
Abstract
Background. Balance and mobility problems are common for people with Parkinson disease (PD). Objective. To determine the relationships of motor and cognitive impairments with specific balance and mobility task performance. Methods. A total of 82 community-dwelling people with idiopathic PD were tested “on” medication. Impairments measured included leg extensor and hip abductor muscle power, freezing of gait, dyskinesia, and executive function. Balance and mobility were classified into tasks requiring anticipatory control with a change in base of support, anticipatory control without a change in support, and reactive adjustments in response to external perturbations. Associations between impairments and tasks were examined using univariable and multivariable linear regression models. Results. Univariable models revealed that muscle power was significantly related to balance and mobility, explaining 7% to 33% of the variability in task performance. Freezing of gait, dyskinesia, and executive function were not consistently related to task performance. Multivariable models that included all impairments plus disease severity, age, gender, and height explained 5% to 43% of the variability in balance and mobility tasks. Leg muscle power was the only impairment with a consistent association with performance of tasks involving anticipatory control with a change in base of support (β = 0.2 to 0.5), but the association of each muscle group was specific to individual tasks. Conclusion. Information gained from this study about the relationships between impairments and specific balance and mobility tasks may be able to guide the development of interventional strategies for people with PD.
Keywords
Introduction
Poor balance and reduced mobility are common problems for people with Parkinson disease (PD). 1 Such problems manifest as slow and inconsistent walking, difficulty standing up from a chair, and difficulty maintaining balance while standing and walking. Problems with walking can occur at all stages of disease severity,1-3 adversely affecting quality of life. 4 Balance problems develop as the disease progresses and may lead to adverse consequences such as falling. 5
People with PD typically present with multiple motor and nonmotor impairments. 6 To date, the investigation of impairments contributing to self-reported activities of daily living7,8 show associations between impairments and reduced activity but do not address the impact of impairments on performance of specific balance and mobility tasks. A small number of studies have addressed the contribution of individual motor impairments to specific mobility tasks. These studies show that bradykinesia, 3 reduced muscle strength, 9 reduced muscle power,10,11 and freezing of gait12,13 are associated with reduced walking speed and that bradykinesia 14 and reduced muscle strength15-17 are associated with reduced speed of standing up from a chair. Other motor impairments such as dyskinesia as well as nonmotor impairments such as reduced cognition are also likely to influence balance and mobility task performance, but these associations have not been investigated.
One recently identified motor impairment that is likely to influence balance and mobility task performance is reduced muscle power (force × speed of muscle contraction).10,11 Reduced muscle power is particularly pronounced at low loads of force production 10 and appears to be a result of reduced muscle strength and bradykinesia but not rigidity or tremor. 18 Because performance of balance and mobility tasks such as walking require small amounts of muscle force to be produced quickly, maintenance of sufficient leg muscle power may be critical for recovering quickly from a loss of balance to avoid falling. Reduced leg muscle power has been shown to be a predictor of mobility and of fall risk in the older population in general,19-21 particularly when producing small rather than large amounts of force. 22 As such, reduced leg muscle power may also be related to impaired performance of balance and mobility tasks as well as risk of falling in people with PD.
Knowledge of the relationships between multiple impairments and performance of specific balance and mobility tasks may assist physical therapists in prescribing specific exercise interventions for individual patients according to each individual’s specific balance and mobility problems. The aim of this study was therefore to determine the relationships of leg muscle power and other impairments, including freezing of gait, dyskinesia, and cognitive impairment, with the performance of specific balance and mobility tasks in people with PD. We hypothesized that muscle power, freezing of gait, dyskinesia, and impaired executive function would be related to the performance of balance and mobility tasks. In addition, we hypothesized that these relationships between impairments, and balance and mobility task performance would persist after adjusting for possible confounding factors.
Methods
Participants
A convenience sample of community-dwelling people with a diagnosis of idiopathic PD was recruited from 2 sources: (1) our university database of people with PD and (2) an advertisement placed in a PD association newsletter. All participants were aged ≥ 40 years and were able to walk independently with or without a walking aid. Participants were excluded if they had significant cognitive impairment (Mini-Mental State Examination score < 24), suffered from other neurological conditions, or suffered from any unstable cardiovascular or orthopedic conditions that would interfere with the safety of assessment and/or interpretation of results. All tests were conducted in a single assessment session of approximately 2.5 hours’ duration in a laboratory. Individuals were tested when they self-reported that their medications were working optimally, usually 1 hour after taking their medication; 9 participants reported going “off” during testing, so testing was suspended until they had taken their medication and reported being “on” again. This study was approved by the relevant Human Ethics Committee, and all participants gave written informed consent prior to testing.
Outcome Measures
Impairments
Muscle power testing was conducted using pneumatic variable resistance equipment (Keiser A420, Keiser Sports Health Equipment, Fresno, CA). The leg extensors were tested using the seated leg press, as previously described, 10 and the hip abductors were tested using the standing hip machine, which involves the participant standing on 1 leg and abducting the other leg to 30° without flexing the hip and knee of either leg while holding on for support. The order of testing left and right sides was randomized for each participant. Leg muscle power was assessed at 6 relative loads (30% to 80% of the 1 repetition maximum [1RM], which is the maximal load that a person is able to lift once through the complete range of motion, at 10% increments) for each leg for the leg extensors followed by the hip abductors. Power output at 40% 1RM for each leg for each muscle group was recorded because the contribution of muscle power produced at lighter loads to mobility is greater compared with muscle power produced at heavier loads.11,22 Measures of leg muscle power reported are the average for both legs for each muscle group.
The presence of freezing of gait was determined by the New Freezing of Gait Questionnaire. 23 Scores range from 0 to 29, with higher scores indicating greater severity of freezing. Dyskinesia was scored as the sum of items 4.1 (time spent with dyskinesias) and 4.2 (functional impact of dyskinesias) from the Motor Complications (part 4) section of the Movement Disorders Society–sponsored Unified Parkinson Disease Rating Scale (MDS-UPDRS). 24 The element of cognition that this study focused on was executive function. Executive function was tested using the Frontal Assessment Battery, 25 with lower scores indicating greater impairment.
Balance and mobility task performance
Balance and mobility tasks were broadly categorized into 3 groups 26 according to the nature of the postural adjustments required: (1) tasks requiring anticipatory control with a change in base of support, for example, walking; (2) tasks requiring anticipatory control without a change in the base of support, for example, reaching while standing; and (3) tasks requiring reactive adjustments in response to external perturbations, for example, reactive stepping.
Anticipatory Control With a Change in Base of Support
Tasks requiring anticipatory control with a change in the base of support included repeated sit-to-stand, fast walking speed, and choice stepping reaction time. 27 The 5-repetition sit-to-stand was performed as fast as possible from a 45-cm chair, with arms folded across the chest. The time taken to complete this task was measured to the nearest millisecond with a handheld stopwatch. This score was then converted to number of stands completed per second to facilitate the interpretation of results. The time to walk 10 m was measured using a handheld stopwatch and the score recorded to the nearest millisecond. Fast walking pace was measured over the middle 10 m of a 14-m corridor, and walking speed was calculated in m/s. Repeated sit-to-stand and fast walking were performed twice, and the best score for each measure was used for data analysis. Choice stepping reaction time 27 was timed using a handheld stopwatch, and the score recorded to the nearest millisecond. This score was then converted to number of steps completed per second to facilitate the interpretation of results.
Anticipatory Control Without a Change in Base of Support
Tasks requiring anticipatory control without a change in the base of support included functional reach 28 and single-leg stand. Functional reach was measured using a tape measure and scores recorded to the nearest 0.5 cm. This measure was performed twice and the best score used for data analysis. Single-leg stand was timed up to 30 s on each leg using a handheld stopwatch, 29 and the score recorded to the nearest millisecond. Measures of single-leg stand reported are the average score for both legs.
Reactive Adjustments
Tasks requiring reactive adjustments in response to external perturbations were rated using the push and release test, 30 which rates the postural response to a sudden release when pushing backward, and the pull test (item 3.12 of the MDS-UPDRS), which rates the postural response to a sudden displacement of the body posteriorly. Both these tests of reactive stepping are rated on a 5-point scale, with higher scores indicating impaired postural adjustments; the scores were summed to provide a measure of reactive balance. For the ease of interpretation of results, scores for reactive stepping were inverted, so that a high score indicated good performance.
Statistical Analysis
We chose a priori to examine leg muscle power at 40% 1RM,11,22 based on evidence suggesting that muscle power produced at low rather than high loads of force is more strongly associated with mobility. 22 Because it is common to examine peak muscle power,31-33 we examined the relationship between peak muscle power and muscle power at 40% 1RM for each muscle group using Pearson’s correlation coefficients. Muscle power at 40% 1RM and at peak power were highly correlated (r = 0.97 for the leg extensors and r = 0.95 for the hip abductors).
To decrease the risk of collinearity, we wished to avoid entering highly correlated predictor variables into the same multivariable model. Thus, we examined the relationships between predictor variables using Pearson’s correlation coefficients prior to conducting multivariable analyses. Because leg extensor and hip abductor muscle power at 40% 1RM were highly correlated (r = 0.81; P < .001), the relationships between these variables and balance and mobility were examined in separate models.
Relationships between impairments (predictor variables) and balance and mobility task performance (outcomes) were examined with univariable linear regression. Each of the predictor variables (muscle power, freezing of gait, dyskinesia, and executive function), disease severity (motor examination section of the MDS-UPDRS), age, gender, and height was entered into 2 multivariable linear regression models (one model containing leg extensor muscle power and the other containing hip abductor muscle power) for each outcome (sit-to-stand, fast walking, choice stepping, functional reach, single-leg stand, and reactive stepping). The proportion of variability in balance or mobility task performance explained by the predictor variables was determined using the R2 statistic from the multivariable linear regression models. Each multivariable linear regression model was also used to determine the relative association between the various impairments, disease severity, age, gender, and height and task performance. Data were analyzed using SPSS version 18 (SPSS Inc, Chicago, IL).
Some muscle power data were missing for participants who were so weak that their predicted 40% 1RM load fell below the lowest setting of the Keiser equipment. For these participants (5% of the sample for the leg extensors and 2% for the hip abductors), values were assigned on the basis of the available power data for each individual. For participants who were physically unable to perform repeated sit-to-stand (1% of participants) or choice stepping reaction time (2% of participants), a value of the sample mean minus 3 standard deviations (SDs) was assigned.
Results
A total of 82 people with PD (55 male, 27 female) participated in this study (Table 1). Of these, 76 participants were taking levodopa: 27 were taking it in isolation, and the remainder were taking it in combination with other medications for PD (dopamine agonists, anticholinergics, MAO-B [monoamine oxidase B] inhibitors, and COMT [catechol O-methyl transferase] inhibitors). Three participants were not taking levodopa but were taking a dopamine agonist with or without an anticholinergic, whereas 3 participants were not taking any PD medications; 8 participants were receiving deep-brain stimulation. Participants took a mean levodopa equivalent dose of 732 mg/d (SD 430 mg/d). Severity of impairments as well as balance and mobility task performance is reported in Table 2.
Participant Characteristics (N = 82)
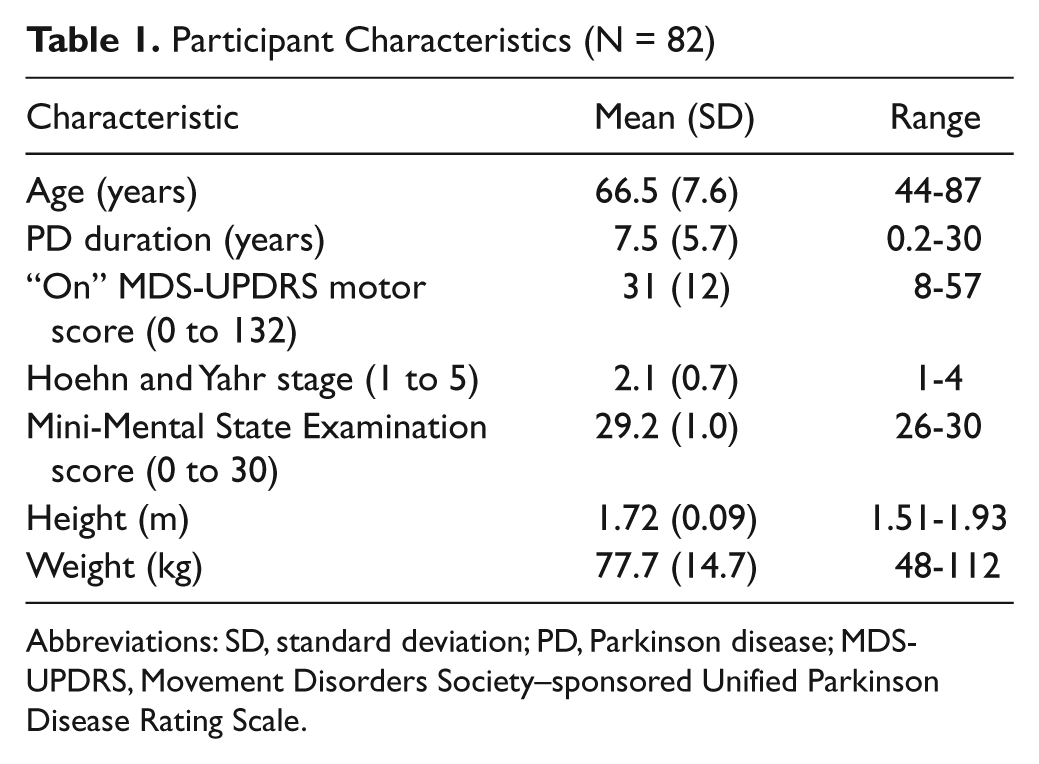
Abbreviations: SD, standard deviation; PD, Parkinson disease; MDS-UPDRS, Movement Disorders Society–sponsored Unified Parkinson Disease Rating Scale.
Mean (SD) Performance on Measures of Impairment and Task Performance for the Sample of Participants (N = 82)
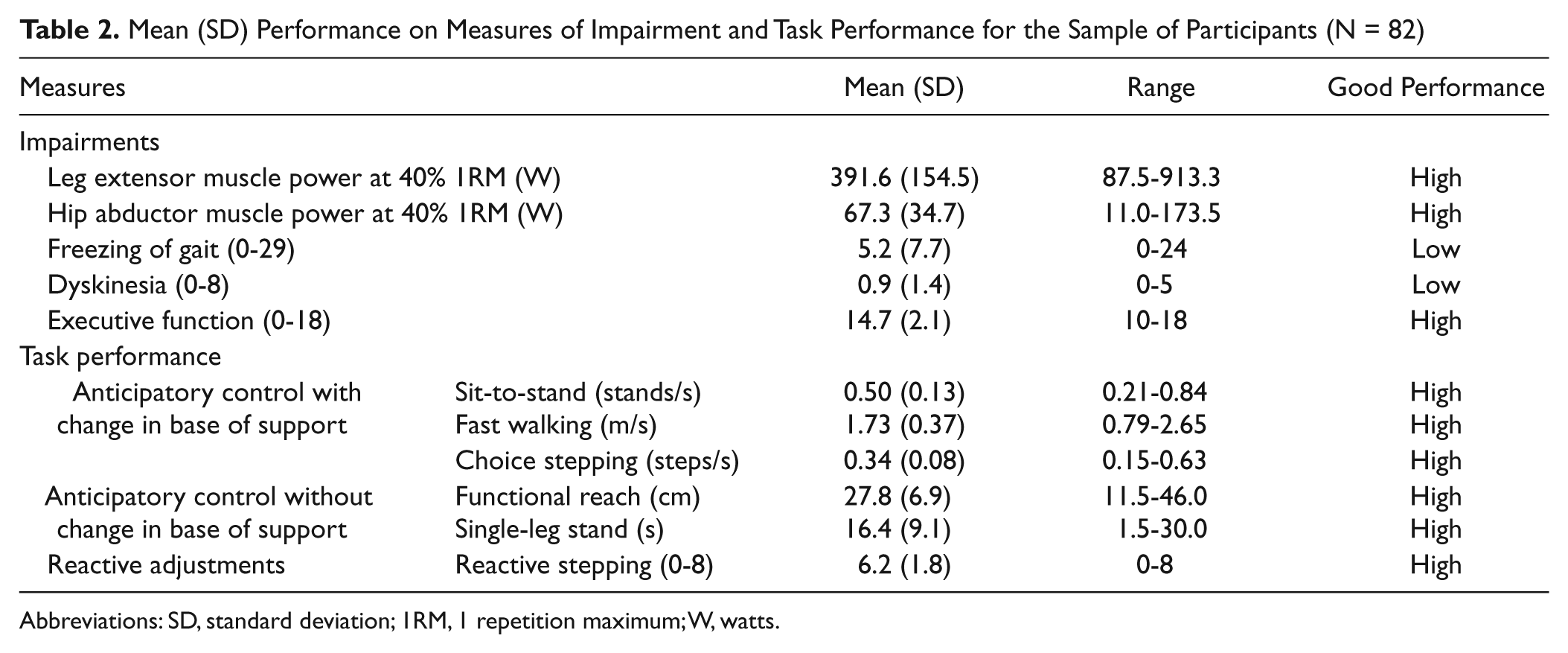
Abbreviations: SD, standard deviation; 1RM, 1 repetition maximum; W, watts.
Anticipatory Control With a Change in Base of Support
Univariable models revealed that leg muscle power explained a significant proportion of the variability in tasks requiring anticipatory control with a change in the base of support, that is, sit-to-stand, fast walking, and choice stepping performance (9%-32% for leg extensor power, 15%-33% for hip abductor power; Table 3). Freezing of gait, dyskinesia, and executive function explained up to 6% of the variability in some but not all these tasks. Multivariable models combining leg extensor or hip abductor muscle power with freezing of gait, dyskinesia, executive function, disease severity, age, gender, and height explained 28% to 43% of the variability in these tasks requiring anticipatory control with a change in the base of support (Table 4). The multivariable models revealed that leg extensor muscle power (β = 0.5; P = .003) and height (β = −0.4 to −0.5; P = .001-.007) had strong associations with sit-to-stand performance, whereas hip abductor muscle power (β = 0.3; P = .02), freezing of gait (β = −0.2 to −0.3; P = .02-.03), and disease severity (β = −0.3; P = .003-.01) had moderate associations with fast walking. Disease severity had a strong association with choice stepping performance (β = −0.4; P < .001), whereas hip abductor muscle power (β = 0.2; P = .048), dyskinesia (β = −0.2; P = .04), and age (β = −0.2; P = .02) had moderate associations with this task.
Univariable Associations Between Impairments (Predictor Variables) and Task Performance (Outcomes)
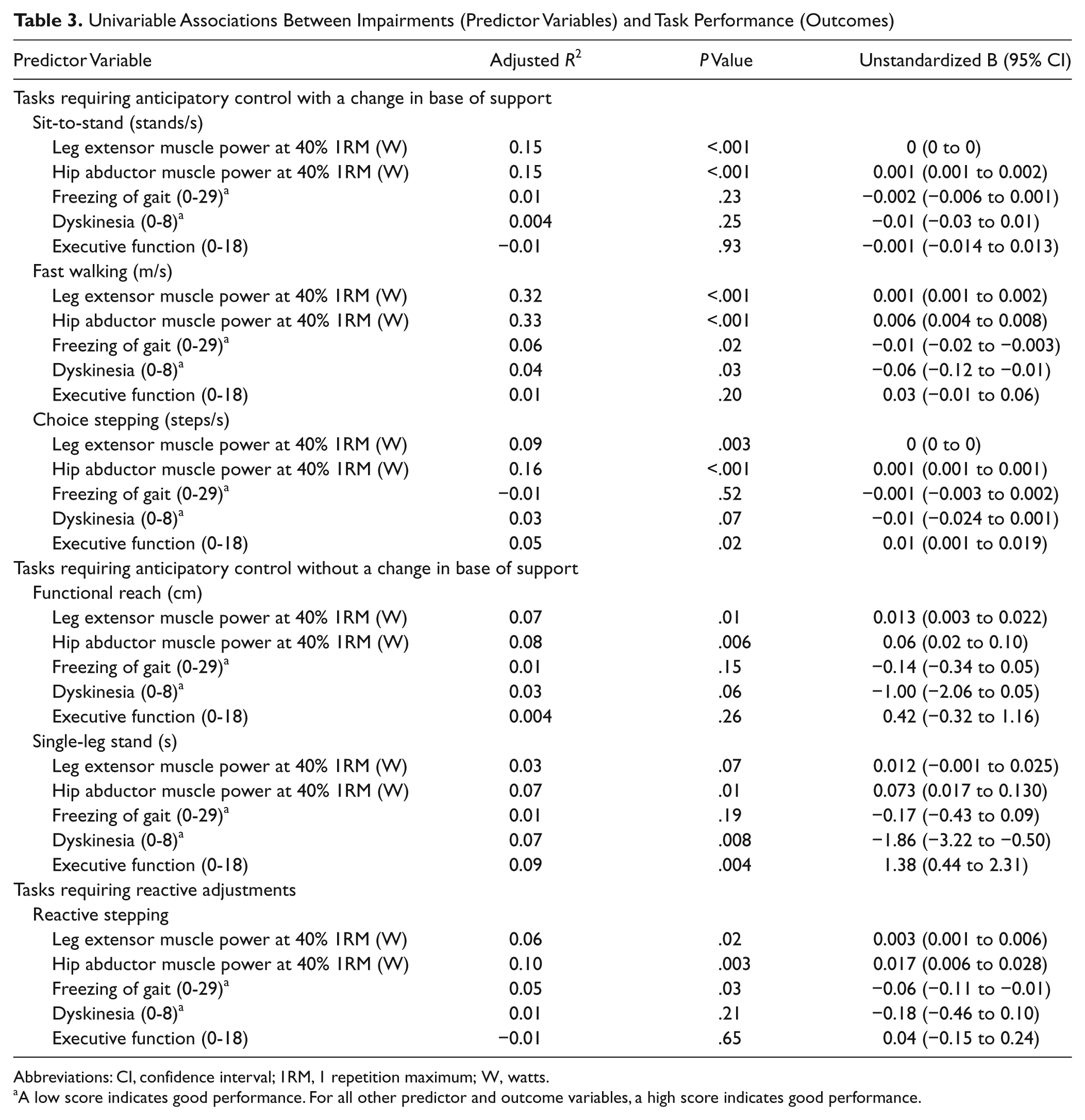
Abbreviations: CI, confidence interval; 1RM, 1 repetition maximum; W, watts.
A low score indicates good performance. For all other predictor and outcome variables, a high score indicates good performance.
Associations Between Impairments (Predictor Variables) and Task Performance (Outcomes) from the 2 Multivariable Regression Models, after Adjusting for Possible Confounders a
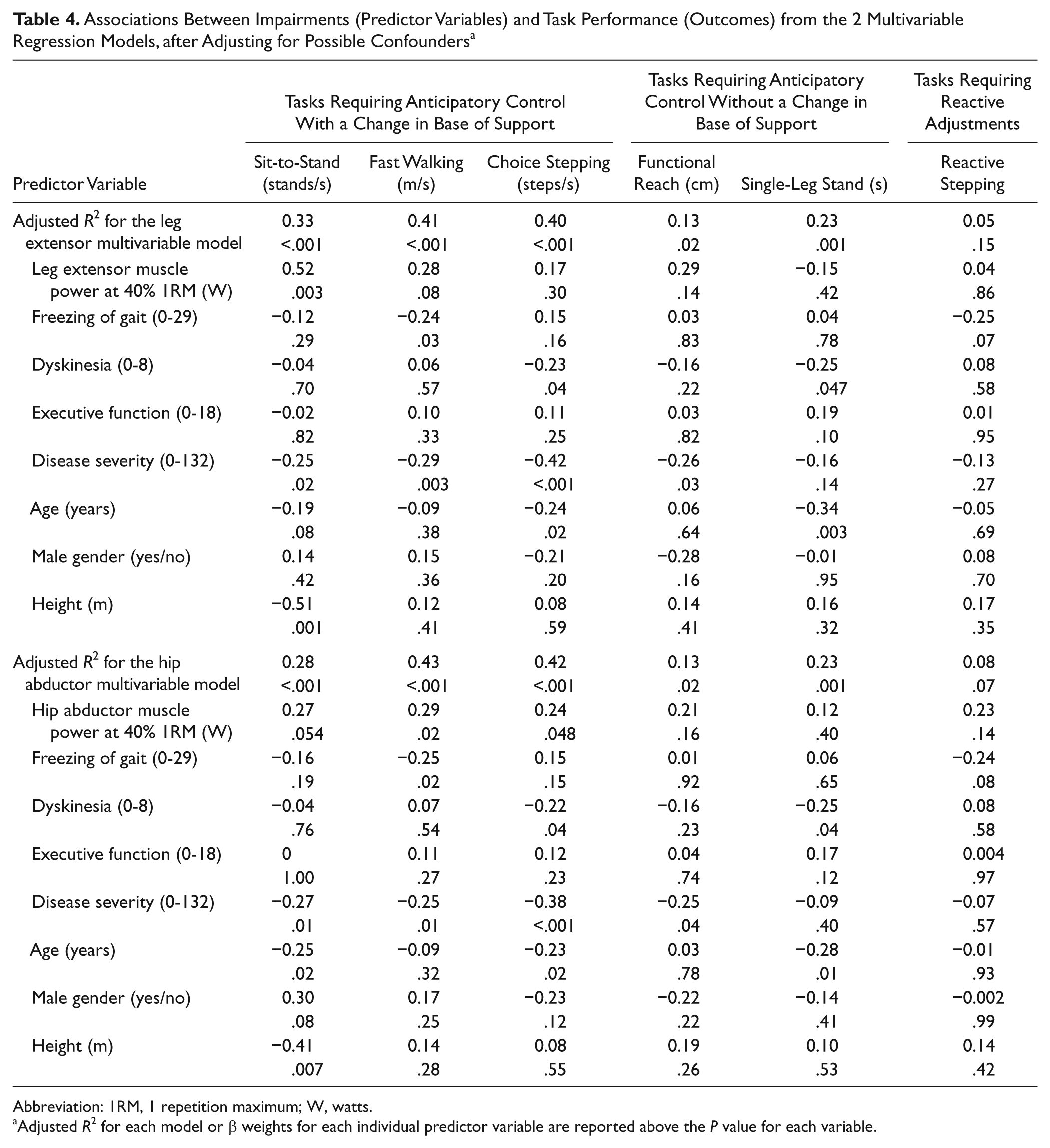
Abbreviation: 1RM, 1 repetition maximum; W, watts.
Adjusted R2 for each model or β weights for each individual predictor variable are reported above the P value for each variable.
Anticipatory Control Without a Change in Base of Support
Univariable models revealed that hip abductor muscle power explained 7% to 8% of the variability in tasks requiring anticipatory control without a change in the base of support, that is, single-leg stand and functional reach, respectively (Table 3). Leg extensor muscle power, dyskinesia, and executive function explained up to 9% of the variability in one but not both tasks. Multivariable models explained 23% of the variability in single-leg stand and 13% of the variability in functional reach (Table 4). The multivariable models revealed that disease severity had a moderate association with functional reach (β = −0.3; P = .03-.04), whereas dyskinesia (β = −0.3; P = .04-.047) and age (β = −0.3; P = .003-.01) had moderate associations with single-leg stand.
Reactive Adjustments
Univariable models revealed that muscle power and freezing of gait explained 5% to 10% of the variability in reactive stepping (Table 3). However, the multivariable models did not explain a significant proportion of the variability in this task requiring reactive postural adjustments (5%-8%; P > .05; Table 4).
Discussion
This study found that motor impairments and executive function had task-dependent relationships with balance and mobility in people with PD. The multivariable models combining leg extensor or hip abductor muscle power with freezing of gait, dyskinesia, executive function, disease severity, age, gender, and height explained the greatest proportion of variability for tasks involving anticipatory postural control with a change in the base of support, that is, walking (41%-43%), choice stepping (40%-42%) and sit-to-stand (28%-33%). These variables accounted for a smaller proportion of the variability for tasks involving anticipatory postural control without a change in the base of support, that is, standing on 1 leg (23%) and functional reach (13%) and only explained 5% to 8% of the variability in reactive stepping.
The relationship of muscle power with balance and mobility task performance was found to depend on both the muscle group and the task under investigation. In univariable analyses, muscle power explained up to 33% of the variability in tasks requiring anticipatory control with a change in base of support. The moderate relationship of hip abductor muscle power with walking and choice stepping may be a result of the role of the hip abductors in maintaining pelvic control to keep the body’s center of mass balanced over the base of support.34-36 The strong relationship between leg extensor muscle power and sit-to-stand found in this study is consistent with previous findings showing that leg extensor muscle strength14,15 and slowness to generate adequate force14,17 are related to sit-to-stand ability in people with PD. In contrast, muscle power only explained 3% to 10% of the variability in tasks requiring anticipatory control without a change in base of support or tasks requiring reactive postural adjustments. This difference may be a result of the requirements of these tasks. The focus of the functional reach test is on distance rather than speed. Single-leg stand probably requires sustained activity at the hip but more rapid changes in muscle activity at the ankle. Studies in the general older population have also found muscle power to be more strongly associated with anticipatory rather than reactive balance. 37
Freezing of gait, dyskinesia, and executive function each explained up to 9% of the variability in some but not all tasks in univariable analyses. As expected, freezing of gait was significantly related to walking.13,38,39 The lack of relationship between freezing of gait and choice stepping is likely a result of the visual cues provided and the concentration required to perform the task. This is consistent with findings showing reductions in freezing of gait with cueing.40-42 Dyskinesia was found to have a small to moderate significant relationship with reduced ability to stand on one leg and slowed choice stepping. The choreic nature of dyskinesia 43 would explain the difficulty in keeping balance while standing on one leg. Slowed choice stepping in the presence of dyskinesia may be explained by the competing demands placed on attention by simultaneously following the task instructions and maintaining balance despite involuntary movements. Anxiety may also be a factor influencing dyskinesia 44 when attempting this attention-demanding task. Surprisingly, executive function did not have a significant independent relationship with task performance in any multivariable model, although it was associated with single-leg stand and choice stepping in univariable models. The element of cognition investigated in this study may account for these findings because other studies suggest impaired attention45-47 to be a contributor to poor performance on tasks with a high attentional demand.
Disease severity had moderate relationships with most balance and mobility tasks, indicating the contribution of PD progression to disability. 8 Age was significantly related to sit-to-stand, choice stepping, and single-leg stand. Deterioration in balance with aging48-50 would account for these results. Additionally, the effect of aging in reducing muscle strength 51 accounts for the relationship between age and sit-to-stand because strength is a major contributor to sit-to-stand performance in older people 52 and in people with PD.14,15 The relationship between height and sit-to-stand performance is likely a result of the use of a standard chair unadjusted to height.
This study has several limitations. We only recruited participants who were able to attend the university laboratory for muscle power testing and who were able to cope with the demanding nature of the testing protocol. In addition, people with significant cardiovascular disease and lower-limb orthopedic conditions were excluded from the study. The wide variation among levels of motor impairments and executive function in this sample suggests that the results are generalizable to people with mild to moderate PD but not severe PD. The cross-sectional nature of this study does not enable investigation of how disease progression influences the relationships between impairments and task performance. Future longitudinal studies would provide greater insight into how symptom progression influences balance and mobility and, thus, would be able to guide long-term nonpharmacological management of people with PD; two such studies are currently under way.53,54
Intervention trials are also required to test the impact of interventions such as motor learning and practice55,56 on balance and mobility in people with PD. For example, there are suggestions that task-specific step training in response to external perturbations may improve reactive stepping.57,58 Muscle power training in people with PD warrants investigation. This suggestion is supported by evidence from the general older population showing improvements in muscle power, 32 mobility, 59 and balance 33 with muscle power training as well as our findings showing that leg muscle power is associated with weakness and bradykinesia. 18
Conclusion
This study has demonstrated that the relationships of impairments with balance and mobility vary according to the specific task undertaken. Additionally, the relationship between muscle power and task performance varies according to the muscle group being investigated and the task. Such information may assist health professionals in developing physical intervention strategies for individuals with PD, which will require evaluation in future studies.
Footnotes
Acknowledgements
The authors wish to thank Jooeun Song for her assistance with data collection. We also thank the people with Parkinson disease who participated in this research.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This research was supported by a seeding grant from the Physiotherapy Research Foundation of Australia (seeding grant number: S10-012). SSP receives financial assistance from a National Health and Medical Research Council of Australia (NHMRC) postgraduate scholarship. CS receives salary funding from the NHMRC. VSCF is on advisory boards and/or has received travel grants from Abbott, Allergan, Boehringer-Ingelheim, Hospira, Lundbeck, and Novartis.