid to the finding that playing in a sitting position resulted in lower EE and intensity as compared with standing. A comparison between consoles suggests that console selection, and not only game selection, can influence activity outcome, though not in the case of individuals poststroke.
Interestingly, playing UE and mobility games demonstrated similar EE and intensity levels as those found when walking at a comfortable speed. Although overground walking is one of the most common modes of PA, it has some implementation barriers, such as weather conditions and space limitations. The integration of AVGs may help to overcome some of these barriers.
While this study focused on the intensity of playing AVGs, the recommendations for PA also include duration and frequency.5,6 Our study only measured continuous game playing of 8 to 10 minutes. This duration meets the short duration requirement recommended for deconditioned individuals,5,6 but not the 30-minute duration of continuous exercise. In the context of this study, frequency was not specifically assessed.
When using games for PA, it is important to consider that the intensity of playing off-the-shelf AVGs is self-imposed and that AVG environments do not allow for the same level of control of the workload as other traditional modes of training, such as walking on a treadmill (eg, by ramp and speed). Traditional aerobic training modes that prescribe a specific level of intensity may promote PA at more vigorous intensities, which can facilitate aerobic fitness. The use of clinical measures, such as HR, allows us to compare the intensity of playing the games with the intensity of standard aerobic training. The exercise intensity for gaming, as measured in this study, is similar to the initial intensities reported in studies of aerobic training with treadmill walking or cycling. However, in these studies, the intensity was progressively increased.52,53 More recently, higher training intensities of 80% to 85% of maximal HR have been reported.54,55 However, when the long-term goal is to promote engagement in PA and to achieve health goals, the use of activity that is based on self-imposed intensity might be beneficial, since it is related to decreased perceived exertion and improved enjoyment.
Our study has several limitations. First, the external validity of the study is limited to a sample of relatively young individuals poststroke who were independent community ambulators. It is possible that participants who are older or more impaired would play the games at lower intensities. Second, to estimate intensity levels based on HR, we used a predicted maximal HR, whereas the validity of predicting HR based on age for individuals poststroke was not established. Finally, the MET calculation was based on the generic resting
Conclusions
Playing AVGs might be a useful tool for increasing the PA of individuals poststroke at a level that can promote health and is similar to walking. The EE and PA intensity did not vary by console and were higher when playing in standing than in sitting.
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article:
This work was supported by an award from the American Heart Association (award ID 11POST7760001).