
Abstract
Background. Fear of falling has been identified as an important and independent fall-risk predictor in patients with Parkinson’s disease (PD). However, there are inconsistent findings on the effects of balance and gait training on balance confidence. Objective. To explore whether balance and gait training with augmented feedback can enhance balance confidence in PD patients immediately after treatment and at 3- and 12-month follow-ups. Methods. A total of 51 PD patients were randomly assigned to a balance and gait training (BAL) group or to an active control (CON) group. The BAL group received balance and gait training with augmented feedback, whereas CON participants received lower-limb strength training for 12 weeks. Outcome measures included Activities-Specific Balance Confidence (ABC) Scale, limits-of-stability test, single-leg-stance test, and spatiotemporal gait characteristics. All tests were administered before intervention (Pre), immediately after training (Post), and at 3 months (Post3m) and 12 months (Post12m) after treatment completion. Results. The ABC score improved marginally at Post and significantly at Post3m and Post12m only in the BAL group (P < .017). Both participant groups increased their end point excursion at Post, but only the BAL group maintained the improvement at Post3m. The BAL group maintained significantly longer time-to-loss-of-balance during the single-leg stance test than the CON group at Post3m and Post12m (P < .05). For gait characteristics, both participant groups increased gait velocity, but only the BAL group increased stride length at Post, Post3m, and Post12m (P < .017). Conclusions. Positive findings from this study provide evidence that BAL with augmented feedback could enhance balance confidence and balance and gait performance in patients with PD.
Introduction
There is a high prevalence (35%-59%) of fear of falling (FoF) in people with Parkinson’s disease (PD),1-3 particularly those who have experienced previous falls, compared with age-matched healthy participants.2-5 An increased level of FoF has been associated with postural instability 2 and increased risk of future falls in individuals with PD.4,6 Excessive FoF can lead to self-induced restricted mobility, increased fall risk, social isolation, depression, and reduced quality of life for PD patients.1,7 Given the debilitating consequences of FoF, treatment intervention that aims to reduce FoF should be implemented for people with PD.
Balance, gait training, and strength training have been shown to facilitate postural stability and walking performance in people with PD,8-15 but their effects on reducing FoF have not been established. Combined balance and strength training has been reported as either having a positive 11 or a negative effect8,10 on reducing FoF, whereas balance and/or gait training have been reported to either reduce FoF9,12 or have no effect at all.14,15 In addition to these inconsistent findings, the longest follow-up duration for the above-mentioned studies was 10 weeks posttraining. 11 Thus, the long-term effects of treatment intervention on enhancing balance confidence remains unknown. Impaired gait performance and postural instability (ie, poor response to perturbation and short single-leg-stance [SLS] time) were found to be significant determinants of FoF.2,16,17 Therefore, interventions that facilitate balance and gait performance could improve balance confidence. Esculier et al 15 recently reported that balance training in an enriched visual feedback environment enhanced the balance abilities of patients with PD. It is possible that combined balance and gait training (BAL) with augmented feedback could enhance balance confidence, balance, and gait performance. This study aims to examine the short- and long-term effects of augmented feedback BAL on enhancing PD patients’ self-perceived balance confidence levels and secondarily to establish the association between self-perceived balance confidence and balance and gait performance in this population. All participants were assessed at baseline, at treatment completion, and at 3 months and 12 months after treatment completion. We hypothesized that augmented feedback BAL would increase self-perceived balance confidence immediately after treatment completion and at 3- and 12-month follow-ups in comparison with an active control (CON) group receiving strength training. In addition, we hypothesized that self-perceived balance confidence would be correlated with balance and gait performance in people with PD.
Method
Participants
This is a single-blinded randomized controlled trial with assessors blinded to group assignment. Participants were recruited from the Hong Kong Parkinson’s Disease Association, a patient self-help group, and the Movement Disorders Clinic at Tung Wah Hospital in Hong Kong. This project was approved by Ethics Committees of The Hong Kong Polytechnic University and Hospital Authority Hong Kong West Cluster. To be included in the study, participants were required to have a diagnosis of idiopathic PD according to the United Kingdom PD Society Brain Bank Criteria, 18 be stable on anti-Parkinsonian medications, be able to walk independently for 10 m, and follow instructions—that is, Mini-Mental State Examination score >23. 19 Patients were excluded if they had other neurological conditions, uncompensated cardiovascular disease, visual disturbance, or recent musculoskeletal disorders in the back or lower limbs that would interfere with balance and locomotion (Figure 1).
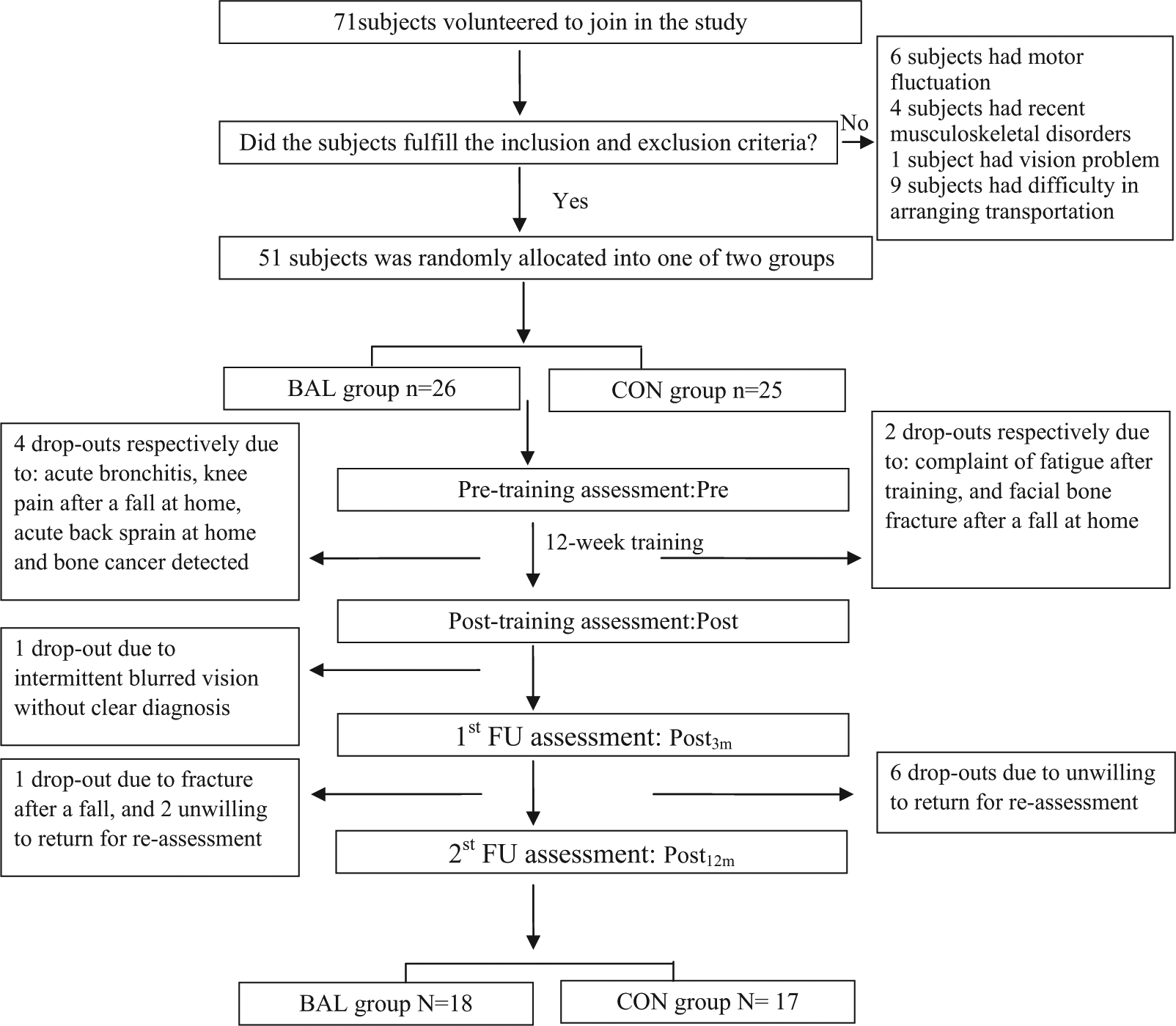
A flow of individuals participating in the study.
The sample size calculation was based on the significant improvement of the ABC score after balance training in Smania et al. 9 Their findings yielded a Cohen’s d effect size of 0.4. 9 By assuming a 5% type I error (α value) and 80% power (β level = 20%), the estimated sample size was 44 to reach significant change in the ABC score after training. 20 To allow for a 10% drop-out rate during the study, 49 patients with PD were recruited. In the present study, we recruited 51 participants and they were randomly assigned (by drawing lots) to 1 of 2 groups: the BAL group (n = 26) or the CON group (n = 25). The randomization was conducted by a researcher who did not participate in any aspect of the study. The group assignment was concealed from the assessor but not from the participants and trainers. All patients provided written informed consent before data collection.
Outcome Measures
All the participants were tested at the peak of their medication cycle (ie, within 2 hours after taking their anti-Parkinsonian medications) by a physiotherapist who was blinded to the group assignments (Figure 1). Demographic data, including gender, age, body weight, and height; fall history; PD duration; severity of PD as measured using a modified Hoehn and Yahr (HY) staging score 21 ; the participants’ level of physical activity as determined by a metabolic equivalent (MET) questionnaire 22 ; and participants’ cognitive status as quantified by the Mini-Mental State Examination score were recorded. 19 In addition, the participants’ daily levodopa dosages were recorded at each assessment interval.
The primary outcome measure was the self-perceived balance confidence level, as measured by the validated Activities-Specific Balance Confidence (ABC) Scale.23,24 The ABC scale has been found to have excellent test-retest reliability (ICC = 0.92-0.99).23,24 Participants were asked to rate their self-perceived balance confidence level from 0 (no confidence at all) to 100 (full confidence) in relation to 16 daily activities, with a higher ABC score indicating a lower level of FoF.
The secondary outcome measures included balance and gait performance. Because our BAL training program emphasized rapid stepping, weight shifting, and leaning over the limits of stability, we used the limit of stability (LOS) test 25 and SLS test to reflect participants’ balance performance. 16 The LOS test, performed using the Smart-EquiTest Balance Master (NeuroCom International Inc, Clackamas, OR), assesses an individual’s ability to initiate voluntary weight shifting to various spatial positions within the base of support without losing stability. Movement velocity and end point excursion were used, with a higher movement velocity and a longer end point excursion indicating better LOS performance. 25 All participants had 1 practice trial, followed by 1 test trial. The SLS test examines an individual’s ability to maintain equilibrium during a transition from a large base of support (both feet) to a small base of support (1 foot). We recorded time-to-loss-of-balance (TimeLB) in seconds with a stopwatch. Timing commenced when the participant’s foot left the ground and stopped if the participant’s foot touched the ground or when the participants reached 30s. 16 The participants had 1 practice trial followed by 2 test trials, and the mean values were used for data analysis. When participants obtained a mean TimeLB of 30 s, they were regarded as having no loss of balance for the SLS test. Self-selected gait velocity (cm/s) and stride length (cm) were recorded using a 5-m instrumented and computerized GAITRite walkway (CIR Systems Inc, Havertown, PA). The participants had 1 practice trial followed by 3 test trials, and the mean values were used for data analysis. All the outcome measures were taken 1 week before the intervention (Pre), immediately after treatment completion (Post), and 3 months (Post3m) and 12 months (Post12m) after treatment completion.
Interventions
The patients in both groups (BAL and CON) received training for 12 weeks, with 2 phases of 4-week laboratory-based training separated by 4 weeks of home-based training. The 8-week laboratory-based training was supervised by a physiotherapist and administered at a frequency of 3 sessions per week. Self-supervised home-based training was performed at a frequency of 5 sessions per week.
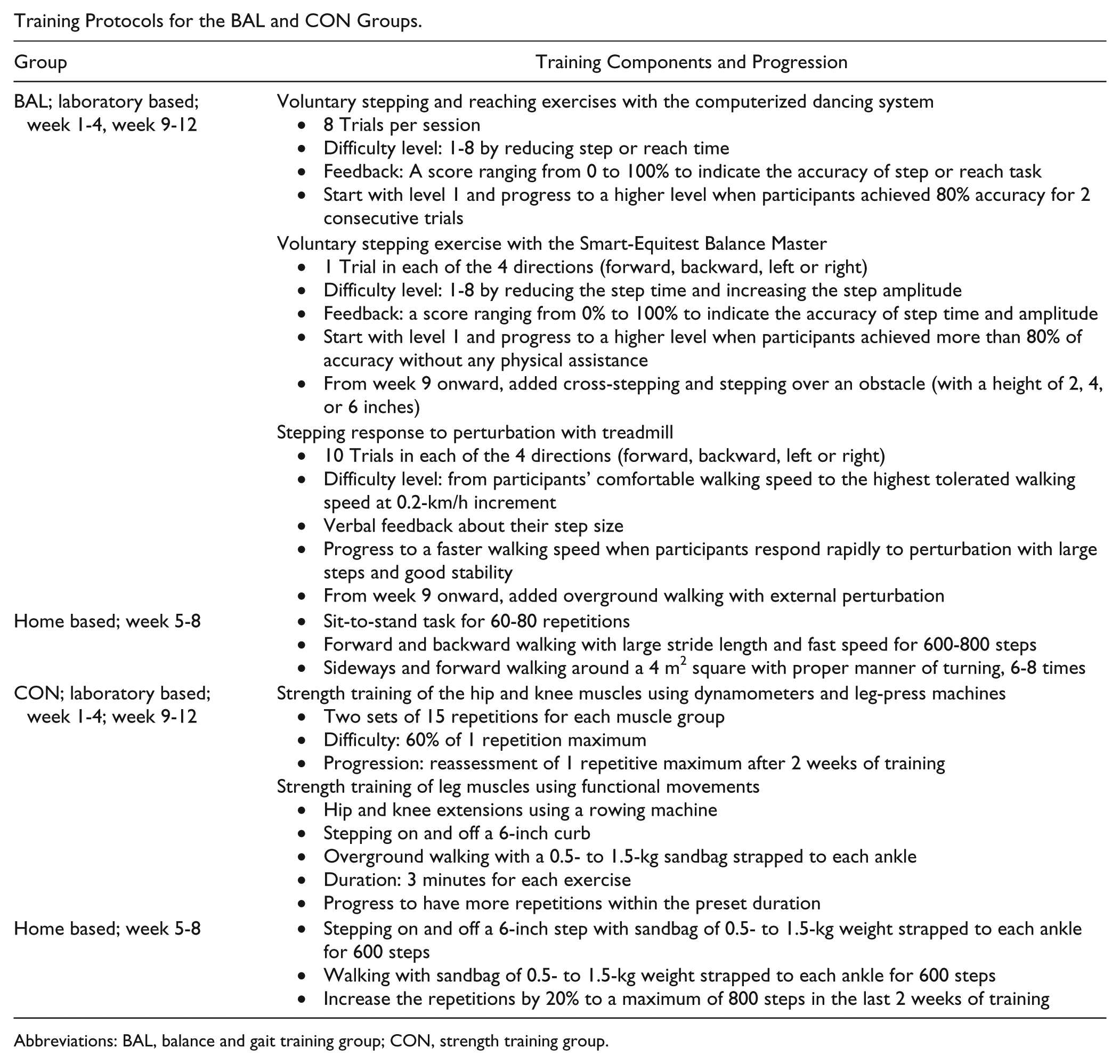
The balance training was designed to focus on enhancing participants’ anticipatory postural adjustment by initiating rapid and large steps and forward reaching, in addition to responding to expected perturbation. 26 Please refer to the appendix for details. A computerized dancing system (KSD Technology Co Ltd. Shenzhen, China) was used to train the step and reaching tasks. The machine features dancing software, a computer, a pressure-sensitive carpet, and 2 light-sensitive rods. The light-sensitive rods were located in front of the participants and on their right and left sides at the longest distance that the participants could reach safely from a standing position. The participants were instructed to stand in the middle of the carpet and to look at the computer screen. In response to visual cues indicating the forthcoming task (ie, either stepping or reaching) and the direction of the action (forward, backward, left, or right for stepping and left-forward or right-forward for reaching), the participants had to perform the correct task in the correct direction at the preset speed. Feedback on the accuracy of the performance after each set of training was indicated by a score ranging from 0% to 100%. On reaching an 80% accuracy level, the speed of the visual cues would be increased for progression. The training session lasted for 15 minutes. Training to increase step amplitude was provided with the use of the Smart-EquiTest Balance Master (NeuroCom International Inc, Clackamas, OR). The participants were instructed to stand on one end of a 45 cm × 150 cm force plate and to look at the computer screen, which displayed a red cursor. When the color of the cursor changed from red to yellow, the participants had to rapidly take a large step and stay in the stride-stance position until the color of the cursor returned to red, at which point the participants could return to their original starting position. The position of the cursor on the screen determined the step amplitude and direction (forward and backward, cross forward and backward, straight left and right, and cross left and right). Feedback on the performance after each set of training was indicated by a score ranging from 0% to 100%. When the participants achieved a score of 80%, the difficulty level would be increased by increasing the step amplitude and speed, changing the stepping pattern from straight to a cross direction and requiring that the participant step over an obstacle. This training lasted for 15 minutes.
Training for the response to external perturbation during walking was performed on a treadmill. The participants stood on the treadmill belt, wearing a harness for safety, and were instructed to walk in 1 of 4 directions maintaining their stability while taking a big step on the sudden starting and stopping of the treadmill belt.26,27 Verbal feedback was given after each trial, and the speed of the treadmill was progressively increased if the participants responded rapidly to perturbation with large steps and good stability. In the last 4 weeks of laboratory-based training, participants practiced overground walking along a 50-m corridor in addition to treadmill-based training. The participants were perturbed by a physiotherapist in different directions and instructed to maintain their stability and continue walking. The participants typically completed gait training in about 30 minutes. The whole laboratory-based training session lasted 60 minutes. During the 4-week home-based training, the participants in the BAL group practiced fall-prone activities, including sit-to-stand and walking and turning in 4 directions, with an emphasis on speed, amplitude, and stability. Each of the home-based training sessions lasted for 20 minutes.
The participants in the CON group received training that emphasized improving the strength of the hip (flexion, extension, and abduction) and knee (flexion and extension) muscles using dynamometers and leg-press machines at 60% of 1 repetition maximum and 2 sets of 15 repetitions in each session. In addition, participants engaged in rowing exercises on a rowing machine stepped onto and off of a 6-inch curb and walked with 0.5- to 1.5-kg sandbags strapped to each lower extremity to improve the strength of the hip, knee, and ankle muscles. For these exercises, the participants were required to complete each exercise within 3 minutes. The duration of each CON training session was 60 minutes. The 4-week home-based CON training consisted of stepping and walking with a 0.5- to 1.5-kg sandbag strapped to each lower extremity. Each home-based training session lasted 20 minutes. The details of the training programs and the progression of both the BAL and CON groups are shown in the appendix.
Data Analysis
Data were analyzed with the Statistical Package for Social Sciences (SPSS, version 17.0). The data normality of the variables was evaluated using the Shapiro-Wilk test. Demographic variables with normal distribution were analyzed with independent t tests to examine the group differences. χ2 tests were used to compare the nominal variables, including gender and fall history. For outcome measures, gait velocity and stride length had normal distributions and were analyzed by 2-way repeated-measures analysis of variance (ANOVA) to examine the treatment effect with time (Pre, Post, Post3m, and Post12m) as a within factor and with groups (BAL and CON) as a between factor. In the case of an interaction being found for the 2-way repeated-measure ANOVA, post hoc t tests and 1-way repeated-measure ANOVA were used to determine the significant between- and within-group differences, respectively. For ABC score and LOS performance without normal distribution, Wilcoxon tests were used to analyze the treatment effects in each group and the Mann-Whitney U test to analyze the group differences at each assessment interval. Bonferroni correction was used in multiple comparisons. For the SLS test, survival analysis with the Kaplan-Meier log-rank χ2 test was conducted to explore between-group differences in TimeLB and no-loss-of-balance events. We defined participants without a loss of balance during the 30-s SLS test as censored participants. 28
An intent-to-treat approach was used for all the analyses. The participants who completed the 12-week training and participated in at least 2 assessments (ie, Pre and Post) were included in the data analysis. The last observation was carried forward for participants who dropped out during the follow-up evaluations. The significance level was set at P < .05.
Results
Four participants in the BAL group and 2 in the CON group did not complete the 12-week training. During the follow-up periods, 1 participant in the BAL group dropped out at the Post3m assessment, whereas 3 participants in the BAL group and 6 in the CON group dropped out at the Post12m assessment. The reasons for each dropout are presented in Figure 1. Using the intent-to-treat rule, the data from 45 participants (BAL = 22, CON = 23) were analyzed in the present study.
Table 1 indicates that there was no significant difference between the BAL and CON groups with respect to the demographic data, PD duration, severity of PD indicated by HY staging score, physical activity level, cognitive status, or fall history. For daily levodopa dosage, there was no significant difference between the participant groups at each assessment interval. For exercise compliance, BAL participants completed 0.8 more treatment sessions than the CON group during the laboratory-based training period. No group difference was found for exercise compliance during the home-based period. Table 2 shows no significant difference between participants who completed the full 12-month study and those who dropped out for all demographic characteristics and outcome measures at baseline, except physical activity level (nondropouts: 3.4 ± 0.3; dropouts: 3.0 ± 1.1; P < .05).
Participant Characteristics. a
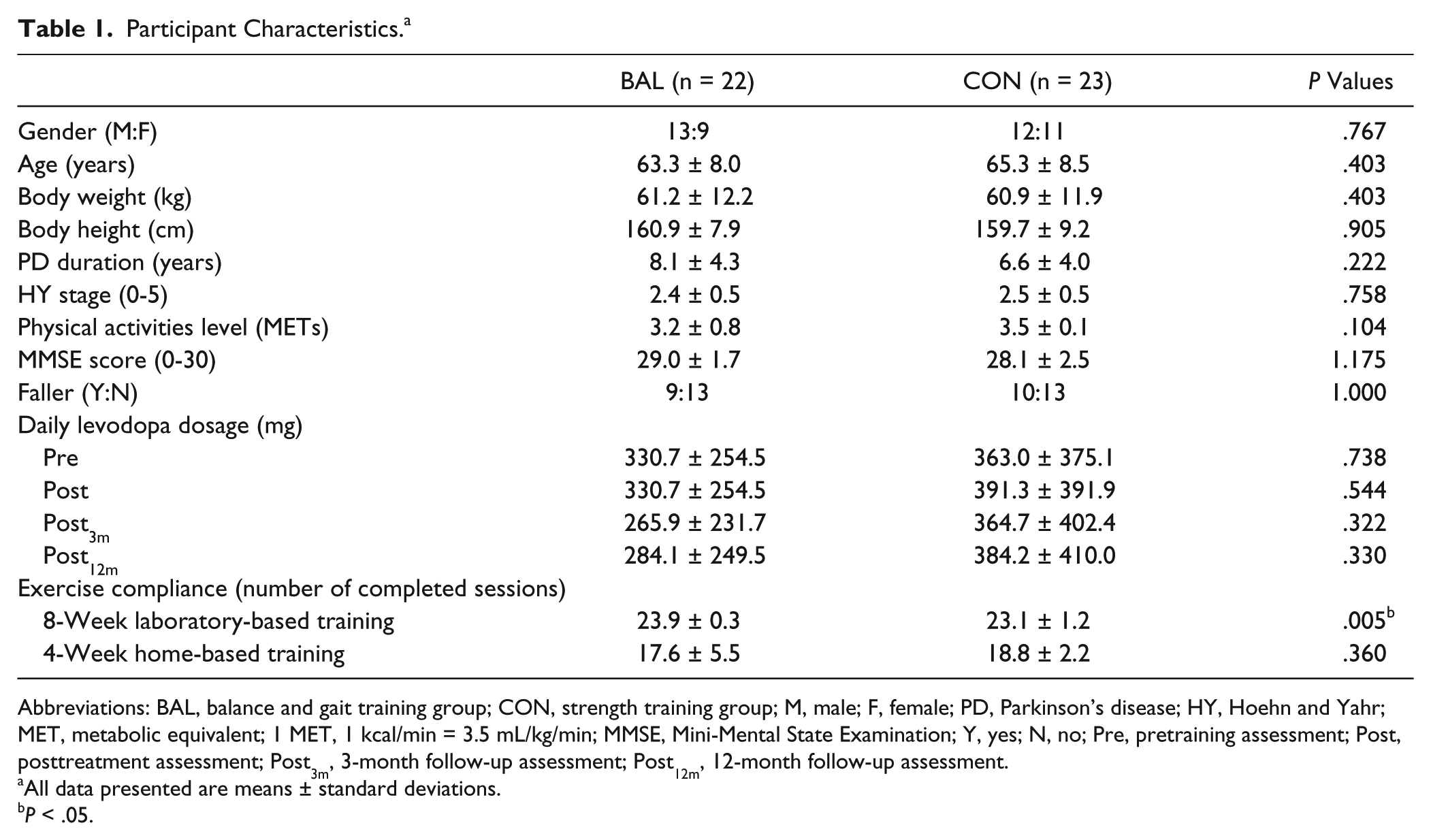
Abbreviations: BAL, balance and gait training group; CON, strength training group; M, male; F, female; PD, Parkinson’s disease; HY, Hoehn and Yahr; MET, metabolic equivalent; 1 MET, 1 kcal/min = 3.5 mL/kg/min; MMSE, Mini-Mental State Examination; Y, yes; N, no; Pre, pretraining assessment; Post, posttreatment assessment; Post3m, 3-month follow-up assessment; Post12m, 12-month follow-up assessment.
All data presented are means ± standard deviations.
P < .05.
Comparison of Demographic Characteristics and Outcome Measures at Baseline Between the Participants Who Dropped Out From the Study (Dropouts) and the Participants Who Did Not Drop Out (Nondropouts). a
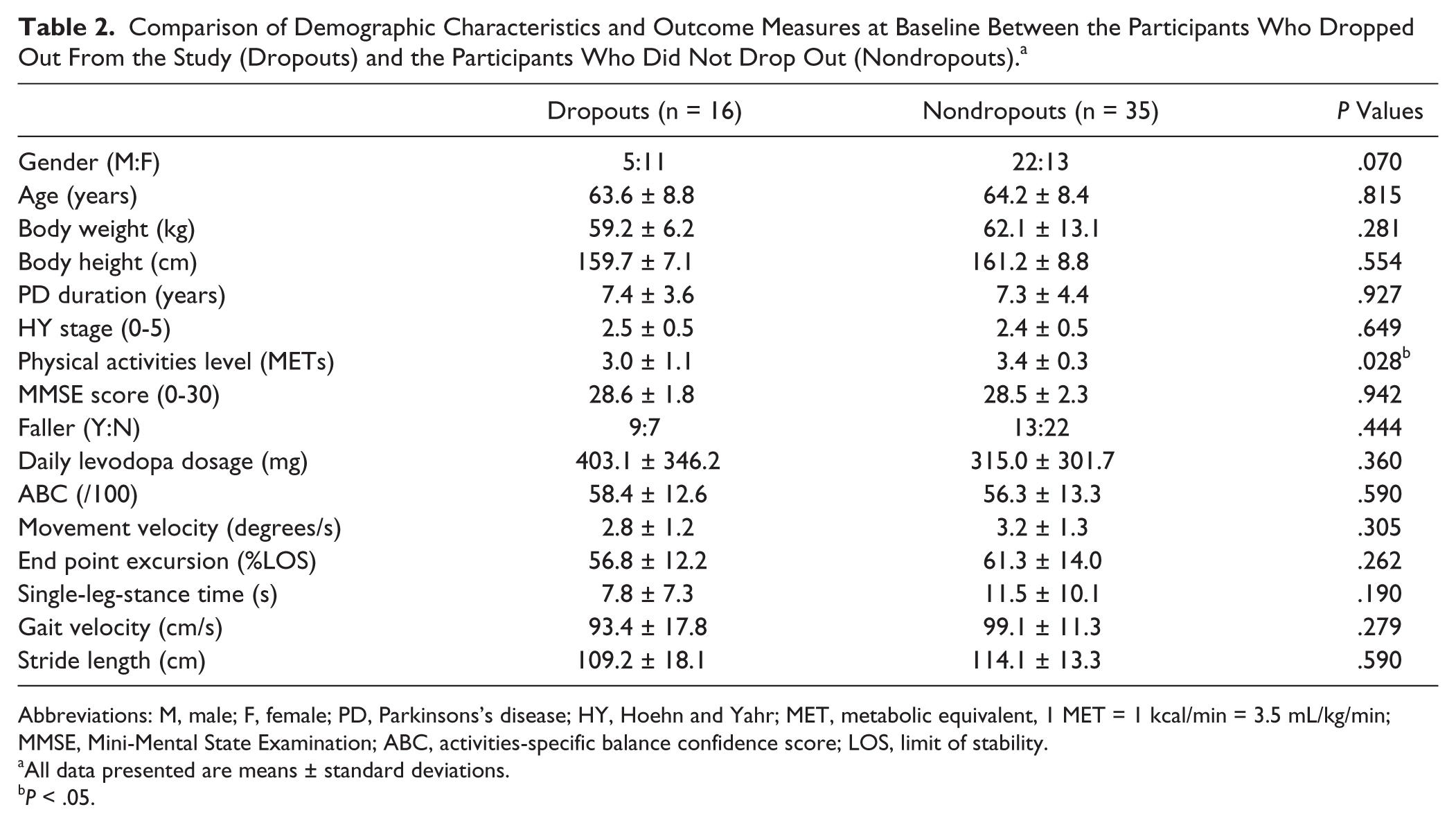
Abbreviations: M, male; F, female; PD, Parkinsons’s disease; HY, Hoehn and Yahr; MET, metabolic equivalent, 1 MET = 1 kcal/min = 3.5 mL/kg/min; MMSE, Mini-Mental State Examination; ABC, activities-specific balance confidence score; LOS, limit of stability.
All data presented are means ± standard deviations.
P < .05.
Short-Term Effects
Table 3 shows the effects of training in the intervention and CON groups. There were no significant differences in the baseline test scores between the 2 participant groups. Regarding the primary outcome of the balance confidence level, the ABC score marginally increased only in the BAL group (by 6%; P = .025, Table 3) immediately after the treatment. For balance performance, both participant groups significantly increased their end point excursion at Post (BAL by 9% and CON by 14%; P < .017, Table 3). BAL participants had longer TimeLB than CON participants but comparable no-loss-of-balance events as CON participants at Post (Table 3, Figures 2A and 2B). For gait performance, both participant groups significantly increased their gait velocity at Post (BAL by 7% and CON by 9%; P < .017). There was a significant Group × Time interaction in the stride length, and only BAL participants significantly increased their stride length at Post (by 13%; P < .017, Table 3).
Between-Group Comparisons of Outcome Measures in ABC, LOS, and Gait Test and Survival Analysis for the SLS Test. a
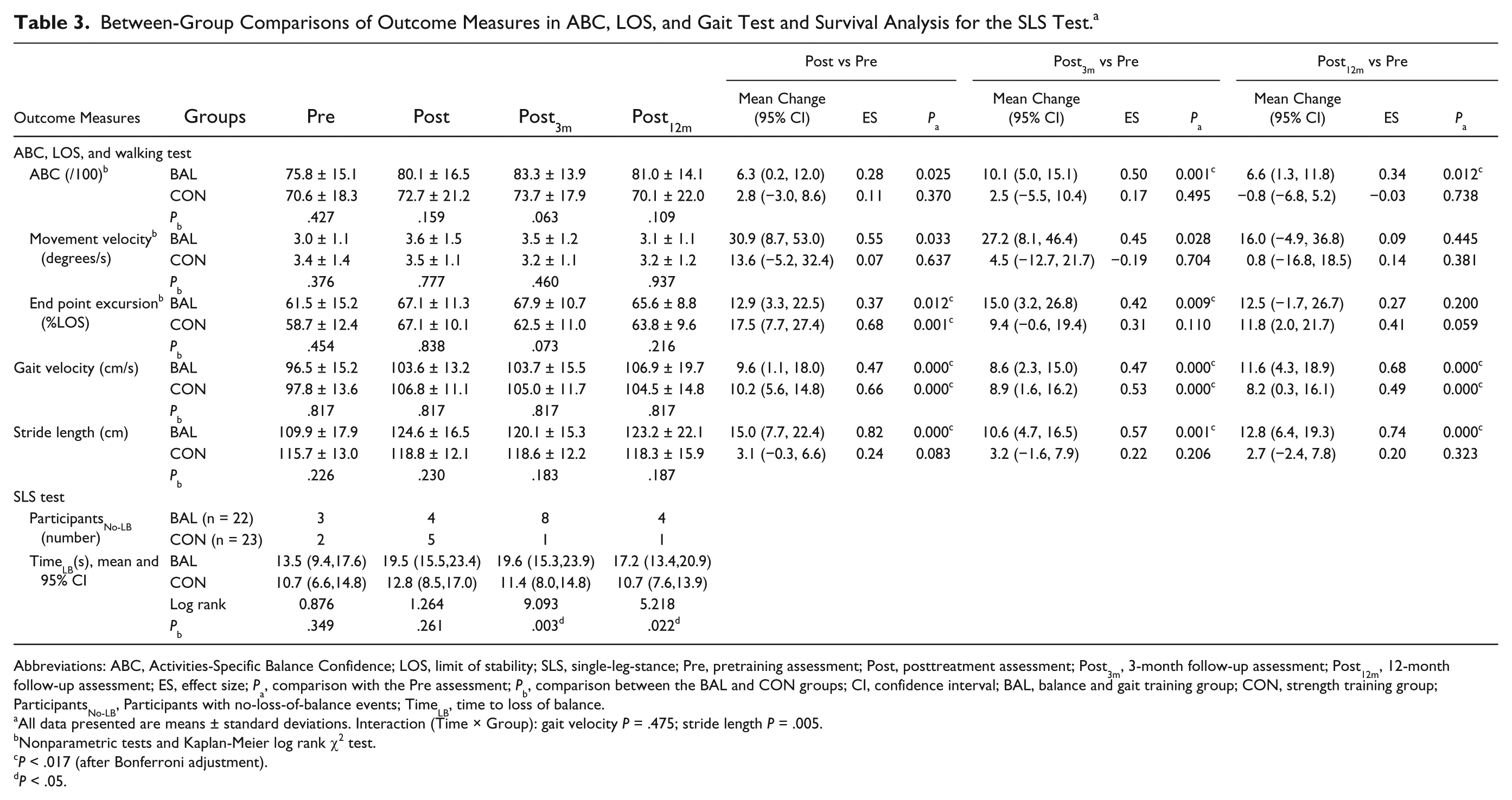
Abbreviations: ABC, Activities-Specific Balance Confidence; LOS, limit of stability; SLS, single-leg-stance; Pre, pretraining assessment; Post, posttreatment assessment; Post3m, 3-month follow-up assessment; Post12m, 12-month follow-up assessment; ES, effect size; Pa, comparison with the Pre assessment; Pb, comparison between the BAL and CON groups; CI, confidence interval; BAL, balance and gait training group; CON, strength training group; ParticipantsNo-LB, Participants with no-loss-of-balance events; TimeLB, time to loss of balance.
All data presented are means ± standard deviations. Interaction (Time × Group): gait velocity P = .475; stride length P = .005.
Nonparametric tests and Kaplan-Meier log rank χ2 test.
P < .017 (after Bonferroni adjustment).
P < .05.
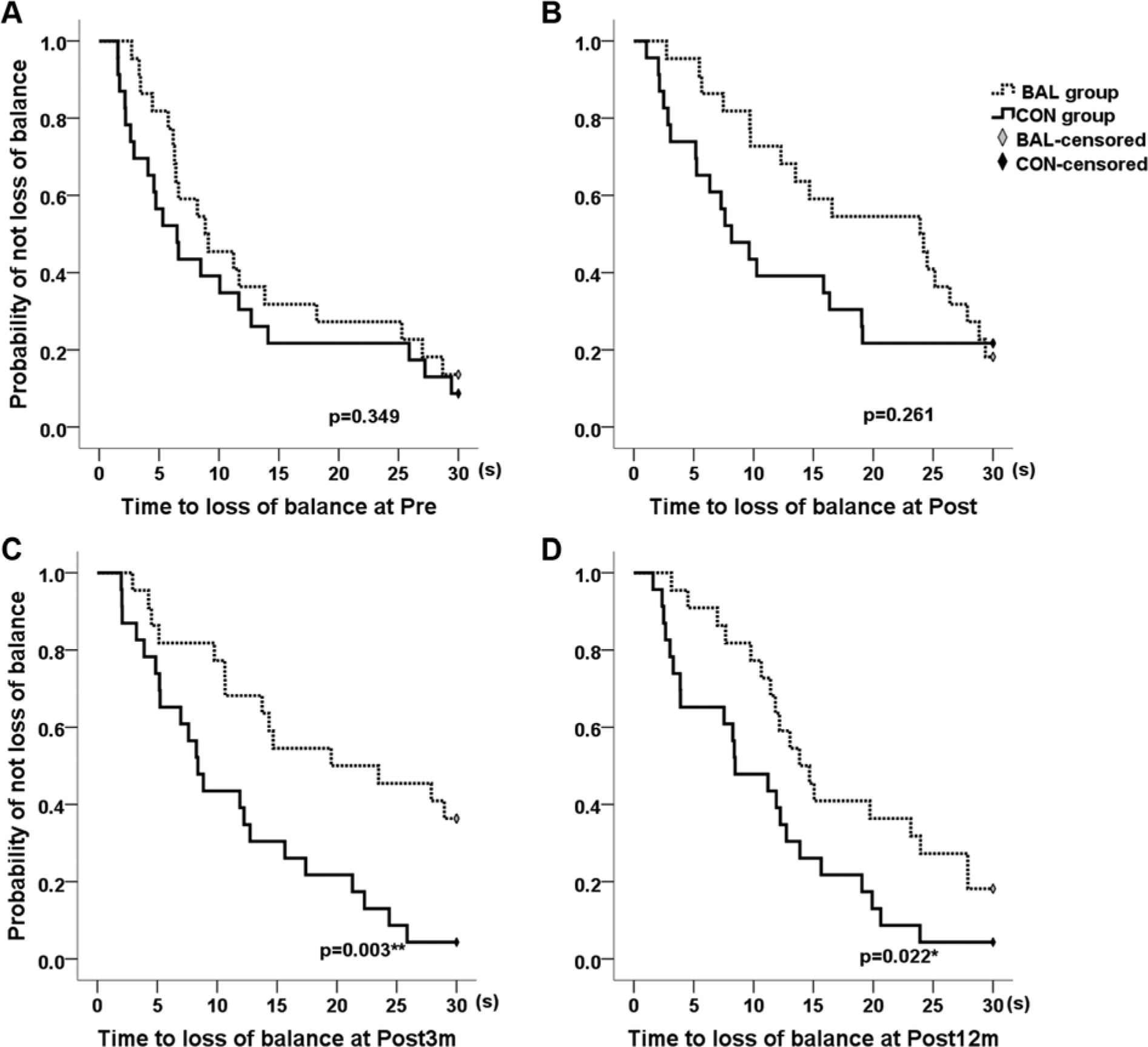
The Kaplan-Meier estimates of survival time to loss of balance in the single-leg-stance test for BAL and CON groups at (A) pretraining assessment (Pre); (B) Posttreatment assessment (Post); (C) 3-month follow-up assessment (Post3m); (D) 12-month follow-up assessment (Post12m).a
Long-Term Effects
At the 3- and 12-month follow-ups, only BAL participants significantly increased their ABC scores, compared with the baseline values (P < .017, Table 3). The ABC scores increased by 10% at Post3m and by 7% at Post12m (P < .017). In addition, there was a marginal between-group significant difference at Post3m, with BAL participants achieving higher ABC scores than those in the CON group (83.3 ± 13.9 vs 73.7 ± 17.9, P = .063). For balance performance, only BAL participants maintained their increase of end point excursion (by 10%; P < .017). BAL participants had significantly longer TimeLB and more no-loss-of-balance events during the SLS test than CON participants at Post3m and Post12m (P < .05; Table 3, Figures 2C and 2D). For gait velocity, both participant groups maintained their gains at Post3m and Post12m (P < .017). However, for the stride length, only BAL participants maintained their improvements at Post3m (by 9%) and Post12m (by 12%; P < .017, Table 3).
Association Between ABC Score and Balance and Gait Performance
Table 4 illustrates the association between ABC score and balance performance and gait variables for participants in the BAL group. The ABC scores were moderately correlated with gait velocity (r = 0.414-0.594), stride length (r = 0.403-0.523, Table 4), and movement velocity at Post3m and Post12m (r = 0.395-0.402).
Associations Between ABC Score and Variables of Balance and Gait Performance in the BAL Group.
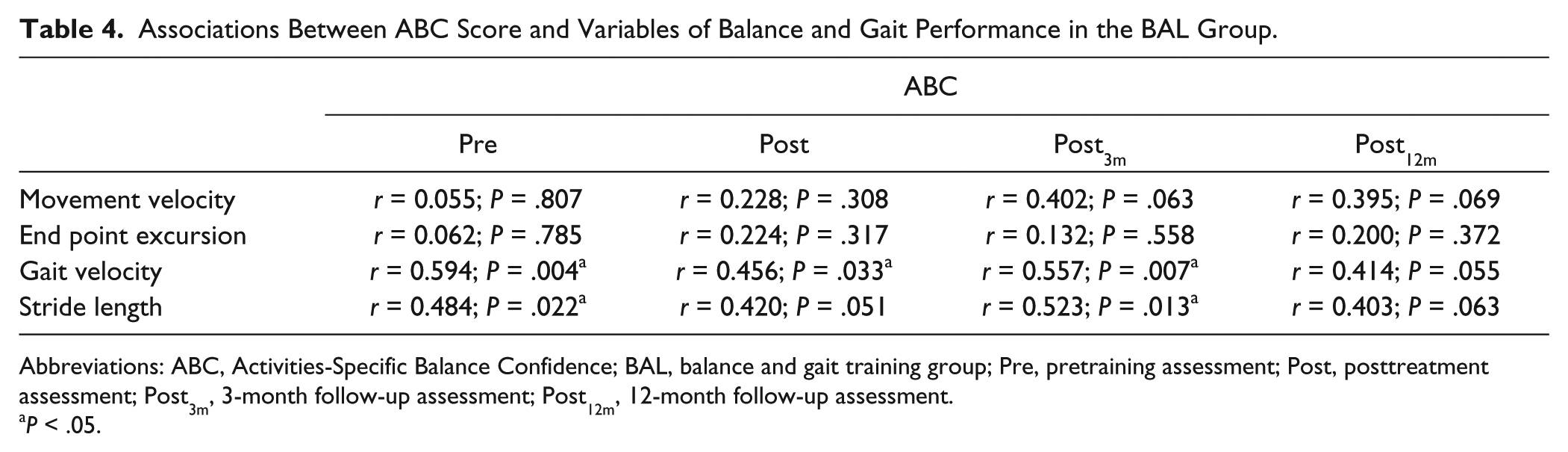
Abbreviations: ABC, Activities-Specific Balance Confidence; BAL, balance and gait training group; Pre, pretraining assessment; Post, posttreatment assessment; Post3m, 3-month follow-up assessment; Post12m, 12-month follow-up assessment.
P < .05.
Discussion
To the best of our knowledge, this is the first study to show that 12 weeks of BAL with augmented feedback led to a marginally significant increase in self-perceived balance confidence level in people with PD, which further increased to a significant level at 3 and 12 months after treatment ended. Our positive findings support the use of BAL in enhancing balance confidence in people with PD.
According to Bandura, 29 performance accomplishments, verbal persuasion, and emotional arousal are essential elements in enhancing self-perceived balance confidence. Our balance training protocol emphasized rapid stepping to promote participants’ stability during a change in the size of the base of support, leaning to enhance anticipatory postural adjustment and stability limits,9,26 and response to external perturbation during treadmill-based gait and step training.12,26,27 With intense practice, the BAL participants progressed to perform volitional stepping from slow to fast speeds and from small to large amplitudes in a stable manner, gaining a larger stability limit and responding to perturbation in a timely and stable manner when walking. In addition, the BAL participants were given a score indicating their performance after each set of training using the dancing system and balance master. Individuals with PD have been found to be more responsive to reward-based learning.30,31 This positive knowledge of results could have aroused positive emotions in the BAL participants to accomplish more postural challenges and achieve a higher confidence level.
The most intriguing finding is that BAL participants continued to increase their balance confidence after treatment completion and sustained this improvement for a duration of 12 months. The positive feedback may have motivated the BAL participants to comply with the training during and beyond the training period. In addition, the blended laboratory- and home-based training encouraged the participants to apply their learnt postural control strategies to their daily functions by performing fall-prone activities—that is, sit-to-stand transfer, stepping, walking, and turning at different directions. This ability to safely transfer learnt strategies from the laboratory to their daily lives could have increased the participants’ confidence level. Given the improvement in their walking skills and balance self-efficacy, participants could have attempted more challenging activities in the community, which might help them to maintain their balance confidence, even 12 months after treatment completion.
Our BAL participants significantly increased their ABC score by 7.5 (10%) at 3 months after treatment completion. The magnitude and the effect sizes of improvement in the ABC score of our BAL participants are comparable to those found by Smania et al 9 at their 1-month follow-up assessment. However, the change of ABC score in our BAL participants is less than the minimal detectable change value (ABC score = 13). 32 The minimal detectable change could vary according to PD severity level, means, and standard deviations (SDs) of the ABC score. Steffen and Seney 32 recruited participants with HY stage 1 to 4, with ABC scores of 70 ± 19. Our BAL participants had HY stage 2 to 3, a higher mean ABC score, and a smaller SD (75.8 ± 15.1). These may lead to smaller but significant changes in Post3m and Post12m. Although the ABC changes are modest, the carryover of its improvement to a duration of 12 months is novel and important. An ABC score >80 has been shown to be associated with a significant reduction of fall risk (odds ratio = 0.06) in PD participants. 6 Our BAL participants had an ABC score of 81.0 at Post12m, together with improvement in balance and gait performance, and their fall risk may be reduced after training.
Previous studies reported associations between balance confidence and objective balance and gait measures.2,16,17 We only established a moderate correlation between ABC score and gait performance. Walking is the most common fall-prone activity,1,5 and the ability to safely perform fall-related daily activities could have increased participants’ confidence levels. 33 The insignificant association between changes in balance confidence and balance performance concurs with previous studies in older people.34,35 We found that the posttreatment increases in the movement velocity (by 20%) and TimeLB (by 44%) were larger than that of the ABC score (7%-10%). A disparity between self-perception and physiological performance may lead to excessive FoF, maladaptation, and needless restriction of mobility and participation. 36 Our findings suggest that both physiological and perceived level of balance performance have to be included to evaluate the effectiveness of fall prevention programs in people with PD.
Interventions such as rhythmic, posturography-based, or dance-based step training37-40; LOS training using Tai Chi 41 ; and compensatory step and gait training using a treadmill12,14 have been shown to enhance balance and gait performance. Our balance training protocol covered all the above-mentioned components and reported increases in maximum excursion, gait velocity, and stride length immediately after 12 weeks of training, a finding that concurred with previous findings.9,12,14,37,39-41 Our BAL participants further maintained their increased maximum excursion and stride length for 3 months, which agreed with the findings of a 48-week Tai Chi training trial. 41 Results of the survival analysis of the SLS test showed that BAL participants had significantly more no-loss-of-balance events and only BAL participants maintained their increased TimeLB at Post3m and Post12m. Furthermore, only the BAL participants maintained their gains in stride length for 12 months. To our knowledge, this is the first study reporting on the longest carryover effect of a balance training program. The long retention after training can be attributed to the inclusion of rapid and large steps and the narrowing of the base of support during standing and walking. 42 Our results support the idea that motor learning is possible in people with PD. 43
The participants in our CON group adopted the training protocols of previous studies,13,44,45 which focused on enhancing the muscle strength of PD patients’ lower extremities. Lower-extremity muscle weakness has been associated with reduced dynamic stability 46 and slowed gait speed.47-49 This could explain the immediate postintervention improvements in the maximum excursion, SLS time, and gait speed, along with the 12-month carryover effect of the gait speed. Despite these improvements, there was no change in balance confidence level, as in previous studies. 13 Motor skill learning is context based; thus, the benefits of strength training alone may not transfer into the safer performance of daily functions. Hence, there was no change in balance confidence level.
This study had several limitations. First, the drop-out rate from baseline to 12 months was moderate at 31% and comparable to 24% to 43% reported in other long-term studies in older persons.50-53 Most dropouts occurred between the 3- and 12-month follow-up periods, and the dropouts had significantly lower baseline physical activity levels than nondropouts (ie, MET = 3.0 ± 1.1 vs 3.4 ± 0.3). Those who had more functional impairment might be less willing to return for reevaluations during the follow-up period. 54 Apart from physical activity level, the nondropouts and dropouts had similar baseline demographic and outcome measures. Although the data have to be interpreted with caution, the dropout of individuals may not substantially affect our results. Second, the sample size was small, and all the participants were community-dwelling with a mild to moderate disease level. Therefore, the results cannot be generalized to patients with advanced-stage PD or those who have been institutionalized. Third, we did not include cognitive behavior training to educate the participants about safe behavior. 55 Fourth, all the participants were examined during their “on” medication period, such that the findings were relevant to their daily functioning. However, testing both “on” and “off” phase is recommended to eliminate the confounding effects of medications. Fifth, we did not report the training effects on gait freezing, fall rate, and other nontraining balance tasks as measured by the Tinetti test 56 or miniBESTest. 57
To conclude, both strength training and BAL using augmented feedback increase stability limits, SLS time, and gait speed immediately after treatment. Only BAL using augmented feedback produced immediate and 12-month carryover effects on enhancing balance confidence, SLS time, and stride length. The positive findings from this study form a scientific basis for formulating treatment interventions that enhance both balance performance and confidence in people with PD. Further work is required to establish the relationship between restoring balance confidence and preventing future falls in the PD population.
Footnotes
Appendix
Training Protocols for the BAL and CON Groups.
| Group | Training Components and Progression |
|---|---|
| BAL; laboratory based; week 1-4, week 9-12 | Voluntary stepping and reaching exercises with the computerized dancing system 8 Trials per session Difficulty level: 1-8 by reducing step or reach time Feedback: A score ranging from 0 to 100% to indicate the accuracy of step or reach task Start with level 1 and progress to a higher level when participants achieved 80% accuracy for 2 consecutive trials |
| Voluntary stepping exercise with the Smart-Equitest Balance Master 1 Trial in each of the 4 directions (forward, backward, left or right) Difficulty level: 1-8 by reducing the step time and increasing the step amplitude Feedback: a score ranging from 0% to 100% to indicate the accuracy of step time and amplitude Start with level 1 and progress to a higher level when participants achieved more than 80% of accuracy without any physical assistance From week 9 onward, added cross-stepping and stepping over an obstacle (with a height of 2, 4, or 6 inches) |
|
| Stepping response to perturbation with treadmill 10 Trials in each of the 4 directions (forward, backward, left or right) Difficulty level: from participants’ comfortable walking speed to the highest tolerated walking speed at 0.2-km/h increment Verbal feedback about their step size Progress to a faster walking speed when participants respond rapidly to perturbation with large steps and good stability From week 9 onward, added overground walking with external perturbation |
|
| Home based; week 5-8 |
Sit-to-stand task for 60-80 repetitions Forward and backward walking with large stride length and fast speed for 600-800 steps Sideways and forward walking around a 4 m2 square with proper manner of turning, 6-8 times |
| CON; laboratory based; week 1-4; week 9-12 | Strength training of the hip and knee muscles using dynamometers and leg-press machines Two sets of 15 repetitions for each muscle group Difficulty: 60% of 1 repetition maximum Progression: reassessment of 1 repetitive maximum after 2 weeks of training |
| Strength training of leg muscles using functional movements Hip and knee extensions using a rowing machine Stepping on and off a 6-inch curb Overground walking with a 0.5- to 1.5-kg sandbag strapped to each ankle Duration: 3 minutes for each exercise Progress to have more repetitions within the preset duration |
|
| Home based; week 5-8 |
Stepping on and off a 6-inch step with sandbag of 0.5- to 1.5-kg weight strapped to each ankle for 600 steps Walking with sandbag of 0.5- to 1.5-kg weight strapped to each ankle for 600 steps Increase the repetitions by 20% to a maximum of 800 steps in the last 2 weeks of training |
Abbreviations: BAL, balance and gait training group; CON, strength training group.
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: The study was supported by S. K. Yee Medical Foundation (5-ZH61) and Hong Kong Parkinson’s Disease Foundation (5-ZH76).