
Abstract
Background. Light touch with a stable object reduces postural sway by increasing axial postural tone in healthy subjects. However, it is unknown whether subjects with Parkinson’s disease (PD), who have more postural sway and higher axial postural tone than healthy subjects, can benefit from haptic touch. Objective. To investigate the effect of light and heavy touch on postural stability and hip tone in subjects with PD. Methods. Fourteen subjects with mid-stage PD and 14 healthy control subjects were evaluated during quiet standing with eyes closed with their arms (a) crossed, (b) lightly touching a fixed rigid bar in front of them, and (c) firmly gripping the bar. Postural sway was measured with a forceplate, and axial hip tone was quantified using a unique device that measures the resistance of the hips to yaw rotation while maintaining active stance. Results. Subjects with PD significantly decreased their postural sway with light or heavy touch (P < .001 vs arms crossed), similarly as control subjects. Without touch, hip tone was larger in PD subjects. With touch, however, tone values were similar in both groups. This change in hip tone with touch was highly correlated with the initial amount of tone (PD, r = −.72 to −.95; controls, r = −.74 to −.85). Conclusions. The authors showed, for the first time, that subjects with PD benefit from touch similarly to control subjects and that despite higher axial postural tone, PD subjects are able to modulate their tone with touch. Future studies should investigate the complex relationship between touch and postural tone.
Keywords
Introduction
It is well known that haptic touch or light touch with a stable object reduces postural sway in young1-3 and elderly subjects 4 as well as in patients with peripheral neuropathy, 5 vestibular loss, 6 and stroke. 7 Yet it is unknown whether subjects with Parkinson’s disease (PD) can benefit from haptic touch to improve postural instability, one of PD’s cardinal symptoms. Understanding the benefits of light touch during standing or walking may have significant implications in rehabilitation for the use of walking aids (eg, cane, walking sticks, walker) 8 and development of strategies to enhance stability and prevent falls.
Haptic sense combines cutaneous and kinesthetic (proprioceptive) inputs, and numerous studies have observed haptic and kinesthetic deficits in both the early and mid-stages of PD,9-16 along with difficulties in integrating somatosensory information.15,17,18 These difficulties in processing somatosensory information might reduce the stabilizing effect of light or heavy touch with a stable object. During light touch contact, when forces applied are physically inadequate to stabilize the body, cutaneous cues from the fingertip and proprioceptive arm inputs are important in providing sensory feedback to reduce postural sway.2,3,16 Nevertheless, the neural mechanism that mediates this effect is controversial. Correlations among body sway, fingertip shear forces, and postural muscle activity suggest that a feedforward activation of postural muscles based on fingertip shear force is involved in stabilizing postural sway during light touch. 16 We recently observed a relationship between postural stability and axial postural tone during haptic touch suggesting that touch decreases postural sway because of increased axial postural tone due to a change in earth-stable reference frame. 1 With our unique “Twister” device, axial hip tone can be measured while subjects actively maintain equilibrium during stance.1,11,19,20 We have shown a significantly increased hip tone during both light and heavy touch of a stable object in young healthy controls. In addition, we found that the subjects’ perception changed with the touch condition. Without touch, subjects wrongly perceived that their trunk rotated in space when, in fact, it was their feet that were rotated. During the light or heavy touch condition, these same subjects correctly perceived their feet rotation. 1 Thus, reduced postural sway was associated with significant increases in axial tone and perception of motion consistent with the central nervous system changing from using a global reference to a local, trunk reference frame for the control of posture during touch.
Since subjects with PD have shown increased axial postural tone,11,19 increased postural sway,21,22 and impaired somatosensory integration,15,17,18 they may also have difficulty modifying their postural tone and sway with touch of a stable surface. In this study, we hypothesized that subjects with PD would not be able to significantly decrease postural sway with light touch because they could not increase their already high axial postural tone.11,19
Methods
Subjects
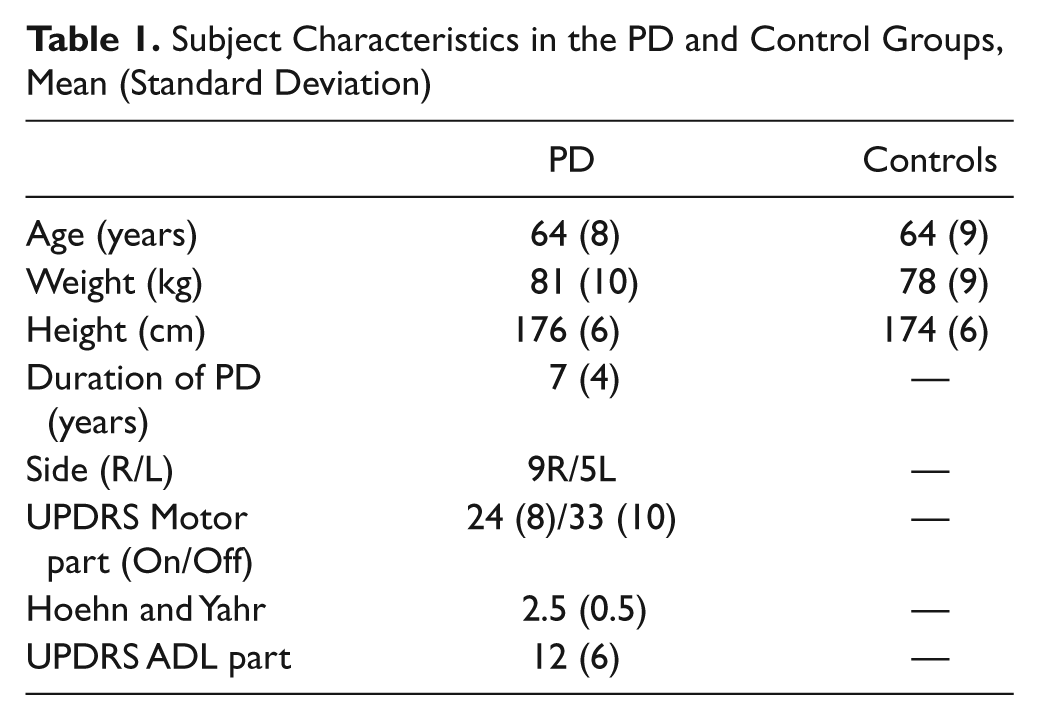
Fourteen healthy male control subjects (64 ± 9 years) and 14 male subjects (64 ± 8 years) with a clinical diagnosis of “idiopathic” PD, treated with levodopa, participated in the study. The subjects were matched for age, weight, and height. PD subjects’ characteristics are presented in Table 1, and more details are available in Franzén et al. 19 None of the subjects with PD had a history suggesting “atypical” PD symptoms, as defined by Hughes et al, 23 or other existing neuromuscular disorders, including severely stooped posture. Subjects with PD with a Hoehn and Yahr score of 2 or 3 were included. The healthy control subjects did not present with recent or unresolved history of musculoskeletal, neuromuscular, or motor disorders. All subjects participating in our study could stand independently for at least 10 minutes. All subjects provided informed consent in accordance to the Oregon Health & Science University Internal Review Board regulations for human subjects studies and the Helsinki Declaration.
Subject Characteristics in the PD and Control Groups, Mean (Standard Deviation)
Protocol
The subjects with PD were assessed “off” medication (OFF), the morning after abstaining from levodopa overnight (washout period ≥12 hours). The measurement of postural sway and axial tone at the hips was first assessed in 3 different touch conditions: no touch (NT), light touch (LT), and heavy touch (HT). Then, the motor part of the UPDRS 24 was administered after which PD subjects took their usual morning dose of levodopa medication. During the following rest period (1 hour), the subjects rated themselves on activities of daily living (ADL) as part of the UPDRS 24 and on the Activities of Balance Confidence scale, 25 to quantify activity limitations and balance confidence. Once the subjects with PD reported feeling “on” (PD ON, ~60 minutes after levodopa intake), the same postural sway, tone, and UPDRS measurements were repeated, starting with the motor part of the UPDRS. The large decrease in UPDRS motor scores (27%, P < .000002) from the OFF state to the ON state clearly indicates that PD subjects were ON levodopa at the time of testing. Control subjects performed all tests only once.
In all 3 conditions (NT, LT, and HT), the subjects stood with eyes closed on a forceplate fixed to the support surface. Axial hip tone was measured by slowly rotating the surface while the hips were fixed to a suspension, which prevents rotation, without restricting horizontal and vertical motion (Figure 1). In each condition, the surface moved clockwise and counterclockwise in relation to the hips, for 4 cycles (1 trial of 4 cycles per condition). In the NT conditions, the subjects were instructed to stand with their arms crossed over their chest. Subjects were instructed to adapt to a natural upright standing position, to relax, and to not resist the platform motion. During the LT condition, the subjects were instructed to lightly touch a stable bar with both index fingers without using the bar to provide support or resisting rotation (Figure 1). During the HT condition, the subjects were instructed to grasp the stabilizing bar with both hands using a palmar grip and comfortably hold on without resisting rotation (Figure 1). Adhesive tape was used to mark the feet location on the platform so that the same position was repeated for each trial. After every complete set of cycles, the subjects were encouraged either to sit or to walk about to prevent fatigue or stiffness. The order of the 3 conditions was randomized and the very first condition, considered a training trial, was rejected from analysis. This condition was later repeated and retained for analysis.
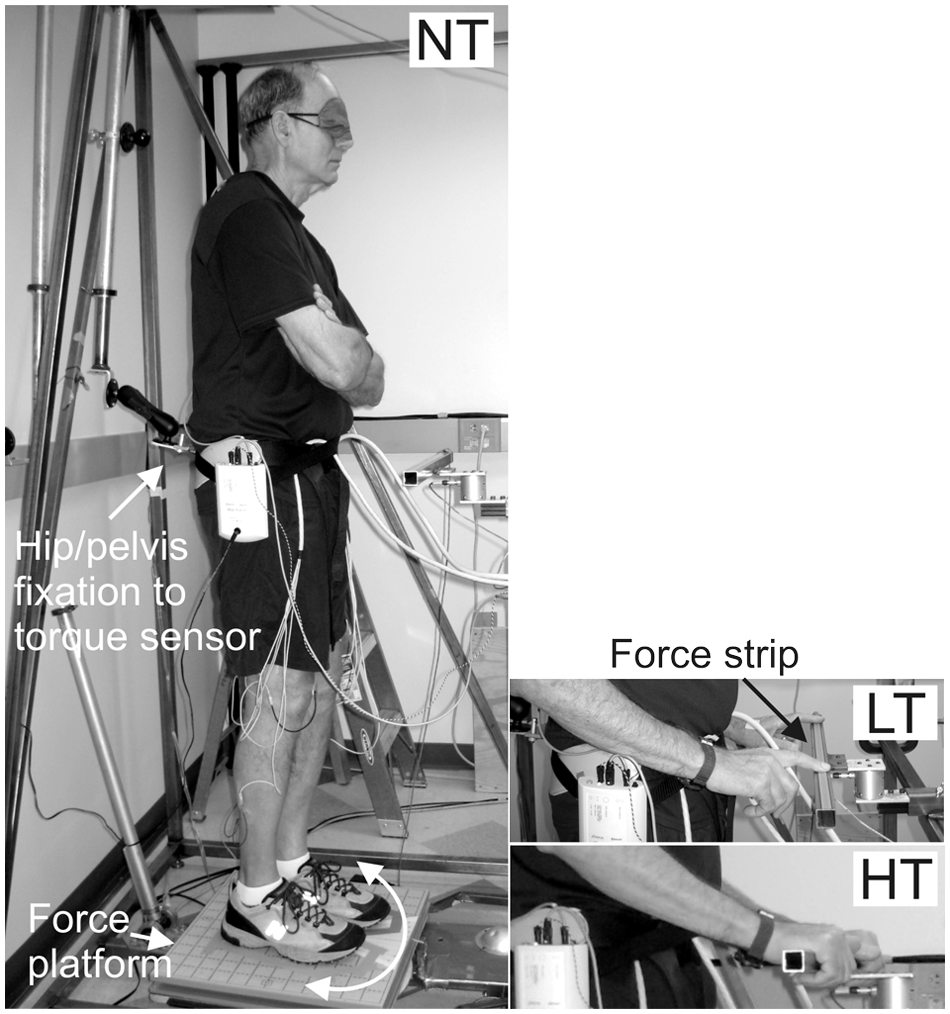
Left: The force platform rotates the feet relative to the fixed hip/pelvis while the torque sensor measures hip resistance/torque during the no touch (NT) condition. Right top: During the light touch (LT) condition, subjects were touching with both index fingers on an adjustable rigid metal bar that was integrated into the external frame of the Twister device. A force sensing strip on the bar beeped if the subjects exceeded the threshold of 2 N. Right bottom: During the heavy touch (HT) condition, subjects were gripping the stabilizing bar with both hands
Measurement of Postural Stability
An AMTI AccuSwayplus force platform (50 × 50 cm; Advanced Mechanical Technology, Inc, Watertown, MA) was integrated into the device measuring hip torque. The force platform measured 3-dimensional forces (Fx, Fy, Fz) and 3-dimensional moments (Mx, My, Mz) to provide the location of the center of pressure (CoP).
Measurement of Axial Tone
Using the Twister device, we quantified axial tone at the hips in all subjects during standing with and without touch. This device is uniquely designed to measure axial torque during active control of postural stability in standing while restricting movement only in axial torsion during yaw twisting. When standing in this device, subjects must use their axial and leg musculature to counteract gravity and to maintain equilibrium, thereby activating their postural tone. As illustrated in Figure 1, subjects stood blindfolded on a horizontal platform that slowly (1°/s) rotated left and right (±10°). The subjects were fixated at the hips with a double-hinged suspension apparatus, preventing only yaw motions in the axial plane and not allowing any support or earth reference in the horizontal or vertical directions. 20 The Twister device provides a repeatable and reliable measure of axial postural tone in healthy individuals1,20 and PD subjects.11,19 In this protocol, torsional strain/resistance was measured about the hips’ yaw axis with a torque sensor (Futek TFF400, Irvine, CA) located between the frame and suspension apparatus, which was attached to a pelvic belt preventing any yaw rotation. A potentiometer signaled the angular position of the platform. The rate of rotation was constant to minimize effects of inertia, except during directional changes where the rotation followed a parabolic trajectory, reducing angular acceleration to <12°/s2 to ensure smooth changes in rotational direction.
For the trials with a touch condition, a 40-cm horizontal rigid metal bar was integrated into the external frame of the Twister (Figure 1). This adjustable stabilizing bar was positioned at waist height in front of the subject at a comfortable distance from the body midline for touching with elbows flexed at approximately 90°. During the LT condition, subjects touched the bar with the tip of their 2 index fingers, and during the HT condition, they grabbed the bar with both hands. A force sensing strip (Interlink Electronics, Camarillo, CA, Part No. 408) mounted on the bar and coupled to a circuit with an adjustable threshold beeped if the subjects exceeded the threshold of 2 N (200g) as negative feedback for the LT condition. Only 2 PD subjects exceeded the threshold and the trials were rejected and repeated. One of those subjects needed to perform the LT condition with the left index finger only because of severe tremor in the right hand. This subject was unable to control the pressure with the right hand or maintain it on the bar.
The resistive torque of the hips and force platform data were recorded at 100 Hz using Spike2 software (Cambridge Electronic Devices, Cambridge, UK) and analyzed offline using Matlab software (Mathworks, Natick, MA).
Data Analysis
Postural sway was measured from the displacement of the CoP during 2 to 4 cycles and cropped into the respective cycle and averaged. Motion of the CoP was quantified separately in the anteroposterior and mediolateral directions by computing the root mean square (RMS) and the RMS mean velocity. 26 The resistive torque in the hip during HT, LT, and NT conditions was quantified as the mean peak-to-peak amplitude for 2 to 4 cycles from one direction of rotation to the next. The first cycle of rotation was excluded from the analysis of the torsional resistance since that cycle might be affected by the subject’s initial postural set or resting short-range stiffness. 19 Torque asymmetry was analyzed as the difference in average torque during CW rotations and that during CCW rotation. 11
Statistical Analysis
Statistical analysis for both postural stability and hip tone measures consisted of a 2-way analysis of variance (ANOVA) on Group (PD OFF meds vs controls) × Condition (NT, LT, and HT) with repeated measures on the last factor to compare PD subjects with control subjects. To test for the effect of medication in the PD group (ON vs OFF) × the conditions (NT, HT, and LT), an ANOVA with repeated measurement on both factors was used. The significance level was set at P < .01 to adjust for multiple ANOVAs. When significant main effects were found, Tukey HSD was used for post hoc analysis. The Pearson product moment correlation (r) and the coefficient of determination (R2) were used to investigate the relationship between tone during touch (LT or HT) and tone without touch (NT) as well as the relation between tone and sway.
Results
Postural Stability
The groups were matched for age, weight, and height (P > .01). Stabilogram sway data from a representative subject with PD in the OFF state shows how much postural sway amplitude was reduced by both light touch and heavy touch during 30 seconds of stance (Figure 2A). As shown in Figure 2B and C, when lightly touching or gripping the bar, both PD OFF and control subjects significantly decreased their anteroposterior RMS sway amplitude by about 60% and the mediolateral sway by ~45% compared to the no touch condition, F(2, 52) = 113.35, P = .000, and F(2, 52) = 46.73, P = .000, respectively. All subjects benefited equally from the touch or grip condition with no main effect of group, F(1, 26) = 0.26, P = .616, and F(1, 26) = 2.52, P = .124, respectively.
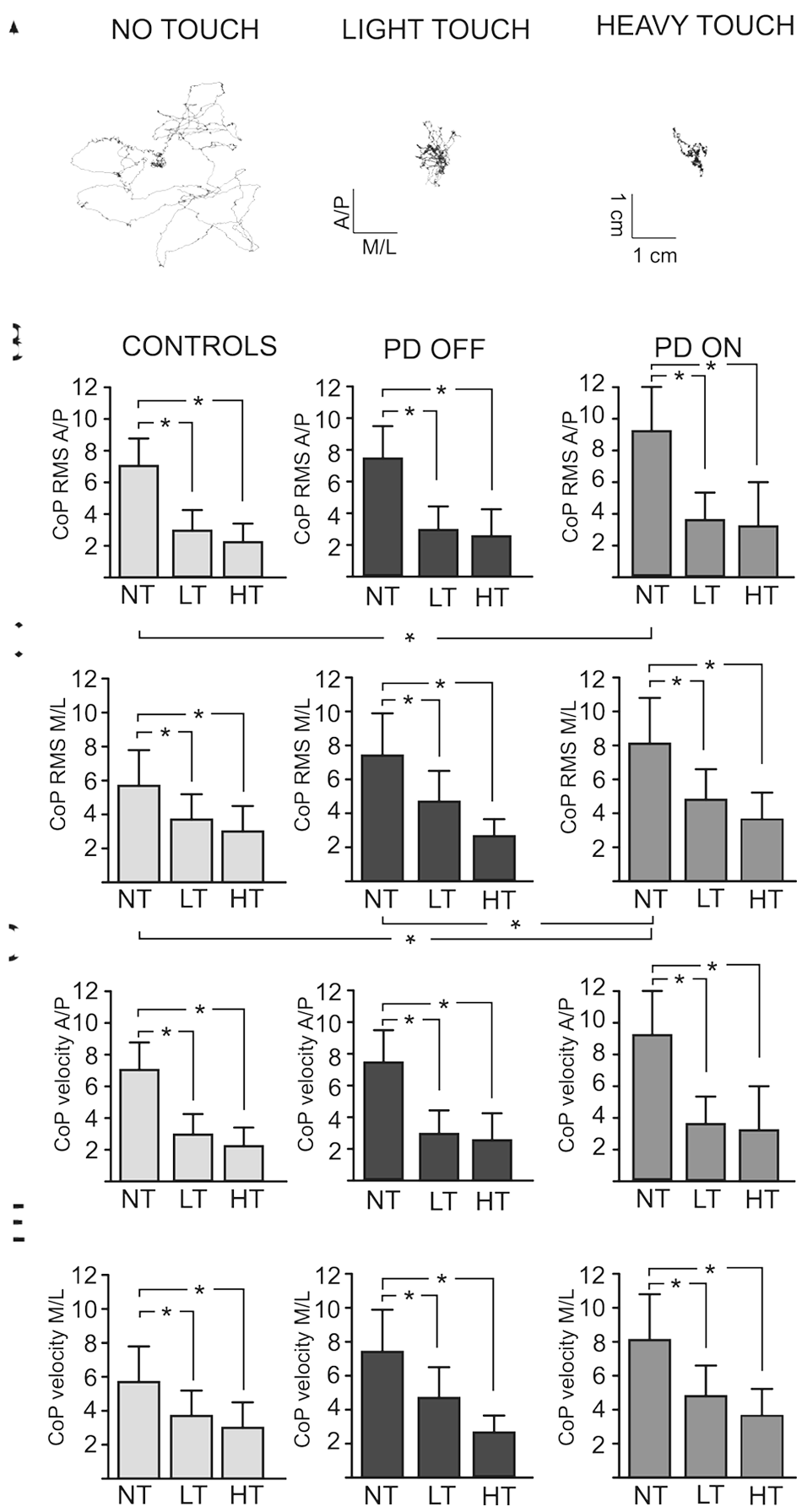
(A) xy-plot of the displacement of the center of pressure (CoP) in both the anterioposterior (A/P) and in the mediolateral (M/L) directions that illustrates the changes in the CoP during light and heavy touch in comparison to the no touch condition in a representative subject with Parkinson’s disease without medication (OFF). (B) The mean and standard deviation of the root mean square (RMS) of the CoP in A/P and (C) M/L directions as well as the CoP velocity in (D) A/P and (E) M/L directions during no touch (NT), heavy touch (HT), and light touch (LT) in age-matched control subjects as well as in subjects with Parkinson’s disease (PD) OFF and ON their medication
When gripping the bar, both PD OFF and control subjects also reduced their sway velocity significantly from the no touch condition in both anteroposterior and mediolateral directions, F(2, 52) = 46.69, P = .000, and F(2, 52) = 33.88, P = .000, respectively (Figure 2C and D). Both groups also benefited from the LT condition by significantly reducing their sway velocity but significantly less than for the HT condition (P = .015 and P = .006, respectively). No main effects of group in either anterioposterior or mediolateral direction were evident, F(1, 26) = 1.03, P = .319, and F(1, 26) = 0.73, P = .404, respectively.
Effect of Dopamine
When subjects with PD were ON levodopa, their sway amplitude (RMS) increased significantly compared to OFF levodopa. The anteroposterior sway amplitude increased by 25% but did not reach significance, F(1, 13) = 6.36, P = .026, whereas the mediolateral sway significantly increased by 15%, F(1, 13) = 9.22, P = .010, ON levodopa. Consequently, with no touch, PD subjects in the ON state, but not the OFF state, showed larger postural sway (RMS in the AP and ML directions) than control subjects (P = .027 and P = .011, respectively). However, the improvement from HT or LT on sway variability, F(2, 26) = 50.36, P = .000, was not affected by the use of levodopa. Sway velocity was not affected by the use of levodopa in either anteroposterior or mediolateral direction, F(1, 13) = 2.10, P = .171, and F(1, 13) = 0.17, P = .688, respectively.
Postural Tone
Overall, the hip postural tone was 16% higher in the PD OFF group than in the control group, but this difference did not reach significance, F(2, 26) = 4.77, P = .038. When touching or gripping the bar, there were no significant group differences in hip tone (PD OFF vs controls, P > .01; see Figure 3).
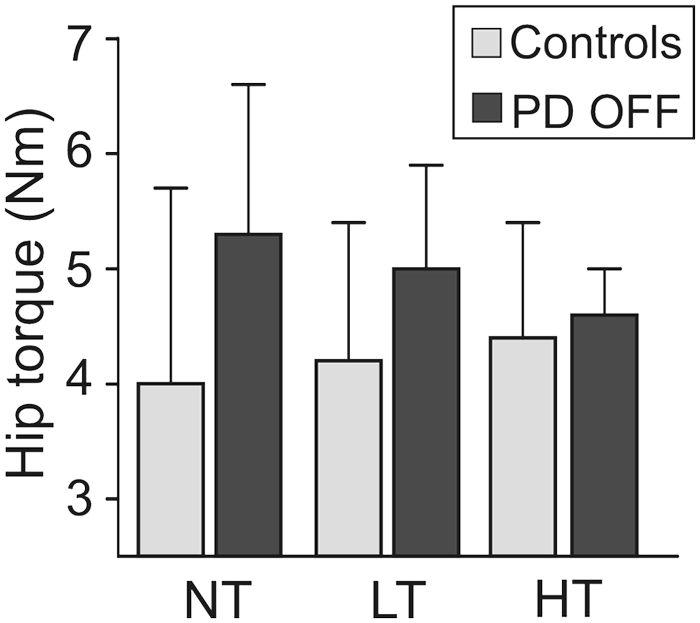
The group main effect, F(2, 26) = 4.77, P = .038, as well as the group mean and standard deviation of the hip resistance to twisting the feet and legs ±10° at 1°/s during no touch (NT), light touch (LT), and heavy touch (HT) in subjects with Parkinson’s disease (PD) OFF their medication and in age-matched control subjects
Figure 4 shows the correlation between the hip postural tone without touch and the percentage change in hip postural tone from NT to LT (Figure 4A) and from NT to HT (Figure 4B). This change in hip tone with touch was highly correlated with the amount of hip tone without touch (PD OFF: LT vs NT r = −.72 and R2 = .52, HT vs NT r = −.95 and R2 = .90; as well as controls: LT vs NT r = −.74 and R2 = .55, HT vs NT r = −.85 and R2 = .72). When touching or gripping the bar, control subjects, who have significantly smaller hip postural tone in the NT condition, increase their hip tone. Alternatively, subjects with PD who generally have higher tone tend to decrease it when touching or grabbing. As illustrated in Figure 4, only small changes in hip postural tone when touching or gripping the bar were observed from subjects (PDs and controls) that had hip tone values near 5 N m (vertical dashed line). The use of levodopa in subjects with PD had no effect on hip postural tone (P > .01) (PD ON: NT = 5.2 ± 1.7 N m, LT = 4.7 ± 1.3 N m, and HT = 4.5 ± 1.0 N m). Furthermore, no difference in torque asymmetry between groups (P = .633) or conditions were found (P = .095).
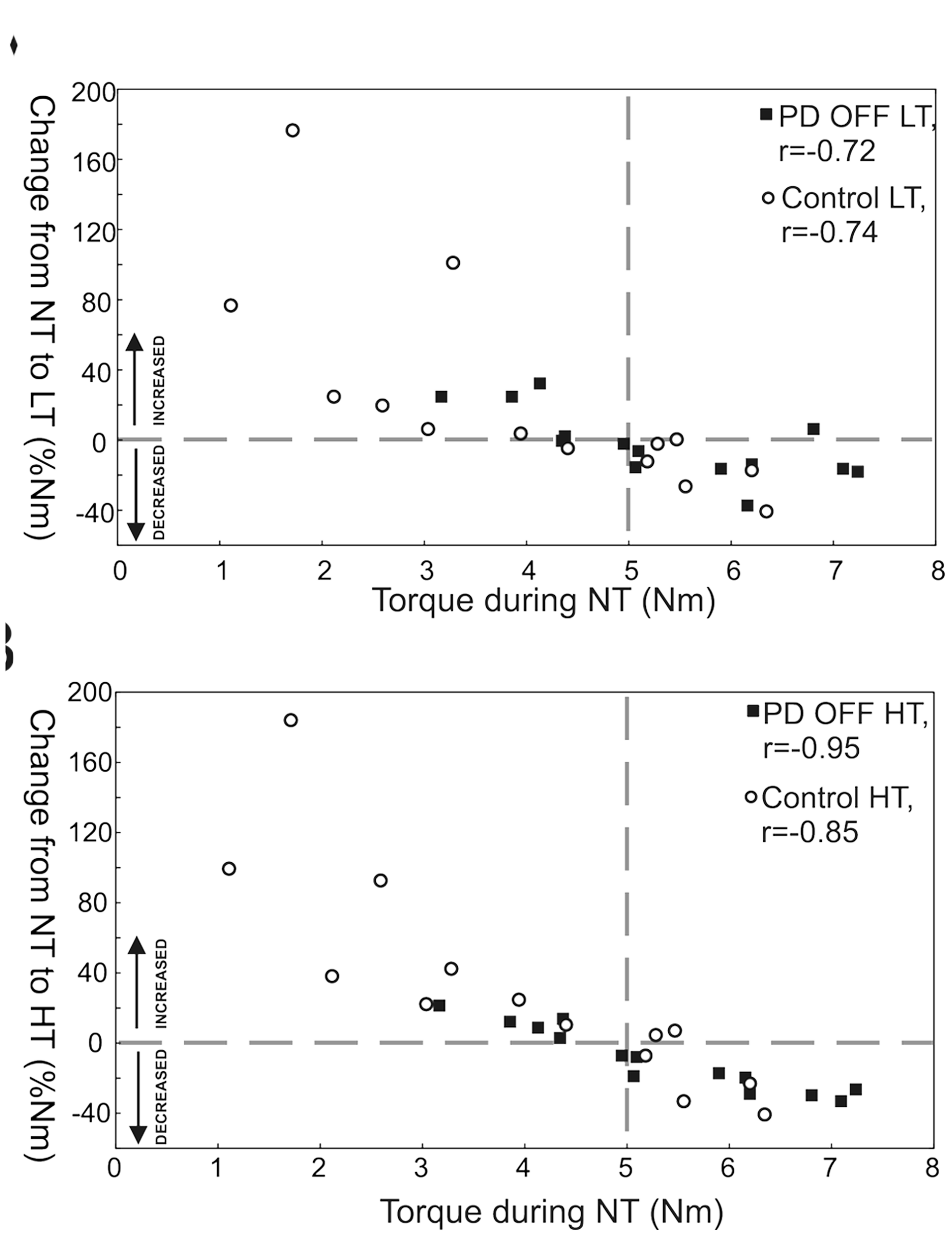
Relation between the hip torque (N m) during the no touch (NT) condition and the percentage change (%N m) in hip torque from the NT condition to (A) the light touch (LT) and (B) the heavy touch (HT) conditions in subjects with Parkinson’s disease OFF medication (PD OFF, black squares) and control subjects (open circles). Above the horizontal dashed line subjects are increasing in hip axial tone during LT or HT in comparison to NT and below subjects are decreasing. The vertical dashed line represents the intersection (approximate 5 N m) between the zero line and the regression lines
Postural Tone and Stability
Our analysis showed a significant correlation between the level of postural hip tone and anteroposterior sway variability in PD subjects (r = .47, R2 = .22). This correlation, however, was not observed in control subjects (r = .00, R2 = .00). While 22% of sway can be explained by hip torque in the PD group, it does not contribute to sway variability in the control group. Analyzing the NT, HT, and LT conditions separately revealed significant correlations between the postural tone and sway variability in the PD group during LT (r = .59, R2 = .35) and HT (r = .61, R2 = .37) but not during NT (r = .40, R2 = .16). There were no correlations in the control group, regardless of the touch condition (NT: r = .29 and R2 = .08, LT: r = −.24 and R2 = .06, HT: r = .24 and R2 = .06). Finally, no correlation between the change in postural tone and the change in sway variability from NT to HT or from NT to LT was observed (PD: r = .02 and R2 = .00, controls: r = .20 and R2 = .04).
The PD group estimated their balance confidence in relation to everyday activities lower as compared to the control group (PD: mean 89, range 61-100; controls: mean 97, range 91-100, P = .005).
Discussion
This study showed, for the first time, that subjects with PD ON or OFF medication significantly improve postural stability with light or heavy touch, a benefit similar to sway reduction observed in control subjects. Reduction in postural sway was associated with reduced axial postural tone, suggesting that tone changes may mediate the effects of light touch on postural stability. PD Subjects Benefit from Haptic Touch Postural sway decreased by ~60% when both subjects with PD and controls lightly touched or gripped a rigid bar during stance on a very slowly rotating surface with eyes closed. The stabilizing effects from touch on postural sway were very similar between light and heavy touch, suggesting that subjects with PD benefit primarily from somatosensory input associated with touch rather than the mechanical support provided by heavy touch.
The effects of light touch are relayed through the somatosensory inputs from the fingertip in combination with whole arm proprioception,2,16,27 providing an additional spatial reference1,27,28 to stabilize posture. Contrary to our hypothesis, subjects with PD significantly reduced their postural sway with touch in a similar way as healthy control subjects. PD subjects benefited from touch to reduce their sway despite previous studies showing deficits in sensing tactile 29 and proprioceptive information9,11-13 as well as in integrating sensory cues.15,17,18 Light touch might act to reduce postural sway like external cues improve motor function in people with PD, via bypassing dysfunctional neural loops with compensatory pathways. External sensory cues, such as auditory, visual, and somatosensory, have been shown to improve motor function in subjects with PD, including improved postural stepping responses and improved gait.30-33 Sensory cuing to improve gait, for example, has been associated with reduced activation of supplementary motor area and basal ganglia pathways and increased function in dorsolateral premotor cortex and cerebellar pathways.34,35
Another explanation to the reduced sway might be that being adjacent to a stable object and thereby having the option to grab on to it, should balance be perturbed, could increase balance confidence and indirectly reduce sway. However, this is less likely since the balance confidence scores in this study were very high in the control group even though they did reduce their sway in the same manner as the PD subjects.
We found that subjects with PD tended to increase sway, as reported in the literature, during NT when ON their medication compared with OFF medication. 22 In fact, deficits in axial kinesthesia 13 as well as proximal proprioception 36 have been observed in subjects with PD using levodopa and could explain the change in sway between OFF and ON medication. On the other hand, when movement ability increases in the ON state, subjects with PD might unconsciously “allow” themselves to sway more than in the OFF state. In the present study, light touch resulted in comparable postural sway when PD subjects were ON or OFF medication and similar to control subjects. These results indicate that touch can attenuate the negative effects of PD and of levodopa on postural sway.
Haptic Input Modifies Axial Postural Tone
This is the first study showing that axial tone might be modified by additional sensory input in subjects with PD. Our previous study 1 in young, healthy adults showed that postural sway decreased as tone increased when touching or gripping a stable bar. Since subjects with PD have high axial tone11,19 and show deficits in processing somatosensory input,15,17,18 we hypothesized that subjects with PD would be unable to modify their tone with haptic touch. In contrast, our results indicated that PD subjects are able to modulate axial tone and generally decrease it.
Most (~65%) of our subjects with PD had higher than normal axial tone during standing without touch (NT) and decreased their tone when touching or gripping the bar. On the other hand, most age-matched control subjects had lower tone during NT and increased hip tone with touch. Interestingly, with touch, both groups reached similar axial tone values of approximately 5 N m. Our previous study showed that an increase in axial tone in young adults during light touch was associated with unmodulated axial muscle activity and reduced variability in the hip torque, reflecting reduced active postural shortening reactions that kept axial tone low. 1 Results from the current study suggest that there is a preferred, or optimal, level of axial hip tone during haptic touch that stabilizes the trunk in space. 37 This level of axial hip tone might be optimal to be able to make postural corrections based on a local trunk reference frame instead of a global reference frame. 1 Consistent with a change in the postural reference frame during light touch, both control and PD subjects reported similar change in perception when touching the bar. As seen in the younger adults, 1 the elderly and PD subjects perceived the relative motion between the legs and the trunk as if the trunk was rotating. With light or heavy touch this sensation changed from trunk to surface rotation.
Despite high levels of axial tone, PD subjects in our study were able to modulate their axial hip tone when touching or gripping a stable bar to a similar level as age-matched control subjects. Unlike previous studies showing that PD subjects with rigidity are unable to flexibly inhibit phasic leg muscle responses to postural perturbations when the support conditions change38,39 or when gripping a stable object, 40 our results imply that remote sensory input can modulate the background tonic postural activity during stance in subjects with PD. This disparity in our results could be due to different structures in the CNS controlling tonic versus phasic postural activity 41 or controlling feedback (postural perturbations) versus feedforward control (postural sway), 42 which might not be affected by the disease in a similar way.
We found that the relationship between postural tone and stability was weaker than we observed in our earlier study in healthy young adults. 1 In that study, 30% of the variance in sway could be explained by the change in tone, while we found no such relationship (R2 = .00) in our current, older control group. A few factors may explain the differences observed in these studies. There is an important age difference (24 years) between these control groups which may explain the larger variance and higher tone values in the current control group. Larger axial hip tone observed in the healthy elderly in the current study might be caused by age-related changes in the muscle properties or in the neuromuscular system, such as co-contraction during stance. 43
If haptic touch can reduce high axial tone and excessive postural sway during quiet stance, this has important implications for rehabilitation. Our results suggest that training programs should encourage the use of assistive devices and touching of stable references in the environment, in addition to other rehabilitation measures.44-46 This combination of strategies may be most important in individuals with high axial tone and severe PD, since postural sway seems to increase with disease severity and duration.21,22
In conclusion, subjects with mid-stage PD with excessive postural sway and excessive axial postural tone benefit from haptic touch. Rehabilitation strategies can draw on this finding to improve functional standing and walking.
Footnotes
Acknowledgements
We thank participants for their time and patience; Triana Nagel, BS, for help with recruitment; Edward King, MS, and Charley Russell, PhD, for assistance with equipment and programming.
Authors’ Note
Caroline Paquette is presently at the Department of Neurology & Neurosurgery, McGill University at SMBD, Jewish General Hospital & Lady Davis Institute, Montreal, Quebec, Canada.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: Supported by NIH R37-AG006457, Center for Health Care Sciences at Karolinska Institutet and Loo and Hans Osterman’s Foundation.