
Abstract
Background. Confidence about balance may be an important factor affecting self-efficacy for daily activities after stroke. Objective. The authors investigated whether confidence changes and the parameters that may predict changes in self-perceived balance within the first year of community reintegration. Methods. In this prospective study, 98 hemiparetic participants who could walk at least 10 m independently were assessed 1, 3, 6, and 12 months postdischarge from rehabilitation by the Berg Balance Scale, Timed Up and Go, 6-minute walking distance, and depression and anxiety scales. The 98 age-/sex-matched controls were assessed at enrollment and the same intervals. Multilevel modeling was used to determine if assessed covariates predicted changes in balance confidence by the Activities-Specific Balance Confidence Scale. Results. Stroke subjects had lower initial balance confidence than controls and showed a statistically significant increase in confidence over 1 year at each assessment. Poor balance and high state anxiety were associated with lower balance confidence. Significant interactions were observed between greater depression, along with more impaired walking capacity and balance tests, in predicting lower change trajectories in confidence. Falls predicted a reduced rate of improvement. Conclusions. Balance confidence after stroke remained lower than controls over the first year. Physical therapies and supportive interventions designed to treat confidence should be initiated at discharge from inpatient rehabilitation.
Introduction
Recovery is ongoing over the first year postdischarge from rehabilitation for individuals who return to the community after stroke. 1 Knowledge about factors contributing to an individual’s recovery may enhance rehabilitation efforts.
Confidence regarding balance may be an important factor contributing to stroke recovery as it has been found to mediate outcomes such as engagement in activities of daily living. 2 Balance confidence is defined as a person’s self-efficacy in executing tasks that challenge that ability. 3 Bandura’s social cognitive theory suggests that self-efficacy has a strong influence on coping efforts and choice of activities and is a strong a predictor of behavior. 4 Individuals living in the community 6 to 12 months after stroke have reduced balance confidence. 5 Poor balance and motor function and decreased walking ability,2,6 history of falls, 7 depression, and being female 8 are associated with reduced balance confidence in individuals with stroke. Reduced confidence may lead to decreased participation in daily and social activities, which, in turn, may result in lower quality of life. To date, no studies have investigated whether balance confidence changes over the first year of recovery in individuals with stroke. Since balance confidence is a relevant rehabilitation outcome and remediable, 9 understanding the natural history of balance confidence could assist in determining the need and timing of interventions for reduced balance confidence, thus enhancing ongoing recovery of individuals with stroke.
The present study investigated whether stroke status predicted change trajectories in balance confidence in individuals with stroke in their first year of community reintegration. Stroke status refers to whether or not an individual has suffered a stroke. Change trajectories reflect patterns of change (ie, linear, quadratic, or cubic). Our primary hypothesis was that balance confidence would remain significantly lower in individuals with stroke than in individuals without a stroke over the 1-year study period. Our secondary hypothesis was that balance confidence would be statistically lower in individuals with stroke than those without a stroke after controlling for important covariates.
Methods
Study Design
This longitudinal study followed individuals with stroke and age-/sex-matched controls with no disability over a 1-year period.
Participants
Entry criteria included a single stroke, residual unilateral lower extremity weakness, and independent walking for a minimum of 10 m. Hemiparetic participants and healthy controls were older than 50 years and English speaking. Exclusions included significant musculoskeletal or neurological conditions other than stroke, residence more than 50 km from the data collection centers, and cognitive or communication impairments. Baseline cognitive status of the participants was screened using the Cognitive Capacity Screening Examination 10 using a cut-point of 15. Stroke subjects were recruited through inpatient rehabilitation units at 5 hospitals in British Columbia and controls were recruited through advertisements in local newspapers and community centers.
Procedures
Participants with stroke were enrolled and assessed within 1 month of discharge from rehabilitation and followed up at 3, 6, and 12 months postdischarge. Controls were evaluated at enrollment and the same intervals. Demographic and stroke characteristics were collected at baseline. This study was approved by the local research ethics board and the local health authorities.
Measures
The Activities-Specific Balance Confidence Scale (ABC) 3 assesses an individual’s confidence in maintaining balance while performing 16 different daily activities. Scores range from 0 to 100 (highest level of confidence). Psychometric properties of the ABC have been established with individuals with stroke. 11 The Berg Balance Scale 12 is a measure of balance performance with scores that range from 0 to 56 (optimal balance). The Berg Balance Scale has been used widely in stroke rehabilitation and is shown to have good psychometric properties. 13 The Timed Up and Go Test was used to measure mobility. The time taken to stand up, walk 3 m, turn around, and return to a seated position was recorded. Evidence supporting reliability and validity of the Timed Up and Go Test has been established in older adults.14,15 The 6-Minute Walk Test (6MWT) 16 was used in this study to measure walking capacity. The farthest distance walked (to the nearest meter) in 6 minutes was recorded. Psychometric properties of the 6MWT have been established in stroke.17,18 The 20-item Center for Epidemiological Studies Depression Scale (CES-D) 19 was used to assess the level of depressive symptoms in the past week. Higher scores indicate increased levels of depressive symptoms with 16 or higher used as a cut-off for depression. 20 The CES-D has been shown to be valid and reliable for stroke patients. 20 The State–Trait Anxiety Inventory for Adults (STAI) 21 was used to measure the level of state anxiety. Scores range from 20 to 80 with higher scores indicating higher levels of anxiety. The STAI has well-established psychometric properties. 22 Finally, the 6-item Interpersonal Support Evaluation List 23 was used to measure perceived support resources; each item is rated on a scale of 0 to 3 with higher scores indicating lower levels of perceived support.
The number of falls the subjects experienced was collected using a monthly fall calendar. Number of falls was classified into 3 categories: no falls, single fall and multiple falls for the statistical analyses.
Stroke characteristic data were extracted from facility medical records. Sociodemographic information (sex, age, partnering status, residence) was collected using study questionnaires. Self-identified chronic conditions and the number of medications taken were also recorded.
Statistical Analysis
A 2-level multilevel model 24 was constructed to determine if stroke status was an important predictor of the change trajectories in balance confidence while controlling for covariates. Multilevel models are mixed-effects models that take into account each individual’s growth trajectory (within person change) and between-person differences in change. 24 The level-1 model describes the within person change and the effects of time varying predictors. The level-2 model describes the between person differences and the effects of time invariant predictors. Variables whose values were significantly different over time were time varying whereas variables whose values remained constant or were not significantly different over time were time invariant. The fixed effects of the output describe the average linear change trajectories, defined by the intercept (initial status) and slope (rate of change), and the average difference in intercept and slope for individuals based on their level-2 predictor values. The random effects describe the residual variance in true intercept and slope across all individuals. We selected a linear change trajectory after examining empirical growth plots and comparing fit statistics (Akaike information criterion and the Bayesian information criterion) of linear, quadratic and cubic growth models. 24 Missing data were treated as missing at random because there were minimal risks that the probability of missing data was related to the unobserved outcomes (Figure 1). 24 Missing data were not imputed, and cases with <2 data points were deleted. 25 All predictor variables were centered on their grand means to facilitate interpretation. 24
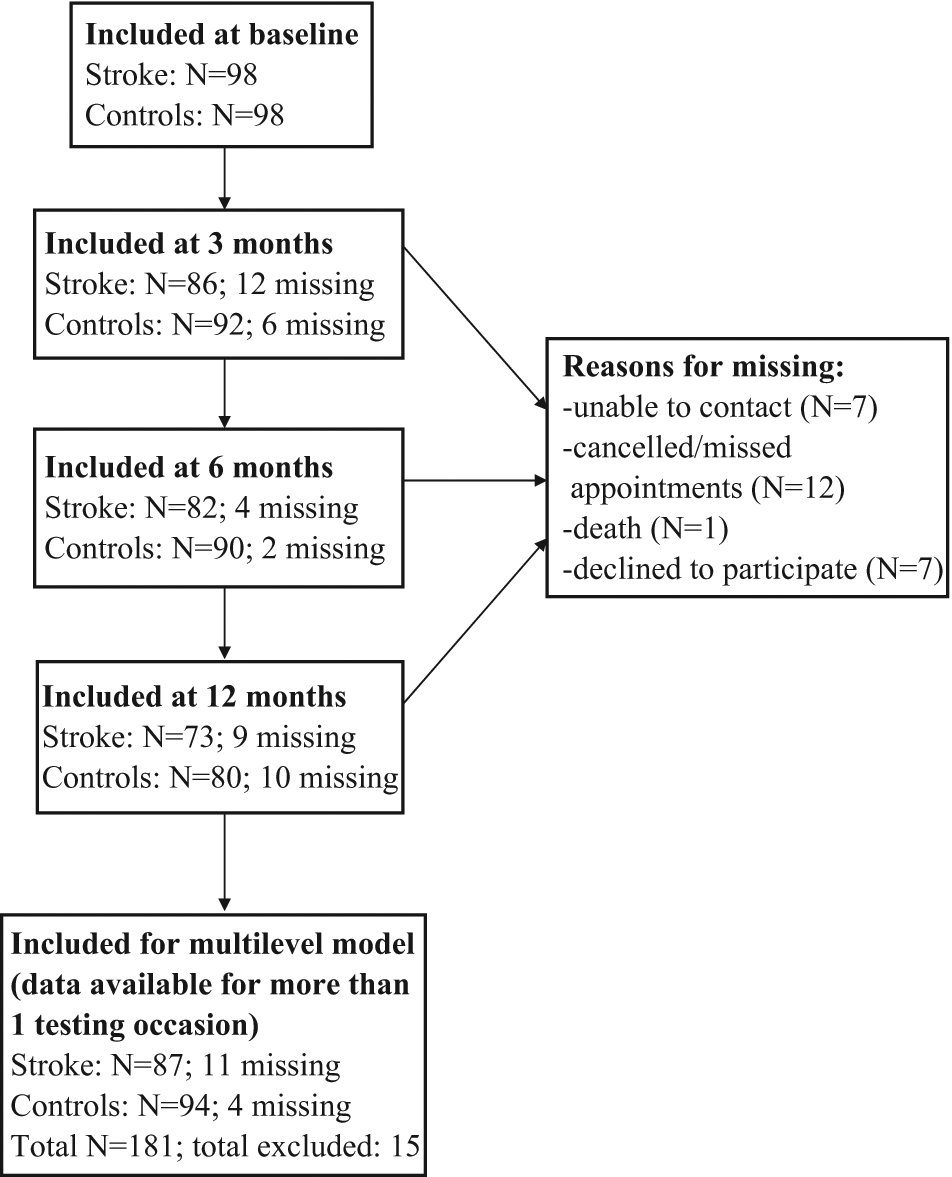
Diagram illustrating participants included at baseline, 3, 6, and 12 months and reasons for missing data.
Longitudinal changes in balance confidence without covariate effects, as well as changes in time varying covariates, were first determined using unconditional growth models. 24 Next, we examined the effect of stroke on changes in balance confidence by including stroke status (individuals with or without stroke), our primary interest, as a time invariant predictor in the level-2 model to create the first conditional multilevel model (model 1). We then included time varying predictors in the level-1 model; nonsignificant residual terms for time varying predictors were fixed to zero in the level-2 model. Other time invariant predictors were included in the level-2 model to create the second conditional multilevel model (model 2). Based on plausibility and prior research, we included interaction terms involving stroke status in the final model. Decisions to retain predictors were also based on comparison of model fit. 24 Deviance statistics were computed and χ2 difference tests were used to test for differences among models. 25 Statistically nonsignificant predictors that did not improve model fit and explain outcome variation were removed. All the analyses were performed using HLM 6.02 software program with level for significance set at P < .05.
Results
A total of 98 individuals with stroke and 98 age-/sex-matched controls participated in the study at baseline. In all, 11 stroke participants and 4 controls were excluded from the analyses because they only provided data from 1 testing session, leaving a total of 181 participants (see Figure 1, which outlines participants included at each testing occasion). Demographic characteristics are shown in Table 1. Significant differences were observed between controls and the stroke sample based on the number of chronic conditions, number of medications, and whether or not they used an ambulatory device.
Demographic Characteristics of Older Adults With and Without a Stroke
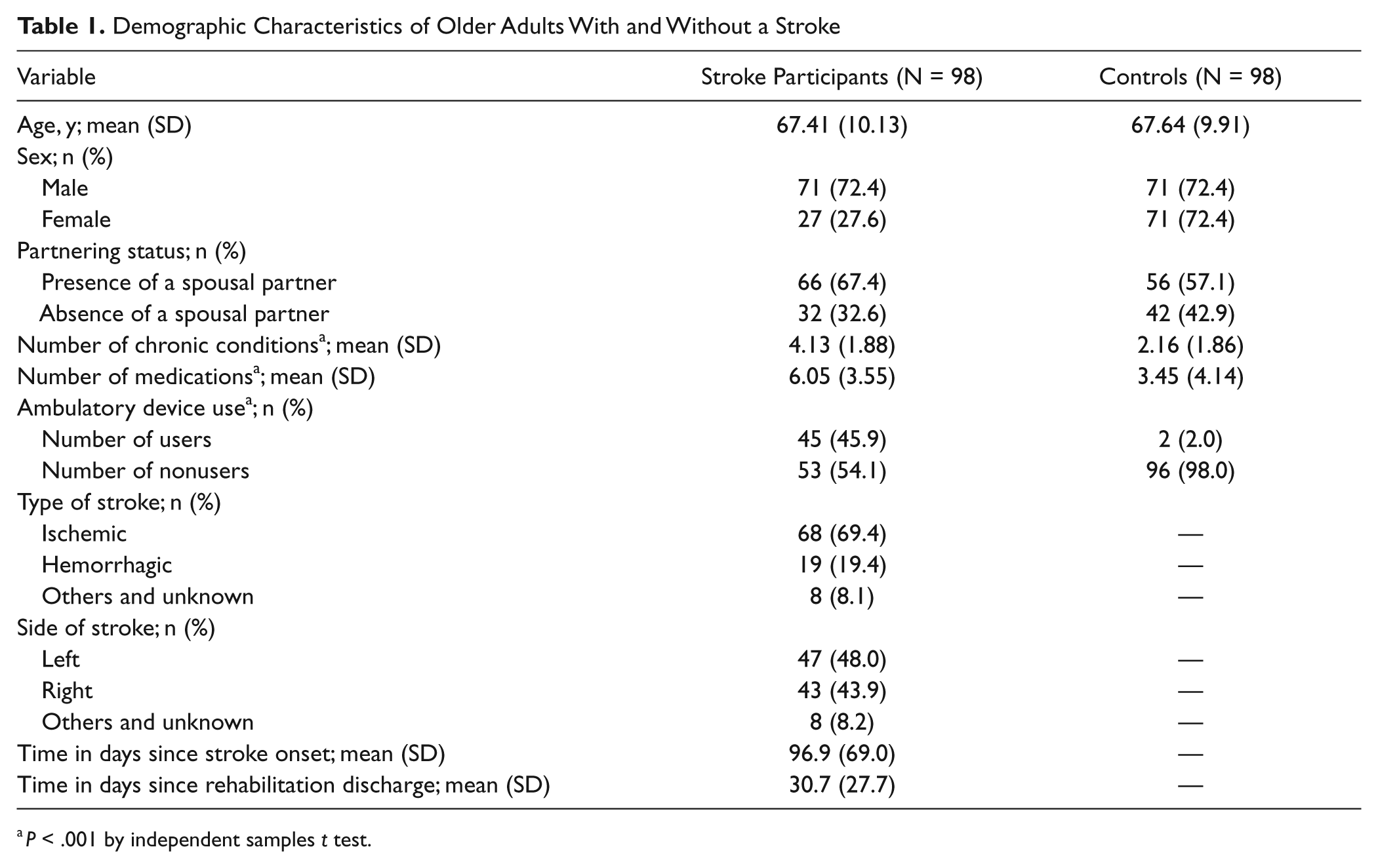
P < .001 by independent-samples t test.
Compared with individuals with stroke, controls had significantly higher balance confidence (mean difference = 32.23 points), better balance performance (mean difference = 9.17 points), better mobility (mean difference = 13.2 seconds), better walking capacity (mean difference = 263.56 m), and lower anxiety state scores (mean difference = 9.95 points). At baseline, controls also had fewer symptoms of depression (mean difference = 8.96 points). All group differences were significant at P < .001. In our sample, 36 individuals with stroke (36.7%) scored at or above the cutoff score for depression on the CES-D at baseline, whereas only 5 controls (5.3%) scored above this cutoff.
Significant changes as determined by the unconditional growth model were observed for balance confidence, mobility, depressive symptoms, anxiety state, and walking capacity over the 12 months (Table 2). There were no significant changes in balance performance and perceived support resources over time; as such, these variables were treated as time invariant and their baseline values were used for the multilevel analyses. When all time varying variables were included in the level-1 model, the residuals terms for Timed Up and Go Test, CES-D, and 6MWT were nonsignificant and were therefore fixed to zero in the level-2 model.
Changes in Balance Confidence and Covariates Over 1 Year
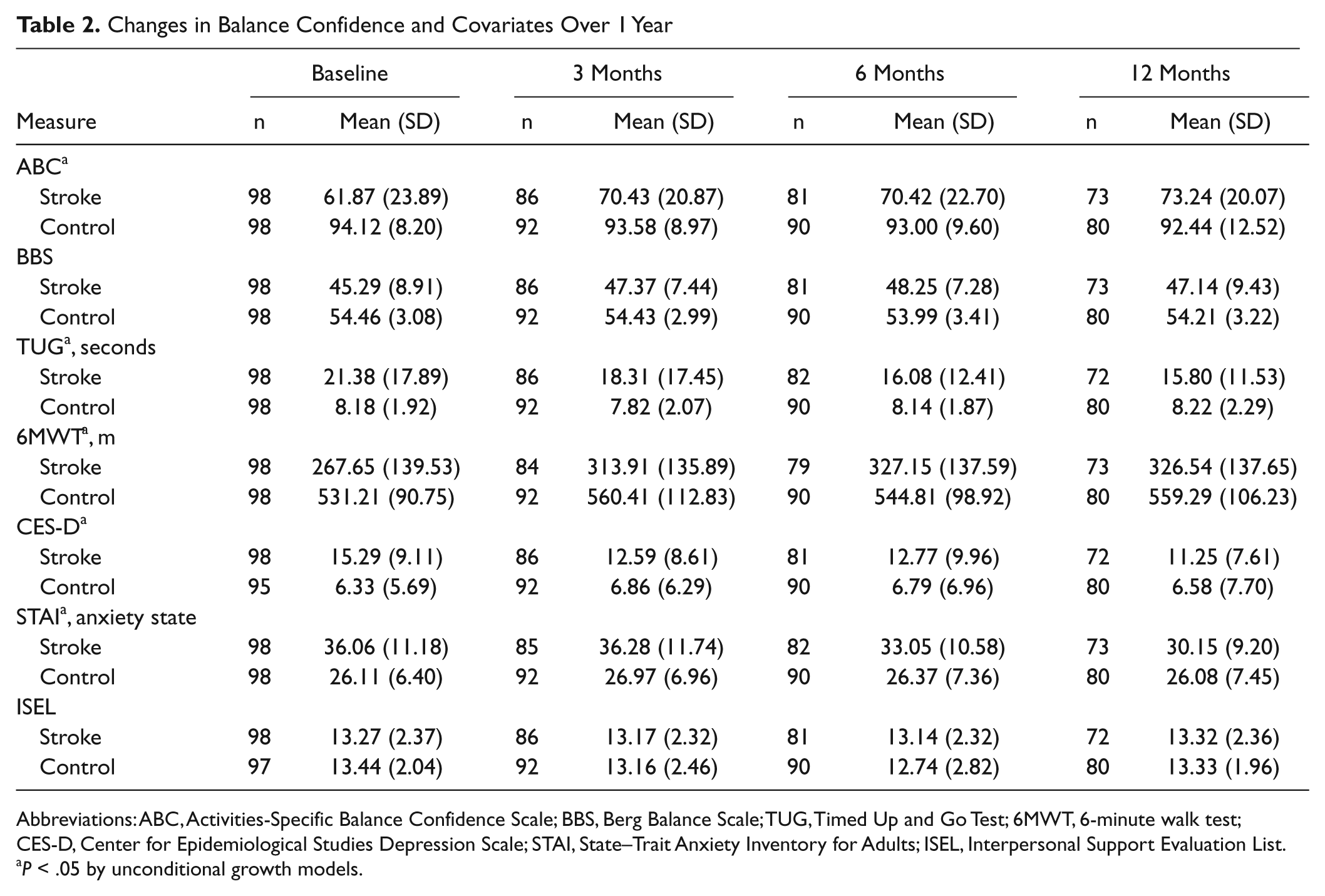
Abbreviations: ABC, Activities-Specific Balance Confidence Scale; BBS, Berg Balance Scale; TUG, Timed Up and Go Test; 6MWT, 6-minute walk test; CES-D, Center for Epidemiological Studies Depression Scale; STAI, State–Trait Anxiety Inventory for Adults; ISEL, Interpersonal Support Evaluation List.
P < .05 by unconditional growth models.
Table 3 presents the results of the unconditional and 2 conditional 2-level linear multilevel models (models 1 and 2). The fixed effects captured the systematic between person differences in change trajectory according to the values of the predictors. 24 Stroke status was a significant predictor of the intercept (P = .000) and slope (P = .000) of the estimated average linear change trajectory in balance confidence in model 1. For individuals without a stroke, the estimated initial ABC score was 94; the initial ABC score was significantly lower by 29.1 points for those with stroke. In terms of rate of change in ABC score, individuals without a stroke showed a nonsignificant decrease of 0.119 points per month, whereas individuals with stroke showed a significant differential of +0.745 points. After controlling for sociodemographic variables and clinical effects of stroke, model 2 revealed that stroke status remained a significant predictor of the intercept (P = .035) and slope (P = .004) of the estimated average change trajectory in balance confidence. In general, poor baseline balance performance (P = .000) was associated with lower initial balance confidence; higher state anxiety was associated with lower balance confidence at any given time (P = .026).
Factors Associated With Linear Change Trajectories of Balance Confidence: Results of Multilevel Modeling
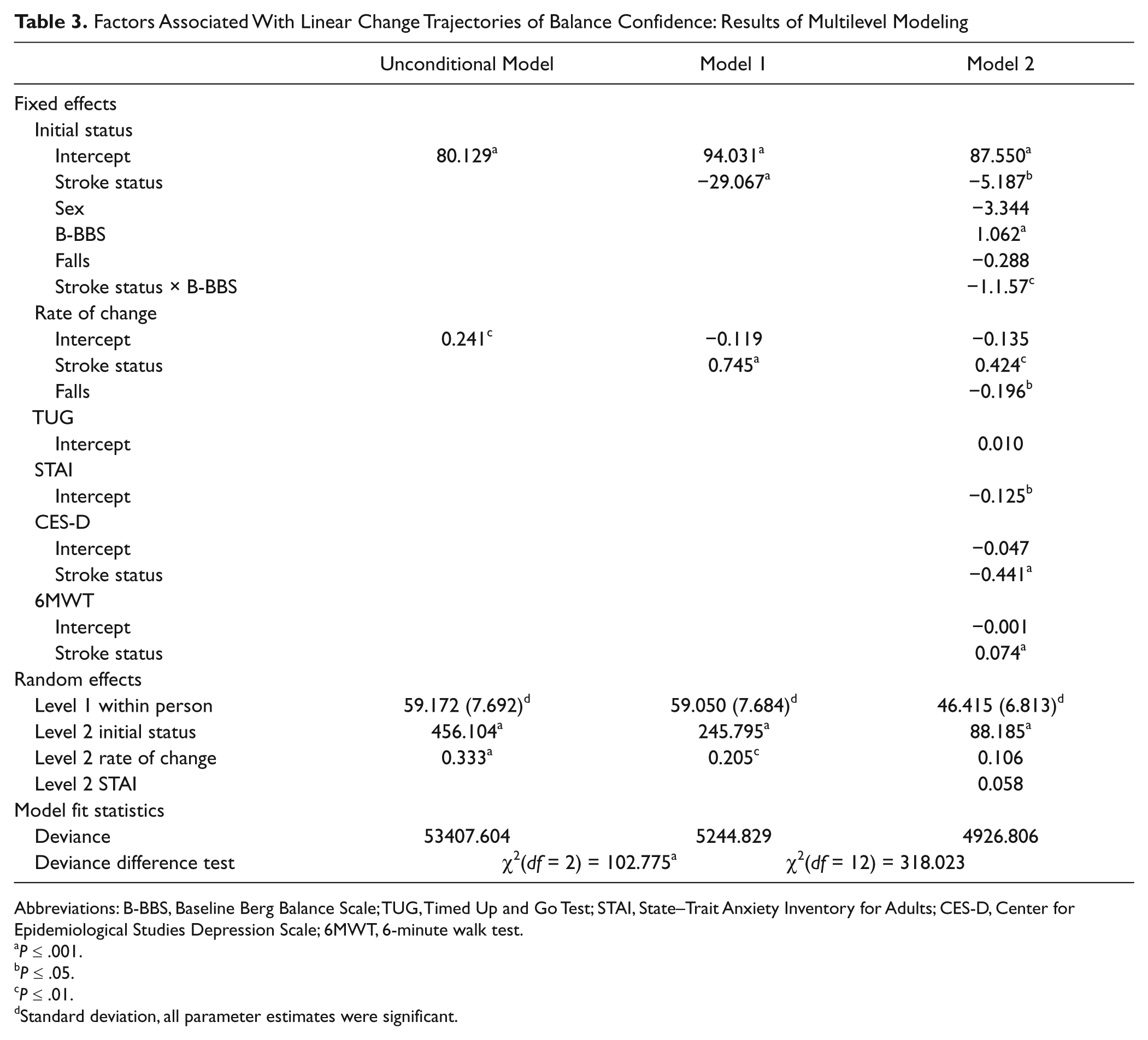
Abbreviations: B-BBS, Baseline Berg Balance Scale; TUG, Timed Up and Go Test; STAI, State–Trait Anxiety Inventory for Adults; CES-D, Center for Epidemiological Studies Depression Scale; 6MWT, 6-minute walk test.
P ≤ .001.
P ≤ .05.
P ≤ .01.
Standard deviation, all parameter estimates were significant.
Three covariates (depressive symptoms, walking capacity, and baseline balance performance) interacted statistically with stroke status when predicting balance confidence (P = .001, P = .000, and P = .007, respectively). Individuals with stroke who scored more depressed than the grand mean had lower balance confidence than individuals who scored less depressed than the grand mean; however, this effect was not observed in the controls. Similarly, only individuals with stroke whose walking capacity was better than the grand mean had higher balance confidence. In general, higher baseline balance performance was associated with higher initial balance confidence (an increase of 1.062 points times their Berg Balance Scale score on the ABC). However, individuals with stroke who had good baseline balance still had lower initial balance confidence than individuals without a stroke.
The estimated monthly rate of change in ABC for individuals with stroke showed an increase over time and was statistically different (0.424 point difference per month; P = .004) than that for the controls who showed a nonsignificant decline (−0.135 point per month, P = .151). After holding stroke status constant, having a single fall within 1 year lowered the ABC score by 0.196 points per month (P = .018), whereas multiple falls doubled the decline.
Discussion
Initial balance confidence remained significantly lower in individuals with stroke than controls. Lower baseline balance performance was associated with lower initial balance confidence, and higher anxiety state was associated with lower balance confidence at any given time. Depressive symptoms, walking capacity, and baseline balance performance interacted with stroke status when predicting balance confidence. Stroke status also predicted rate of change in balance confidence over the first year with the number of falls predicting change regardless of stroke status.
Our study revealed that, after controlling for sociodemographic variables and the clinical effects of stroke, individuals with stroke still showed significantly lower initial balance confidence than the controls. Although this finding is compelling, it is plausible that other variables not measured in this study (eg, use of an ambulation aid) may explain the remaining variability in balance confidence. Future studies are required to investigate the effects of these other factors.
Our sample mean of 61.87 (±23.89) is comparable with that of a previous study with stroke (59, 95% confidence interval = 55-64), 8 but our study included a control group. In our sample, more than 70% of stroke subjects had a baseline ABC scored <80. As suggested by Myers et al, 26 for individuals who score <80 on the ABC, there is room for improvement on balance confidence. Our finding suggests that individuals with stroke are consistently at risk for having low balance confidence. Therefore, they should be screened at or before discharge of rehabilitation for this problem so that treatment can be implemented in a timely manner.
Individuals with stroke who had increased symptoms of depression appeared to have lower balance confidence compared with those without a stroke. While previous studies report significant associations between depressive symptoms and balance confidence in nonstroke subjects,27,28 our work is the first to establish an interaction between stroke status and depressive symptoms. Increased symptoms of depression have been known to be an important predictor of participation, satisfaction with community reintegration, and quality of life poststroke.29-31 Considerable effort has been placed on finding the best treatment to reduce depressive symptoms poststroke. 32 In our sample, the percentage of individuals with stroke who were depressed at baseline was within the range of previously reported prevalence rates (30% to 50%) of poststroke depression in community-based individuals. 33 Since depression poststroke is highly prevalent, our findings provide a possible explanation of why individuals with stroke may have lower balance confidence and raises important questions about the covariation and association of depressive symptoms and balance confidence. Further investigation of this important relationship is warranted because it may imply that treating balance confidence could potentially enhance the treatment effect of depressive symptoms in individuals with stroke or vice versa. Furthermore, there may be parallel improvement in balance confidence and depressive symptoms if they are treated together.
Finding that stroke status interacted with walking capacity in predicting balance confidence is logical, previous studies8,34 suggested that change in balance confidence in a sample of stroke patients was associated with change in walking capacity after a task-specific walking intervention. It may be that stroke-specific impairments limit the distance walked, 35 therefore those with low walking capacity are at a higher risk of having reduced balance confidence.
Consistent with findings of previous studies examining stroke and nonstroke subjects,36-38 we found that poor baseline balance performance is associated with lower initial balance confidence in both individuals with stroke and controls. However, we also found that initial balance confidence is lower furthermore in individuals with stroke than controls, even though they may have the same level of balance performance. This further supports the idea that having strong self-efficacy enhances an individual’s ability to use their skills. Therefore, it may be equally important to treat balance confidence when treating individuals with stroke who also have impaired balance.
Our findings reveal that although individuals with stroke showed an increased rate of change in balance confidence during the first year after discharge from rehabilitation, having at least 1 fall slows down this rate significantly; in individuals without a stroke, it increases the rate of decline. Falls did not affect initial confidence in balance in our subjects. No clear association between balance confidence and falls was found in cross-sectional studies of older adults 39 and after stroke. 7 Our study is the first to establish a temporal relationship between balance confidence and falls. It may be equally important to provide interventions to reduce balance-related impairments40-43 and falls in order to increase balance confidence in daily activities.
We found that the association between depressive symptoms and walking capacity with balance confidence were modified by stroke status for individuals with stroke, but not in the controls. One limitation of this interpretation could be that the controls had much less variability in their CES-D scores and had near normal 6MWT walking distances.
Although assessments were obtained by trained collectors and monitored by a single research coordinator and 2 of the 3 centers had the same data collector throughout the study, the reliability of data collection could be another limitation. In addition, the results are limited to individuals with stroke of mild to moderate severity who had inpatient rehabilitation, so the findings may underestimate the problem of reduced balance confidence in the stroke population. Future studies should include individuals with stroke who are more restricted in mobility, such as wheelchair users. In that case, different measures for self-efficacy will be needed.
Conclusions
Individuals with stroke are at risk for having reduced confidence in their balance in the first year of community reintegration when compared with age-matched individuals without a stroke. More depressive symptoms, poorer walking capacity, and lower baseline balance performance are risk factors for lower balance confidence. The stroke participants showed a significantly faster rate of increase in balance confidence during the first year of community reintegration compared with controls, but having at least 1 fall slowed down this rate significantly. Since balance confidence is both remediable and a relevant rehabilitation outcome, individuals with stroke should be screened for reduced balance confidence by the time of discharge from rehabilitation so that they can receive prompt treatment.
Footnotes
Acknowledgements
We thank all the participants and the site coordinators who assisted with recruitment.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This work was supported by the Heart and Stroke Foundation, British Columbia and Yukon (no grant number), the Canadian Institutes of Health Research (MSH-76731, MSH-63617), and the Michael Smith Foundation of Health Research (CI-SSH-00379).