
Abstract
Background. Constraint-induced movement therapy (CIMT) has gained emerging evidence and popularity in children with unilateral cerebral palsy (CP). However, many issues remain unanswered regarding the best approach. Objective. This study investigated the additional effects of an intensive therapy program to promote hand function combined with home-based modified CIMT (m-CIMT). Methods. Fifty-one children (mean age 8 years 9 months) were randomized to m-CIMT alone or m-CIMT with intensive therapy (IT). All children had to wear a constraint on the unaffected hand for 1 hour, 5 days/week for 10 weeks. Children in the m-CIMT + IT group also received 3 sessions of 45 minutes weekly of intensive therapy for distal muscle strengthening and hand function, using unimanual and bimanual activities. The Assisting Hand Assessment (AHA) was the primary outcome measure. Secondary outcome measures were muscle tone, strength, Melbourne Assessment, Jebsen–Taylor test, and ABILHAND-Kids questionnaire. Assessments were administered at baseline, after intervention, and at 10-week follow-up. Results. Significant between-group differences in AHA were in favor of the m-CIMT + IT group (P = .04). Both groups demonstrated comparable improvements in muscle tone (P = .002), strength (P < .0001), grip strength (P = .02), and unimanual capacity (Melbourne Assessment and Jebsen–Taylor, P < .0001). Younger children and children with poorer hand function benefited from both interventions, whereas older children and children with better hand function only benefited from the combined approach. Conclusions. The combination of m-CIMT with an intensive therapy program on distal hand function and strength enhances the effects of m-CIMT alone for improving bimanual performance.
Keywords
Introduction
Over the past 10 years, research into upper limb interventions for children with unilateral cerebral palsy (CP) has grown exponentially. 1 A treatment modality gaining popularity among clinicians and researchers is constraint-induced movement therapy (CIMT). 2 CIMT combines a constraint of the unaffected hand with intensive training of the affected side for more than 3 hours per day for at least 2 consecutive weeks (massed practice). There is mounting evidence of treatment efficacy across a wide array of delivery methods, including various constraint types, treatment models, intensities, and durations. 3 Notwithstanding the increasing awareness of the value of CIMT in upper limb rehabilitation, many questions remain unanswered.
A first important question is the optimal intensity and duration of CIMT. Indeed, treatment efficacy has also been demonstrated for a modified form of CIMT (m-CIMT), using less restrictive constraints during less than 3 hours per day over a longer period (distributed practice).4-6 Second, it remains unclear which children benefit most from CIMT and its modified version. In previous studies, predictive factors have rarely been investigated. A study by Eliasson et al 4 identified age and severity as significant predictors of favorable bimanual performance, whereas 2 other studies concluded that the efficacy of intensive training approaches was not age-dependent.7,8 The limited number of studies of prognostic factors and their conflicting results highlight the need to further investigate the response to m-CIMT in children of different ages and impairment levels.
Another question is whether combining m-CIMT with an adjunct intervention augments the treatment effect versus m-CIMT alone. Recently, new models have been developed that incorporate a bimanual component to m-CIMT training, based on the recognition of the limitations of unimanual training.9,10 However, the effects of combining bimanual training with m-CIMT compared to m-CIMT alone, but with otherwise identical conditions, need further exploration.
A prospective cohort study based on cross-sectional data in 81 children with unilateral CP suggested that both unimanual and bimanual activities were largely determined by distal muscle strength. 11 Only one small trial has investigated the effects of upper limb strength training in 9 children with unilateral CP; this study found an increase in wrist extensors strength but no improved hand function. 12 It might be hypothesized that the effects of strength training can be facilitated by combining it with functional training such as m-CIMT. In this study, we aimed to investigate the effects of home-based m-CIMT with an integrated therapy program on distal muscle strength and hand function, adopting a unimanual and bimanual approach. We hypothesize that such an integrated approach may facilitate the carryover effect of improved distal muscle strength and hand function to better bimanual performance. In addition, we aimed to identify demographic and clinical characteristics of children who benefited most from m-CIMT with intensive therapy versus m-CIMT alone.
Methods
Participants
Children with unilateral CP were eligible to participate if they (a) were aged between 4 years 6 months and 12 years, (b) had minimal ability to grasp with the affected hand, and (c) showed sufficient cooperation to perform the assessments and participate in the intervention. Children were excluded if they had previously undergone upper limb surgery or if they had received botulinum toxin injections in the upper limb within 6 months prior to study entry. Children were recruited via the CP-care program of the University Hospital Leuven and were enrolled prospectively between August 2009 and April 2010. The protocol was approved by the Ethical Committee of the University Hospital Leuven, and informed consent was obtained from the parents.
Design
The study was designed as a randomized, controlled, and evaluator-blinded trial. To obtain comparable groups, children were first stratified according to the Manual Ability Classification System (MACS), 13 levels I, II, and III. Additionally, children were stratified according to their age group. Children aged between 4 years 6 months and 8 years were assigned to group A, and those between 8 years and 12 years to group B. Within these 6 strata (IA, IB, IIA, IIB, IIIA, and IIIB), children were randomly assigned to the modified CIMT group (m-CIMT, a) or the modified CIMT plus intensive therapy group (m-CIMT + IT, b). A permuted block design of 4 was used, created by a computer random number generator, for example, aabb-abab-bbaa-baba. In this procedure, a block size of 4 and allocation ratio of 2:2 was specified, and subjects were randomly allocated within each block. Randomization was performed by an independent person who was not involved in the selection procedure and did not have access to clinical information about the children.
Sample size estimates were based on the projected treatment effect of the primary outcome measure, the Assisting Hand Assessment (AHA). 14 The smallest detectable difference (SDD), when the random variation depending on rater error and child behavior variation is taken into account, is 5 units on the 0 to 100 AHA-unit scale. 15 Previous results from longitudinal data over 1 year in 81 children with unilateral CP yielded an AHA standard deviation (SD) of 6 units. 16 Based on an effect size of 5 units, a SD of 6 units, statistical power of 80%, and an α level of .05, a sample size of 24 children in each group was required to be able to detect a difference between groups equal to or larger than the SDD. This number was increased to anticipate for inevitable dropouts.
Intervention
For children in both groups, the m-CIMT intervention included wearing a constraint and structured skills practice provided by the parents and supervised by the main investigators. Children wore a splint on the unaffected hand for 1 hour, 5 times a week, for 10 weeks (total time 50 hours). The splint was a rigid orthosis, individually adjusted and covering fingers, thumb, and wrist. Parents received instructions on how to stimulate their child to use their affected side during the time of wearing the constraint. The focus hereby was mainly on improving the unimanual capacity of the affected hand. They were provided with a list of fine, gross motor, and daily life activities, individually adjusted to the child’s level. Parents were also instructed about motivational and behavioral aspects that could interfere with the training. Halfway through the intervention period, parents were contacted to discuss the feasibility of the program and the child’s progress, and if needed, adjustments to the program were suggested.
Children in the m-CIMT + IT group additionally received an integrated program with a focus on distal muscle strength and hand function, using a unimanual and bimanual approach. The intensity was 3 times a week for 45 minutes (total time 22 hours 30 minutes). Treatment was provided additionally to the routine therapy. All therapists were asked to fill in a questionnaire on the intensity and content of the routine therapy the children received.
The program was performed by the individual physiotherapist or occupational therapist. To determine the content of the program, a manual was developed by the main investigators encompassing exercises for different hand functions (eg, grasp, release, in-hand manipulation, bimanual coordination) and different muscle groups. Individual goals were set up, and a selection of exercises was made based on body function measures and video-based assessments of the Melbourne Assessment of Unilateral Upper Limb Function 17 and the AHA. 14 The goals were discussed with the child’s therapist, and they were instructed on how to perform the exercises and gradually increase the difficulty level. During each session, analytical exercises and functional activities were performed. Analytical exercises for specific muscle groups were executed in 3 series of 10 repetitions, for example, to improve strength and selectivity of wrist extension or supination. Functional activities were performed as repetitive and structured practice of unimanual and bimanual activities. Finally, to enhance transfer to a functional context, the parents and child were asked to choose 2 bimanual activities of daily living. During the last 5 to 10 minutes of each therapy session, these activities were trained based on motor learning principles. The practical implementation of the motor learning principles included task analysis, repetitive whole-task practice, practice specificity, feedback, environmental adaptation, and grading of difficulty level according to the stage of motor learning. 18
All therapy equipment was provided. Halfway through the intervention period, the child and his/her therapist were visited by the main investigator. The degree of difficulty of the exercises and therapy equipment were then adapted to the child’s progress.
To evaluate compliance, parents were asked to fill in an activity log on the frequency and duration of wearing the constraint and the executed activities. The therapists were asked to record frequency and duration of effective therapy time. The expected compliance level was set at 80%, which corresponded to 40 hours of wearing the constraint. For the therapy program, this was equal to 18 hours over 10 weeks.
Assessment
Children were assessed at baseline (T1), after intervention (T2), and after 10 weeks of follow-up (T3). Assessments were administered at the Clinical Motion Analysis Laboratory of the University Hospital Leuven by 1 physiotherapist blinded to group assignment. Video assessments were scored by 2 assessors blinded to group allocation and order of assessment.
The AHA was the primary outcome measure. This measurement assesses in 22 items how effectively the affected hand is spontaneously used in bimanual activities. 14 Raw scores were converted to 0 to 100 logit-based AHA units. 15 The test shows high interrater and intrarater reliability. 19
Secondary outcome measures included body function measures and 3 other activity measures. At the body function level, muscle tone, manual muscle strength, and grip strength were evaluated using a reliable standardized test protocol. 20 Muscle tone was evaluated with the Modified Ashworth Scale (MAS). 21 A total score was calculated (0-36), which included muscle groups of the shoulder (adductors, extensors, internal/external rotators), elbow (flexors/extensors), and wrist and hand (pronators, wrist flexors, finger flexors). To assess muscle strength, manual muscle testing (MMT) was used according to Daniels and Worthingham. 22 A total score was calculated (0-30) comprising the scores for elbow flexors/extensors, forearm pronators/supinators, and wrist flexors/extensors. Grip strength was assessed as the mean of 3 maximum contractions recorded with a Jamar dynamometer.
At the activity level, the capacity of the affected hand was measured with the Melbourne Assessment 17 and the Jebsen–Taylor test. 23 The Melbourne Assessment scores unimanual capacity in 16 items. Raw scores were converted to a percentage score. The Jebsen–Taylor test measures movement speed in 6 unimanual tasks. The time to carry out the task was registered. The performance in activities of daily life was further assessed with the ABILAND-Kids questionnaire, which comprises 21 mainly bimanual activities for which parents rate the difficulty. 24 Raw scores were converted to logits. For these assessments, high levels of reliability and validity have been shown.24-26
Statistical Analysis
Observations were summarized using means and SDs or medians and interquartile ranges, as appropriate. Baseline characteristics and outcome measures were analyzed to check for differences between groups using independent t tests, Wilcoxon rank sum tests, or Fisher’s exact tests. Linear mixed models were used to study time effects of the interventions. Such models correct for the correlation among repeated observations within subjects using random effects. They also provide valid inferences when some observations are missing, provided that the reason for observations being missing is not related to unobserved outcomes. 27 Interactions between treatment and time were analyzed to test for differences in improvement over time between the 2 treatment groups. In case of a significant interaction between treatment and time, time trends were tested in each treatment group separately. Data were tested for normality by Shapiro–Wilk tests and graphically checked for symmetry. In case of skewness, an exponential transformation was used for the Melbourne Assessment scores, and a natural logarithmic transformation for the Jebsen–Taylor test and muscle strength scores. Significant time trends were further investigated with pairwise post hoc tests to compare individual time points. Additionally, the effect size was calculated using the Cohen’s d formula. 28 According to Cohen, effect sizes of .2 to .5 are considered as small, .5 to .8 are medium, and >.8 are large.
To identify which children benefited most, the variables “age,” “initial AHA score,” “time of wearing the constraint,” and “total amount of therapy” were included as covariates in the models for the primary outcome measure, together with their interaction with time and treatment. “Age,” “time of wearing the constraint,” and “total amount of therapy” were entered in the model as continuous variables. The total numbers of hours wearing the constraint was calculated for the total group (m-CIMT and m-CIMT + IT groups). The total amount of therapy (ie, time wearing the constraint plus total amount of intensive therapy) was calculated for the m-CIMT + IT group. “Initial AHA score” was entered as a class variable (cutoff level at 65 units) with a “high initial AHA score” or “low initial AHA score.” Additionally, to investigate the possible interference of the amount of routine therapy (upper limb physical and occupational therapy), which the children received in addition to the m-CIMT or m-CIMT + IT, this variable was included as a covariate in the model for the primary outcome measure.
The 2-sided 5% level of significance was used. All statistical analyses were performed using SAS version 9.2 (SAS Institute, Inc, Cary, NC).
Results
Participants
Sixty-six children were invited for participation. The parents of 15 children did not consent to participate. Three children declined for medical reasons, while the parents of 12 children decided not to be involved because the commitment of practicing 1 hour per day and possibly 3 additional therapy sessions was too high. The main reasons were lack of time due to schoolwork, other therapies, or leisure activities.
Twenty-six children were randomly allocated to the m-CIMT group and 25 to the m-CIMT + IT group. Three participants from the m-CIMT group discontinued the intervention. One other child in this group withdrew at the follow-up assessment. Information on the participating children and missing data are presented in Figure 1.
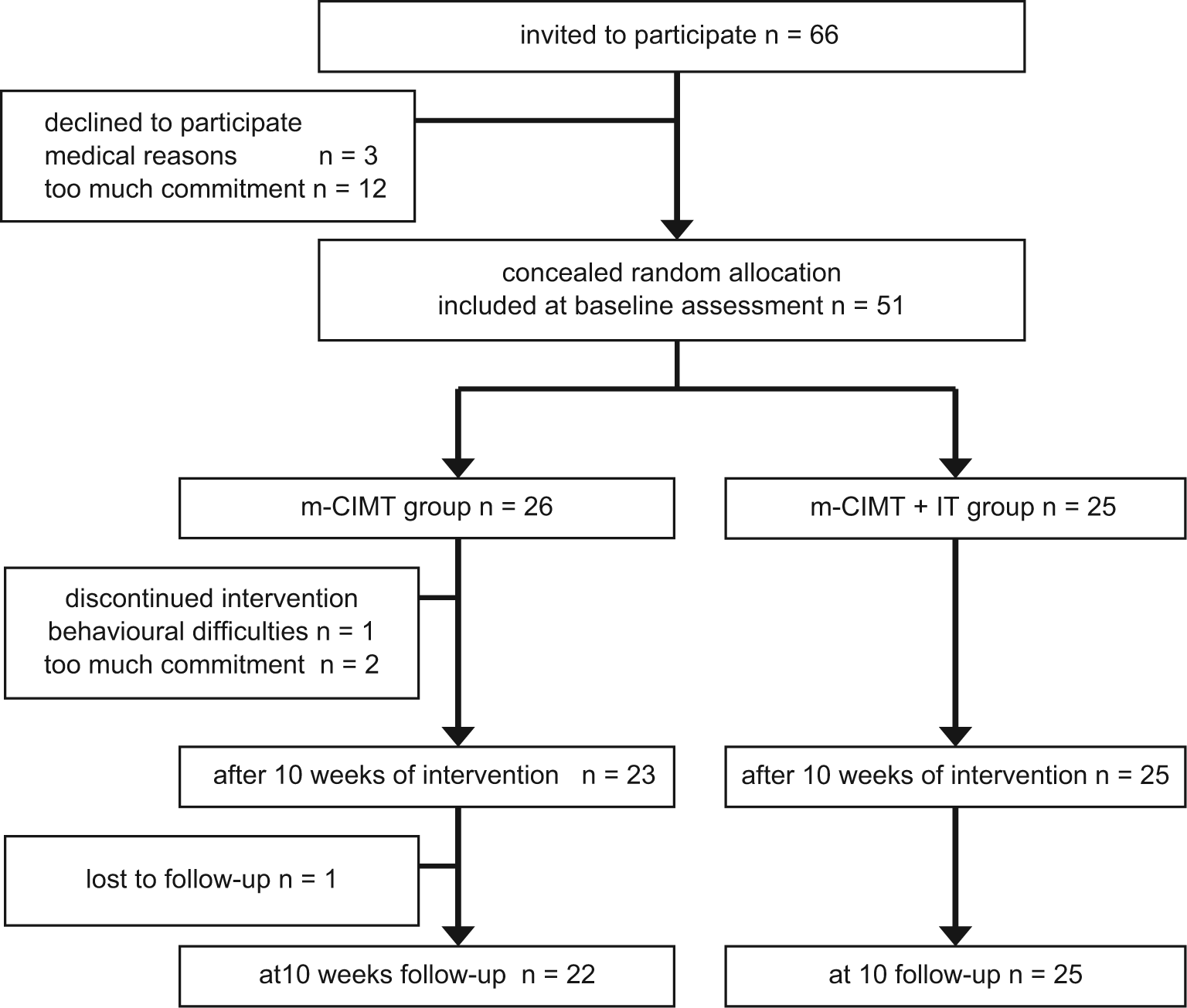
Number of children participating and details of missing data at the 3 measurement points.
The mean age for the total group was 8 years 9 months (SD = 2 years 2 months). Twenty-eight children had a left-sided unilateral CP. Thirty-seven out of 51 children attended mainstream schools. According to the MACS, 13 4 children were classified as level I, 38 as level II, and 9 as level III. Baseline characteristics showed no significant differences between groups (Table 1). All children received regular physical therapy varying from 1 to 5 sessions weekly, with a median duration of 120 minutes per week (range = 30-180 minutes). Of this therapy time, a median of 27 minutes per week was spent on upper limb treatment (range = 0-90 minutes). Ten children also received occupational therapy, with a median duration of 60 minutes (range = 30-90 minutes). There was no statistical difference between both groups in the amount of routine upper limb therapy (P = .38). During the intervention period, the children continued their routine therapy and additionally received an upper limb training program (m-CIMT or m-CIMT + IT).
Baseline Characteristics in Both Groups.
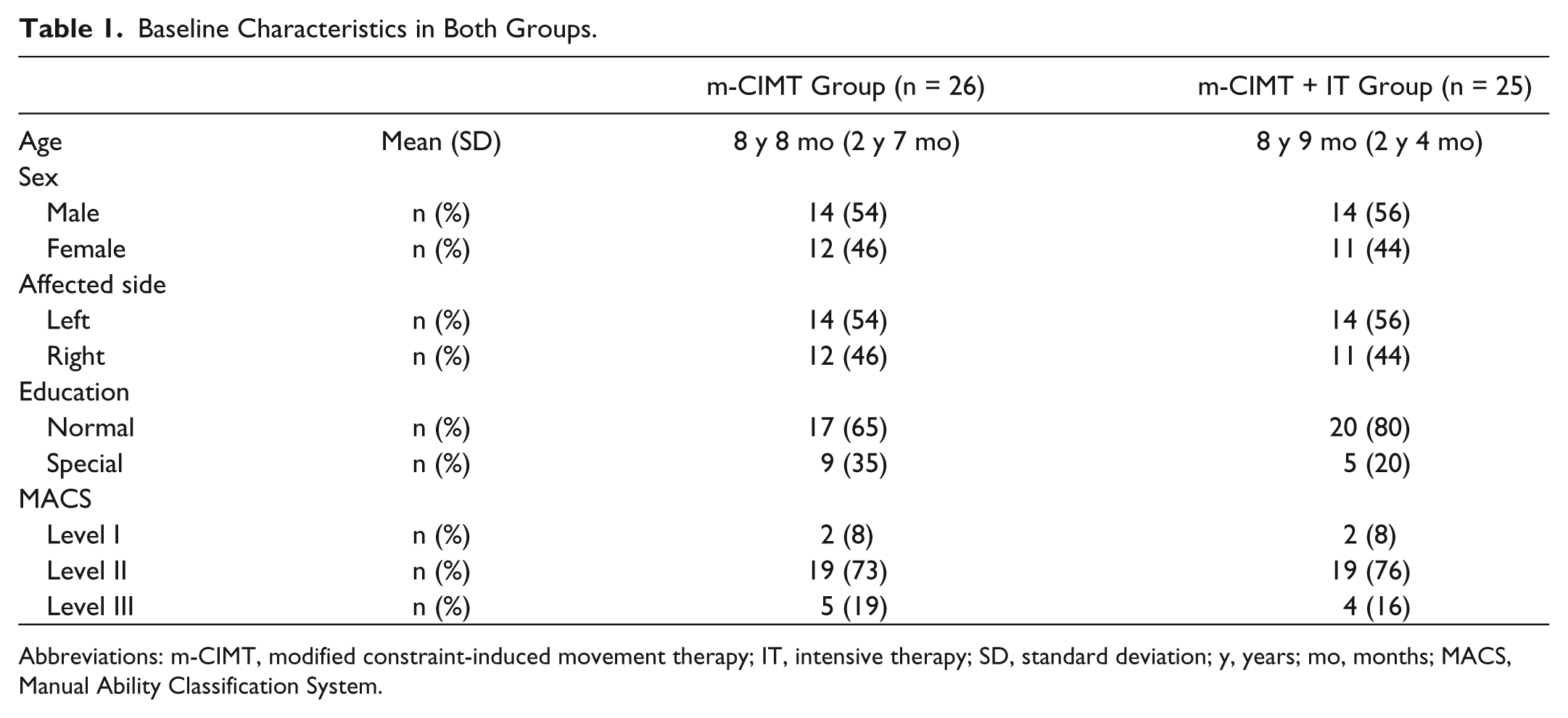
Abbreviations: m-CIMT, modified constraint-induced movement therapy; IT, intensive therapy; SD, standard deviation; y, years; mo, months; MACS, Manual Ability Classification System.
Compliance
The mean time spent wearing the constraint was 39 hours 30 minutes (SD = 12 hours) in the m-CIMT group and 39 hours 15 minutes (SD = 14 hours) in the m-CIMT + IT group. In the m-CIMT group, 15 out of 23 children wore the splint for more than 80% of the expected time (>40 hours). For the m-CIMT + IT group, a compliance of more than 80% was reached in 17 out of 25 children. There was no significant difference in compliance between groups. Children in the m-CIMT + IT group received a mean therapy time of 20 hours 30 minutes (SD = 3 hours). Twenty-two out of 25 children received more than 80% of the expected therapy sessions (>18 hours).
Treatment Efficacy
There were no significant differences between groups at baseline for all outcome measures. Results of the outcome measures for both groups are summarized in Table 2.
Descriptive Statistics of Outcome Measures at Baseline, After Intervention, and at 10 Weeks Follow-Up and Statistical Comparison (P Values).
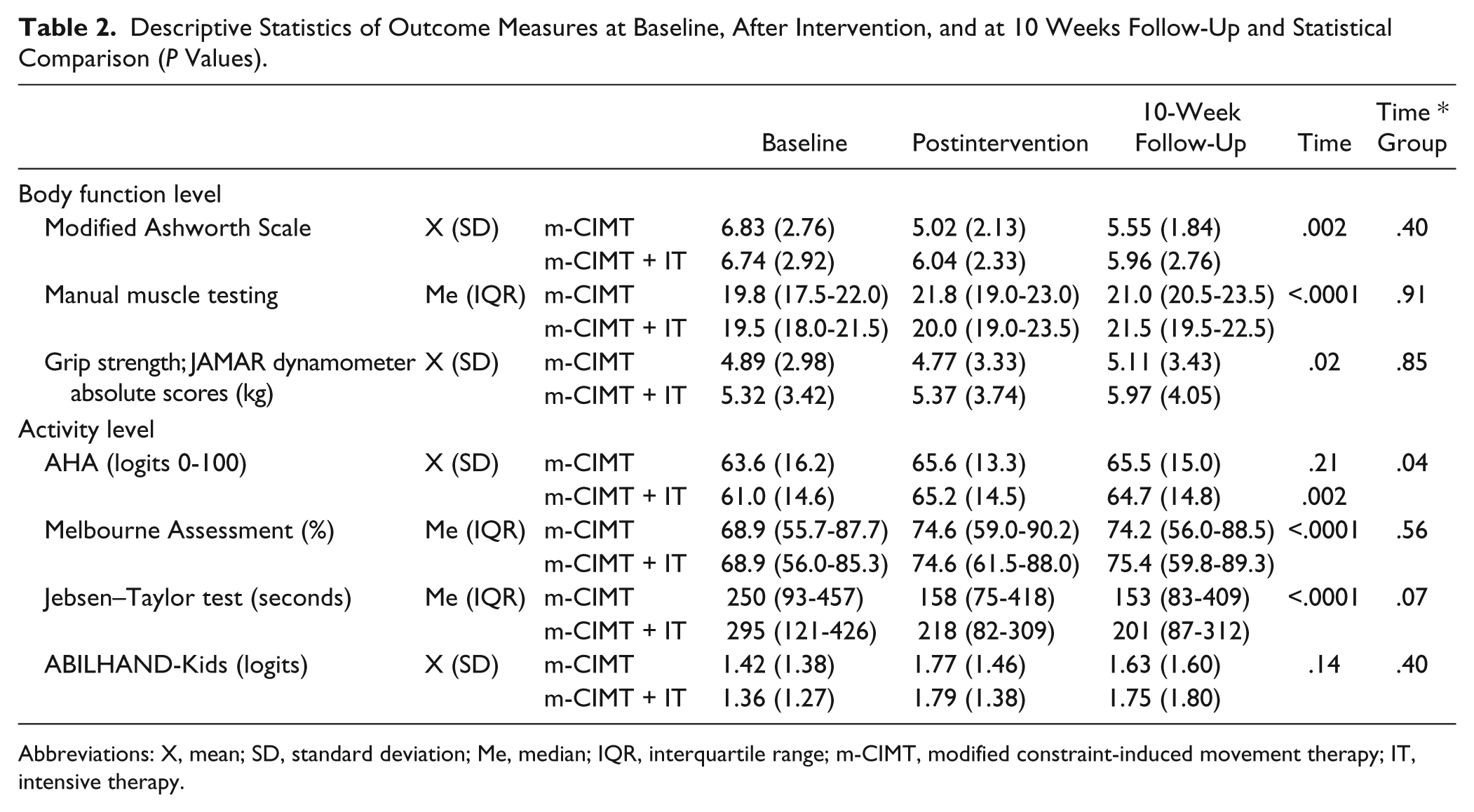
Abbreviations: X, mean; SD, standard deviation; Me, median; IQR, interquartile range; m-CIMT, modified constraint-induced movement therapy; IT, intensive therapy.
Primary Outcome
Results revealed a significant group-by-time interaction effect for the AHA in favor of the m-CIMT + IT group (F = 3.32, P = .04). Children in the m-CIMT + IT group showed a significant improvement (F = 8.54, P = .002), whereas the AHA scores in the m-CIMT group did not change (F = 1.67, P = .21). Post hoc tests showed immediate gains in the m-CIMT + IT group (T1-T2: t = −4.12, P = .0004), which were retained after follow-up (T1-T3: t = −2.68, P = .01). The mean difference between baseline and after intervention was 4.20 units (SD = 5.04) in the m-CIMT + IT group and 0.77 units (SD = 4.88) in the m-CIMT group, which accounted for an effect size of .66. Between baseline and follow-up, the mean change was 3.64 units (SD = 6.43) in the m-CIMT + IT group and 1.95 units (SD = 5.63) in the m-CIMT group, accounting for an effect size of .28.
Individual variation was high in both groups. In the m-CIMT + IT group, 10 children achieved an improvement larger than the SDD, whereas an improvement larger than the SDD was achieved in 6 children in the m-CIMT group.
Secondary Outcomes
At the body function level, no significant differences between groups were found. Analysis of time effects revealed that muscle tone decreased significantly (F = 6.47, P = .002). Manual muscle strength (F = 26.89, P < .0001) and grip strength (F = 4.19, P = .02) showed a significant increase. Post hoc tests showed that immediate effects were retained after follow-up for all body function measures (P < .01).
At the activity level, there was no significant group-by-time interaction effect for the Melbourne Assessment (F = 0.59, P = .56) or the ABILHAND-Kids questionnaire (F = 0.93, P = .40). There was a trend for greater improvement in the Jebsen–Taylor test in the m-CIMT + IT group (F = 2.68, P = .07).
Time effects showed a significant improvement in the Melbourne Assessment (F = 19.85, P < .0001) and the Jebsen–Taylor test (F = 45.76, P < .0001). Post hoc tests showed that significant gains in the Melbourne Assessment and the Jebsen–Taylor test were retained after follow-up (P < .0001). In most children, a positive effect in the Melbourne Assessment was seen, but individual changes exceeded the reported SDD of 7.4% 29 in only 4 of the 23 children in the m-CIMT group and in 6 of the 25 children in the m-CIMT + IT group. For the Jebsen–Taylor test, individual changes are expressed as a percentage of the baseline score. Large percentage changes were attained in both groups, which were more pronounced in the m-CIMT + IT group. The ABILHAND-Kids questionnaire showed no significant changes in scores (F = 2.0, P = .14).
Prognostic Factors
For bimanual performance, a significant interaction was found between time, treatment, and age (F = 2.96, P = .02). Figure 2A illustrates the interaction with age, in which children were divided into a younger (4 years 6 months to 8 years) and an older age group (8 to 12 years). Mean change in AHA scores are presented between baseline (T1) and immediately after intervention (T2), and between baseline (T1) and follow-up (T3) for the m-CIMT and the m-CIMT + IT groups. Younger children improved in the AHA in both intervention groups, whereas older children improved only in the m-CIMT + IT group.
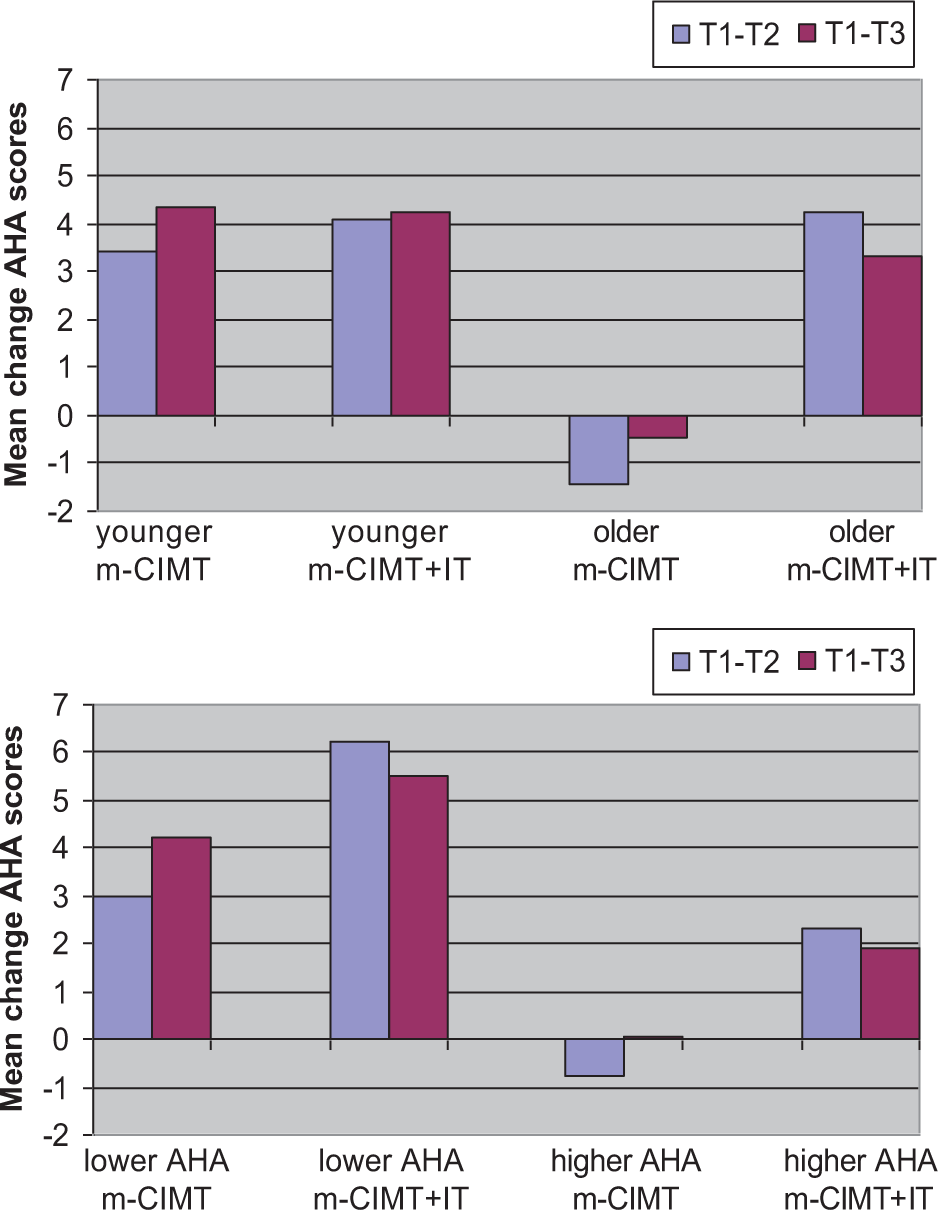
Mean change in AHA scores between baseline (T1) and immediately after intervention (T2), and between baseline (T1) and follow-up (T3) for the modified CIMT group (m-CIMT) and the modified CIMT plus intensive therapy group (m-CIMT + IT). Children were divided into the following: (A) An age group younger than 8 years (younger) and an age group older than 8 years (older); (B) A group with Assisting Hand Assessment (AHA) scores lower than 65 units (lower AHA) and a group with AHA scores higher than 65 units (higher AHA).
A significant interaction was also found between time, treatment, and initial AHA score (F = 2.36, P = .03). Children with a lower AHA score at onset made progress in bimanual performance in both intervention groups, although gains were more pronounced in the m-CIMT + IT group. Children with a higher AHA score improved only in the m-CIMT + IT group (Figure 2B). No significant interaction was found between time, treatment, and time of wearing the constraint for the total group (P = .26). For the m-CIMT + IT group, there was no significant interaction between time and total therapy time (time of wearing the constraint + intensive therapy time; P = .91). Finally, there was no significant interaction between time, treatment, and the amount of routine therapy.
Discussion
A randomized controlled trial in 51 children with unilateral CP was conducted to investigate the additional effects of an intensive therapy program combined with home-based m-CIMT. Children in the m-CIMT + IT group showed significantly greater improvement in bimanual performance compared to children in the m-CIMT group. A medium effect size between groups of 0.66 in the AHA was found, which was larger than in other upper limb intervention studies with ES varying between 0.22 and 0.59.9,25,29-31 The effect sizes were larger only in the studies of m-CIMT in very young children (effect size = 1.12-1.5).4,5,32 The model in this study, which incorporated a bimanual component to the m-CIMT training, resulted in improved bimanual practice. This supports the principles of training-specificity, implying that “you progress to what you actually practice.” Two recent studies similarly investigated a combined approach, in which m-CIMT was followed by bimanual training, also leading to an improvement in bimanual performance.9,10
Other outcome parameters of activity level showed no differences between groups. Only the Jebsen–Taylor test revealed a trend toward greater change in the m-CIMT + IT group. Also, at the body function level, no differences between groups could be demonstrated. In view of the focus of the therapy program on distal muscle strength, we would have expected differences in muscle strength to favor this group. Vaz et al 12 found a significant change in wrist extension strength after a strength program. However, analytical exercises to improve strength were only a minor part of the intensive program. To gain muscle strength, a more specific and intensive training protocol seems to be required.
Our study showed overall improvements in muscle strength, grip strength, muscle tone, and unimanual capacity through m-CIMT with or without an intensive therapy program. Moreover, immediate gains were retained after follow-up. These improvements are considered clinically relevant when compared to a longitudinal study in 81 children with unilateral CP where no changes were observed for these outcome measures over 1 year of routine therapy. 16 Our results also corroborate the findings of previous studies.3,7,29,33,34 However, an essential difference is that the intensity of the constraint was only 1 hour per day versus at least 2 hours in previous studies. Despite the limited application of the constraint, positive results were shown. A unique aspect of our study was the application of m-CIMT in the home situation, provided by parents and supervised by the main investigators. This individually based distributed practice encourages the intensive use of the affected hand in the child’s natural environment. Eliasson et al4,32 evaluated a limited m-CIMT application of 2 hours at home with beneficial effects in children aged between 18 months and 4 years. Our study suggests that this type of m-CIMT can also be effectively applied in children older than 4 years. However, these findings are based on a nonrandomized design and should be interpreted with caution. A randomized controlled design is needed to investigate different intensities of m-CIMT to optimize cost-efficiency.
Nonetheless, the feasibility of this type of m-CIMT is an important consideration. Most studies using an intensive CIMT or m-CIMT program of 2 weeks reported that participants quickly adapted to the constraint with minimal difficulties. 3 It could be questioned whether distributed practice over a period of 10 weeks at home is as feasible. Our data showed a large variability in time spent wearing the constraint. Nine children in the m-CIMT group and 8 in the m-CIMT + IT group did not reach the 80% compliance level of 40 hours. The main reason for this was lack of time due to schoolwork, other therapies, or leisure activities. Some parents also reported that it was difficult to find attractive activities, especially in children with poor hand function. These results underpin our beliefs that when implementing m-CIMT at home, a careful selection of children and families and close supervision by the therapist is warranted. However, despite our program being based at home with limited supervision, only 3 participants did not complete the 10-week program that supports the adherence to the training protocol.
A second aim was to identify which children benefited most from the interventions. Younger children showed benefits from both interventions, whereas older children only improved in bimanual performance in the m-CIMT + IT group. It seems that younger children can learn to incorporate the arm into the body frame and to use the arm more spontaneously. This may be related to the developmental nonuse phenomenon and can potentially explain the positive results in previous studies in young children.4,5,32 Furthermore, response to treatment was better in children with an initially lower ability. However, children with better abilities receiving the intensive therapy program also showed beneficial gains, which might be explained by the individually tailored program. In these children, high-level unimanual tasks, for example, in-hand manipulation and finger selectivity, and increasingly complex bimanual coordination tasks were trained. Further data analysis (not reported) showed that the beneficial gains in younger children and children with initially lower AHA units were not significantly related to a higher amount of time wearing the restraint or therapy time. Furthermore, it could be questioned whether the difference in AHA baseline scores between groups, with lower scores in the m-CIMT + IT group, could be an influencing factor for the greater level of improvement in this group. However, the difference between groups of 2.6 units was not significant and smaller than the SDD of 5 units. Further exploration of the prognostic factors showed that children with initially lower AHA scores benefited most, and in this subgroup, the mean baseline score was similar in both intervention groups (48.7 units). We therefore believe that the difference in baseline scores does not negate our findings. Another possible interfering factor could be the routine therapy that the children received in addition to m-CIMT or m-CIMT + IT. However, the total amount of routine therapy was not a significant covariate, implying that the amount of routine therapy did not have an impact on the treatment effects. In the literature, predictive factors have rarely been investigated,4,7,8 and the conflicting results highlight the need for large multicenter trials to investigate the individual characteristics of children who benefit most from these therapeutic approaches. Other factors such as body function measures, cognitive factors, type of brain lesion, and cortical reorganization should be explored.
This study also warrants some critical reflections. All children in the m-CIMT + IT group received the IT program from different therapists and this may have induced variability within the programs. However, efforts were made to standardize the training by developing a manual and carefully instructing therapists. Second, by adding an intensive therapy to the m-CIMT program, it is unclear whether the effect was based on the content of the specific program or rather on the higher intensity of practice. A direct comparison between treatment programs of equal intensities would further clarify this matter. Another limitation of the study was that no control group was included. However, many studies have already shown positive effects of m-CIMT training versus no training. 3 Also, in a longitudinal study over 1 year in children following routine therapy, no evolution was found in body function measures, the Melbourne Assessment, or the AHA. 16 Finally, the follow-up assessment was performed 10 weeks after intervention, which is too short to judge long-term retention of the reported gains. Further research is needed to pursue longer term outcomes.
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.