
Abstract
Background and purpose. This study aims to determine the long-term effects of a new Memory Self-efficacy (MSE) training program for stroke patients on MSE, depression, and quality of life. Methods. In a randomized controlled trial, patients were allocated to a MSE training or a peer support group. Outcome measures were MSE, depression, and quality of life, measured with the Metamemory-In-Adulthood questionnaire, Center for Epidemiological Studies–Depression Scale (CES-D), and the Who-Qol Bref questionnaire, respectively. We used linear mixed models to compare the outcomes of both groups immediately after training, after 6 months, and after 12 months, adjusted for baseline. Results. In total, 153 former inpatients from 2 rehabilitation centers were randomized—77 to the experimental and 76 to the control group. MSE increased significantly more in the experimental group and remained significantly higher than in the control group after 6 and 12 months (B = 0.42; P = .010). Psychological quality of life also increased more in the experimental group but not significantly (B = 0.09; P = .077). However, in the younger subgroup of patients (<65 years old), psychological quality of life significantly improved in the experimental group compared to the control group and remained significantly higher over time (B = 0.14; P = .030). Other outcome measures were not significantly different between both groups. Conclusions. An MSE training program improved MSE and psychological quality of life in stroke patients aged <65 years. These effects persisted during 12 months of follow-up.
Introduction
Memory Self-efficacy (MSE) is an important aspect of metamemory and is described as “a sense of mastery and control about memory functioning.” 1 It is based on the theoretical construct of self-efficacy, first introduced by Bandura. 2 It is the subjective experience of one’s memory capacity (as measured with objective memory tests). A high sense of MSE reflects a high level of confidence in one’s memory capacity.2,3 In healthy elderly people, 4 in traumatic brain injured patients, 5 and in stroke patients,6-8 MSE and memory complaints have been found to be related to psychological factors such as depression and neuroticism. The relationship between memory capacity and MSE seems to be less strong. 9 Subjective psychological factors rather than objectively measured memory capacity determine MSE and the presence of memory complaints. Effective training programs aimed to improve MSE have been developed for healthy older people and nursing home residents.10,11
In the literature, no evidence is found to support or refute the effectiveness of memory rehabilitation on objective or subjective memory measures in stroke patients. 12 The only memory rehabilitation program that is recommended for stroke patients with memory deficits is the use of external compensatory strategies. 13 Additional psychoeducation may be more effective in reducing subjective memory complaints in stroke patients. The goal of psychoeducation may be to understand and to be able to cope with memory complaints after stroke.
Many stroke survivors report symptoms of depression and reduced quality of life, factors that are related to MSE and functional outcome.6,14-16 We hypothesized that if MSE can be improved after stroke, this may result in increased quality of life and fewer depressive symptoms. An improved MSE may translate into a better sense of psychological well-being and better participation in social activities in which memory capacity is challenged, such as playing cards, grocery shopping, and attending birthday parties.
Therefore, we developed a new MSE training program for stroke patients, which focuses on improving MSE through psychoeducation in addition to learning memory compensatory techniques. In this training program, patients are educated about memory in general, and compensatory strategies are trained, as is the current practice standard. Additionally, patients learn about the influence of other factors such as mood and self-confidence on memory functioning in a group therapy setting. This MSE training already proved to be effective in increasing MSE in chronic stroke patients immediately after training. 17 This study aims to determine the long-term effects of the MSE training program on MSE, depression, and quality of life assessed at 6 and 12 months’ follow-up. We also studied potential age effects by dividing the study population into an elderly stroke group (≥65 years) and a younger stroke group (<65 years). Furthermore, we studied the effects of the MSE training on subjective general problem experience and social participation.
Materials and Methods
Former patients from the Rijndam Rehabilitation Centre, Rotterdam and the Heliomare Rehabilitation Centre, Wijk aan Zee, the Netherlands, were recruited between 2008 and 2010 if they were (1) 18 months or more postonset after their first and only stroke, (2) between 18 and 80 years of age, and(3) living independently and (4) if they reported subjective memory complaints during a first semistructured interview with the researcher. Exclusion criteria were progressive neurological disorders such as dementia or multiple sclerosis, insufficient knowledge and comprehension of the Dutch language, alcohol or drug abuse, and subdural hematomas or subarachnoid hemorrhages.
The study design was a multicenter randomized controlled trial. Patients were approached by their former physician and informed about the scope of the study, without details about the contents of the experimental and control group. All patients who agreed to participate signed an informed consent form. The Medical Ethics Committee of the Erasmus Medical Centre in Rotterdam, the Netherlands, approved the study.
Groups of patients were randomized following a block design of 10 per center. The allocation of the group to either experimental or control condition was performed by an independent investigator using a randomization program. The group size was 4 to 6 patients. Patients were not informed to which group they were allocated. Blinded and trained research assistants assessed all patients at home within 3 weeks prior to the intervention (T0). Within 10 days after the last session of the intervention (T1), after 6 months (T2), and after 12 months (T3), patients were reassessed. All measurements were performed with a research assistant present. Research assistants assisted in the case of aphasia by, for example, reading questions aloud.
The MSE training was adapted for stroke patients from an MSE training program developed by Verhey and Ponds. 18 The training aimed at improving subjective memory experience and memory functioning in healthy older people with memory complaints. The MSE training has a strong focus on psychoeducation and consists of 3 parts: (1) a general theoretical introduction on memory and stroke, (2) a training on internal and external memory strategies to improve compensating abilities, and (3) psychoeducation on the influence that mood, anxiety, and memory-related worries have on memory complaints. The training program involved 9 sessions of 1 hour, given twice a week. Patients received a training booklet with information about the sessions, and homework assignments were handed out after each session.
No therapeutic interventions were performed in the control group. Those in the control group were educated about causes and consequences of stroke and shared their problems with peers. They followed the same schedule of 9 sessions of 1 hour. Hand-outs of the sessions were provided. No homework assignments were given. A trained psychologist moderated both conditions.
Patient charts were obtained, and semistructured interviews were performed to gather demographic information and characteristics of the stroke. Personality, coping, the presence of aphasia, and executive disorders were assessed at baseline.
MSE was measured using the 3 subscales of the Metamemory in Adulthood questionnaire. 19 This questionnaire is translated and validated for a Dutch population by Ponds and Jolles. 20 The subscales Change, Capacity, and Anxiety are used to compute an MSE score, ranging from 3 to 15. A higher score represents a higher level of confidence in one’s memory capacity. The subscale Strategy was used to measure the use of memory strategies before and after the intervention, which ranges from 1 to 5. Examples of questions on internal and external memory strategies are, “Do you try to visualize a face in order to remember a name?” and “Do you use a calendar to remember important dates such as birthdays or wedding days?” Depression was measured using the Center for Epidemiological Studies-Depression Scale (CES-D). 21 A score of 16 or higher (range 0-60) is indicative for depression. Quality of life was measured using the multidimensional WhoQol-Bref questionnaire. 22 The mean scores ranging from 1 to 5 of the domains psychological quality of life and social factors of quality of life were used. In addition, the Visual Analogue Scale of the Euroqol-5D, ranging from 0 to 100, which measures quality of life in general, was used as the outcome measure in this study. The Visual Analogue Scale is presented as a vertical line such as a thermometer, on which patients indicate their general quality of life; 0 represents the worst possible health situation, and 100 represents the best possible health situation. Social participation was measured using the Social Support List. 23 The overall sum score, ranging from 12 to 48, is used as outcome measure for social participation. The Dutch version of the Auditory Verbal Learning Test (AVLT), 24 with scores ranging from 0 to 15, and Story Recall of the Rivermead Behavioural Memory Test (RBMT), 25 scores ranging from 0 to 42, were used to assess verbal memory capacity. Problem experience was assessed using an abbreviated version of the Impact on Participation and Autonomy. 26 In this version, the patient is asked to indicate the level of problem experience (ranging from 1-3: no problems, minor problems, major problems) in each domain of the questionnaire (mobility, self care, finance, education, work, activities around the house, social contacts, leisure time, and supporting others). We used the mean score on general problem experience as outcome measure.
Statistical Analysis
Based on a study design with 2 groups and 4 repeated measurements, with an estimated correlation of 0.70 within subjects, an α of .05, a power of 0.80, and an estimated effect size based on the variance explained and a partial η2 of 0.055 27 (which corresponds to a Cohen’s f effect size of 0.24 or a Cohen’s d of 0.48), we calculated that a total sample size of 140 patients would be needed to detect a significant difference between the groups.
All statistical analyses were performed using SPSS PASW version 18 for Microsoft Windows. Both groups were compared at baseline on demographic, clinical, and (neuro)psychological determinants using independent t tests for continuous variables and χ2 tests for categorical variables. We compared the baseline scores of MSE with published norm values 20 and calculated the z-scores and predicted scores for the AVLT and the RBMT delayed recall scores based on age and educational level.
The effect size with Cohen’s d was calculated based on the means and standard deviations (SDs) of the change scores over the intervention period. The proportion of patients improving at least 1 SD on the MSE scale was compared between the groups. 27 We performed repeated-measures analyses using linear mixed models for each of the outcome measures to compare both groups over 3 time points (T1, T2, and T3), adjusted for baseline measures (T0). We started with unstructured correlation matrices and simplified if possible to compound symmetry matrices. Fixed factors in the analyses were group, measurement time point, and baseline values. Interaction effects of these variables were taken into account. Nonsignificant variables were removed from the full model to simplify the model. We used a P value of <.05 for statistical significance. Additional to these analyses, we repeated all mixed models in subgroups of age, based on the previous finding that the effect of the MSE training is larger in younger patients than in older patients. 17 In the Netherlands, people typically retire at the age of 65 years; therefore, we divided the study population into a younger group of <65 years and an older group of ≥65 years.
Results
Patient Population
In total, 153 patients were randomized to either the experimental or the control group. Patient inclusion is described in the flow chart (Figure 1). The mean age of the total population was 58 years (SD = 9.7 years), and 55% was male. Mean time poststroke was 54 months (SD =37 months). In 57%, the stroke was left sided, and in 68%, the type of stroke was ischemic.
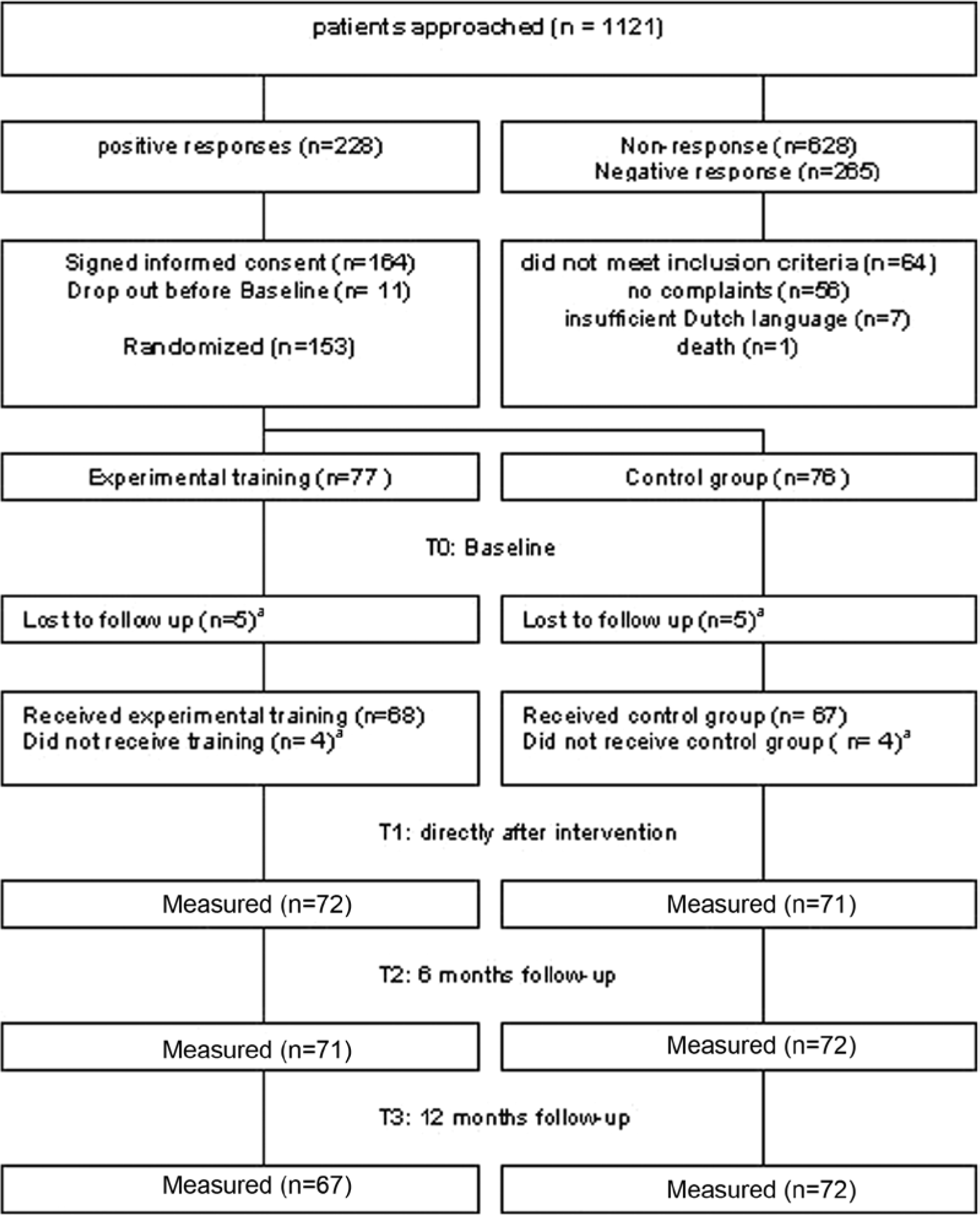
Flowchart patient inclusion
The study population was divided into 2 age groups: 38 (27%) patients were ≥65 years old, and 115 (73%) patients were <65 years old (Table 1). Older patients were more often men and had lower depression scores and lower memory capacity scores than the younger patients at baseline. There were no significant baseline differences between the experimental and control groups in either subgroup (Table 1), except for the delayed recall score (AVLT) in the younger group. Baseline MSE scores (Table 1) were below average in the younger group compared with a Dutch norm population (age <65 years: MSE norm = 9.86, SD = 0.71) and low compared with a subpopulation without memory complaints (age <65 years: MSE norm = 10.15, SD = 0.56). In the older age group, the baseline scores were on average comparable with the norms (age ≥65 years: MSE norm = 8.65, SD = 0.76) but low when compared with a subpopulation without memory complaints (age ≥65 years: MSE norm = 10.01, SD = 0.63). 20 Baseline delayed recall scores of the AVLT and RBMT (Table 1) were also low compared with norm scores based on age and educational level (age <65 years: AVLT = 9.73, RBMT = 16.70; age ≥65 years: AVLT = 8.11, RBMT = 14.87).
Baseline Characteristics of the Experimental and Control Groups, by Age Group a
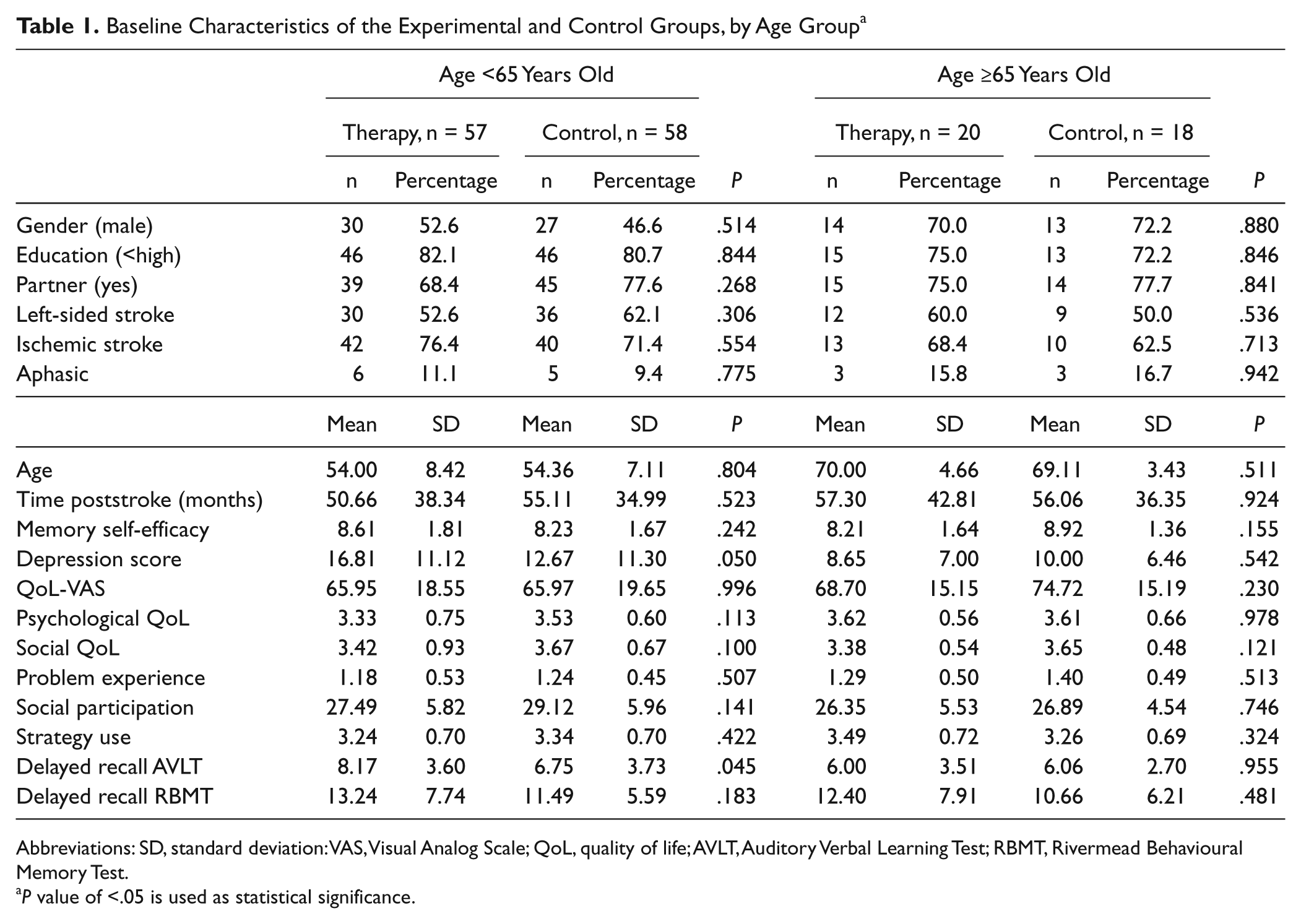
Abbreviations: SD, standard deviation: VAS, Visual Analog Scale; QoL, quality of life; AVLT, Auditory Verbal Learning Test; RBMT, Rivermead Behavioural Memory Test.
P value of <.05 is used as statistical significance.
Comparison Between Experimental and Control Groups
MSE improved significantly over the intervention period in the experimental group compared with the control group (P = .010), and this effect was sustained after 6 and 12 months in the total study population. The Cohen’s d effect size was 0.37 over the intervention period. In the experimental group, 15% of the patients improved at least 1 SD on the MSE scale, which is significantly more than the 4% in the control group (P < .024). Depression scores declined in both groups, but group difference did not reach significance (P = .148). Psychological QoL improved more in the experimental than in the control group, but this result was not statistically significant either (P = .077). Other quality-of-life measures did not differ between groups (Table 2). Participants in both groups reported a decrease of problem experience (P = .014) over the follow-up period of 12 months, but no differences between the experimental and control groups were found. Self-reported strategy use remained unchanged in either group (P = .934). No differences in social participation were found between the experimental and control groups over time (P = .341).
Effects of MSE Training in the Intervention Group Compared With the Control Group
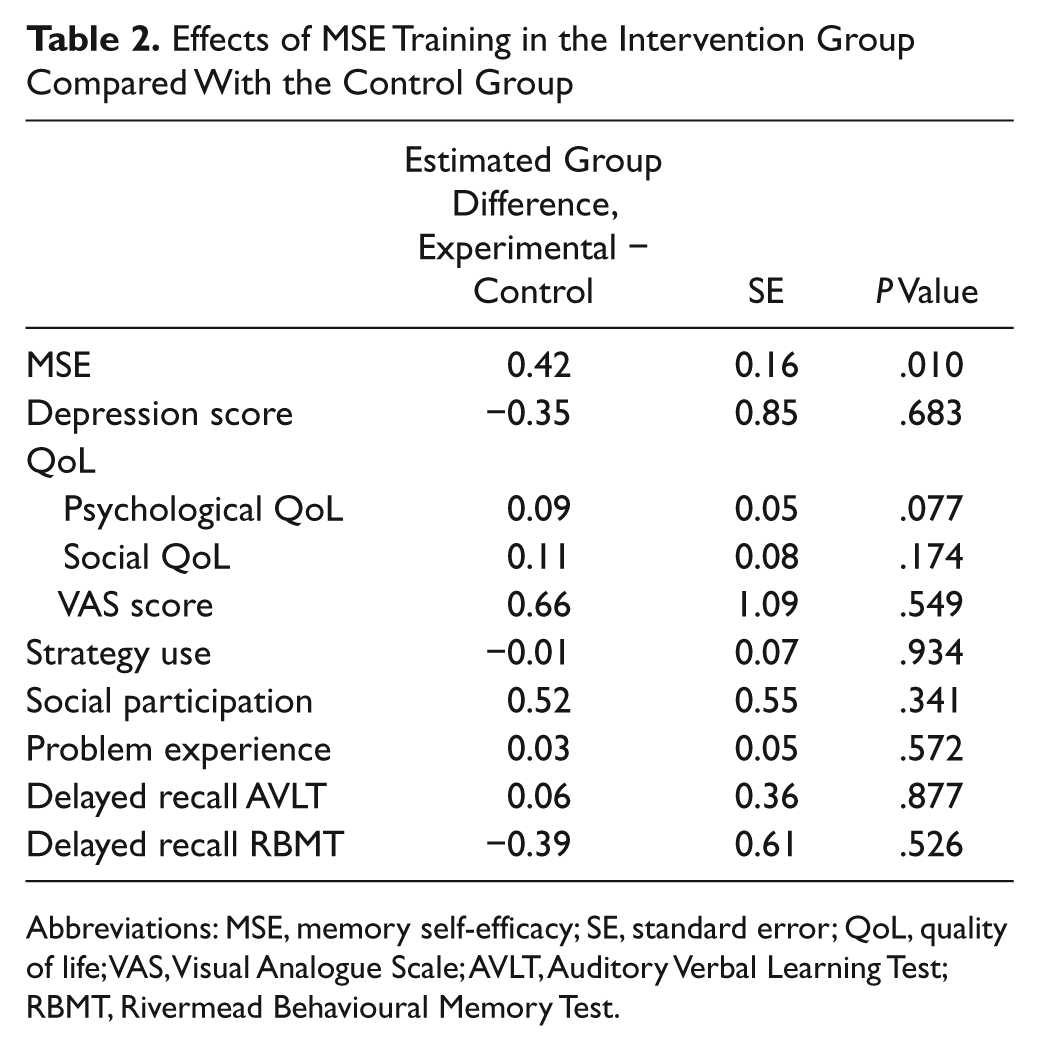
Abbreviations: MSE, memory self-efficacy; SE, standard error; QoL, quality of life; VAS, Visual Analogue Scale; AVLT, Auditory Verbal Learning Test; RBMT, Rivermead Behavioural Memory Test.
Subgroup Analyses
In younger patients in the experimental group, MSE improved significantly more than the MSE score in the control group (B = 0.56; P < .003), and this effect remained stable over 12 months’ time (Figure 2). After adjustment for the difference in baseline memory capacity (measured with the AVLT), the group difference in MSE effect was equivalent (B = 0.61; P < .001). Adjustment for depression score did not alter these results. In older patients, the experimental group did not differ significantly from the control group in MSE scores over time (P = .913). The psychological domain of quality of life also improved significantly more in younger patients in the experimental group (B = 0.14; P < .030) than in the control group. These findings remained stable over 12 months (Figure 3) and did not alter after adjustment for baseline depression score (B = 0.16; P < .016). Further adjustment for baseline memory capacity did not change these results. The older patients showed no improvement in psychological quality of life in either group (P = .829; Table 3). Other outcomes did not differ between the experimental and control groups over time in subgroups of age.
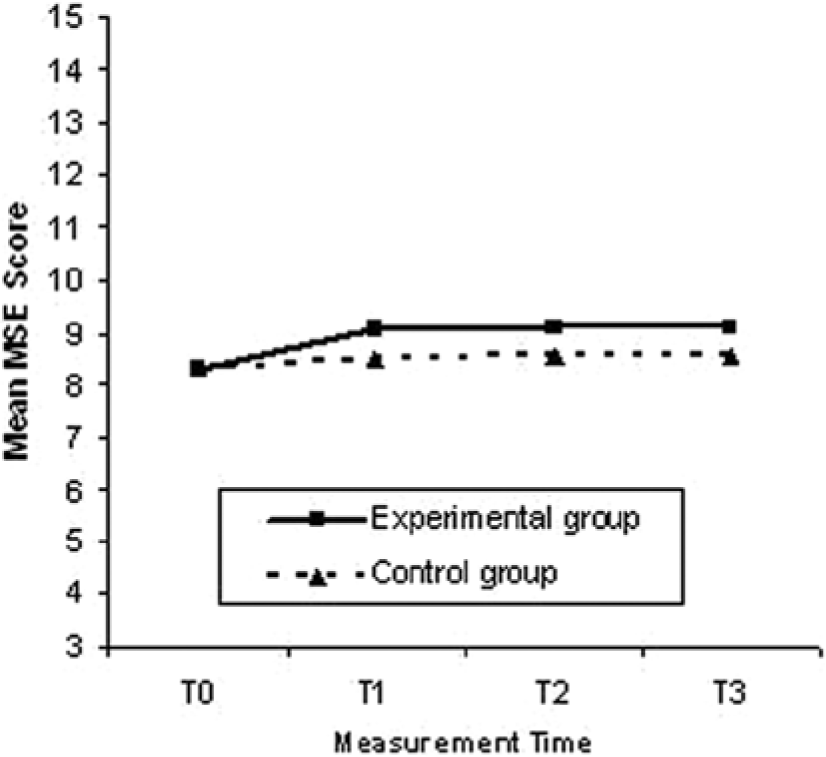
Training effect of MSE in patients 65 years old and younger
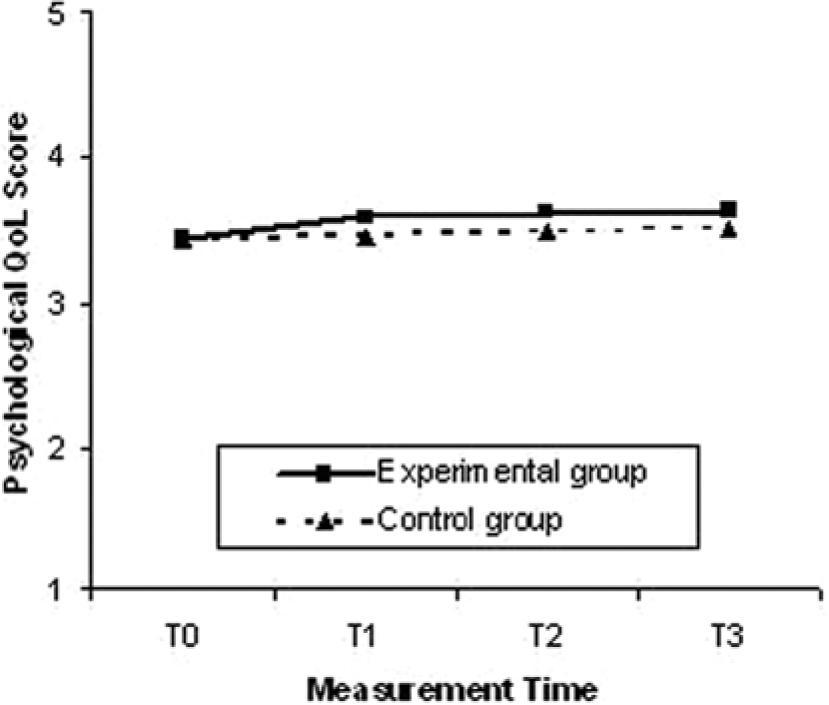
Training effect of psychological quality of life in patients 65 years old and younger
Effects of MSE Training Per Age Group: <65 Years (n = 105) and >65 Years Old (n = 38)
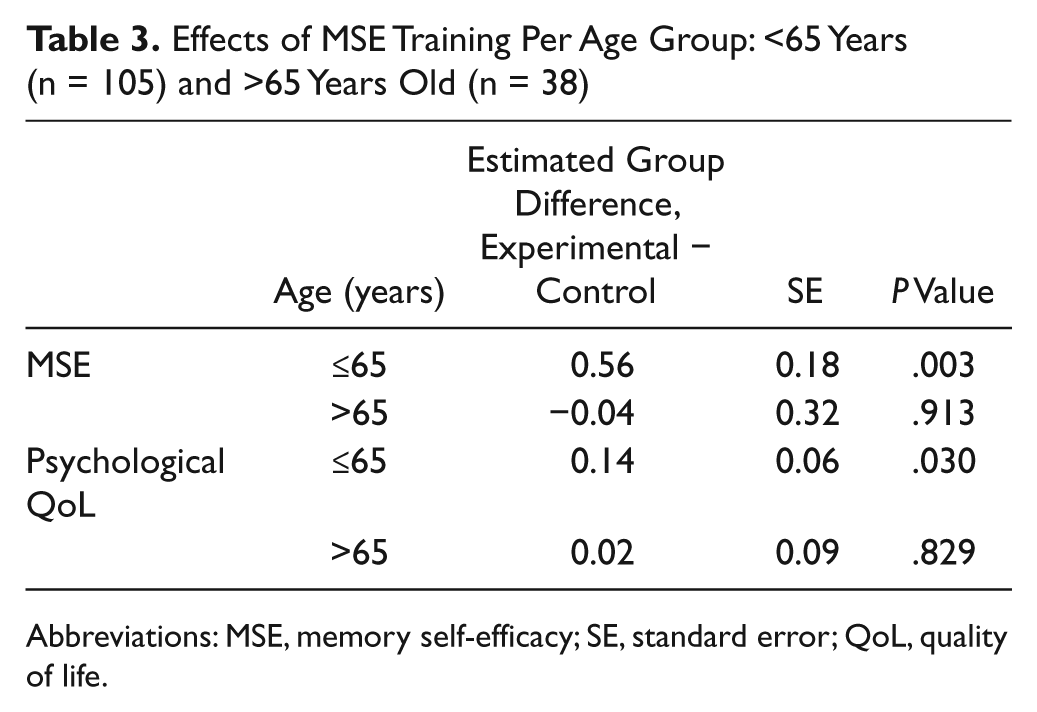
Abbreviations: MSE, memory self-efficacy; SE, standard error; QoL, quality of life.
Discussion
To our knowledge, this study is the first randomized controlled trail on MSE training in patients after stroke in the chronic stage. The newly developed MSE training program improved MSE in chronic stroke patients, and this effect continued over a period of 1 year after the intervention and was particularly present in younger patients. With this training, we were able to improve the confidence that patients have in their memory functioning. In addition, the MSE training improved psychological quality of life, which lasted over the 12 months’ follow-up time in patients younger than 65 years.
Cicerone et al 13 reviewed the available treatment methods for memory deficits after traumatic brain injury and stroke. External strategy use seems to be the only effective rehabilitation treatment for memory deficits after stroke.13,28 This new MSE training provides an additional treatment method to decrease memory complaints after stroke using 3 main components: compensatory techniques, MSE, and psychoeducation. This combination seems to be of additional value to existing memory rehabilitation treatment. In other studies, improvements in memory functioning were not sustained after training in stroke patients. 29 We found long-lasting improvements in MSE as well as in the psychological domain of quality of life.
Chronic memory complaints after stroke constitute a big problem for memory rehabilitation, which should be addressed by additional training such as MSE training. The long-lasting effects of MSE training increase the relevance of the effects that we found. Although the effect size seems relatively small on the group level, we found that our effect size of 0.37 is comparable to effect sizes (0.24) found in other studies using the Metamemory in Adulthood questionnaire. 30 Furthermore, we found that 15% of the patients in the intervention group improved at least 1 SD on the MSE scale, which is, in our opinion, a clinically relevant effect in a chronic stroke population. An effect on actual memory performance is difficult to achieve and was not found in this study, other than a practice effect. The fact that psychological aspects of quality of life can be improved in younger stroke patients by means of this new MSE training argues for further investigating the possibilities to bring this training into clinical practice.
Despite the fact that learning compensatory strategies in this MSE training program did not have an effect on strategy use, patients reported a higher confidence in their memory functioning. In other studies, the use of external strategies is recommended as treatment, although the use of external strategies is not always consolidated after training.12,29 Because this study was carried out in a chronic stroke population, strategy use may already have reached its maximum in this population, especially because these patients received standard memory training during their admission in a rehabilitation center. If this study had been carried out in the active rehabilitation phase in patients after stroke in the subacute stage, it is possible that compensatory strategies could have been learned more easily with MSE training than after standard memory rehabilitation programs. This should be studied in future effect studies of the MSE training program in an earlier stage of rehabilitation.
Mood was not significantly affected in either the experimental or the control group. Depressive symptoms decreased on average in both groups, but because of heterogeneity within the groups, this decrease did not reach significance. Furthermore, social participation did not change over the intervention and follow-up periods. The SSL is mainly about social relationships, which may not change as a result of a higher MSE. Offering the MSE training program earlier in rehabilitation may have a larger effect on mood and social participation as well.
A drawback of the MSE training is that the effects are not found in elderly stroke patients. Because the stroke population is growing and the age of the population is increasing, we did not want to exclude elderly patients. The older patients differed from the younger patients in gender (more men) and having fewer depressive symptoms and lower memory capacity scores, which may explain why the MSE training was less effective in older patients. Furthermore, the baseline MSE score of the older group was equivalent to an elderly norm population, whereas the baseline MSE score of the younger group was low compared with the norm score. Also, the quality-of-life scores tended to be higher in the elderly compared with the younger subgroup and in combination with fewer depressive symptoms, there was less to gain for the elderly patients. In the Netherlands, elderly patients with multiple physical and cognitive deficits are mostly referred to nursing homes. Thus, only the relatively healthy elderly stroke patients are referred to rehabilitation centers and could therefore be included in this study.
Regardless of group or age, the only problem experience decreased over the intervention period. The MSE training could be further adapted to better fit the elderly stroke population with low MSE scores. Changes in duration of the training, increasing the number of sessions, decreasing the information load in individual sessions, and age-related examples of memory-demanding situations are all examples of possible adaptations for elderly patients.
A limitation of this study may have been the influence of the same psychologist moderating all sessions in the experimental and control groups, which might have decreased the contrast between both groups. However, possible trainer effects between groups were ruled out by this study design.
In conclusion, the newly developed MSE training is a valuable addition to current memory training programs. The current program is particularly useful for younger patients. Offering the program in an earlier phase after stroke and making further adaptations for older patients may have an additional beneficial effect on the clinical relevance of the training.
Footnotes
Acknowledgements
The authors would like to thank all participating patients: Marieke Visser, Arlette Thiellier, Wendy Boerboom, and Anushka Wardenaar are thanked for performing measurements. No disclosures are applicable.
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This study is funded by the Kinder Fonds Adriaanstichting (Children’s fund Adriaanstichting) Grant Number: 07.03.28-2007/0082.