
Abstract
Background. Arm nonuse, defined as the difference between what the individual can do when constrained to use the paretic arm and what the individual does when given a free choice to use either arm, has not yet been quantified in individuals poststroke. Objectives. (1) To quantify nonuse poststroke and (2) to develop and test a novel, simple, objective, reliable, and valid instrument, the Bilateral Arm Reaching Test (BART), to quantify arm use and nonuse poststroke. Methods. First, we quantify nonuse with the Quality of Movement (QOM) subscale of the Actual Amount of Use Test (AAUT) by subtracting the AAUT QOM score in the spontaneous use condition from the AAUT QOM score in a subsequent constrained use condition. Second, we quantify arm use and nonuse with BART by comparing reaching performance to visual targets projected over a 2D horizontal hemi–work space in a spontaneous-use condition (in which participants are free to use either arm at each trial) with reaching performance in a constrained-use condition. Results. All participants (N = 24) with chronic stroke and with mild to moderate impairment exhibited nonuse with the AAUT QOM. Nonuse with BART had excellent test-retest reliability and good external validity. Conclusions. BART is the first instrument that can be used repeatedly and practically in the clinic to quantify the effects of neurorehabilitation on arm use and nonuse and in the laboratory for advancing theoretical knowledge about the recovery of arm use and the development of nonuse and “learned nonuse” after stroke.
Introduction
Most individuals with upper-extremity disability resulting from a stroke face difficulties in effectively using their paretic arm and hand in daily activities, resulting in significantly reduced quality of life.1-3 Such nonuse has been defined as the difference between what the individual can do when constrained to use the paretic arm and what the individual does when given a free choice to use either arm. 4 Nonuse in individuals with hemiparetic stroke (or with other predominantly unilateral motor neurological disorders) can arise from a number of factors such as pain, limited range of motion, and the higher effort and attention required for successful use of the impaired hand. 5 Nonuse has furthermore been hypothesized to have a learned component.6-9 According to this learned nonuse hypothesis, nonuse would develop either after unsuccessful repeated attempts to use the affected arm and hand or after negative consequences resulting from paretic limb use (such as spilling hot coffee or dropping an object).
Despite the high clinical and scientific significance of nonuse, it is unclear how to directly quantify nonuse in individuals poststroke. Sterr et al. 8 studied nonuse in brain-injured adolescents with the Quality of Movement subscale of the Motor Activity Log test (MAL QOM) 10 and the Amount of Movement subscale of the Actual Amount of Use Test (AAUT AOU).8,11 Nonuse was estimated by the difference between the actual test score and the score obtained when the participants actually perform the tests with the affected hand.
Neither the MAL QOM or the AAUT AOU fulfills the 5 criteria for an ideal measurement tool in neurological rehabilitation 12 however—namely, simplicity, objectiveness, test-retest reliability, external validity, and sensitivity. First, both the MAL and the AAUT require adequate training of the tester by experienced therapists. Second, the MAL relies on subjective participants’ ratings of the amount of use and QOM of their more affected arm in daily activities. Third, to preserve validity, the modified AAUT cannot be administered repeatedly, and as such, it may lack good test-retest reliability. Fourth, the AAUT AOU has low scoring resolution. 13 In light of these limitations and in order to advance both theoretical and practical knowledge about recovery of arm use after stroke, tools that use objective activity monitoring are needed. 13
The goal of the present study is 3-fold. First, we investigate the existence of nonuse in participants with chronic stroke, as measured with the AAUT QOM. Second, we propose a novel, simple, and quick-to-administer laboratory-based measurement tool, the Bilateral Arm Reaching Test (BART), to quantify paretic arm use and nonuse objectively and repeatedly. Third, we investigate whether measurement of arm nonuse with BART in participants with chronic stroke is reliable in test-retest and whether it exhibits external validity when compared with nonuse as estimated with the AAUT QOM.
Methods
Participants
A total of 24 participants with chronic stroke (18 male, 6 female) were enrolled in this study. The inclusion criteria were as follows: (1) Mini-Mental State Examination score > 25/30, (2) at least 6 months poststroke, (3) no pain in the paretic arm and hand, (4) right-hand dominant prestroke, and (5) the ability to reach a target displayed at 30 cm anterior to the midline trunk; for the validity study, an additional criterion was (6) no visual neglect, as measured by the ability to cross all the lines in both left and right work spaces in Albert’s test. 14 Prestroke hand dominance was self-reported.
The upper-extremity score of the Fugl-Meyer test (FM-UE) 15 was administered to all participants poststroke by 4 different testers, all physical therapists with more than 2 years of clinical experience. In addition, 10 nondisabled (4 male, 6 female), right-handed (according to Edinburgh Handedness Inventory), 16 age-matched participants were recruited (age of participants poststroke ± standard error [SE]: 62.25 ± 2.64 years; age of nondisabled participants: 58.10 ± 3.76 years; t test: P = .390). Note that participants in the latter group were not recruited to serve as controls but to compute a normative hand use value (see below and appendix, Figure A.1).
To test BART test-retest reliability, 19 participants with stroke performed 3 test sessions at least 4 days apart. To assess BART validity, 15 participants with stroke performed 2 test sessions at least 4 days apart. Validity was assessed with BART data from the second test session. Note that 5 participants were only enrolled to assess validity and, therefore, just performed 2 test sessions. Also, 10 participants participated in both reliability and validity and thus performed 3 sessions. The study was approved by the institutional review board of the University of Southern California, and all participants read and signed a written informed consent form prior to study enrollment.
Actual Amount of Use Test
The AAUT was administered to the 15 participants poststroke enrolled in the validity study first in the spontaneous use condition and then in the constrained use condition, as in Sterr et al. 8 We analyzed only the first 14 items of the original 17-item AAUT because the last 3 items are related to general activities such as gesturing and posture. The AAUT was administered by 3 experimenters and rated by 1 evaluator, a physical therapist with more than 2 years of clinical experience. We used the AAUT QOM instead of the AAUT AOU to test the external validity of BART for 2 reasons. First, the constrained use condition AAUT (cAAUT) AOU scores in Sterr et al. were close to maximum for most participants. Second, we recently showed greater variability and insensitivity to treatment effect for the AAUT AOU compared with the AAUT QOM. 13
The AAUT QOM scores in the spontaneous use condition, sAAUT, and in the constrained use condition, cAAUT, were calculated and expressed as average scores, from 0 to 5. Nonuse was computed as nuAAUT = cAAUT − sAAUT.
Bilateral Arm Reaching Test
Apparatus
Because target distance and location largely influence arm choice in pointing movements,16,17 BART displayed 1 of 100 targets at each trial in pseudorandom order on a 2D hemi–work space. Targets were white disks 2 cm in diameter projected on the table from an overhead projector with a preset target presentation schedule. Targets were displayed on 6 arcs, all ranging between 10° and 170° (0° is on axis and is parallel to the body, to the right). Arc radii ranged from 10 to 30 cm, with equal 4-cm distances between arcs. The targets were placed every 10° along the arcs. The leftmost and rightmost targets in the upper corners were not presented, making a total of 100 targets ([6 arcs × 17 positions per arc] − 2 targets). Two Mini-Bird model 500 (5-mm) magnetic sensors (Ascension Technology Corporation) were positioned on the tip of the index finger of each hand to measure finger motion and arm choice (sampling 100 Hz).
Testing procedure
Participants were seated with a seat belt to limit upper-body movement. 17 The position of the chair was adjusted to ensure that participants could comfortably reach to the end of the work space without bending their trunks. The participants were instructed to place both index fingers on the home position (a green disk of 2 cm in diameter), as shown in Figure 1.
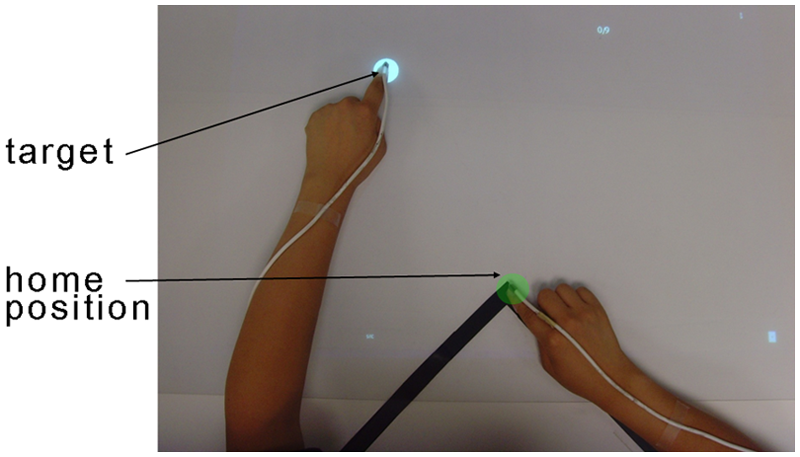
Measuring arm use with the Bilateral Arm Reaching Test: the home position is identified by the green circle and a target by the white circle. For each trial, participants were instructed to reach to the target with their choice of hand using the index finger as quickly and accurately as possible. Magnetic sensors were attached to the tips of index fingers to record choice of hand and performance
In both spontaneous and constrained use conditions, after a target was presented, participants were instructed to reach the target as quickly and as accurately as possible, to remain in contact with the target until it disappeared, and to return to the home position. After the start position was maintained for 1 s, the home target disappeared, and a target appeared at 1 of 100 locations. The intertrial interval was 3 s. A successful trial was defined as when participants reached the target within 1.2 s. A pleasant sound was played following successful trials; an unpleasant sound was played following unsuccessful trials. Dragging the arm along the table surface was instructed to be inappropriate and was discouraged whenever observed by the experimenter.
In the spontaneous use condition, participants were instructed to use either hand to reach each successively displayed target. Targets appeared twice at each position in pseudorandom order, resulting in 200 trials. Participants were reminded that there was no right or wrong answer in their choice of arm but were instructed to maximize the number of successful trials. In the constrained use condition, participants poststroke were instructed to reach each target with the index finger of the paretic arm. Targets appeared once at each position in a pseudorandom order, resulting in 100 trials. Note that nondisabled participants only performed the spontaneous condition because we noticed in our beta version that all nondisabled individuals could reach all targets in the hemi–work space within 1.2 s (and thus obtain a maximum score in the constrained condition).
BART-Dependent Measures
Overview
By definition, nonuse is computed by subtracting what poststroke participants do from what they can do. In BART, direct subtraction of successful movements made by the paretic arm in the spontaneous condition from those made in the constrained condition would not work, however, for the following reason. Nondisabled participants can reach targets in both left and right work spaces with their dominant right hand within 1.2 s with no failures. However, when given a choice, they use their right hand for the right work space and their left hand for the left work space. Computation of nonuse by simple subtraction of the “spontaneous reach area” from the “constrained area” would yield large nonuse for nondisabled participants, which is not appropriate. We therefore assumed that the average nondisabled participant has zero nonuse. To compute nonuse, we computed average nondisabled participant hand use in the spontaneous BART condition and used this normative hand use as a mask to the performance data of the participant poststroke. In this way, when paretic arm use in the spontaneous condition is equal to the normative hand use, there is zero nonuse. When arm use in the spontaneous condition is less than the normative hand use, there is positive nonuse.
Spontaneous use (sBART)
To compute arm use in participants poststroke, we quantified the successful trials made by the affected arm (for age-matched controls, we quantified the successful trials made by the dominant arm). For each target, we computed the probability of successful reach with the paretic arm: Pfree(success, handChoice = affectedArm| target). A second-order logistic regression model interpolated and smoothed these probabilities to obtain a probabilistic use map over the 2D work space. The logistic regression model has an extended input feature space, [x2, y2, xy, x, y, 1], where x and y are the coordinates of the 2D work space. The choice was established based on our data showing that the indifference line (ie, line of 50% choice probability) can be very curved in participants poststroke (eg, Figure 2D); a simple first-order logistic regression model cannot account for such curvature. sBART was then computed by integrating the volume beneath the probability surface given by the logistic regression model of use, using a 1000 × 1000 grid over the work space.

Computing nonuse with BART in 1 session over the 2D reaching work space for right-affected poststroke participant, ID2, in session 3: A. Constrained use (performance) probability for ID2. B. Average spontaneous use probability for right-handed nondisabled participants (normative hand use). C. Constrained use (performance) probability after masking with normative hand use of panel (B) poststroke. D. Spontaneous use probability. E. Nonuse probability for ID2. Color coding: red = 100% use of the paretic arm (right arm for healthy controls), blue = 0% use of the paretic arm. The indifference line, indicated by the thick black line, corresponds to the 50% decision boundary. Note that the nonuse probability map in (E) is solely for illustrative purposes; it was obtained by subtracting, for each target, the probability of successful reach with the affected arm in the spontaneous condition from the probability of successful reach with the affected arm in the constraint condition
Performance after masking (cBART)
We first defined the probability of reaching each target successfully with the affected arm (see Figure 2 for steps of the computation):

where Pconst (success | target) was computed from a second-order logistic regression model (as above) with the successful trial data in the constrained use condition (Figure 2A) and Pfree_healthy(handChoice=affectedArm | target) was computed from a logistic regression model with the successful trial data from the spontaneous condition for nondisabled age-matched controls (normative data, see Figure 2B). cBART was then computed by integrating the volume beneath the probability surface given by (Figure 2C) PPerf(success, handChoice = affectedArm|target).
Nonuse (nuBART)
Finally, nuBART was computed by subtracting sBART from cBART and taking possible negative values to 0, in line with the definition of nonuse and similarly to nonuse as estimated with the AAUT. Thus,

where the function |x|+ returns x if x > 0 and 0 otherwise.
Statistical Analyses
The number of trials per session in the spontaneous use condition (200) was determined from a sensitivity analysis of choice data: We increased the number of trials from 50 to 400, and observed that sBART converged between 150 trials and 200 trials for all participants (data not shown).
For each variable, sBART, cBART, and nuBART, we performed test-retest reliability and external validity computations. Reliability was assessed with intraclass correlation coefficients (ICCs) for 3 sessions and with Pearson or Spearman correlations for session-to-session measurements. External validity was tested with Pearson or Spearman correlations. External validity for sBART, cBART, and nuAAUT were tested by correlations with sAAUT, cAAUT, and nuAAUT, respectively. In addition, we tested for possible correlations between nuBART and months since stroke and age and tested the effect of the side of paresis.
For all analyses, the level of statistical significance was set at P < .05. When the data were not normal (as tested with the Shapiro-Wilk test), nonparametric statistics were used (as indicated in the results). Data analyses were performed using the SPSS 13.0 and MATLAB 7.5. All average results are reported as average ± SEs.
Results
Demographic and Stroke Characteristic Data
Table 1 summarizes the demographic data for the 24 participants poststroke. There was no difference in age between groups (62.25 ± 2.64 poststroke, 58.10 ± 3.76 controls; P = .390). In the stroke group, there was no difference between affected sides (P = .186). Time from stroke onset was 79.46 ± 12.19 months (range = 11-275 months). The FM-UE was 49.21 ± 2.18 (range = 22-63). The 15 participants in the validity study had a score of 0 on Albert’s test, indicating no neglect.
Demographic Data of the Stroke Group.
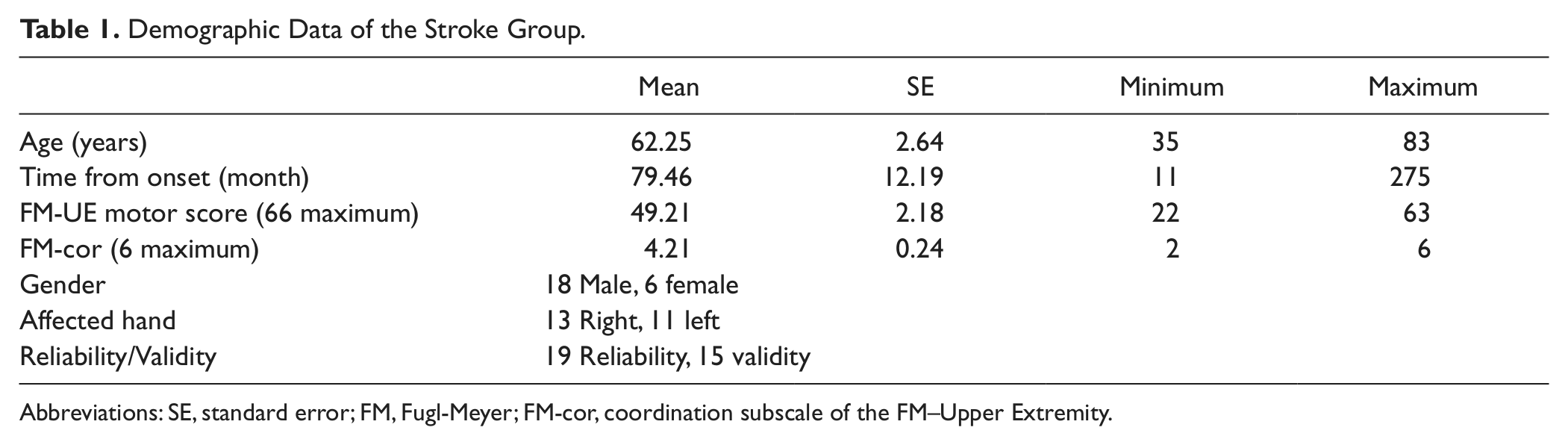
Abbreviations: SE, standard error; FM, Fugl-Meyer; FM-cor, coordination subscale of the FM–Upper Extremity.
Measuring Use, Performance, and Nonuse With the AAUT Test
For those 15 poststroke participants enrolled for the validity study, the sAAUT QOM was 1.50 ± 0.32 and cAAUT QOM was 3.17 ± 0.28. Nonuse nuAAUT was normally distributed (P = .209) and significantly greater than 0 (1.67 ± 0.18; P < .0001, 1-sample t test). Thus, all participants did exhibit some degree of nonuse overall, although the range of nonuse observed was large (range = 0.18-2.64; Figure 3).
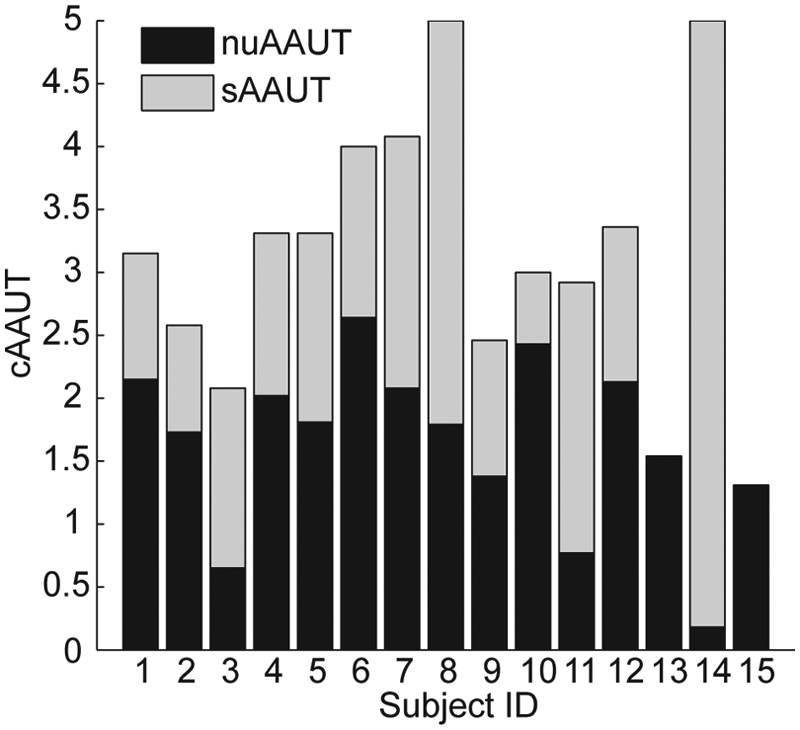
Arm use and nonuse in participants poststroke as estimated from AAUT QOM. The total height of each bar is cAAUT, the score in the constrained use condition. Because nuAAUT = cAAUT − sAAUT, cAAUT decomposes into sAAUT (gray), performance in the spontaneous use condition, and nuAAUT (black), estimated arm nonuse
The cAAUT correlated with FM-UE (r = 0.758; P = .001). nuAAUT did not correlate with the FM-UE, as expected (r = −0.136; P = .629); see appendix, Figure A.2. In addition, nuAAUT did not correlate with stroke duration (P > .5). There was no difference in nuAAUT between left- and right-hand paresis (P > .1, Mann-Whitney U test). There was a trend for a positive correlation between nuAAUT and age (r = 0.473 and P = .075, Pearson).
Measuring Use, Performance, and Nonuse With BART
Nondisabled participants
All nondisabled participants successfully reached all targets within the 1.2-s time constraint (Figure 2B). The mean indifference line was slightly shifted leftward of the midline. Consequently, mean sBART of nondisabled participants was greater than 0.5, with sBART = 0.60 ± 0.10, indicating a 10% handedness bias on average.
As discussed above, our results highly depend on our computation of the normative hand use. We therefore verified with a bootstrap analysis that arm choice showed little variability among the right-handed, nondisabled, age-matched participants (appendix, Figure A.1).
Participants poststroke
Figure 4 shows examples of use and nonuse probability maps (nonuse maps are shown for illustrative purpose only because nonuse was computed by subtracting sBART from cBART, in line with the definition and with nonuse as estimated with the AAUT) for 3 participants: a participant with little nonuse (ID10); a participant with large nonuse, albeit mild impairment (ID1); and a participant with moderate nonuse and impairment (ID3). In participants with low sBART values, the indifference line was not often straight and could form an island instead of a straight boundary on the 2D map (see, eg, Figures 2D and 4, ID3, spontaneous use).
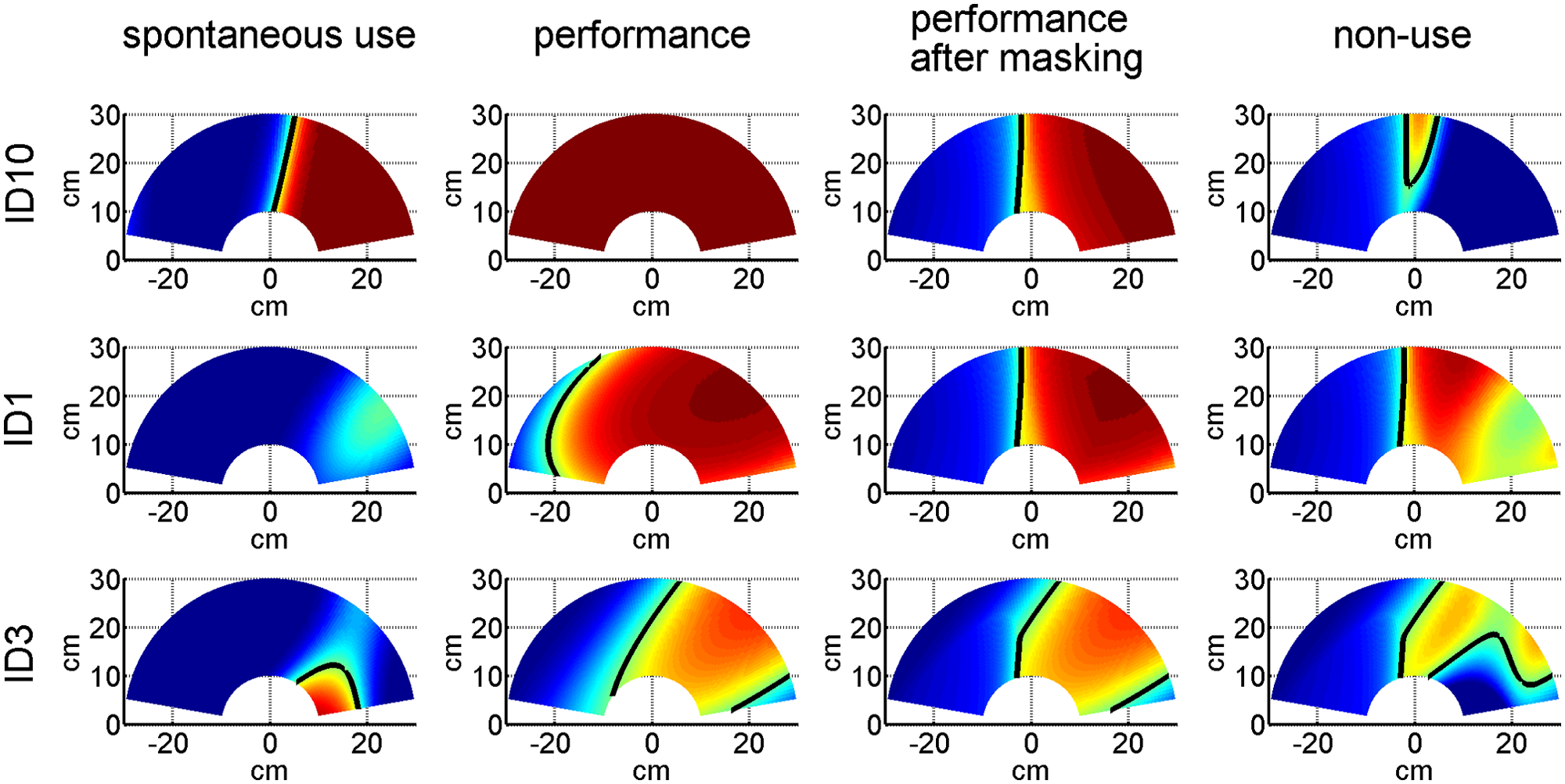
Examples of use and nonuse with BART in 1 session over the 2D reaching work space for 3 right-affected participants poststroke. Each row represents a different participant: a participant with little nonuse (ID10; session 2, FM 63, coordination subscale of the FM-UE [FM_cor] 5, sBART = 0.64, cBART = 0.57, nuBART = 0.113), a participant with large nonuse, albeit mild impairment (ID1; session 2, FM 57, FM_cor 4, sBART = 0.10, cBART = 0.54, nuBART = 0.433), and a participant with moderate nonuse (ID3; session 2, FM 49, FM_cor 3, sBART = 0.18, cBART = 0.340, nuBART = 0.239). Maps from left to right for each row: spontaneous use, performance, performance after masking with normative hand use data, and nonuse. As in Figure 2, nonuse maps are shown for illustrative purpose only
For those 24 poststroke participants enrolled for the study overall, sBART was 0.28 ± 0.04, and cBART was 0.41 ± 0.03. The nuBART was significantly greater than 0 (0.17 ± 0.04, P < .001, 1-sample Wilcoxon signed ranks test), although not normally distributed (P < .01 Shapiro-Wilk test).
There were, however, large differences in use, performance, and nonuse across participants poststroke. Out of 24, 8 participants, 2 with left and 6 with right hemiplegia, exhibited no arm use, with sBART = 0. Of these participants, 3 showed maximal performance cBART—these 3 participants thus exhibited maximal nonuse with BART. The other 16 participants use their arm to some extent because sBART was positive (0.42 ± 0.03, P < .001, Mann-Whitney). We found that 8 of these participants, all with left hemiplegia, exhibited non-disabled-like patterns of use (sBART = 0.4 for left hemiplegia and 0.6 for right hemiplegia).
Out of 24, 13 participants, 6 with left and 7 with right hemiplegia, had non-disabled-like performance, as measured by cBART. Among the other 11 participants, cBART was 0.26 ± 0.03 for the 5 left- and 0.40 ± 0.08 for the 6 right-hemiplegic participants (because of the masking procedure, average maximum cBART was 0.4 for left hemiplegia and 0.6 for right hemiplegia; see above). We verified that the 11 participants with lower performance had a lower coordination subscale of the FM-UE (FM_cor; median FM_cor of 3, range = 2-5) than the 13 participants with non-disabled-like performance (median FM_cor of 5, range = 4-6; P < .05, Mann-Whitney).
Out of 24, 11 participants, 9 with left and 2 with right hemiplegia, showed no nonuse, with nuBART = 0. The 13 participants with positive nonuse had a median nuBART = 0.235 (different from 0, P = .0001, Mann-Whitney). Most participants with right hemiplegia exhibited at least some degree of nonuse (2 out of 13) in contrast to participants with left hemiplegia for whom only 2 out of 11 exhibited greater than zero nonuse. Finally, there were no significant correlations of nuBART with months since stroke (P > .4) and age (P > .5).
BART Test-Retest Reliability
For the 19 participants poststroke who participated in the reliability study, sBART was 0.25 ± 0.04 for the first session, 0.28 ± 0.05 for the second session, and 0.29 ± 0.04 for the third session. sBART, cBART, and nuBART had good test-retest reliability across the 3 sessions: sBART ICC was 0.840 (P < .0001), cBART ICC was 0.807 (P < .0001), and nuBART ICC was 0.786 (P < .0001; note, however, that these ICC results should be considered with caution because sBART and nuBART were not distributed normally). The correlations of sBART, cBART, and nuBART between sessions 1 and 2 were good (sBART: r = 0.668, P = .002, Spearman correlation; cBART: r = 0.803, P < .0001, Pearson correlation; nuBART: r = 0.711, P = .001, Spearman correlation) and increased between sessions 2 and 3 (sBART: r = 0.854, P < .0001, Spearman correlation; cBART: r = 0.883, P < .0001, Pearson correlation; nuBART: r = 0.950, P < .0001, Spearman correlation). This demonstrates excellent reliability of BART between sessions 2 and 3 but lower reliability between sessions 1 and 2. As a result, we considered the first session as a familiarization session and only analyzed the data from session 2 in the validity study.
Unlike nondisabled participants who could always reach all the targets within 1.2 s, reach success in the sBART condition was lower for participants with stroke, although success rates improved somewhat over the sessions (first session success rate = 87.26% ± 2.64%, second session = 91.97% ± 1.96%, and third session = 91.02% ± 2.19%; repeated ANOVA, P < .037; session 1 vs 2: paired t test, P = .012; session 2 vs 3: paired t test, P > .5).
External Validity of BART Use sBART, Performance cBART, and Nonuse nuBART
Here, we validate sBART, cBART, and nuBART with equivalent AAUT QOM measures for 15 participants who participated in the validity study using BART measurements from the second session. Correlation between sBART and sAAUT QOM was good (r = 0.679, P = .005, Spearman). Correlation between cBART and cAAUT QOM just reached significance (cAAUT QOM r = 0.515, P = .05, Spearman). Finally, correlation between nuBART and nuAAUT was good (r = 0.683, P = .005, Spearman). Figure 5 shows nuAAUT as a function of nuBART. Note that nuBART was 0 for 6 participants and very close to 0 (0.008) for another participant.
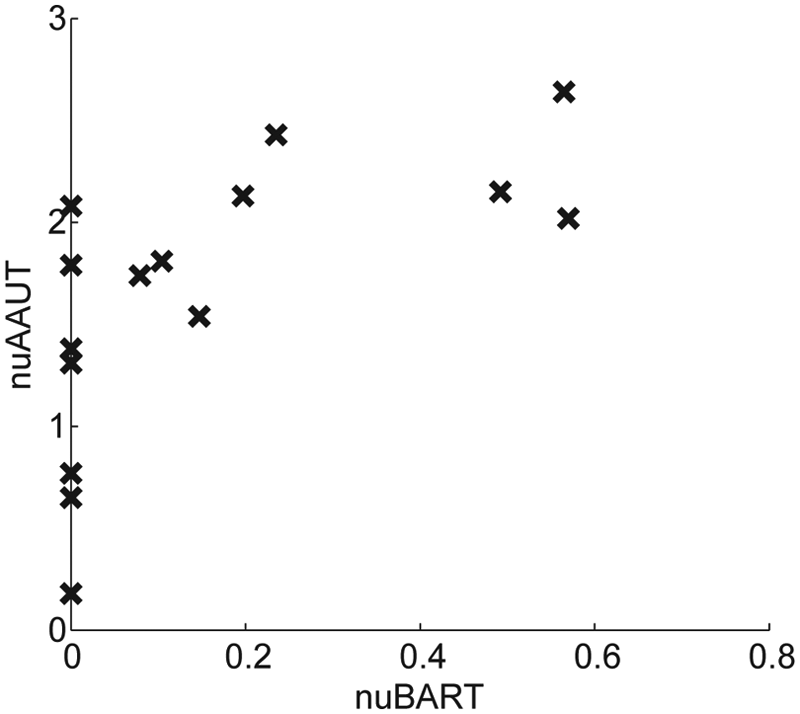
External validity of nuBART shown by plotting nuAAUT as a function of nuBART for 15 participants poststroke in the validity study (correlation between nuBART and nuAAUT, r = 0.683, P = .005, Spearman)
Discussion
The present study makes 3 important and novel contributions. First, to our knowledge, this study quantified paretic arm nonuse in individuals with chronic stroke for the first time. For this purpose, we subtracted average use obtained in the spontaneous use condition of the AAUT QOM from average performance obtained in the constrained use condition of the AAUT QOM. Second, we have developed a novel laboratory-based measurement tool, the BART, to measure arm nonuse objectively. BART is simple to administer, requires minimal instructions to the participant and personnel training, and is objective. Third, we showed that nonuse measured with BART has excellent test-retest reliability and good external validity, with nonuse measured with the AAUT QOM. Although we have developed and studied BART especially for individuals poststroke, we believe that BART can reliably quantify arm use and performance over the long run in participants with other lateralized conditions such as Parkinson’s disease, cerebral palsy, hand retransplantation, or scapular pain.
We found no correlation between either measure of nonuse, nuAAUT and nuBART, with time since stroke and age. However, we found with BART that nonuse depends on the arm affected. Most participants with affected right (dominant) arm exhibited nonuse; in contrast, most left-arm participants showed no nonuse. This result is in line with previously reported differences in use between affected left and right hands. 18 It also indirectly supports the learned nonuse hypothesis: right-handed left hemiplegic participants presumably have few opportunities to experience negative consequences following use of their paretic arm in daily activities. This result needs to be independently reproduced, however, because we found no such difference between arms with the nuAAUT.
As a measure of arm use, BART has several advantages compared with existing instruments such as the MAL and AAUT. First, it provides an objective and quantitative measure of voluntary paretic arm use in daily life poststroke. Second, BART exhibits excellent reliability for repeated measures, making it ideal for examining the effectiveness of rehabilitation on nonuse. In contrast, the AAUT is best used only once, or at most only infrequently, as in the EXCITE trial. 19 Third, BART is simple and timesaving. Unlike the MAL, which takes at least an hour to administer, a single BART session takes less than 15 minutes.
There are nonetheless several limitations to the present study. First, nonuse quantified with the AAUT may be at least partly the result of a learning effect. We indeed found a small improvement on the tasks that the participants could perform (score > 0) in the constrained AAUT condition (mean score 3.61 ± 0.11 on these tasks) compared with the spontaneous AAUT condition (3.26 ± 0.13 on these tasks; paired t test: P < .0001). Thus, although a small learning effect cannot be excluded, it is small compared with the average nuAAUT (0.35 vs 1.67). Second, because of the difficulty in recruiting prestroke left-hand dominant participants, we only developed BART for prestroke right-hand dominant individuals. Third, we did not control for compensatory arm movements such as excessive shoulder elevation and abduction during reaching, 20 and we observed that several participants were using such compensatory strategies. Fourth, we set the time allowed to complete the reaching movements to a single value of 1.2 s. In our beta version of BART, we noticed that without a time limit in the constrained condition, participants poststroke reached almost all targets. In the beta version, median movement time was 845 ms. We thus hypothesized that 1.2 s could discriminate the performance of poststroke individuals with mild to moderate impairments from that of nondisabled controls. However, with this 1.2-s time limit, 13 out of 24 participants poststroke still showed control-like performance as measured by cBART. This suggests that 1.2 s is too long for these 13 participants. In contrast, 8 participants chose not to use the paretic arm at all in the second session, as measured by sBART. This suggests that 1.2 s is too short for at least these 8 participants. Thus, in future work, we will need to parameterize BART to detect nonuse across a large proportion of patients. Fifth, the pointing task in BART mimics only 1 aspect of upper-extremity use (eg, reaching) but does not include other actions that might be part of daily use, such as stabilizing, grasping, and so on. This may explain why we found a somewhat lower-than-expected correlation between the AAUT and BART in the spontaneous condition. In future work, improved systems could, for instance, present tools that allow grasping at different spatial locations. Task-based rehabilitation robots21,22 could be modified for this purpose. Finally, although administering BART requires very little expertise, the hardware (mini-bird magnetic sensors and projector mounted above table) needed in the current implementation makes it a research tool only. In addition, the current method to compute use and nonuse is somewhat complicated, notably with the second-order logistic model fit implemented in MATLAB. Whereas a simpler method based on counts at each target may be appropriate to compute overall use and nonuse, the proposed method leads the way for the spatial assessment and treatment of nonuse (see Figures 2 and 4).
Besides the Sterr et al. study, 8 we are aware of only 2 other studies that have attempted to measure use and nonuse in individuals poststroke. First, Johnson et al. 23 evaluated nonuse in 5 participants poststroke by measuring errors during a steering task in affected, unaffected, and bimanual arms conditions. Second, Brown 24 measured arm use (but not nonuse) in 13 participants with stroke with a device similar to our BART device with 5 actual reaching tasks involving proximal and/or distal hand movements.
In addition to its usefulness in measuring use and nonuse, BART may be useful to elaborate our understanding of motor control and decision making underlying reaching choice and notably the factors that affect changes in these choices, including changes in performance as a result of motor therapy. We have previously proposed and have begun to test an “optimal therapy threshold” hypothesis,25-27 according to which a minimum amount of therapy is needed to reach a minimum arm use level, such that use and performance continue to improve following therapy. BART can be helpful in determining such a threshold with repeated measurements of use and nonuse before, during, and after therapy.
Footnotes
Appendix A
Acknowledgements
We thank Dr Young Geun Choi for help with computer programming, Dr James Gordon for his inputs during development of the task, Neerav Parikh and Jijye Lee for help with data collection.
Authors’ Note
CEH and SK contributed equally to this work.
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This work was in part supported by NIH grants P20 RR020700-01, R03 HD050591-02, and R01 HD065438-01A2. CEH is in part supported by the WCU program through the National Research Foundation of Korea funded by the Ministry of Education, Science and Technology (R32-10142). RO is in part supported by the Funding Program for Next Generation World-Leading Researchers, Japan and SRPBS, MEXT, Japan.