
Abstract
Background. Pain is one of the most common and disabling “nonmotor” symptoms in patients with dystonia. No recent study evaluated the pharmacological or physical therapy approaches to specifically treat dystonic pain symptoms. Objective. To evaluate the effectiveness of KinesioTaping in patients with cervical dystonia (CD) and focal hand dystonia (FHD) on self-reported pain (primary objective) and on sensory functions (secondary objective). Methods. Twenty-five dystonic patients (14 with CD and 11 FHD) entered a randomized crossover pilot study. The patients were randomized to 14-day treatment with KinesioTaping or ShamTaping over neck (in CD) or forearm muscles (in FHD), and after a 30-day washout period, they received the other treatment. The main outcome measures were 3 visual analog scales (VASs) for usual pain, worst pain, and pain relief. Disease severity changes were evaluated by means of the Toronto Western Spasmodic Torticollis Rating Scale (CD) and the Writer’s Cramp Rating Scale (FHD). Furthermore, to investigate possible KinesioTaping-induced effects on sensory functions, we evaluated the somatosensory temporal discrimination threshold. Results. Treatment with KinesioTape induced a decrease in the subjective sensation of pain and a modification in the ability of sensory discrimination, whereas ShamTaping had no effect. A significant, positive correlation was found in both groups of patients between the improvement in the subjective sensation of pain and the reduction of somatosensory temporal discrimination threshold values induced by KinesioTaping. Conclusions. These preliminary results suggest that KinesioTaping may be useful in treating pain in patients with dystonia.
Introduction
Idiopathic focal dystonia is a disorder characterized by prolonged involuntary muscle contractions causing abnormal postures of a single body part (blepharospasm, spasmodic torticollis, writer’s cramp). Although dystonia is commonly defined as a “motor” condition, 1 “nonmotor” symptoms are increasingly recognized as an important determinant of quality of life in dystonic patients.2-4 Pain is one of the most common and disabling “nonmotor” symptoms occurring in up to 70% of patients with cervical dystonia and up to 30% of patients with focal hand dystonia.2-5 Current treatment for focal dystonia is symptomatic and can range from pharmacological (drugs, botulinum toxin) to surgical (selective peripheral denervation, deep brain stimulation) interventions. 6 These treatments may also be effective in relieving pain in a number of patients; however, no recent study evaluated specific approaches to treat dystonic pain symptoms. Moreover, there is a paucity of literature examining the effect of physical therapy approaches in dystonia,7-9 and to our knowledge, no study was specifically focused on improving pain symptoms.
KinesioTaping is an alternative taping technique, currently used in rehabilitation in the treatment of various musculoskeletal and neuromuscular deficits.10-12 Recently KinesioTaping has been used in patients suffering from orthopedic and neurological diseases with promising results in relieving pain.13-15
We designed a randomized crossover clinical study to evaluate the effectiveness of KinesioTaping in patients with cervical dystonia (CD) or with focal hand dystonia (FHD) on self-reported pain. The experimental intervention was KinesioTaping over the neck muscles (in CD) or over the forearm muscles (in FHD) for 2 weeks; the control intervention was a sham tape (ShamTaping) application.
The primary outcome measure was the identification of changes in pain severity assessed by means of visual analog scales. Furthermore, since patients with dystonia present specific sensory abnormalities, that is, the temporal discrimination between tactile stimuli (defined as the ability to perceive 2 tactile stimuli applied to the skin as clearly distinct),16,17 we investigated possible KinesioTaping effects on objective sensory functions. Evaluation of the somatosensory temporal discrimination threshold (STDt) and changes in disease severity were assessed as secondary outcome measures.
Methods
Study Design
The study was a single-center randomized crossover pilot study. Patients were randomly assigned to the experimental (KinesioTaping) or control (ShamTaping) treatment, and after a 30-day washout period, they received the alternative treatment. The randomization sequence was created using computer generated random number tables, with 1:1 allocation of individuals to either the intervention group or the control group. Subjects were assessed 4 times: at the inclusion visit (T0), after 14 days with the tape in situ (T1), after a 30-day washout period (T2), and after 14 days with the tape in situ (T3). Outcome assessors and patients were unaware of group assignments. All authors vouch for the completeness and accuracy of the data and attest to the fidelity of the trial to the protocol. The randomization and the study design are summarized in Figure 1A and B.
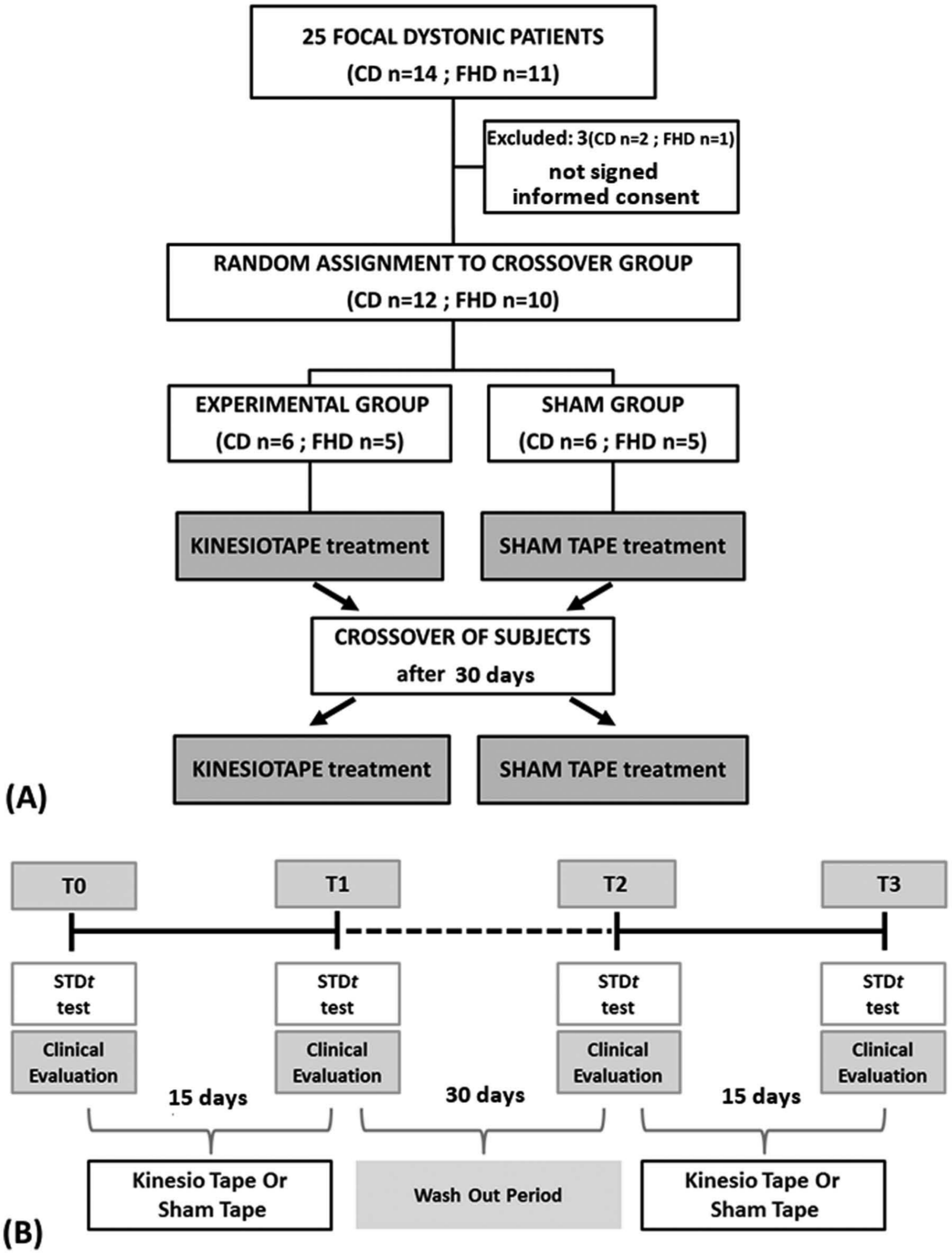
(A) Flow chart of recruitment and randomization of study participants. (B) Time line of the experimental protocol.
Participants
A total of 25 consecutive outpatients affected by focal dystonia (according to standard diagnostic criteria) 18 entered the study. All participants were recruited from the outpatients of the Movement Disorders clinic of the Department of Neuroscience, University of Genoa. For each subject, informed consent was obtained prior to the experiments according to our institutions’ policy and according to the Declaration of Helsinki. The study was approved by the local ethics committee of the University of Genoa. The randomization and the study design are summarized in Figure 1.
The following exclusion criteria were applied: (a) past history of neurological disorders other than dystonia, (b) presence of psychiatric or sensory/somatic abnormalities, (c) cognitive deficits (Mini-Mental State Examination [MMSE] score < 24); and (d) treatment with botulinum toxin in the past 6 months. Three subjects did not meet the inclusion criteria and were excluded from the study.
Participants were naïve to the purpose of the study and they did not have any previous experience of KinesioTaping application.
Cervical Dystonia
This group consisted of 12 patients (Female = 8; mean age = 55.83 ± 9.0 years) affected by CD. Disease duration ranged from 3 to 19 years (mean = 7.2 ± 5.9 years). The severity of motor impairment was evaluated by means of the Toronto Western Spasmodic Torticollis Rating Scale, 19 and the mean severity score was 18.08 ± 6.6. All patients presented a prevalent rotational torticollis with involvement of the sternocleidomastoid (SCM). Detailed demographic and clinical information are provided in Table 1.
Baseline Demographic and Clinical Characteristics of the Participants.
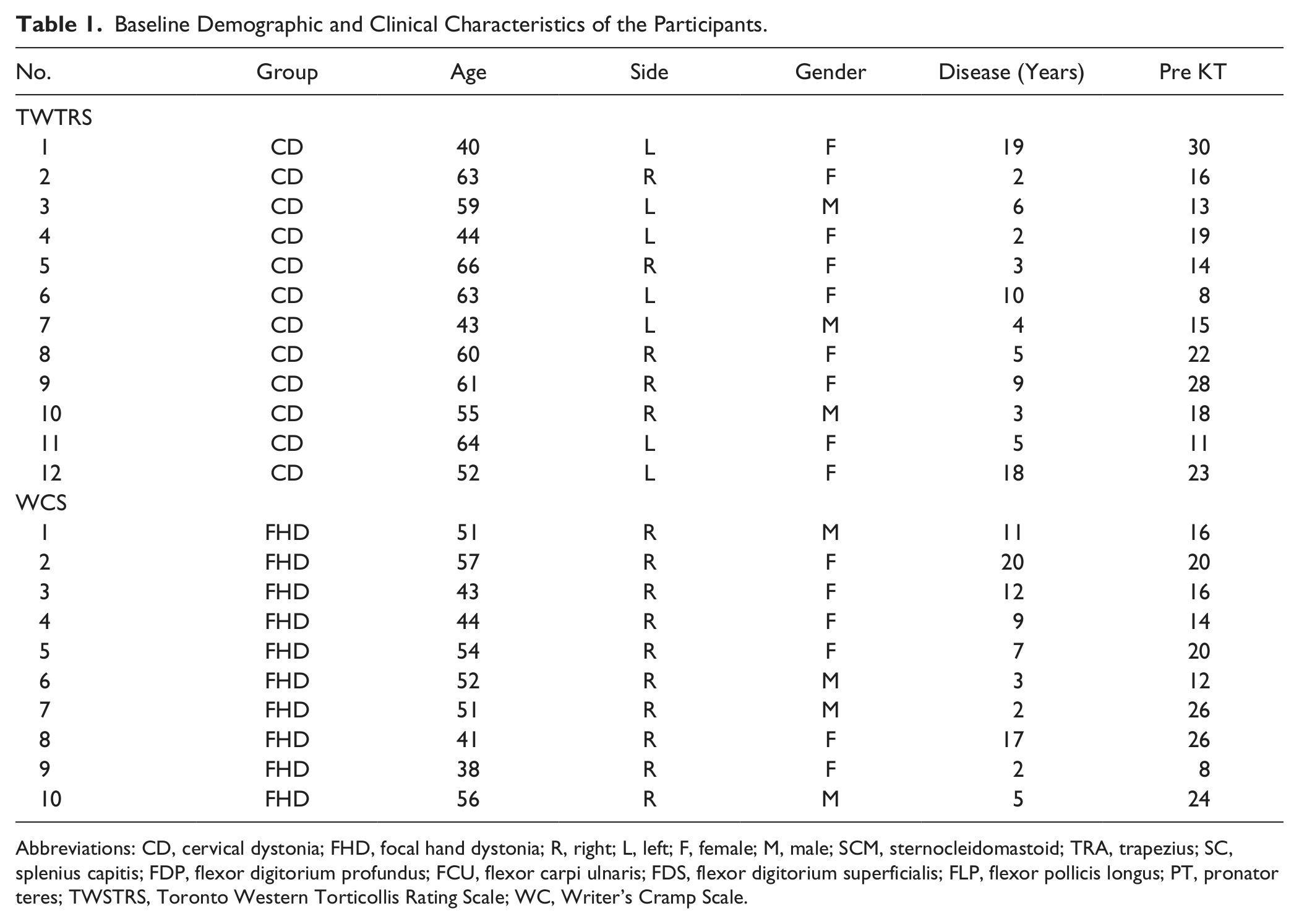
Abbreviations: CD, cervical dystonia; FHD, focal hand dystonia; R, right; L, left; F, female; M, male; SCM, sternocleidomastoid; TRA, trapezius; SC, splenius capitis; FDP, flexor digitorium profundus; FCU, flexor carpi ulnaris; FDS, flexor digitorium superficialis; FLP, flexor pollicis longus; PT, pronator teres; TWSTRS, Toronto Western Torticollis Rating Scale; WC, Writer’s Cramp Scale.
Focal Hand Dystonia
This group consisted of 10 patients (Female = 7; mean age 48.7 ± 6.5 years) affected by writer’s cramp in the dominant hand. All participants were right handed (Edinburg Handless Inventory). Duration of the disease ranged from 2 to 20 years (mean = 9.2 ± 6.3 years). Disease severity was evaluated by means of the Writer’s Cramp Rating Scale, 20 and the mean severity score was 18.2 ± 5.8. In all patients the dystonic features were prevailing in the wrist flexor muscles.
Detailed demographic and clinical information are provided in Table 1.
Taping Interventions
All participants were taped by the same investigator (a certified KinesioTaping physiotherapist) who did not participate in the outcome assessment. The treatment group received, as first intervention, a standardized therapeutic application of KinesioTape, while the control group started with an ineffective taping application (ShamTape). A standard beige KinesioTape was used for all the applications, and we choose “I”-shape strips as they have been indicated as effective in treating pain symptoms. 21 Taping was replaced by the physiotherapist involved in the study every 4 days.
For the experimental treatment, the tape was applied with paper-off tension, which means applying the tape directly to the skin as it comes off the paper backing (approximately with 15% to 25% of available tension). 21 In patients with CD, KinesioTape was applied over the SCM dystonic muscle by means of 2 “I-strips”: the first strip was placed on the medial (sternal) head and the second was applied on the lateral (clavicular) head of the SCM muscle (Figure 2A). KinesioTape was applied from the mastoid bone to the clavicle (rostrocaudal direction) with the SCM placed in a position of maximum stretching. In patients with FHD, KinesioTape was applied over the medial-upper part of the forearm dystonic muscles by means of 2 “I-strips”: each of them was applied on the flexor carpi radialis (FCR) and on the flexor carpi ulnaris (FCU; Figure 2A). KinesioTape was applied in a rostro-caudal direction while the forearm muscles were stretched.
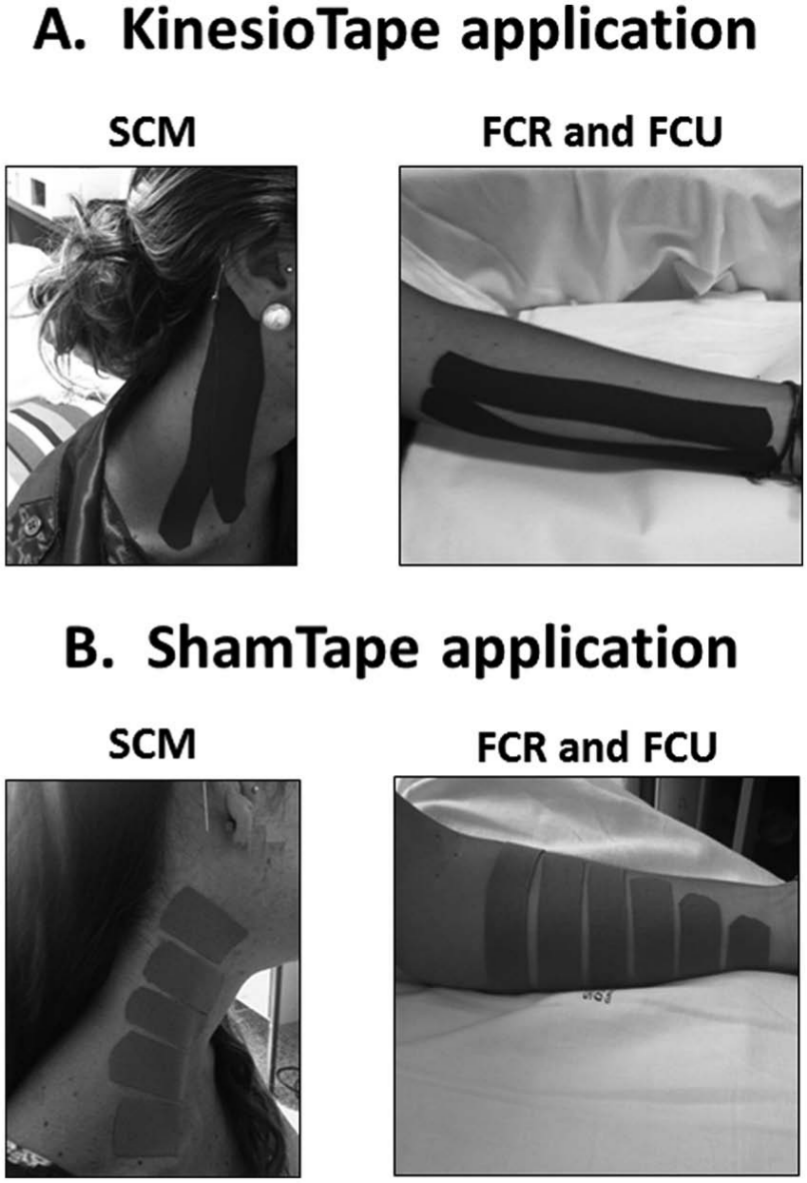
KinesioTape (A) and Sham (B) application.
For the control treatment (ShamTaping), smaller “I-strips” of KinesioTape were used and they were applied, with no tension and without stretching the muscles, perpendicularly to the muscle belly (starting from the middle and progressing to each side) over the same dystonic muscles as in the experimental group (Figure 2B). Although the specific therapeutic elements of KinesioTaping (ie, longitudinal stretch, start and ending point tape application) were removed, the procedure was very similar to that adopted in the experimental KinesioTaping treatment. Patients were informed that they will be submitted to 2 different types of taping techniques, each one potentially effective, and the patients were not able to distinguish between “real” and “sham” taping. On the other hand, due to the nature of the intervention it was not possible to blind the physiotherapist to patient allocation.
Outcome Measures
Clinical Assessment
Main outcome measures were 3 visual analog scales for usual pain (VAS-U), worst pain (VAS-W), and Pain Relief (VAS-PR). In addition, we evaluated disease severity changes by means of the Toronto Western Spasmodic Torticollis Rating Scale (for CD) and the Writer’s Cramp Rating Scale (for FHD).
Evaluation of Somatosensory Temporal Discrimination Threshold
In all the patients, STDt was tested in 2 different body regions: in the neck and in the forearm (one affected and one unaffected depending on patients’ type of focal dystonia). Testing was performed on the skin overlying the muscles where the tape was applied. Fourteen normal subjects (NS), age (49.1 ± 9.3) and gender (Females = 8) matched with dystonic patients were recruited as a control group, and STDt was tested on the same body areas.
STDt was determined by delivering square wave electrical pulses with a constant current stimulator with a D360 amplifier (Digitimer Limited, D360, Welwyn Garden City, UK). The stimulation intensity was defined for each subject by delivering a series of stimuli at increasing intensity from 2 mA in steps of 1 mA; the intensity used for STDt was the minimal intensity perceived by the subject in 10 of 10 consecutive stimuli. Paired stimuli were applied starting with an inter-stimulus interval (ISI) of 0 ms (simultaneous pair) and progressively increasing the ISIs (in 10 ms steps). Twenty-four ISIs (from 0 to 230 ms) were included in our experimental protocol. During the test the ISIs were applied in a random sequence and subjects had to report whether they perceived a single stimulus or 2 temporally separated stimuli. The first of 3 consecutive ISIs at which patients recognized the stimuli as temporally separated was consider the STDt. 22
In patients with focal dystonia, STDt was tested immediately before taping application, at T0 and at T2 and 12 hours after the tape was removed at T1 and T3. Specifically, patients were instructed to remove the taping on the last day of treatment at 9
Statistical Analysis
For continuous variables, since data were not normally distributed (according to the Kolmogorov–Smirnov statistical test), nonparametric tests were used to assess at baseline differences in clinical data between groups (VASs for pain) and, separately for each group (CD and FHD), the effect of “Treatment” (real or sham) on clinical outcomes (VASs for pain and disease severity score). Mann–Whitney U test was used for between-subjects analysis, and the Wilcoxon rank-sum test was used for within-subjects analysis.
STDt values in patients and healthy subjects were compared in a between-group repeated-measures (RM) ANOVA with the factor “Group” (NS, CD and FHD) as the main between-subjects factor and the factor “Body region” (neck and forearm) as the main within-subjects factor.
RM ANOVA with the factors “Treatment” (real and sham), “Time” (before and after treatment), and “Body region” (neck and forearm) as within-subject factors and “Group” (CD and FHD) as between-subjects factor was used to compare STDt changes induced by KinesioTaping treatment in dystonic patients.
To evaluate if there were any lasting effects on VASs for pain and STDt during the washout, we compared values at the 2 baselines (T0 vs T2) by means of paired t tests, separately in the groups of patients who underwent first experimental or control KinesioTaping treatment.
Spearman’s correlation coefficient was used for assessing possible correlations between changes in STDt values and changes in disease severity and pain scores.
When ANOVA gave a significant result (P < .05), post hoc analysis was performed using t tests.
All statistical analyses were performed with SPSS 18.0.
Results
Evaluation of Pain
At baseline, the VAS scores for pain were significantly higher in the CD group than in the FHD group (VAS-U: P < .001; VAS-W: P = .014). KinesioTaping treatment induced a decrease in the VAS scores for pain in both CD (VAS-U: P = .003; VAS-W: P = .002) and FHD (VAS-U: P = .01; VAS-W: P = .004), whereas the VAS scores for pain did not change after ShamTaping treatment either in CD (VAS-U: P = .65; VAS-W: P = .15) or FHD (VAS-U: P = .48; VAS-W: P = .32). The percentage of pain relief was 45% in CD and 19% in FHD after KinesioTaping treatment, whereas it was 5% in CD and 6% in FHD after ShamTaping treatment. No lasting effects of either KinesioTaping (VAS-U, P = .19; VAS-W, P = .35) or ShamTaping treatment (VAS-U, P = .10; VAS-W, P = .20) on VAS scores were found when comparing the 2 baseline values (T0 vs T2).
In CD, neither KinesioTaping (P = .74) nor ShamTaping treatment (P = .56) influenced disease severity score, evaluated by means of the Toronto Western Spasmodic Torticollis Rating Scale. In FHD, neither KinesioTaping (P = .41) nor ShamTaping treatment (P = .38) influenced disease severity score, evaluated by means of the Writer’s Cramp Rating Scale. All clinical data are reported in Table 2.
Mean (SD) Baseline and Postintervention of Primary Outcome Measures for Participants. Mean (SD) Baseline Disease Severity Score. a
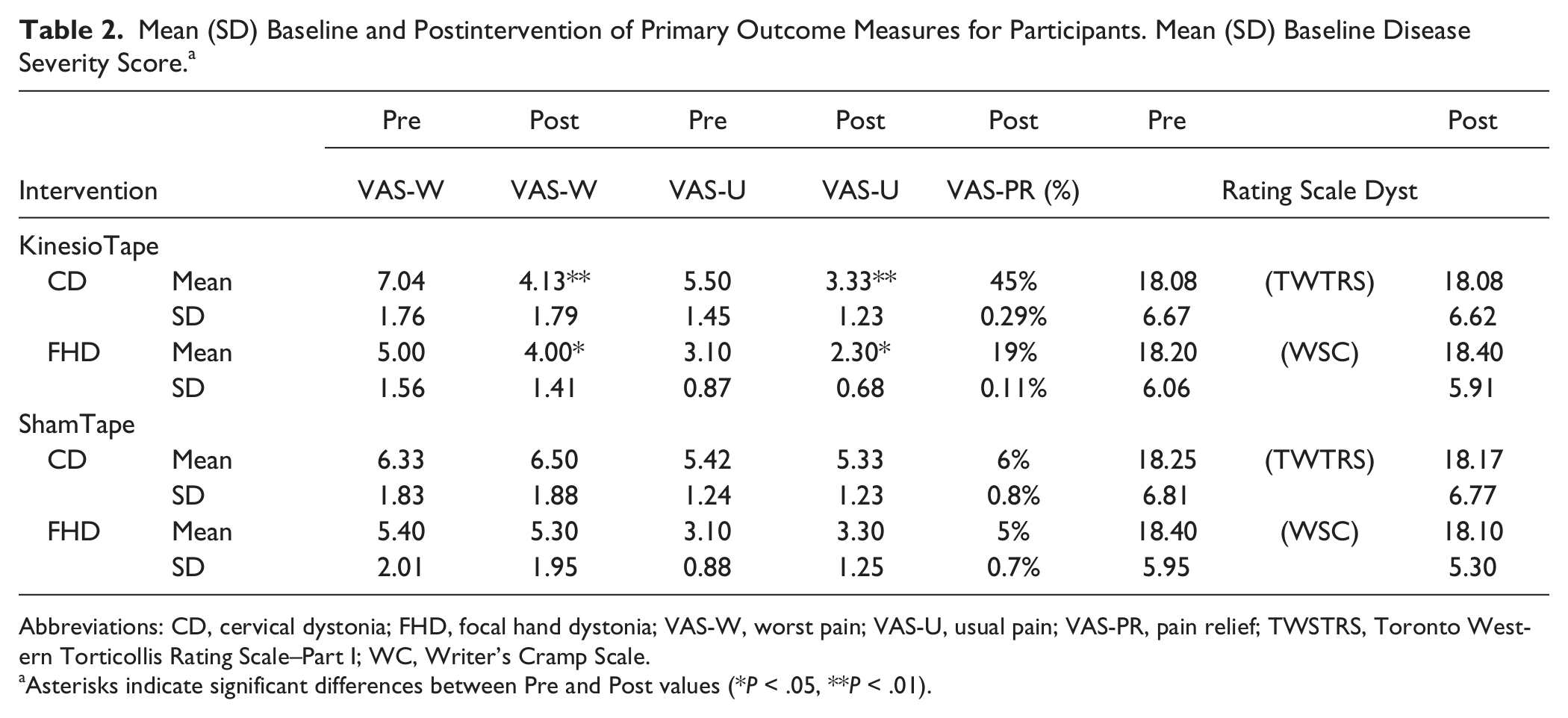
Abbreviations: CD, cervical dystonia; FHD, focal hand dystonia; VAS-W, worst pain; VAS-U, usual pain; VAS-PR, pain relief; TWSTRS, Toronto Western Torticollis Rating Scale–Part I; WC, Writer’s Cramp Scale.
Asterisks indicate significant differences between Pre and Post values (*P < .05, **P < .01).
At the end of each period of taping application, no side effects (such as skin irritation and/or hypersensitivity) were observed and patients reported a positive feedback on acceptability.
Evaluation of STDt
The intensity of electrical stimuli for STDt testing was unchanged across the different time points of STDt recordings (P always >.05).
As expected, STDt values in the affected and unaffected body regions at baseline were higher in patients than in healthy subjects. RM ANOVA showed a significant factor “Group” (F(2, 33) = 9.04; P = .001), a significant factor “Body region” (F(1, 33) = 3.73; P = .035), and a significant interaction “Group* Body region” (F(2, 33) = 4.03; P = .027). Post hoc analysis revealed that STDt values were lower in NS than in CD and FHD patients for both the neck (CD, P < .0001; FHD, P = .008) and the forearm regions (CD, P = .008; FHD, P < .0001). No difference in the STDt values of neck and forearm regions was found between CD and FHD patients (neck, P = .39; forearm, P = .2).
KinesioTaping induced a reduction of STDt in dystonic patients only in the affected (and treated) body region whereas ShamTaping left the abnormal STDt unchanged in the 2 body regions (Figure 3). RM ANOVA showed a significant interaction “Treatment* Time* Body region* Group” (F(1, 20) =36.98; P < .0001). Post hoc analysis revealed that, in patients with CD, the KinesioTape applied over the neck induced a decrease of STDt in the neck (before vs after treatment P < .0001), but not in the forearm (before vs after treatment P = .11). Furthermore, in CD patients, the ShamTape applied over neck left the STDt unchanged in the 2 body regions (neck: before vs after treatment P = .87; forearm: before vs after treatment P = .77). In FHD patients, the KinesioTape applied over the forearm induced a decrease of STDt in the forearm (before vs after treatment P < .0001), but not in the neck (before vs after treatment P = .71). Furthermore, in FHD patients, the ShamTape applied over the forearm left the STDt unchanged in the 2 body regions (neck: before vs after treatment P = .32; forearm: before vs after treatment P = .28).
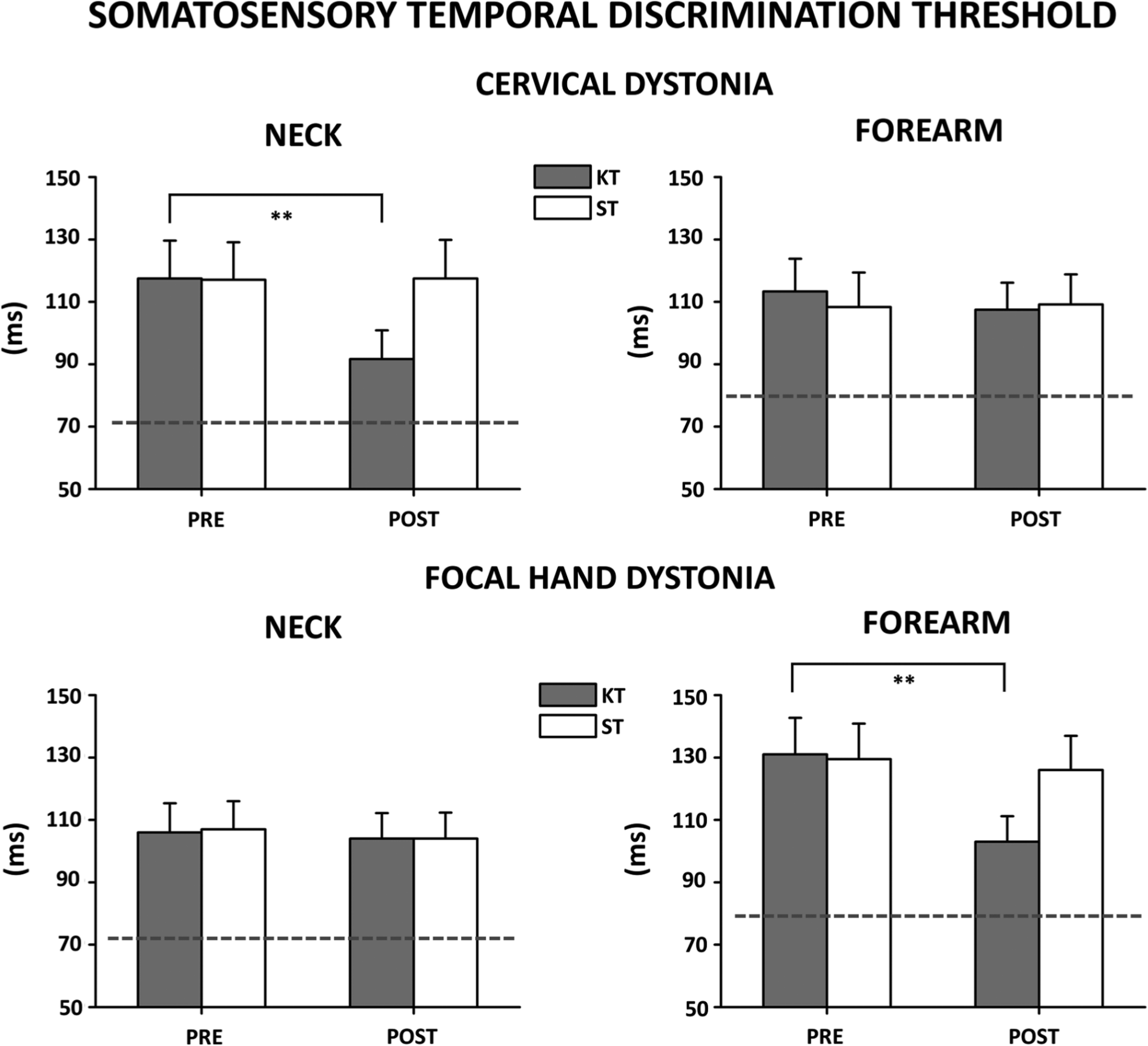
Somatosensory temporal discrimination thresholds (STDt) tested in 2 body parts (neck and forearm) in patients with cervical dystonia (CD) and focal hand dystonia (FHD) before and after KinesioTaping (KT) and ShamTaping (ST) treatment in the neck muscles and forearm muscles, respectively.
After KinesioTaping treatment the reduction of STDt was 20% in either neck (in CD) and forearm (in FHD); however, STDt values were still higher in patients than in healthy subjects and RM ANOVA showed a significant factor “Group” (F(2, 33) = 5.05; P = .012). Post hoc analysis revealed that STDt values were still lower in NS than in CD (P = .015) and FHD patients (P = .008) whereas there was no difference between CD and FHD (P = .72).
Finally, it is worth noting that no lasting effects of either KinesioTaping (P = .83) and ShamTaping treatment (P = .31) was found when comparing the 2 STDt baseline values (T0 vs T2).
Clinical Correlation
Changes in STDt values induced by KinesioTaping in the affected body region were positively correlated with changes in the VAS-U score for usual pain both in patients with CD (Spearman rho = 0.64; P = .026) and FHD (Spearman rho = 0.61; P = .045), thus suggesting that STDt changes might, at least in part, be a consequence of the reduction of the subjective sensation of pain induced by KinesioTaping (see Figure 4).
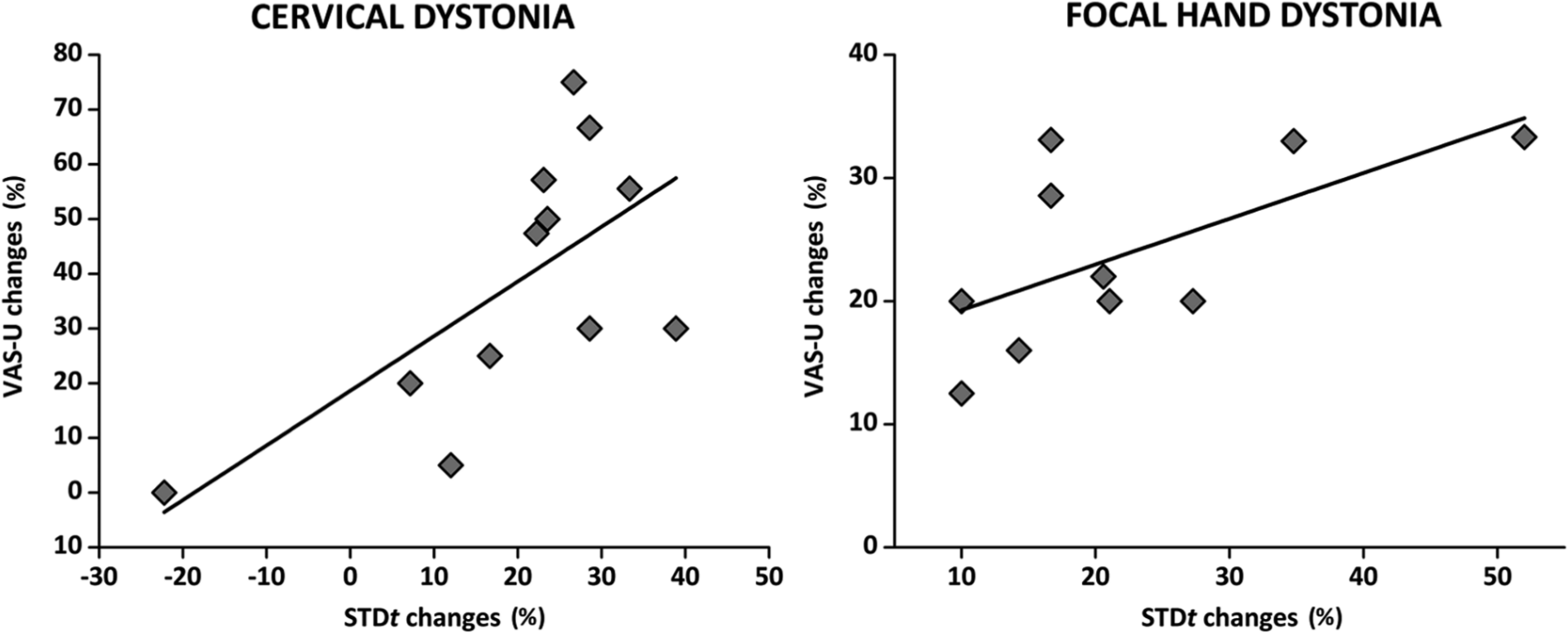
Linear correlation between changes in STDt values and changes in the VAS-U score for usual pain induced by KinesioTaping treatment, in patients with cervical dystonia and focal hand dystonia.
Discussion
The aim of the present study was to assess the possible effectiveness of KinesioTaping in relieving pain symptoms in patients with focal dystonia. Furthermore, to elucidate the possible effects of KinesioTaping on sensory functions, we included in the study the evaluation of STDt, which is consistently abnormal in dystonic patients.22-24
Treatment with KinesioTape induced a decrease in the subjective sensation of pain (assessed with the VAS) and a modification in the ability of sensory discrimination. Indeed, after 14-day treatment with KinesioTape, the VAS scores for usual and worst pain were significantly reduced in patients with both cervical and focal hand dystonia, whereas no change was observed after sham treatment. As expected, the STDt was higher in dystonic patients than in healthy subjects 25 in both affected and unaffected body regions. 22 After KinesioTaping, STDt selectively decreased in the affected body regions (neck for CD, forearm for FHD), where the KinesioTape was applied. Furthermore, a significant positive correlation was found in both groups of patients between the improvement in the subjective sensation of pain (decrease of VAS for usual pain) and the reduction of STDt values induced by treatment. On the other hand, no modification of dystonia severity was observed after KinesioTaping treatment. Such discrepancy is not surprising, since a large body of evidence suggests that dystonic pain cannot be entirely explained by excessive muscle contraction and the severity of dystonia in the neck muscles does not always correlate with the duration or intensity of neck pain. 26 Indeed, treatment with botulinum toxin can improve dystonic contractions without relieving pain or vice versa.27-30
The Effect of KinesioTaping on Pain
Pain is a common and disabling symptom that presents across all the different types of focal dystonia. One potential reason for such high prevalence is that the threshold for experiencing pain may be reduced in dystonic subjects. Pain-pressure thresholds were about 2 times lower in 9 patients with idiopathic cervical dystonia versus a group of age- and gender-matched controls. 31
Patients with dystonia may also have abnormalities in pain processing, even in body parts without dystonic involvement. For example, in the same study, the unaffected masseter muscles of patients with idiopathic cervical dystonia also showed reduced pain-pressure thresholds compared with the control group. 31 Another potential mechanism for enhanced pain includes changes in the somatosensory system that have been largely documented in patients with focal or generalized dystonia. These include changes in excitability on neurophysiological testing, abnormal cortical representation of dystonic body parts, and changes in somatosensory cortical activity during movement. 32
The observed reduction of self-reported pain after 14 days of treatment with KinesioTape is in line with recent studies showing the efficacy of this treatment in improving pain not only after acute but also in chronic injuries. 13 Three possible mechanisms may be considered to explain the pain relieving effect. First, KinesioTaping seems to in increase the flow of blood and lymphatic fluids due to a lifting effect, which creates a wider space between the skin and the muscle and interstitial space. Second, when mechanical loads create a deformation of the skin, the tape is supposed to stimulate the cutaneous mechanoreceptors. 33 This activation causes local depolarizations that trigger nerve impulses along the afferent fibers traveling toward the central nervous system. Pain modulation according to the “gate control theory” is a plausible explanation as it has been proposed that KinesioTaping provides an increased afferent feedback. 34 Finally, we cannot exclude that, by acting on cutaneous mechanoreceptors and proprioceptors KinesioTaping might influence sensory integration at a central level in patients with dystonia.
The Effect of KinesioTaping on Somatosensory Temporal Discrimination
One intriguing result of the present study is that KinesioTaping treatment was able to improve the ability to discriminate 2 somatic stimuli temporarily separated. Furthermore, the reduction of STDt values induced by treatment was significantly and positively correlated with the improvement in the subjective sensation of pain, suggesting that the KinesioTaping-induced reduction of pain may contribute to the modulation in sensory discrimination ability.
The somatosensory temporal discrimination is a purely sensory process that allows the brain to select relevant sensory inputs for processing information coming from external sources. A recent study by Conte and coworkers 35 showed that, by applying theta burst stimulation to the cortical areas involved in processing sensory discrimination, the STDt is probably encoded in the primary somatosensory area (S1), possibly depending on intrinsic S1 neural circuit properties. This finding agrees with previous observations showing that single-pulse transcranial magnetic stimulation over S1 interferes with STDt processing.36,37 Accordingly, in dystonia, Tamura et al 38 showed that in a group of patients with focal hand dystonia the abnormal STDt correlates with altered intracortical inhibition of somatosensory evoked potentials (SEPs). The authors showed an inverse correlation between STDt and the activity of inhibitory circuits within the somatosensory cortex, suggesting that inhibitory mechanisms within the sensory areas play a main role in STDt process. In particular, surround inhibition is an inhibitory mechanism within the somatosensory system that helps sharpen acuity and aids in 2-point discrimination.39-41 Patients with dystonia present abnormalities in surround inhibition processes within the somatosensory system. 42
In experimental studies, it has been demonstrated that surround inhibition under noxious electrical stimulus is stronger, possibly to provide finer discrimination during the noxious stimulus.43,44 A direct correlation between pain and defective surround inhibition within the somatosensory cortex has not yet been provided in dystonia. However, we can hypothesize that the KinesioTaping-induced reduction of pain may cause a modulation of surround inhibitory mechanisms within the somatosensory cortical representation of the area treated with KinesioTape. Such modulating effect of nociceptive inputs on intracortical inhibitory processes in the sensory areas is not likely to be the sole mechanism involved in STDt abnormalities in patients with dystonia. Indeed, STDt abnormalities have been reported in affected and unaffected body regions (without correlation with disease severity) and even in patients’ unaffected relatives, suggesting that STDt may represent a primary endophenotypic trait.22-25
We might postulate that 2 different mechanisms are involved in discrimination abnormalities in dystonia: a “peripheral” mechanism, dealing with the amount of sensory information coming from periphery (including nociceptive inputs), and a “central” mechanism, dealing with multimodal sensory integration at the central level that involves the interplay between cortical and subcortical structures including basal ganglia.
Study Limitations and Future Research
It is important to stress the exploratory nature of this study and its limitations. First, because of the study design (crossover), follow-up evaluations were not performed. Future studies designed to assess what is the optimal duration of the KinesioTaping treatment and possible long-term effects in a large cohort of patients would be useful.
Second, the secondary aim of the present study was to assess the possible effectiveness of KinesioTaping in modifying motor symptoms in dystonia. However, motor disability has been assessed by means of numeric rating scales, which are congruent with clinical practice, but present poor sensitivity in measuring small changes. Further works based on kinematic quantitative evaluation of movements might provide valuable information for early detection of improvement of movements after KinesioTaping treatment. Finally, we hypothesized that the reduction of pain may contribute to the modulation in sensory discrimination ability, since we found a correlation between the reduction of STDt values and the improvement in the subjective sensation of pain in the affected (and treated with KinesioTape) body parts. However, since we did not evaluate the effect of KinesioTape on STDt in nonaffected body parts, we cannot exclude other potential physiological mechanisms that are worthy to be investigated in future research.
Conclusions
The present preliminary results suggest that KinesioTaping may be useful in treating pain in patients with dystonia. In addition, KinesioTaping treatment is likely to interfere with the mechanism underlying abnormalities in temporal discrimination between tactile stimuli in focal dystonia.
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.