
Abstract
Background. Previous research using the streamlined Wolf Motor Function Test (SWMFT) has focused either on the 3- to 9-month period or on the >12-month period after stroke and lacked the information for those at 9 to 12 months. Whether SWMFT scores reflect motor deficit and recovery from early to late stages after stroke remains unclear. Objective. A retrospective study using the Functional Ability Scale (FAS) was conducted to evaluate whether all SWMFTs items measure the poststroke recovery of upper extremity (UE) motor function and if they could be used for patients within 9 to 12 months after a stroke. Methods. Rasch analysis was conducted, and data were drawn from patients 3 months to years after a stroke. Results. The continuum of UE motor function in SWMFT-FAS was supported. Subacute patients had the best motor function, followed by the 9- to 12-month group, and then chronic patients. Variation in UE motor function was large (2.35-2.72 logits), and motor abilities of these 3 groups overlapped. The 8 SWMFT items could target a broad range of UE motor function, from −8.28 to 7.80 logits. The average difficulty of these 8 items also matched the UE motor ability of the subgroup at 9 to 12 months after stroke, and individual versions of the SWMFT performed well to assess the motor ability of this group. Conclusions. The SWMFTs had sound hierarchical properties. The SWMFT-Chronic or the SWMFT-Subacute could be used to evaluate UE function of this subgroup at 9 to 12 months after stroke.
Stroke is one of the leading causes of disabilities and death during adulthood. 1 Approximately 50% of stroke survivors have some upper extremity (UE) dysfunction, 2 highlighting the need to study rehabilitation training for UE dysfunction. With the continuing emphasis on evidence-based practices in health care, evaluation of existing measures is critical, and knowing that assessment scores can place patients on a continuum from low to high functional status and reflect progress of patients during treatment has become increasingly pertinent.3,4
The Wolf Motor Function Test (WMFT) 5 is a widely used measure to assess UE motor function after stroke. This scale was developed initially to evaluate UE performance in chronic patients after stroke receiving forced use treatment of hemiplegic UE. The most current version of the scale includes 17 items, 6 comprising 15 function-based tasks and 2 strength-based tasks used to assess the time for completing individual tasks (termed WMFT-TIME), the quality of implementing each task, and strength. The present study focuses on the quality of performance on the WMFT only.
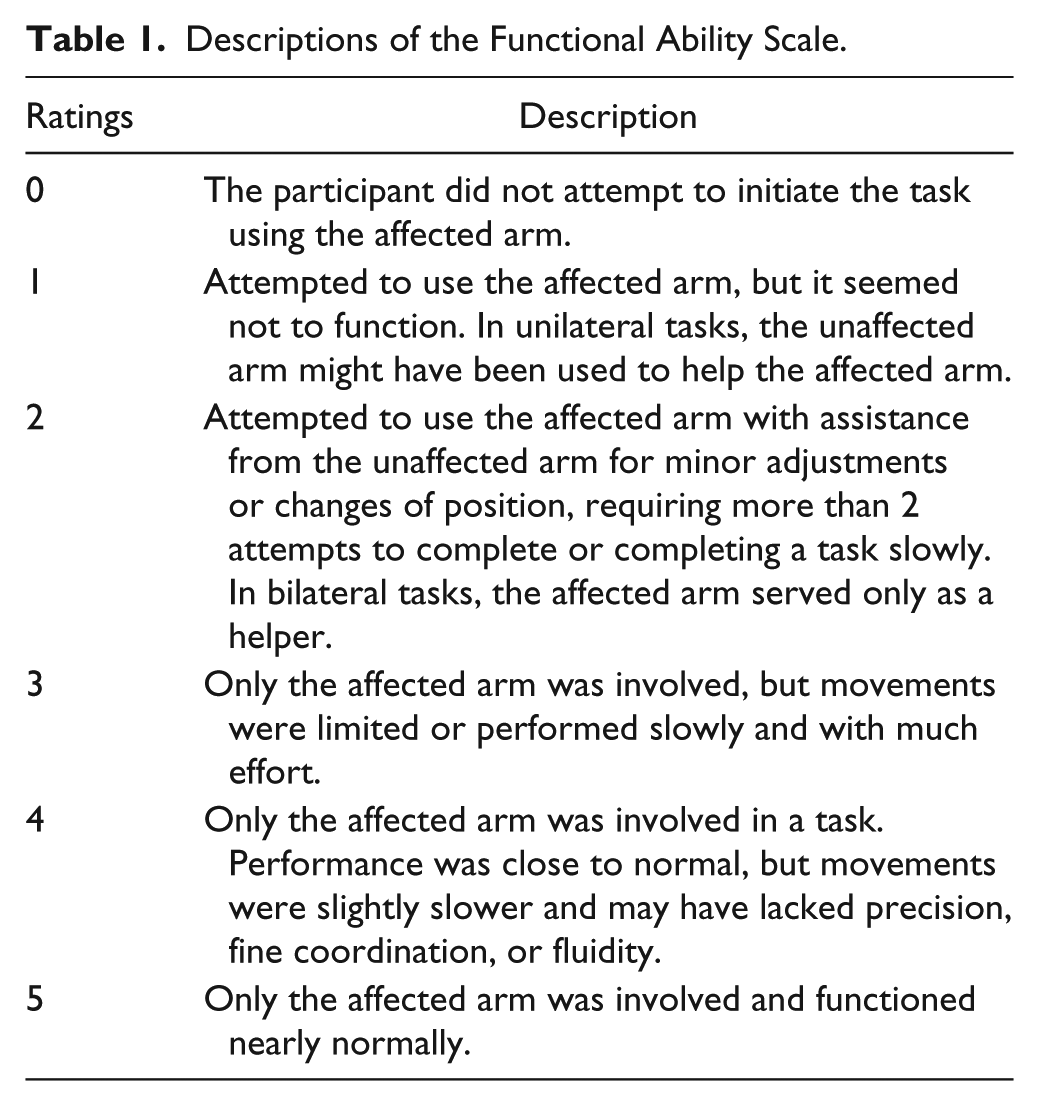
The WMFT–Functional Ability Scale (FAS) is specific for evaluating the quality of UE performance in each functional task. A 6-point rating scale is used in which 0 indicates “no attempt to use the affected arm” and 5 shows “movement of affected arm that appears to be normal.” (See Table 1 for detailed descriptions.) Research has recognized high interrater and test-retest reliability of the WMFT-FAS and high internal consistency.7-9 With regard to concurrent and predictive validity, the WMFT-FAS demonstrated a moderate to good relation with the Fugl-Meyer Assessment9,10 and was good to excellent with the UE subscale of the Stroke Rehabilitation Assessment of Movement. 9 Studies by Woodbury et al 11 and Wolf et al 6 further concluded that the WMFT-FAS could differentiate patients with higher UE motor function from those with lower function. Given the excellent reliability6-9 and validity,9-11 use of the WMFT-FAS has been extended to investigate the effectiveness of robotic therapy, 12 bilateral arm training, 13 and mirror therapy. 14
Descriptions of the Functional Ability Scale.
To reduce the burden of administration and provide the most pertinent information about recovery potential, Bogard et al 15 suggested 2 versions of a streamlined WMFT (SWMFT) for use with subacute and chronic patients. Data were drawn from 222 participants in the Extremity Constraint Induced Therapy Evaluation trial, and multiple regression methods were conducted to examine the relations between the WMFT-TIME and 3 covariates: functional level, sex, and concordance. Prominent tasks were selected according to whether changes in the patient’s performance were significantly related to overall improvement on the WMFT-TIME. One version was the SWMFT for subacute patients (SWMFT-S), which targeted patients within 3 to 9 months after a stroke. It measured 6 tasks: hand to table, hand to box, reach and retrieve, lift can to mouth, lift pencil from table, and fold towel. The other version was the SWMFT for chronic patients (SWMFT-C), targeting patients 12 months or more after a stroke. It consisted of 4 tasks identical to those in SWMFT-S (hand to box, lift can, lift pencil, and fold towel) and 2 additional tasks of “extend elbow weight” and “turn key in lock.” These tasks reflected improvement in motor function at different stages after a stroke and suggested the necessity of grouping WMFT tasks specific to different chronicity.
Two studies16,17 have empirically examined the psychometric and clinimetric properties of the SWMFTs. One study 17 conducted Rasch analysis to investigate construct validity and reliability of the SWMFT-S and SWMFT-C FAS in 2 groups of patients. This study supported the unidimensionality and high reliability (.90) for both versions of the scale. The hand-to-box and hand-to-table tasks in the SWMFT-S scale showed a high correlation of greater than .90, so removal of 1 of these 2 items was recommended. Overall, the SWMFT-S and SWMFT-C were found to be good tools to understand UE motor function in different subgroups of patients after stroke.
Wu et al 16 investigated responsiveness and criterion-related validity of the SWMFT-S (TIME scale) in subacute stroke patients with onset of 3 to 9 months. Performance time on individual tasks was used to estimate responsiveness and relationships with criteria measures. They suggested that the responsiveness of the SWMFT-S was comparable to the original performance time scale of the WMFT. The SWMFT-S also demonstrated good concurrent validity and even better predictive validity than the WMFT, and the study concluded that the SWMFT improved clinical utility.
These 2 studies focused on changes and improvement in specific subgroups of stroke patients and examined the use of the SWMFT-S or SWMFT-C in subacute or chronic patient groups, respectively. To date, no studies have examined whether the SWMFT-S or SWMFT-C can be used with patients at 9 to 12 months after a stroke.
Starting at the subacute stage, patients gain improvement in single-joint proximal reaching movements without object grasping, and at later stages, recovery occurs in multiple-joint proximal and distal movements for reaching to grasp functional objects.18-21 However, investigations on individual-onset groups (onsets of 3-9 months and of more than 12 months) and the lack of information on those at 9 to 12 months after a stroke do not provide strong support that the SWMFTs matches theoretical expectations of motor deficit and recovery. Although the original WMFT was consistent with motor theories, the streamlined versions of WMFT might lose important aspects because of removal of items and fail to capture UE long-term recovery after stroke.
The purpose of the current study was to extend previous findings and fill this gap in knowledge about the SWMFT. The study proposed using samples from patients at a broad range of onset after stroke and combining scores on individual SWMFT tasks to examine if the SWMFT-FAS can quantify UE motor recovery from the subacute to chronic stages. In addition, the study examined if the FAS scores of the SWMFTs could be used to detect UE performance of patients at 9 to 12 months after a stroke. The overall aim of this study was to (a) evaluate the construct of the combined SWMFT-FAS and (b) determine which items work better to assess UE motor function in the subgroup of patients at 9 to 12 months after a stroke. Specifically, the study addressed the following questions:
Do SWMFT items work together to measure the continuum of UE motor function from 3 months to years after a stroke?
Do all items function as expected?
Does the sample in the current study provide a wide enough range of UE motor function to evaluate recovery from stroke in patients in stages from subacute to chronic?
Does the item-difficulty hierarchy match clinical knowledge about progress after stroke?
Is the SWMFT-FAS able to evaluate UE motor function from low to high in the 9- to 12-months poststroke group?
Method
Participants
Data were drawn from 351 participants enrolled in ongoing investigations of poststroke motor rehabilitation between 2010 and 2012. The study recruited participants from 6 hospitals in Taiwan, and each received one of the following treatments: conventional rehabilitation, bilateral arm training, distributed constraint-induced therapy, robot-assisted therapy, or mirror therapy. Inclusion criteria included (a) a score of Brunnstrom stage II or above for the proximal and distal parts of the affected upper limb 22 ; (b) a score of 18 or higher on the Mini-Mental State Examination 23 ; (c) first-ever stroke; and (d) no major medical problems, such as severe aphasia, a vision problem, or poor physical condition, which were diagnosed by physicians. The human ethics committees at all participating sites approved the study, and all participants provided informed consent.
Procedures
Five independent, certified occupational therapists evaluated volunteer participants’ cognitive and motor function to screen for eligibility. The 5 independent evaluators attended intensive training courses provided by the senior investigators and passed a demonstration and written tests. All evaluators and principal investigators met regularly for quality assurance of the administration and evaluations. The full 17-item WMFT was administered, and all participants were asked to execute all tasks using the affected arm. If necessary, participants were allowed to perform the task with the help of the unaffected arm.
Eligible participants were assigned randomly to different treatment groups to receive 90-minute treatments 3 days a week for 3 or 4 weeks. Treatments were provided by 6 certified occupational therapists who had received comprehensive training for administering intervention protocols. After treatment, evaluators blinded to treatment groups rated participants’ performances again. All treatments and assessments were administered at the individual study sites.
Outcome Measure
The SWMFT-S and SWMFT-C include 4 identical items and 2 items specific to each version, yielding 8 SWMFT items. The current study analyzed the SWMFT-FAS scores before treatment. Table 1 lists details of the FAS.
Data Analysis
Responses to the 8 SWMFT items were selected to investigate the continuum of UE motor function in subgroups of 3 to 9 months (subacute), 9 to 12 months, and more than 12 months (chronic) after stroke and to determine which items best assessed UE motor ability in the 9- to 12-month poststroke group. The current study used the Rasch rating scale model in Winsteps 3.75.0 software 24 to examine the test structure of the 8 chosen items (such as unidimensionality and the item-difficulty hierarchy) and the relationship between item difficulty and motor function in the 3 groups.
The Rasch model 25 was developed to transform binary, categorical, and ordinal data to interval data (termed as logits). Item difficulty and individual ability are calibrated on the same ruler (logit units) for further comparisons. A logit is a unit of measurement reporting relative differences between item difficulty and person ability estimates. A fundamental assumption of the Rasch model is that all items reflect a single underlying construct (termed unidimensionality). Principal components analysis (PCA) of the residuals and item fit are used to examine against the assumption. An ideal instrument is assumed to have variances explained by the first dimension that exceeds 50%, 26 and all items have mean squares (MnSq) and standardized z (Zstd) scores in an acceptable range. 27 Values of MnSq indicate the size of the deviation from the expected difficulty predicted by the Rasch model (misfit) and are summarized into 2 types of unexpected responses: responses close to an item’s difficulty (infit) and responses far away from an item’s difficulty (outfit). 28 The Zstd is the standardized value of the MnSq for indicating the statistical significance of the misfit. The ideal value of MnSq is 1. An item that has an MnSq outside the acceptable range of 0.5 to 1.5 and a Zstd beyond the range of −2.0 to 2.0 is considered a misfit item.26,29 An item with an MnSq higher than 2.0 would be removed because it could degrade the whole measurement.26,29
Rasch analysis simultaneously estimates difficulty of items and individuals’ UE motor functions, and the item-person map describes the relationship between the two. 28 Items on the left side are ordered from the easiest at the bottom to the most difficult at the top. On the right side, the more capable participants are located at the top and the less capable at the bottom. For rating scale data, each item has a difficulty estimate and a series of thresholds (often termed Rasch-Andrich thresholds) at which the likelihood of obtaining a given score (below the threshold) is exceeded by the likelihood of receiving the next higher score (above the threshold). 28 An ideal instrument should have item response thresholds that cover a similar range as the person ability distribution. 30 The item-person map is also used to indicate which items target UE motor function of specific patient groups and provide suggestions for use of the SWMFTs in patients 9 to 12 months after a stroke.
Results
Preliminary Analysis
Participants were divided into 3 groups by stroke onset: subacute, 94 participants; 9 to 12 months poststoke, 58; and chronic, 199. These 3 subgroups had similar backgrounds (Table 2). The chronic group had an older average age (54.85 years; standard deviation [SD], 11.23) than the other 2 groups. The average Mini-Mental State Examination scores for 3 groups ranged from 27.40 to 27.90 (SD, 2.10-2.92), and the average years of education were almost equivalent across the 3 groups (range, 10.37-10.53 years; SD, 3.30-4.25). Most participants in each group were men (67.3% to 77.7%), and the subacute group had a smaller proportion of women (22.3%) than the other 2 groups (27.6% to 32.7%).
Demographic Information of the 3 Onset Groups.
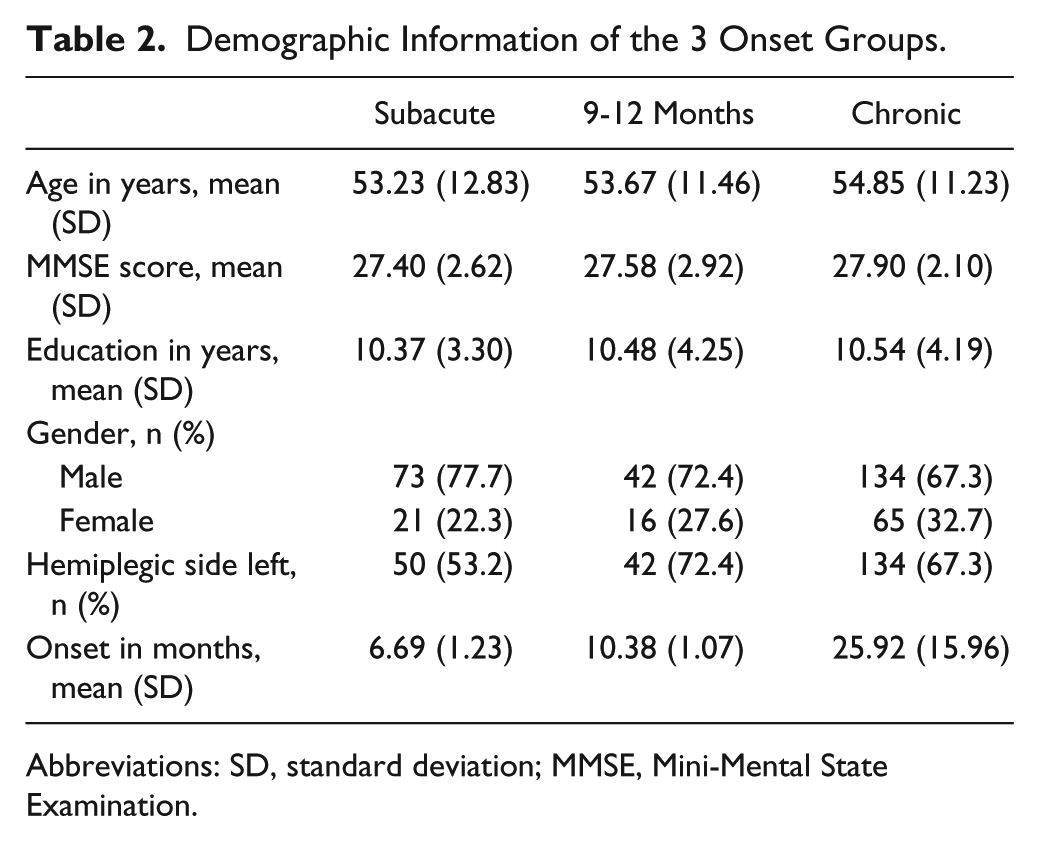
Abbreviations: SD, standard deviation; MMSE, Mini-Mental State Examination.
Unidimensionality
Results from the PCA of residuals showed that the Rasch model explained 72.2% of the variance. All but one item had infit or outfit MnSq values within the acceptable range. The reach-and-retrieve task had a slightly higher outfit MnSq value, 1.54, at a significance level of .05, but did not reach the removal criterion of +2. Thus, the assumption of unidimensionality held in the SWMFTs, and all of the SWMFT items functioned properly.
Upper Extremity Motor Function and Item Difficulty
Figure 1 is the item-person map, which shows item difficulty estimates and person ability estimates for the 351 participants by group. Variations in UE motor function among the 3 groups were large, and the groups overlapped. Figure 1 shows that the study sample had a broad range of UE motor function, thus providing enough information to evaluate recovery at stages from subacute through chronic.
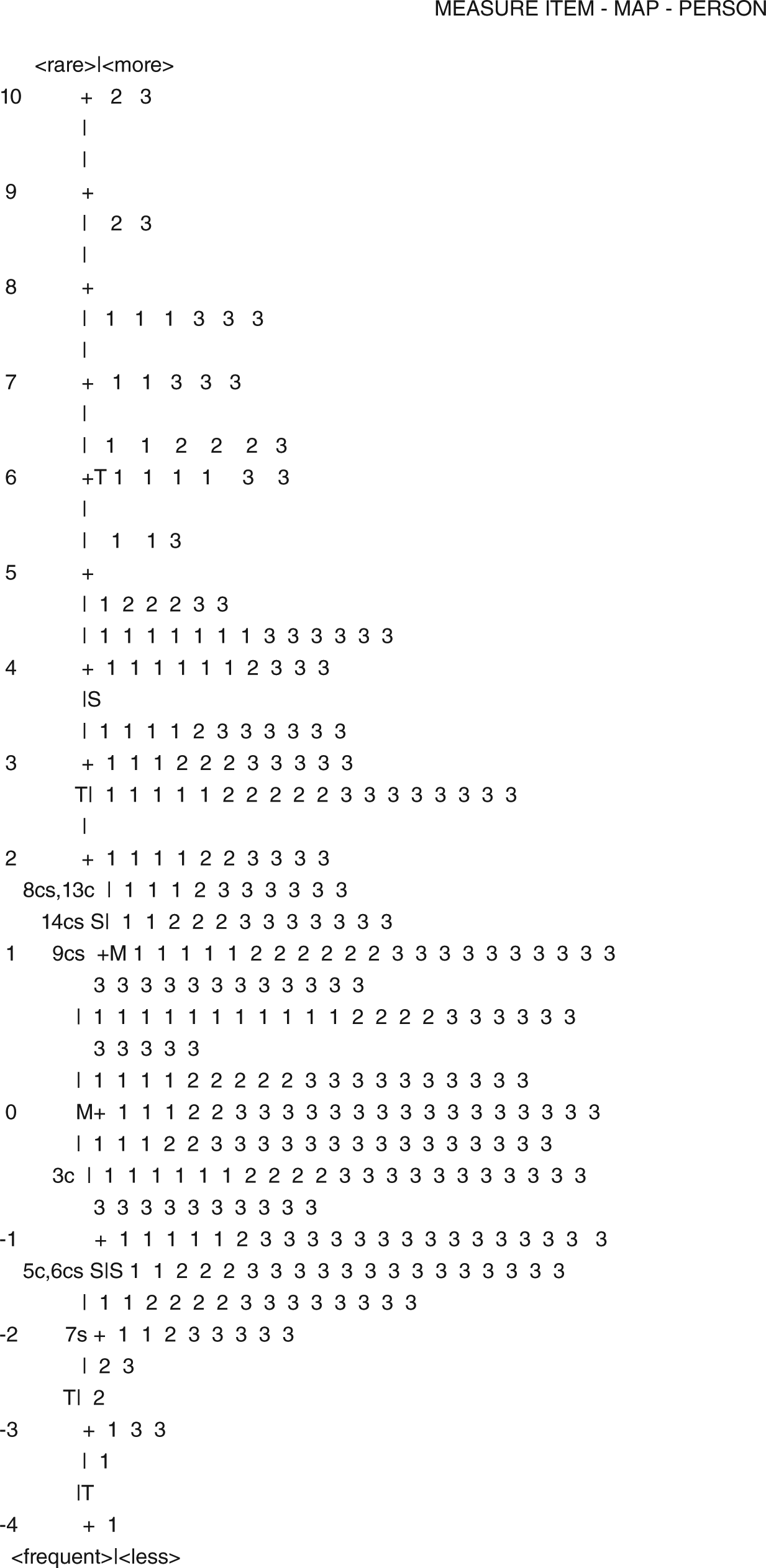
The item-person map.
Table 3 shows that the most difficult task was turn key in lock, followed by lift can to mouth. The easiest task was reach and retrieve, followed by hand to table. The average difficulty of SWMFT items covered the lowest and highest UE motor function, from −1.49 to 1.59 logits. With the use of a 6-point scale, the overall item difficulty covered a substantial range of the targeted construct, from a low of −8.28 logits to a high of 7.80 logits (Table 2). The 8 chosen items worked appropriately to reflect recovery of UE motor function after stroke in those from early to late stages. Scores on the items indicated progress in UE motor function in patients as early as 3 months after a stroke.
Estimated Item Difficulties of the Streamlined Wolf Motor Function Test for Subacute and Chronic Patients.
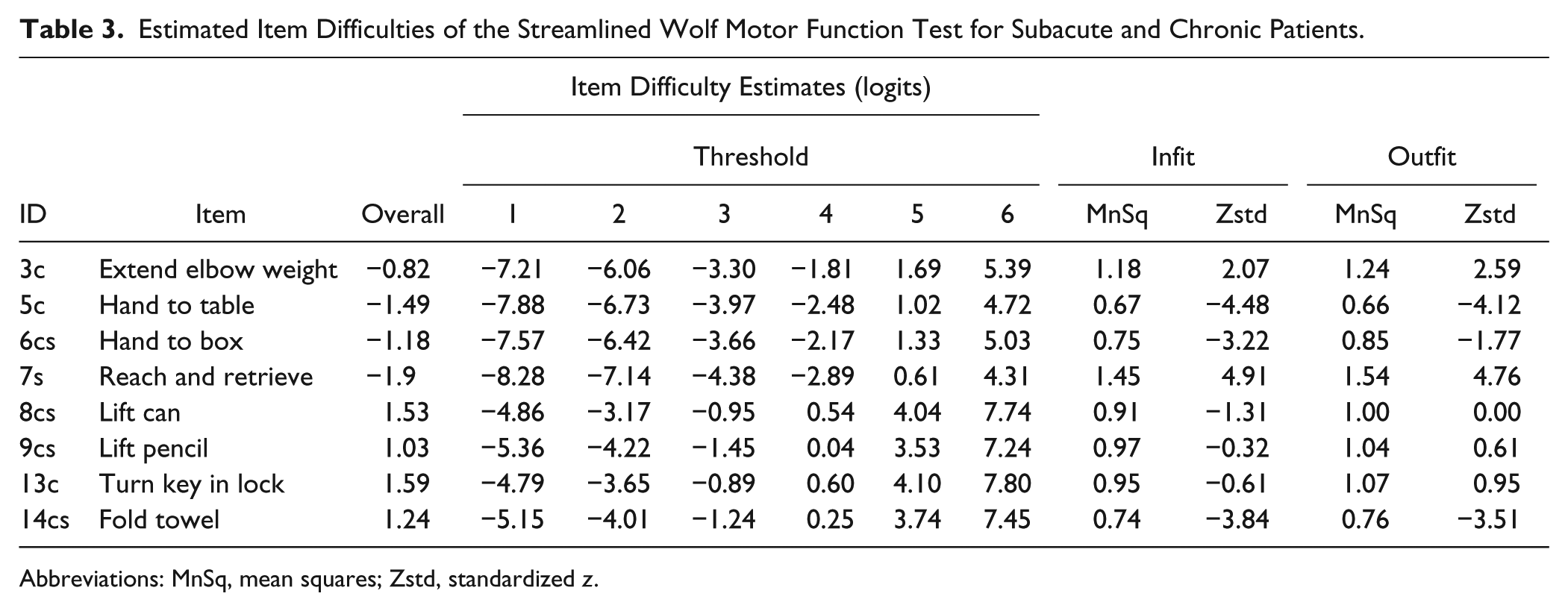
Abbreviations: MnSq, mean squares; Zstd, standardized z.
The study found 2 participants who were the most capable. They obtained full scores on all 8 items, and the estimated UE motor function was 10.17 logits. One participant was from the 9- to 12-month poststroke group, and the other was from the chronic group. One individual from the subacute group was the least capable, with an estimated UE motor ability of −4.06 logits. The mean UE motor function for the entire group was 1.11 logits (standard error [SE], 2.47). The subacute group showed the best UE motor function, with a mean of 1.85 logits (SE, 2.72), followed by the 9- to 12-month group, with 1.33 logits (SE, 2.68). The chronic group had the lowest value, at 0.78 logits (SE, 2.38).
The 9- to 12-Month Poststroke Group
Figure 1 shows that most of the participants in the 9- to 12-month poststroke group had mild to moderate UE motor function, ranging between −2.0 and 3.0 logits. The corresponding range of items includes all 8 items, which means that all SWMFT items targeted the UE motor function of this group well. Further investigation showed that both versions had test reliability higher than .90, and the distribution of item difficulty covered a substantial range of UE motor function in the 9- to 12-month poststroke group. The SWMFT-S or the SWMFT-C could be used in this group.
Discussion
This study extended knowledge of use of the SWMFT-S and SWMFT-C in subacute and chronic patients to examine if the SWMFT-FAS could be used to evaluate long-term progress from 3 months to years after a stroke. The sample included a wide range of patients from the subacute through the chronic stages who had a wide range of UE motor function. Responses to the 8 items before treatment were evaluated using Rasch analysis. Findings revealed that the combined SWMFT-FAS was unidimensional and covered a substantial range of UE motor function to target UE motor abilities of patients in stages from subacute through chronic. SWMFT-S and SWMFT-C items were both appropriate for the UE motor function of the 9- to 12-month poststroke group and could be used to place patients along a continuum from low to high function.
The SWMFT-FAS is an observational tool designed for clinicians to evaluate the performance quality of UE motor function after stroke and assess changes or improvement after treatment. It is always beneficial to use samples that include those in different stages of recovery and a wide range of UE motor function and to examine if the tasks work as expected when performed by those with different levels of ability.
This retrospective study was the first attempt to use data from individuals in early and late poststroke stages to evaluate if ratings on the SWMFT-FAS items reflect increased quality of UE motor function. As Figure 1 shows, participants were quite evenly distributed along the linear logit measurement scale, and no cluster was observed anywhere on the map. The wide range of UE motor function exhibited in the sample provided abundant information with which to evaluate recovery of UE motor ability after a stroke.
Unidimensionality
The PCA result supported the unidimensionality of the SWMFT, implying that all items functioned appropriately to measure the continuum of UE motor ability from 3 months to years after a stroke. Item fit statistics indicated that all but 1 item, reach and retrieve, had acceptable fit. The outfit MnSq value of this misfit item was slightly higher than the acceptable maximum of 1.5 but did not reach the cutoff of 2 to be removed from the test.26,29 The study concluded that all SWMFT items worked consistently to measure the performance of UE motor ability in patients in stages from subacute to chronic. This important finding confirmed the clinical utility of the SWMFT and provided an encouraging starting point for measuring changes or improvement after a stroke.
Upper Extremity Motor Function and Item Difficulty
The Rasch-derived item-difficulty hierarchy was consistent with original expectations for WMFT items and consistent with motor theories. The original expectations of the WMFT items were that tasks requiring control of primarily a single joint were rated as less difficult than those requiring control and coordination of multiple joints.5,11 The current study found that the hand-to-table and hand-to-box tasks were easier and that the turn-key-in-lock task was difficult. The study findings also validated the motor control literature, which says that task difficulty increases with the amount of accuracy required, the amount of precision required, and the number of performance steps (such as fold towel and turn key in lock). 11 The item-difficulty hierarchy of the SWMFT matched clinical knowledge about the progress from 3 months to years after a stroke.18-21
The 9- to 12-Month Poststroke Group
Rasch analysis and item difficulty use the same metrics to calibrate participants’ UE motor function, and the item-person map illuminates the relationship between individual UE motor ability and item difficulty. It becomes possible to use corresponding logits to match individual ability to specific items. Nearly 70% of participants in the 9- to 12-month poststroke group had moderate UE motor function (−2 to 3 logits), and the ranges of average item difficulty of the SWMFT-S and SWMFT-C were matched to this group. In addition, further examination of the 2 versions suggested that they worked well to measure the UE motor function in this group. The SWMFT-S or SWMFT-C, as well as the combined version, could be used to differentiate patients with low and high function in the 9- to 12-month poststroke group.
The reach-and-retrieve task showed slightly problematic item fit, a noteworthy finding that coincides with the findings of Woodbury et al, 11 who documented that subacute patients earned a rating of 0 for this item but not for any other WMFT items. In their data set, 43% of responses to this item were missing at baseline, primarily because of incorrect weight start position and incorrect participant start position. However, no problematic ratings for or missing responses to this item were found when the current study data were reexamined. Further investigation is needed to confirm whether this item works efficiently to measure UE motor function after a stroke.
Another limitation results from the very specific inclusion rules used for the current study. Most participants had mild to moderate UE dysfunction and did not have severe UE dysfunction or cognitive problems. Also, patients who had had more than 1 stroke were excluded. These restrictions on inclusion in the study might limit the generalizability of its conclusions.
Last, unequal sample sizes of the 3 groups might limit the conclusions regarding group comparisons. The chronic group sample size was 2 times that of the subacute group and nearly 3.5 times that of the 9- to 12-month group. Patients with moderate or severe UE motor dysfunction at the subacute or acute stages are usually in an unstable medical condition and not willing to participate in stroke rehabilitation research. Patients at the chronic stage, even though with severe motor dysfunction, are in stable condition in terms of physical ability and persistence and are more willing to attend the research training to improve their daily function. As a result, samples at the chronic stage showed worse UE motor function, with evidence of lower WMFT scores and logit scores, than the subacute group. Future studies should recruit patients with severe UE dysfunction and include equal sample sizes across all groups to validate the findings of the current study.
Conclusions
The SWMFT is a useful assessment to evaluate recovery progress in early through late stages after a stroke. SWMFT items maintained the unidimensional structure of the original WMFT, and the item-difficulty hierarchy matched the original item expectations of the WMFT and of motor recovery theories. The SWMFT-S and SWMFT-C, as well as the combined test, enable measurement of UE motor function in patients at 9 to 12 months after a stroke. Further research is needed to investigate the reach-and-retrieve task and to validate findings in patients with severe UE dysfunction, more cognitive impairment, and those with multiple strokes.
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This project was supported in part by the National Health Research Institutes (Grant Nos. NHRI-EX101-9920PI and NHRI-EX101-10010PI), the National Science Council (Grant Nos. NSC-102-2314-B-182-001 and NSC-100-2314-B-002-008-MY3), and Chang Gung Memorial Hospital (Grant No. CMRPD1C0401) in Taiwan.