
Abstract
Objective. This study examines performance of Wolf Motor Function Test (WMFT) tasks in terms of the ability of EXCITE trial participants (who had suffered a stroke 3-9 months before recruitment) to complete the task within the timed interval. Methods. Data were collected from participants who received constraint-induced movement therapy (CIMT) 3 to 9 months poststroke (CIMT-I, n = 106) or 15 to 21 months poststroke (CIMT-D, n = 116). Performance on the 15 timed WMFT tasks was converted into binary values, and changes in completion of the tasks were analyzed with generalized estimating equation methods, under the assumption of a binomial or Poisson process for completion. Results. During CIMT, the CIMT-I group showed significant within-group improvements in 3 fine-movement tasks and in total noncompleted tasks (noncompletes), whereas the CIMT-D group did not (P ≤ .0036). CIMT-I improvement was significantly greater than CIMT-D improvement for the lifting pencil task and total noncompletes. During the year following CIMT, neither group showed significant changes in completion of WMFT tasks. Over all time intervals, only the CIMT-I group displayed significant improvement in several tasks and total noncompletes. Between groups, there were significant and almost-significant differences between the improvements of the 2 groups in 3 tasks requiring fine distal movement. Conclusion. Receiving CIMT earlier appears to improve reacquisition and retention of WMFT tasks, especially those requiring fine motor skills. Combined with earlier findings, these results indicate that improvements in existing motor abilities are possible with both immediate and delayed CIMT, but early CIMT is necessary for significant reacquisition of tasks.
Introduction
Over the past 30 years, forced use paradigms have effectively improved motor function in patients with mild to moderate stroke.1-3 Constraint-induced movement therapy (CIMT) combines forced use with shaping and repetition, and over the past decade, CIMT has been shown to be effective in enhancing motor function in patients with mild to moderate stroke of varying chronicity.4-10 One such effort, the Extremity Constraint Induced Therapy Evaluation (EXCITE) trial, studied patients 3 to 9 months poststroke and examined the effects of 2 weeks of CIMT delivered immediately after randomization (CIMT-I) as compared with CIMT delivered after a 1-year delay (CIMT-D). 11 As in several other studies of CIMT, the EXCITE trial used the Wolf Motor Function Test (WMFT) as an outcome measure.8,12-15 The inability to complete a WMFT task within the 2-minute timed interval indicates a severe level of impairment, whereas a restored ability to perform a task within the 2 minutes indicates a qualitative improvement in ability. 6
Analysis of the EXCITE data set revealed that those patients who received CIMT immediately showed greater improvement than those who received CIMT after a 12-month delay (WMFT performance time and Motor Activity Log, P < .0001; Stroke Impact Scale Hand and Activities domains, P < .0009 and 0.0214, respectively). However, the 2 groups achieved an equivalent level of function by 24 months. 11 As clinicians and investigators continue to seek therapeutic applications that yield clinically meaningful changes, another study examined the ability of EXCITE participants to complete WMFT tasks. 16 In this study, the completion rates were examined over the first therapy period, in which CIMT-I participants received CIMT and CIMT-D participants did not. For tasks that were not completed at the baseline visit, CIMT-I participants were significantly more likely to complete tasks after the period than were CIMT-D participants. This finding was particularly true of tasks requiring dexterity. The total number of tasks completed also improved significantly.
Here, we again adopt a binary definition of performance on the WMFT (completion within the 2 minutes of permitted time for performance vs failure to complete) during examination of the entire EXCITE trial data set. The present analyses extend the previous findings by looking at changes over 3 additional time periods, as described in the Methods section. This extended effort provides the first opportunity to understand the prolonged impact of CIMT on the ability to complete tasks that previously could not be completed within the 2-minute time period. Based on accumulating evidence that earlier (but not immediate) provision of CIMT may induce favorable plasticity within the nervous system, 17 we anticipated that both groups would reacquire task completions but the gain would be greater among participants who received CIMT earlier.
Methods
Patient Characteristics
Patients, all of whom were recruited within the institutional review board guidelines of EXCITE locations (Emory University, University of Alabama at Birmingham, University of Florida, Ohio State University, University of Southern California, University of North Carolina, and Wake Forest University), were evaluated and, if meeting the inclusion criteria as described previously, randomized into 1 of 2 groups using a dynamic assignment procedure.6,14 One group began 2 weeks of CIMT immediately after randomization (CIMT-I, n = 106), and the other delayed their CIMT for 1 year (CIMT-D, n = 116) but had the option to receive usual and customary care for that first year. Each group had a follow-up evaluation 12 months after the CIMT.11,18
Analysis by Participant
The WMFT was administered to participants several times during the EXCITE trial (Figure 1). 14 WMFT scores were evaluated by multiple evaluators across sites, with 1 evaluator at each site for the 5-year study duration. Each of these evaluators was assessed annually for reliability. Reliability consistently met the criterion of equal to or greater than 0.9 but if it had not at any point, the evaluator would have been required to undergo more training.
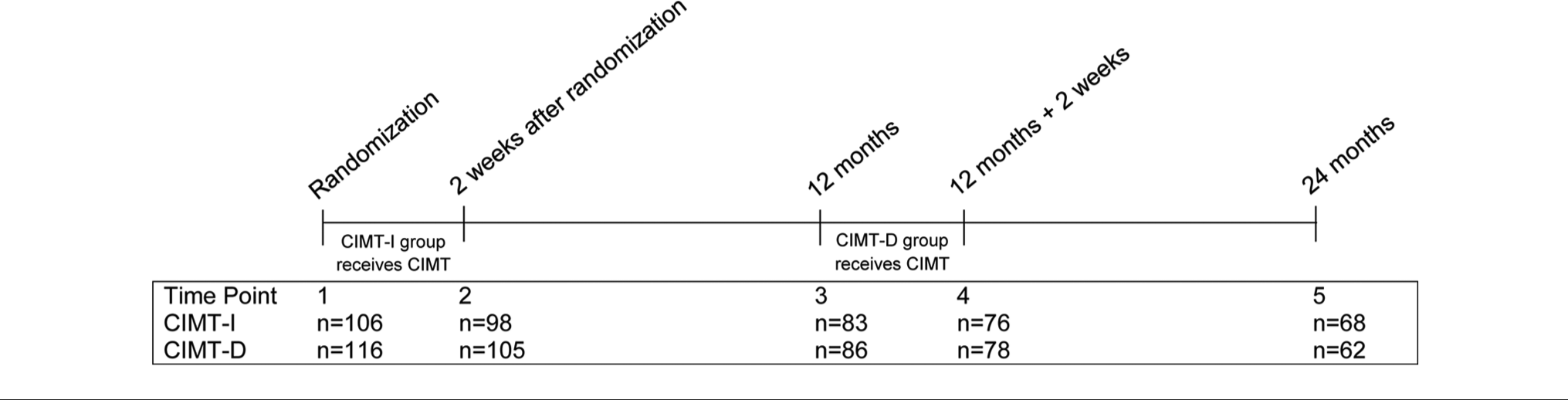
Timeline of the study, including sample size of the 2 groups at specific time points. Key time points include the following: immediately prior to randomization (time point 1), 2 weeks after randomization (time point 2), 12 months after randomization (time point 3), 2 weeks thereafter (time point 4), and 12 months later (time point 5). Between time points 1 and 2, the CIMT-I group received the intervention, whereas the CIMT-D group could receive usual and customary care consisting of any treatment except CIMT. 11 Between time points 3 and 4, the CIMT-D group received the CIMT intervention. Time point 5 occurred 24 and 12 months after the CIMT-I and CIMT-D, respectively, received the intervention. Abbreviations: CIMT, constraint-induced movement therapy; CIMT-I, CIMT immediate; CIMT-D, CIMT delayed.
Comparison 1 examined change over the CIMT period (CIMT-I, point 1 to 2 vs CIMT-D, point 3 to 4). Comparison 2 examined change over the period following the end of training (CIMT-I, point 2 to 3 vs CIMT-D point 4 to 5). Comparison 3 examined change from before training to 1 year later (CIMT-I, point 1 to 3 vs CIMT-D point 3 to 5). For each patient, the WMFT data from the evaluations were collected, and performance for each task was categorized as completed or not completed based on the participant’s ability to complete the task within 120 s.
Analysis by Task
Comparing the total number of completed and noncompleted tasks (hereafter referred to as completes and noncompletes) per WMFT task at the various time points reveals changes in participants’ ability to perform tasks. Shifts in completes from one time point to another were categorized as one of the following: No Change Completes (task successfully completed at first and second evaluation), New Completes (reacquisition; task not completed at first time point but was completed at second time point), No Change Noncompletes (task not completed at either the first or second time point), Regress Events (task completed at first time point but not completed at second time point).
Statistical Analysis
Task completion was determined for each participant and classified in binary fashion as either completed or not completed. The total array of binary values was then examined for each of the 15 timed WMFT tasks. The analysis of the dependent binomial completion data was done using generalized estimating equation methods in PROC GENMOD in SAS 9.3. The data were modeled as dependent (5 visits, time points 1-5) binomial (completed task or failed to complete task) data for the CIMT-I and CIMT-D participants. To perform specific comparisons, defined contrasts were evaluated. This method ensured that the results were both optimal in the estimation of error terms (because all observations are included) and consistent over comparisons. The total number of noncompleted data were modeled again as a generalized estimating equation analysis, using a Poisson process for the count of noncomplete cases. A Bonferroni correction was calculated to account for the comparison of 14 tasks and was .0036 (α = .05/14 = .0036). One of the 15 tasks could be completed by all participants and showed no change (Table 1, task 1, column 2); consequently, this task was not included in the correction. This adjustment resulted in a substantial reduction in α level and aimed to avoid both type I and type II errors. Regress events were examined using tests of independent proportions, using the Bonferroni corrected α level.
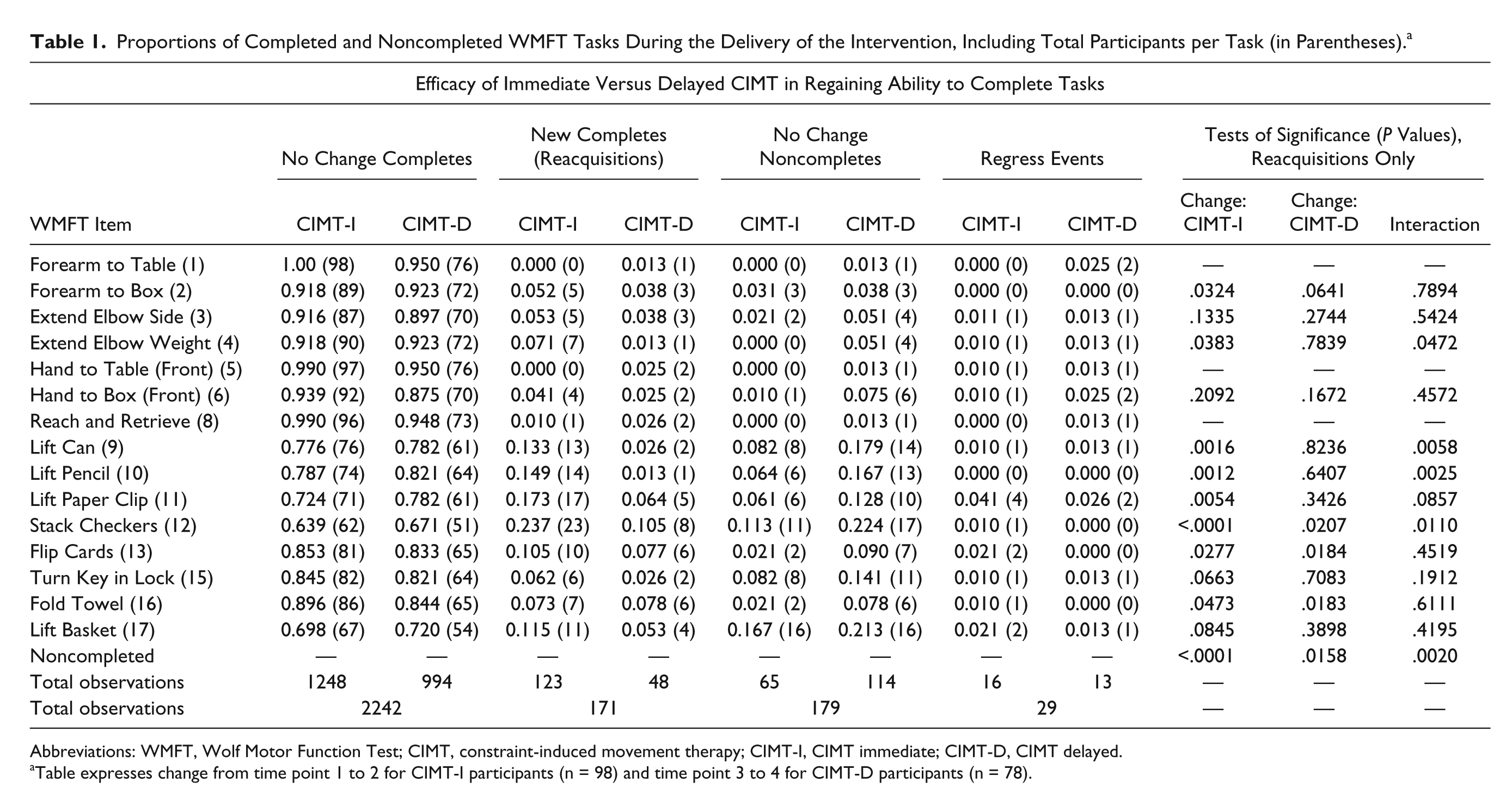
Proportions of Completed and Noncompleted WMFT Tasks During the Delivery of the Intervention, Including Total Participants per Task (in Parentheses). a
Abbreviations: WMFT, Wolf Motor Function Test; CIMT, constraint-induced movement therapy; CIMT-I, CIMT immediate; CIMT-D, CIMT delayed.
Table expresses change from time point 1 to 2 for CIMT-I participants (n = 98) and time point 3 to 4 for CIMT-D participants (n = 78).
Results
Patient Retention
Of the original 106 CIMT-I participants, 98 finished the treatment, and 83 completed the follow-up 12 months later. Of the 116 participants randomized into the CIMT-D group, 86 began the treatment 12 months later, 78 completed the treatment, and 62 completed the 12-month evaluation (Figure 1). At baseline, there were no significant differences between the study groups in demographic, stroke-related, or cognitive characteristics. 6
Efficacy of Immediate Versus Delayed CIMT Treatment in Task Completion
The CIMT-I group received a 2-week CIMT training interval within 3 to 9 months poststroke. In contrast, the CIMT-D group received the training 15 to 21 months poststroke. 11 Among within-group changes, the CIMT-I group showed significant improvements in the ability to lift a can (proportion of reacquisitions = 0.133), lift a pencil (proportion of reacquisitions = 0.149), and stack checkers (proportion of reacquisitions = 0.237; tasks 9, 10, and 12) and in the total proportion of noncomplete tasks reacquired (Table 1). The group also showed large improvements in lifting a paper clip (task 11, proportion of reacquisitions = 0.173), which trended toward significance following the Bonferroni correction (P = .0054). In contrast, the CIMT-D group showed no significant changes over the course of their 2 weeks of training.
Comparing between groups (Table 1, column 12) revealed that the CIMT-I group had significantly greater improvement in reacquiring lifting a pencil (task 10) and in the proportion of total noncompletes. This group also demonstrated improvement in lifting a can (task 9), although the difference between the groups’ reacquisitions of this task trended toward significance after the Bonferroni correction (P = .0058). Note that results are not presented for tasks 1, 5, and 8; this is because the analysis had technical difficulties as a result of the low frequency of noncompletes for these tasks.
Persistence of CIMT Gains (12 Months)
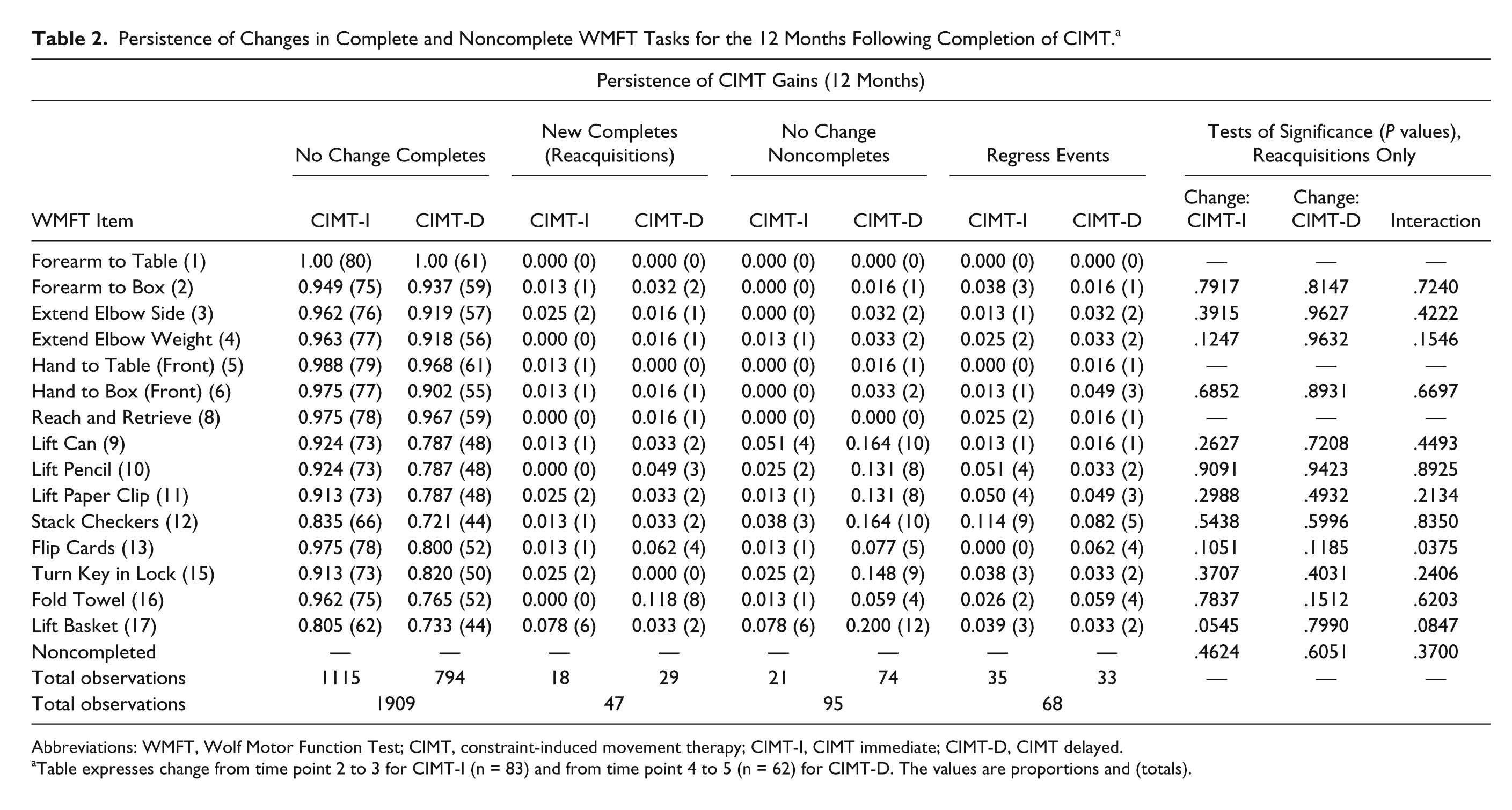
The persistence of CIMT gains was examined 12 months after the conclusion of CIMT training. There were no significant within-group changes, suggesting that the gains made during the training intervals for both groups were maintained for 12 months (Table 2). There were no significant differences in task reacquisition between groups.
Persistence of Changes in Complete and Noncomplete WMFT Tasks for the 12 Months Following Completion of CIMT. a
Abbreviations: WMFT, Wolf Motor Function Test; CIMT, constraint-induced movement therapy; CIMT-I, CIMT immediate; CIMT-D, CIMT delayed.
Table expresses change from time point 2 to 3 for CIMT-I (n = 83) and from time point 4 to 5 (n = 62) for CIMT-D. The values are proportions and (totals).
Overall Change (Treatment + Persistence)
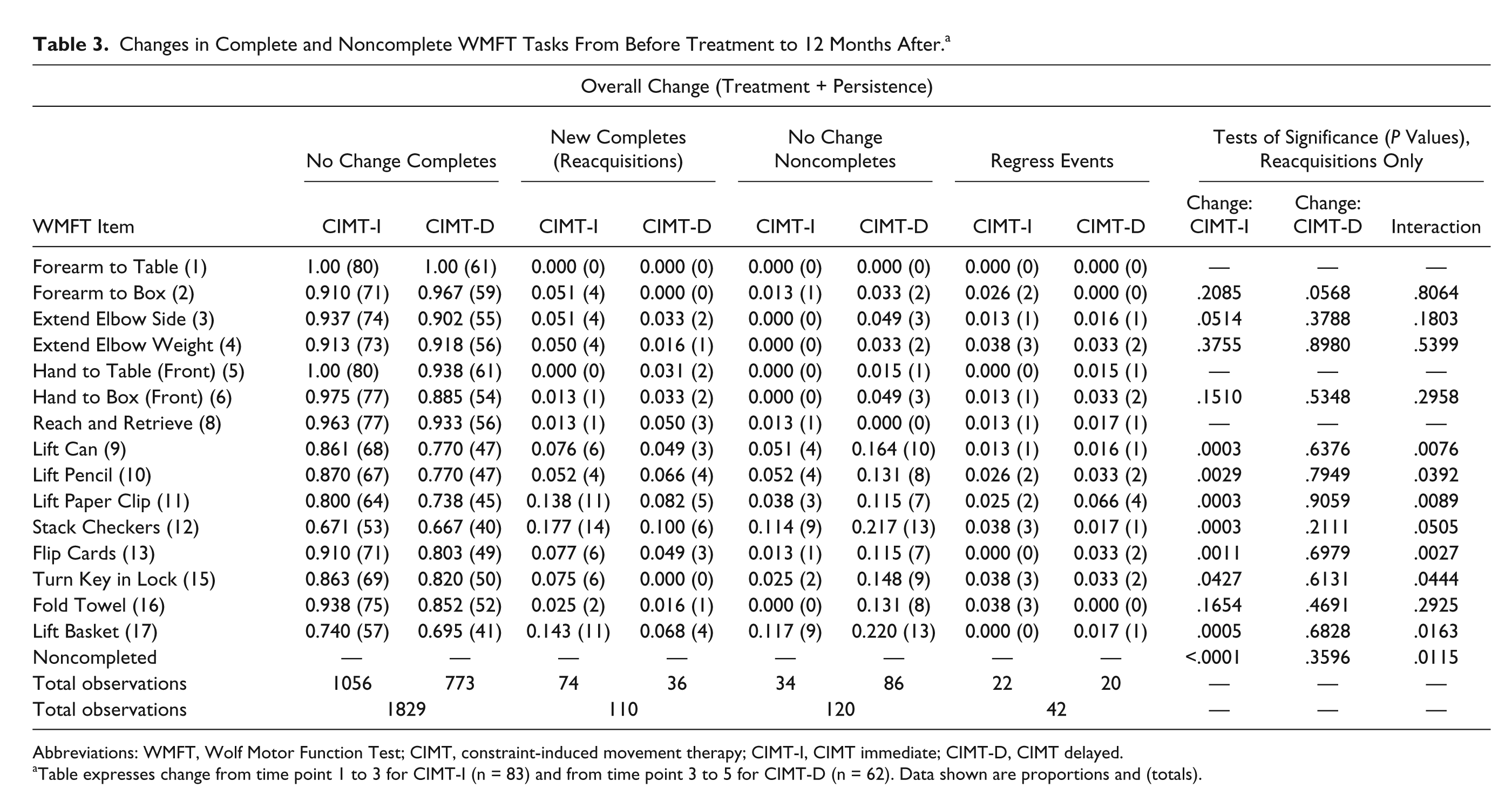
The overall change in function from pre-CIMT to 12 months after completion of CIMT was examined (for the CIMT-D group, this does not include the year of usual and customary care prior to the intervention). With respect to within-group changes, the CIMT-I group showed significant gains in lifting a can, pencil, and paper clip; stacking checkers; flipping cards; lifting a basket (tasks 9-13 and 17) and the total number of noncompletes (Table 3). Conversely, the CIMT-D group showed no significant changes during the corresponding time period. The between-group differences in reacquiring tasks favored the CIMT-I group and were significantly different in flipping cards (task 13) and trended toward being significantly different in lifting the can and the paper clip (tasks 9 and 11; P = .0076 and .0089, respectively).
Changes in Complete and Noncomplete WMFT Tasks From Before Treatment to 12 Months After. a
Abbreviations: WMFT, Wolf Motor Function Test; CIMT, constraint-induced movement therapy; CIMT-I, CIMT immediate; CIMT-D, CIMT delayed.
Table expresses change from time point 1 to 3 for CIMT-I (n = 83) and from time point 3 to 5 for CIMT-D (n = 62). Data shown are proportions and (totals).
When we examined overall changes prior to CIMT through 12 months thereafter, there remained a Group × Time interaction for lifting the can (task 9), with the CIMT-I group showing significant reacquisition of this task (see Table 3). Notably, among tasks that could be completed at baseline, lifting a can is one of the key WMFT items that predict improvement. 19
Regress Events
Regress events (loss of the ability to complete a task) were seen in each of the time periods. However, there were no significant differences between groups in regress events, as evaluated by a test of independent proportions.
Discussion
The change in the ability to complete a task that could previously not be achieved within the 120 s window can be considered a meaningful functional change. Thus, if a patient is unable to perform a task such as “stacking checkers” in 2 minutes (which can be performed by an unaffected person in less than 2 s), a profound functional deficit is present. Tracking changes in noncompleted WMFT items provides a measure of clinically relevant improvements in function, and unlike analysis of change scores among tasks that could be completed, 6 analysis of noncompleted items revealed differences in the groups’ improvement that were sustained for 12 months after treatment.
Efficacy of CIMT Training
During the 2 weeks of CIMT, the CIMT-I group displayed significant improvements (reacquisitions) in several tasks, whereas the CIMT-D group showed no significant within-group differences during their training period. There were significant differences between the 2 groups in lifting a pencil and total noncompletes, and differences in lifting the can trended toward significance (summarized in Table 4). This finding complements previous observations that earlier provision of CIMT results in a faster performance among tasks that could be completed prior to delivery of the intervention. 11 However, we cannot exclude the possibility that reacquisitions made during the intervening year reduced the CIMT-D group’s potential for improvement during CIMT training. During the year between randomization and provision of CIMT, participants in the CIMT-D group could receive non-CIMT therapies, and approximately 25% did. 11 By the start of their CIMT sessions, the CIMT-D group showed some improvement; there were differences between the CIMT-I group at time point 1 and the CIMT-D group at time point 3 (the time points immediately prior to CIMT training). 11 Thus, a floor effect may have contributed to the lack of significant improvements in the CIMT-D group during the 2 weeks of CIMT.
Summary of Significant Improvements in Ability to Complete WMFT Noncomplete Items (Reacquisitions) Over the Course of the Study.
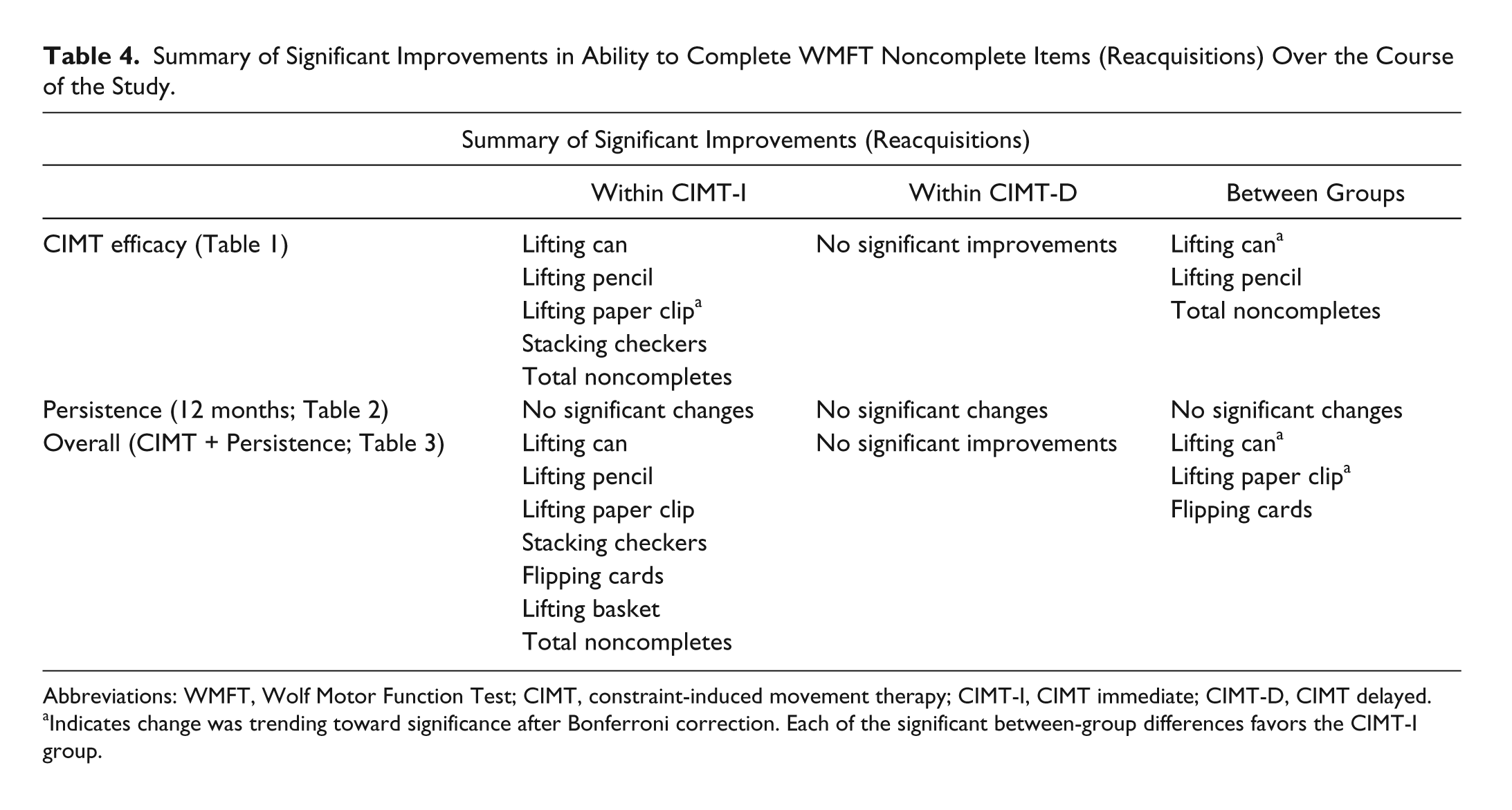
Abbreviations: WMFT, Wolf Motor Function Test; CIMT, constraint-induced movement therapy; CIMT-I, CIMT immediate; CIMT-D, CIMT delayed.
Indicates change was trending toward significance after Bonferroni correction. Each of the significant between-group differences favors the CIMT-I group.
Persistence of Gains Made During CIMT
During the year following CIMT training, neither the CIMT-I nor CIMT-D groups showed significant changes in their abilities to complete more WMFT items, nor were there substantive losses in ability to complete a task (regress events). These observations suggest that the gains made during CIMT training are enduring, likely because of the fact that regaining the ability to complete a WMFT task indicates that one can now complete—and thus practice—similar tasks in daily life. This situation would encourage participants to engage the limb more frequently in other tasks that require comparable skill.
However, there were a few instances of regress events in both groups, particularly in lifting a paper clip (4 and 3 regress events for the CIMT-I and CIMT-D groups, respectively) and stacking checkers (9 and 5 regress events for the CIMT-I and CIMT-D groups, respectively). When regress events were compared between groups, few differences were found. These regress events suggest that for some tasks, capacity to maintain these improvements might decline or that a task previously achievable was now unachievable 1 year after CIMT training. The extent to which these observations might be attributed to patient characteristics would require a larger sample of CIMT participants who demonstrate comparable changes.
Overall Change
Unlike the CIMT-D cohort, the CIMT-I group showed significant reacquisition of several tasks during the trial. This finding indicates that receiving CIMT earlier is more efficacious than receiving it a year later. Additionally, CIMT-mediated gains and increased task completions may form a basis for further improvements in functional ability through more frequent use of the impaired limb. Unfortunately, use of real-time, home-based measuring devices for limb use was beyond the scope of the EXCITE study. The increase in completed tasks from immediately post-CIMT to 12 months later, coupled with the Group × Time interaction favoring the CIMT-I group 12 months post-CIMT, support the notion of acquired impetus for further use when exposed to CIMT within 3 to 9 months poststroke. This further use phenomenon may also explain why some tasks, such as flipping cards and lifting a basket, show no significant improvement in the CIMT-I group during the 2 weeks of CIMT, yet show significant improvements over the course of the year (pre-CIMT to 12-month follow-up).
Nature of Task Improvements
Our findings indicate that early CIMT training confers clinically meaningful changes. It is interesting to note that the gains seen in the CIMT-I group are primarily in tasks using fine-motor skills and distal muscles, such as lifting a can, lifting a pencil, lifting a paper clip, stacking checkers, and flipping cards. This occurrence may be a result of several factors. First, these tasks have higher proportions of noncompletes (0.117-0.333) than most other tasks (0.000-0.086) immediately before CIMT training. 16 Thus, these tasks appear to offer a greater opportunity for improvement. Second, based on informal comments from therapists, more emphasis might have been placed on fine, distal movements rather than on arm-trunk kinematics or correcting for compensatory trunk motion. This compensation can hinder reacquisition of normal kinematics20,21 and might limit improvement in tasks using proximal muscles. Finally, therapists are often reluctant to promote repetitive motion at the shoulder joint because this location is often a source of existing or treatment-induced pain in stroke survivors. 22 This concern limits work on tasks using proximal muscles and therefore might contribute to fewer reacquisitions in these tasks. However, this precaution might have been unnecessary because CIMT was not found to exacerbate pain or fatigue when assessed at 1 EXCITE trial location. 23
Two of the fine-movement tasks—lifting a can and lifting a pencil—have been previously identified as 2 of 6 key WMFT tasks that both CIMT-I and CIMT-D participants could initially perform and for which substantive improvements were noted. These tasks help comprise the streamlined WMFT.19,24 Our findings are strengthened by the fact that CIMT-I participants showed significant improvement in their ability to reacquire these 2 WMFT tasks (lifting can and lifting pencil) that had previously been shown to be key indicators of improvement when they could be done initially. These improvements are quite robust, first being seen during CIMT training and then maintained at the 12-month reevaluation.
Improvements in motor function are likely a result of CIMT-dependent plasticity. Such plasticity has been manifested previously in CIMT studies among participants with comparable inclusion criteria. The improvements were seen as expansions in volume and shifting in center of gravity for transcranial magnetic stimulation maps governing thumb 25 and wrist movements. 26 In a similar study, CIMT was found to increase the transcranial magnetic stimulation motor map area relating to finger movement. 27 Functional magnetic resonance imaging data among EXCITE participants have also revealed increased activation within the ipsilesional cortex following CIMT. 28
As seen in Tables 1 to 3, the CIMT-I group experienced significant reacquisitions, whereas the CIMT-D group did not. One would presume that various therapies combined with any use of the limb by the CIMT-D group during the year preceding CIMT should reduce the number of noncompleted tasks to reacquire. However, this does not appear to be the case. Using 0.1 as a reasonable proportion threshold, the CIMT-D group had proportions of noncomplete tasks greater than 0.1 in 11 of 15 tasks (73.33%) immediately prior to CIMT training, whereas the CIMT-I group had proportions of noncompletes greater than 0.1 in 7 of 15 tasks (46.67%) prior to their CIMT. 16 Thus, further study is needed to understand what factors contributed to the lack of significant reacquisitions in the CIMT-D group.
Regress Events
There were no between-group differences in regress events in the 3 time periods examined in this study. In both groups, the greatest total number of regress events occurred in the year after CIMT training. However, this pattern was not always true for individual tasks. For both groups, the highest percentages (more than 5.0%) of regress events were seen in the reach and retrieve, lifting paper clip, stacking checkers, flipping cards, and turning a key in a lock tasks (data not shown). These tasks are particularly challenging, rated as some of the most difficult tasks in the WMFT. 29 This difficulty may have been manifest in some participants who might not have undertaken tasks that require kinematically comparable movements in their daily lives. On the other hand, many CIMT-I participants may have taken on the challenge embedded within these tasks, resulting in their significant reacquisition. Future investigations directed toward improvement in task performance should consider exploring the bases for these contrasting outcomes.
Limitations
Our findings would be improved by monitoring the specific nature and dosing of therapies received by the CIMT-D group before CIMT training. Although time-consuming, such an effort would provide insight into the gains attained prior to CIMT and the potential floor effect that may account for this group’s lack of significant task reacquisition. Additionally, following participants for a longer time would provide a better understanding of the long-term impact of early compared with later CIMT.
During training, trunk restraint would have limited compensatory strategies20,21 and reduced their influence on motor performance, thus providing a clearer understanding of participants’ functional abilities. Including kinematic data during task performance could have provided insight regarding participants’ movement strategies and movement quality. Other groups have analyzed the kinematics of movements and attribute the increased use of the paretic limb after CIMT to improved hand dexterity, increased attention to the paretic limb, improved speed, and better coordination between the shoulder and elbow. 30 In other studies, participants receiving CIMT showed better reaching strategies than a control group 31 and improved spatial and temporal efficiency. 32
Summary
Improvements in existing motor abilities are possible with both immediate and delayed receipt of CIMT, as reported previously. 11 However, significant reacquisition of the ability to complete tasks is only seen with early CIMT treatment (Table 4). Thus, while delivering CIMT to patients more than a year after their mild to moderate strokes is beneficial, prescribing CIMT at 3 to 9 months postinsult may be even more efficacious with regard to the recovery process.
Footnotes
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This work was funded in part by the National Center for Medical Rehabilitation within the National Institute of Child Health and Development and the National Institute of Neurological Diseases and Stroke (R01 HD 37606).