
Abstract
Background. Contralaterally controlled functional electrical stimulation (CCFES) is an experimental treatment intended to improve hand function after stroke. Objective. To compare the effects of 6 weeks of CCFES versus cyclic neuromuscular electrical stimulation (NMES) on upper extremity impairment and activity limitation in patients ≤6 months poststroke. Methods. Twenty-one participants were randomized to CCFES or cyclic NMES. Treatment for both groups consisted of daily stimulation-assisted repetitive hand-opening exercise at home plus twice-weekly lab sessions of functional task practice. Assessments were made at pretreatment and posttreatment and at 1 month and 3 months posttreatment. They included maximum voluntary finger extension angle, finger movement tracking error, upper extremity Fugl-Meyer score, Box and Blocks test, and Arm Motor Abilities test. Treatment effects were estimated using a 2-factor repeated measures analysis of variance with the value of the baseline measure as a covariate. Results. Seventeen patients completed the treatment phase (9 CCFES, 8 cyclic NMES). At all posttreatment time points, CCFES produced larger improvements than cyclic NMES on every outcome measure. Maximum voluntary finger extension showed the largest treatment effect, with a mean group difference across the posttreatment time points of 28° more finger extension for CCFES. Conclusions. The results favor CCFES over cyclic NMES though the small sample size limits the statistical power of the study. The effect size estimates from this study will be used to power a larger trial.
Introduction
Contralaterally controlled functional electrical stimulation (CCFES) is a new treatment aimed at improving recovery of volitional hand function in patients with hemiplegic stroke.1,2 CCFES stimulates the paretic finger and thumb extensors with an intensity proportional to the degree of volitional opening of the contralateral unimpaired hand. The unimpaired hand wears an instrumented glove that detects the degree of hand opening. 1 The device enables patients with hemiplegia to open their paretic hand and practice using it in functional tasks (Figure 1).

Contralaterally controlled functional electrical stimulation system. Volitional opening of the unaffected hand produces a proportional intensity of stimulation to the paretic hand extensors. The system enables patients with hemiplegia to practice tasks
Three features of CCFES potentially make it more effective at treating hand paresis than other neuromuscular electrical stimulation (NMES) methods (ie, cyclic NMES, 3 electromyography-triggered NMES, 4 or switch-triggered NMES 5 ). First, CCFES produces peripheral neural activity that may be more temporally correlated with central neural activity, and thus possibly better at promoting Hebbian plasticity. The patient not only controls when the stimulation comes on (as in electromyography- or switch-triggered NMES) but also controls the moment-to-moment intensity of stimulation and therefore the degree of hand opening, possibly producing a more compelling perception of restored motor control. When this coupling of motor intention to motor response occurs repetitively, it may induce synaptic remodeling and reorganization of cortical areas.6-10 Second, CCFES uses movement from the unaffected hand to produce symmetric and nearly simultaneous movement of the affected hand. Bilateral symmetric movement exercise may reduce upper limb impairment in some stroke patients, 11 and the mechanisms that underlie these improvements 12 may also be operative with CCFES. Third, because the user controls the timing and degree of hand opening in a way that does not interfere with the fluidity of task practice, the CCFES system is more conducive to practicing goal-oriented functional hand tasks, which have been shown in both animal 13 and human 14 studies to be important in driving functional reorganization of cortical maps and facilitating motor recovery after stroke.
The feasibility of CCFES to reduce hand impairment was demonstrated in our previous case series studies in stroke patients with chronic (>6 months) upper extremity hemiplegia.1,2 Each of the 6 participants in those studies experienced reductions in at least one of several measures of upper extremity impairment after a regimen of CCFES. We initiated this study to begin to explore the effects of CCFES in patients who are within 6 months of their stroke.
The purpose of this early-phase, randomized clinical trial was to estimate the effect of 6 weeks of CCFES on upper extremity impairment and activity limitation by comparing CCFES to cyclic NMES. We chose cyclic NMES as a comparison treatment because it allows us to rule out the effects of factors that are not unique to CCFES, such as therapist attention, expectations, practice effects, and time in the laboratory or in exercise, as well as the effects of muscle stimulation (eg, muscle strengthening).
Methods
Participants
Participants were recruited from the inpatient and outpatient stroke rehabilitation services of an academic medical center. The institutional review board approved the study protocol and each participant gave written informed consent prior to their eligibility assessment. The criteria for inclusion were as follows: ≤6 months from first hemorrhagic or nonhemorrhagic stroke, finger extensor strength ≤4/5 (Medical Research Council scale), sufficient active shoulder and elbow movement to volitionally position the hand in the workspace, functional hand opening in response to electrical stimulation, ability to follow 3-stage commands, and available caregiver to assist with the stimulator if needed. Patients with 3 or 4/5 finger extensor strength also had to be unable to open the hand adequately to acquire or release an object (water bottle) to be considered for enrollment. Patients were excluded if they had intramuscular botulinum toxin injections in any upper limb muscle within 3 months preceding study entry, edema or absent sensation of the affected forearm or hand, uncompensated hemineglect, severe shoulder or hand pain, severe depression, or insufficient passive range of motion of the wrist or fingers to allow a functional degree of hand opening.
After their baseline assessment of upper extremity impairment and activity limitation (described below), participants were randomly assigned to either CCFES or cyclic NMES via a computer-generated blocked randomization sequence with a block size of 6. A block size of 6 was chosen because this study was originally planned as a 3-arm randomized clinical trial. To avoid interfering with inpatient rehabilitation, the study enrollment procedures (i.e., eligibility and baseline assessments) were initiated no earlier than 1 week prior to discharge from the hospital so that all participants started the treatment phase of the study after being discharged to home.
Electrical Stimulation Systems and Stimulation Parameters
For both treatment groups, surface electrodes (2-in. square and/or 1.25-in. round) were positioned on the forearm and hand to produce functional hand opening. The muscles targeted for activation were the extensor digitorum communis and extensor pollicis longus. The abductor pollicis longus or brevis, dorsal interossei, or extensor indicis proprius were also stimulated if needed to produce functional hand opening. No more than 3 independent monopolar channels (using a common anode) of stimulation were used for any participant in this study. The stimulators used in this study delivered biphasic rectangular current pulses; the pulse frequency was set at 35 Hz, and the pulse amplitude was set at 40 mA for all but 1 participant who required 60 mA. A minimum and maximum intensity (pulse duration) of stimulation was determined for each channel of stimulation. The minimum intensity was just sub–motor threshold; the maximum was that which produced functional hand opening without pain.
For the CCFES group, the stimulator was programmed to modulate the pulse duration from each stimulation channel from minimum to maximum in proportion to the amount of opening of an instrumented glove worn on the nonparetic hand (Figure 1). The glove consisted of an assembly of 3 bend sensors (Images SI Inc, NY) in cloth sheaths attached to the dorsal side of the index, middle, and ring fingers. 1 Proportional impedance changes in the sensors modulated an analog voltage input to the stimulator. The stimulator issued sound and light cues to tell the CCFES participant when and for how long to attempt to open both hands during an exercise session. For the cyclic NMES group, the stimulator was programmed to automatically and repetitively ramp the pulse durations from minimum to maximum in 1 second, maintain the stimulation at maximum for several seconds (see below), and then ramp down the stimulation in 1 second, repeating this cycle at a rate that matched the sound and light cue timing of the CCFES group. For the cyclic NMES group, sound and light cues indicated when the stimulation ramped on and off, and no glove was worn on the contralateral hand.
Each participant, and caregiver if necessary, received instructions and training from their treating therapist on how to put on the electrodes and use the stimulator at home according to their group assignment. A picture was taken of the electrodes in their proper positions to assist correct positioning.
Treatments
The CCFES and cyclic NMES treatments lasted 6 weeks. Both treatments consisted of 2 components: (a) therapist-guided functional task practice twice a week at the research laboratory and (b) self-administered repetitive stimulated hand opening exercise daily at home.
The laboratory sessions consisted of practicing a finger movement control task for 15 minutes followed by 75 minutes of using the paretic hand to perform functional tasks. For the finger movement control task, an electrogoniometer was attached to the index finger of the paretic hand and displayed the degree of finger opening as a cursor that moved up and down as the participant opened and closed the hand. The task required the participant to keep the cursor between 2 parallel traces (a track) that scrolled right-to-left across the screen. 15 The track was scaled to the range of opening that the participant could achieve that day. Functional task practice involved hand opening and closing to pick up, manipulate, and release objects commonly used in daily life. The tasks were graded in difficulty from easy-to-acquire-and-manipulate to tasks requiring wider hand opening, greater skill, graded hand opening (controlled release), and coordination of hand function with proximal upper limb movement. A task was repeated numerous times over approximately 15 minutes before switching to a different task, adding complexity as movement was mastered.
Participants in the CCFES group used their stimulator to assist the paretic hand in performing the tracking task and hand function tasks. Participants in the cyclic NMES group practiced the tasks without stimulation because cyclic NMES is not conducive to assisting with tasks since it is not controlled by the participant. To make up for the difference in the amount of stimulation received by the 2 groups during lab sessions, the cyclic NMES group was prescribed more stimulation than the CCFES group during the home exercises so that both groups were prescribed an equivalent total duration of stimulation every week.
The self-administered hand opening stimulation exercise consisted of 2 sessions per day at home. For the CCFES group, a session lasted 55 minutes and consisted of three 15-minute sets separated by 5 minutes of rest. For the cyclic NMES group, a session lasted 75 minutes and consisted of four 15-minute sets separated by 5 minutes of rest. Both groups were prescribed approximately 12 hours of stimulation per week (including the stimulation received by the CCFES group during lab sessions).* During each 15-minute set, the CCFES participants were prompted by light and sound cues to repeatedly attempt to open both hands for several seconds and then relax both hands for several seconds. CCFES participants were specifically instructed to attempt to open both hands in response to the cues. For participants in the cyclic NMES group, the stimulator automatically opened the paretic hand repeatedly with the same duty cycle as the CCFES cues. Cyclic NMES participants were specifically instructed to relax and let the stimulator open their hand without adding their own effort or moving their unaffected hand. For both groups, the hand open/relax durations (cues for the CCFES group) were adjusted approximately every 2 weeks, starting at 6 seconds open and 20 seconds relax, then changing to 8 seconds open/16 seconds relax, and finally to 8/10. This graded duty cycle was to progressively build strength with longer duration muscle contractions and more repetitions. 16 Participants filled out diaries to keep track of when they did their exercise sessions. Along with the diaries, compliance was monitored by the usage logging capability of the stimulator. The participants were instructed to perform the 2 sessions per day whenever they chose but to separate them by at least 2 hours to avoid muscle fatigue. On the days they came for lab sessions, they were instructed to perform only one exercise session at home at least 2 hours after their lab session.
Outcomes Assessment
A blinded therapist assessed upper extremity impairment and activity limitation at baseline, end of treatment (EOT), and at 1 and 3 months post-EOT. The impairment measures included maximum voluntary finger extension angle (primary endpoint), finger movement control (tracking test), the upper limb portion (maximum score = 66) of the Fugl-Meyer motor assessment 17 , and the Box and Blocks Test. 18 Activity limitation was measured with the Functional Ability component (0 to 5 ordinal scale) of the Arm Motor Abilities Test (AMAT). 19
Maximum voluntary finger extension angle was measured with a custom-built electrogoniometer that recorded the angles of the metacarpophalangeal (MP) and proximal interphalangeal (PIP) joints of the index finger simultaneously. Participants were seated with their forearms and wrists supported and stabilized in a neutral posture. From this resting position, they were instructed to open their fingers as fully as possible in response to a 4-second audio cue while the joint angles from the electrogoniometer were sampled with a computer. The MP and PIP angles were added together, providing a composite measure of degree of finger extension, where 0° corresponds to full extension of the MP and PIP joints; the more negative the angle, the more flexed the finger. Three trials were repeated after a practice trial, resting 1 minute between trials. The average degree of voluntary finger extension attained during the last second of the audio cue was calculated for each trial and averaged over the 3 trials.
The finger movement tracking test made use of the same setup as the maximum voluntary finger extension assessment, and was similar to the tracking task described above except that the track used here was a single 30-second sine wave trace with a frequency of 0.1 Hz (1 cycle in 10 seconds) scrolling across the screen. The sine wave trace was scaled to the middle 70% of the participant’s voluntary range of motion as determined that day by the maximum voluntary finger extension test.20-22 A cursor was displayed on a computer screen, its vertical position corresponding to the degree of finger extension. The participant was instructed to try to keep the cursor on or as close to the scrolling sine wave trace as possible by opening and closing the hand with no stimulation. Three trials were repeated after a practice trial, resting 1 minute between trials. The average vertical distance between the cursor and target trace (ie, the percentage of the participant’s active range of motion) was calculated for each trial, and the tracking error was the lowest error of the 3 trials.
Data Analysis
Baseline characteristics and scores were summarized with means (±standard deviations) for continuous variables, and frequencies for categorical variables. For each outcome measure, a 2-factor repeated measures analysis of variance that included the baseline value of the same measure as a covariate was used to compare the effectiveness of CCFES and cyclic NMES across the posttreatment time points (EOT, 1-month follow-up, and 3-month follow-up). For each outcome measure and each group, the analysis calculated posttreatment mean scores adjusted for baseline, which allows the 2 treatments to be compared at a common value of baseline severity, a method superior to using simple gain scores. 23 Time-by-treatment interactions were assessed but none were significant. Given the early phase of this study and small sample size, ordinary significance testing (ie, using P values) is inherently unreliable in that “significant” results are way too often false positives and “nonsignificant” results are too often false negatives.24-26 Accordingly, our analysis focuses on estimates and confidence intervals.
Results
A total of 21 participants were randomized to CCFES or cyclic NMES; 4 did not complete the treatment phase (Figure 2). The analyses are based on the remaining 17 participants, 9 in the CCFES group and 8 in the cyclic NMES group. All participants had either cortical or subcortical strokes except 1 CCFES participant with a combination subcortical/brainstem lesion. Most of the demographic characteristics and baseline variables related to the stroke and neurological status were similar in the 2 groups, but the small sample size created imbalance regarding severity of motor impairment and activity limitation at baseline, with the CCFES group starting treatment in a more impaired and functionally limited state than the cyclic NMES group, on average (Table 1).
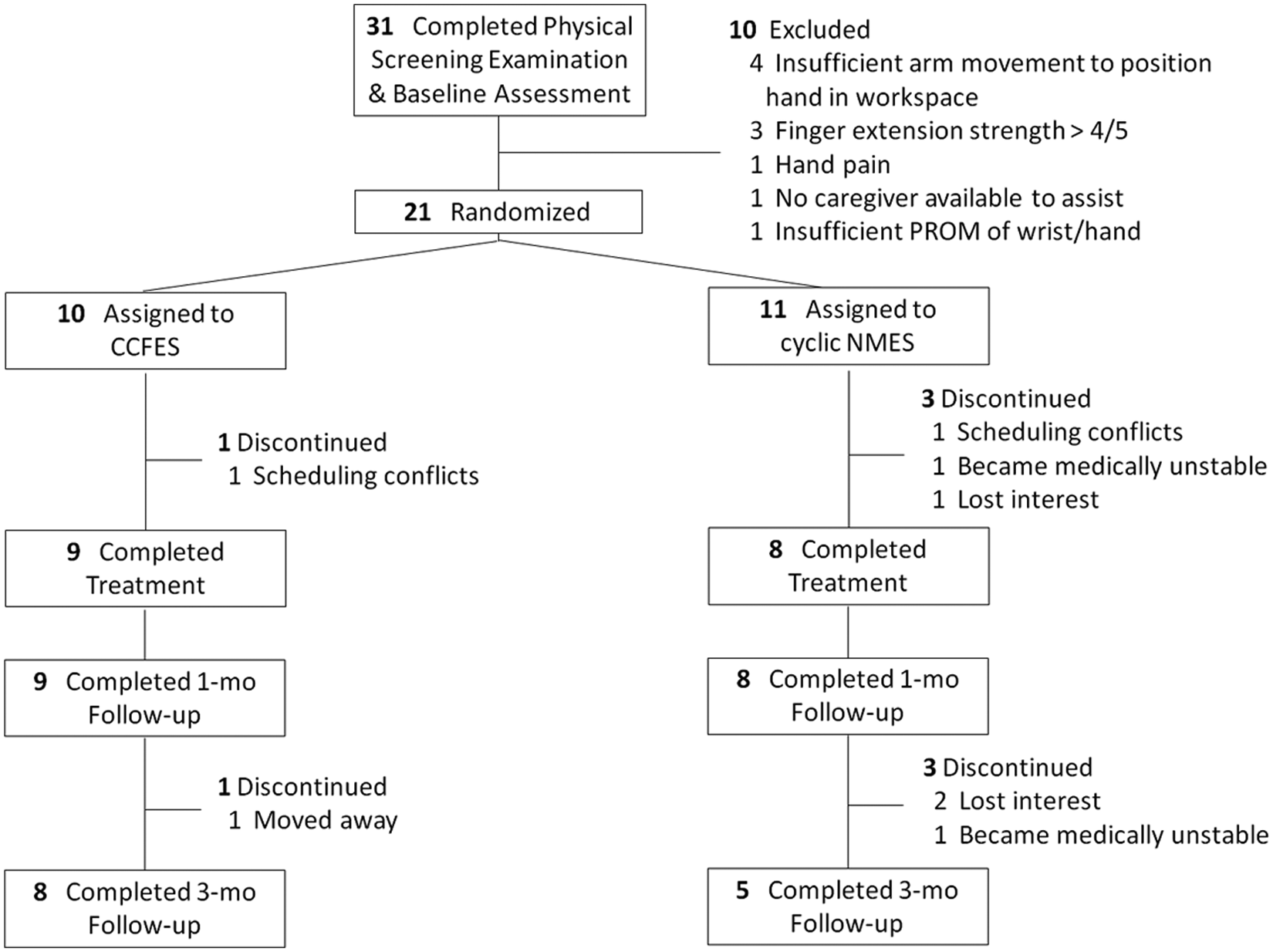
Flow of participants through the study
Baseline Characteristics and Scores a
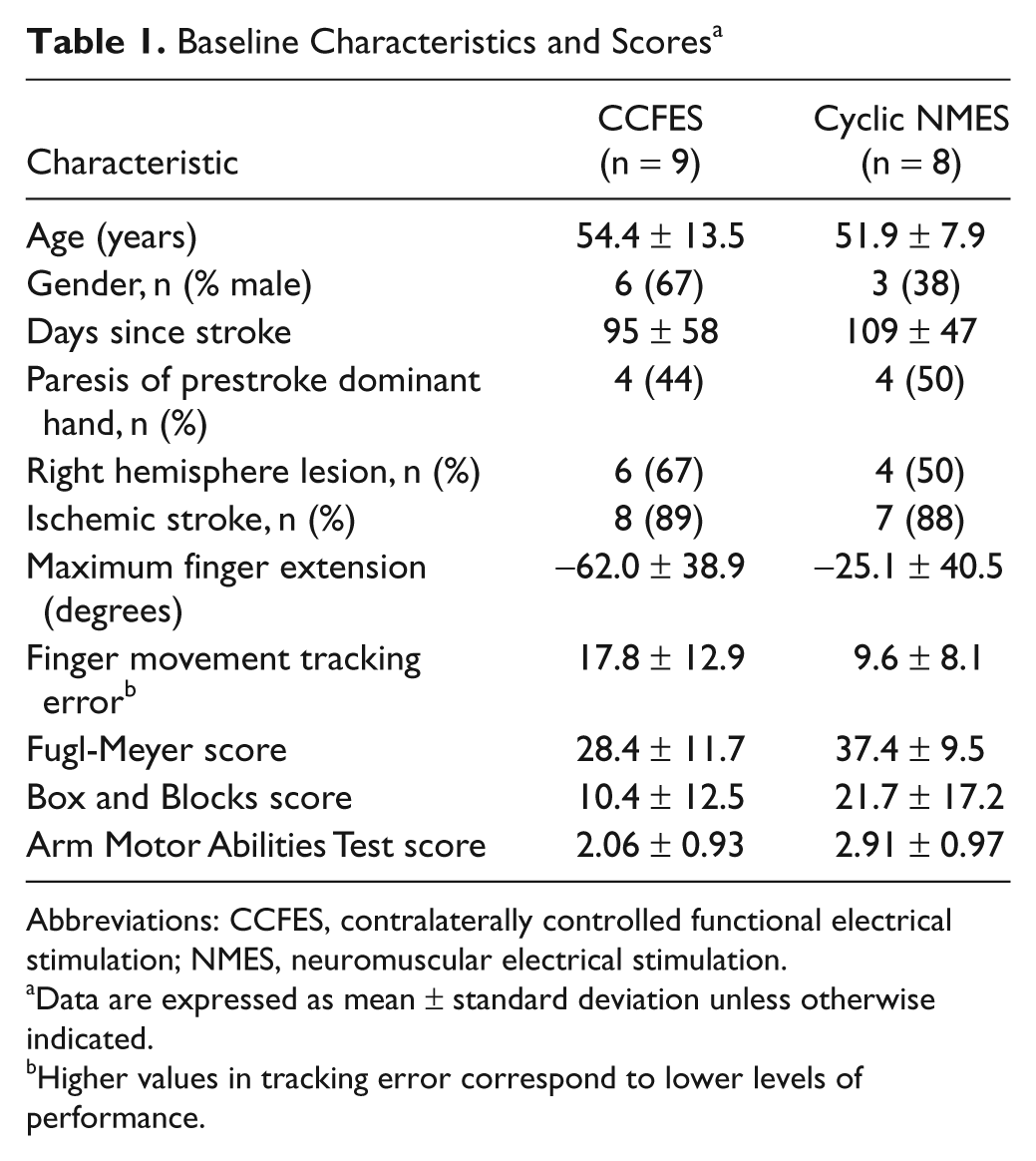
Abbreviations: CCFES, contralaterally controlled functional electrical stimulation; NMES, neuromuscular electrical stimulation.
Data are expressed as mean ± standard deviation unless otherwise indicated.
Higher values in tracking error correspond to lower levels of performance.
All the CCFES participants were able to put on the electrodes and glove independently. Compliance with the self-administered portion of the treatments was similar for both groups. All participants were prescribed 72 sessions of home stimulation exercise. According to the electronic data logger, the percentage (mean ± standard deviation) of prescribed sessions performed was 73 ± 27 for the CCFES group and 78 ± 26 for the cyclic NMES group. All participants were scheduled for 12 visits with the treating occupational therapist. The average number of visits kept was 11.0 ± 0.7 for the CCFES group and 10.4 ± 3.1 for the cyclic NMES group. Of the 9 CCFES participants, 6 (67%) had concomitant occupational therapy during the study’s treatment period compared with 7 of 8 (87%) cyclic NMES participants. The average number of hours of concomitant occupational therapy during the 6-week treatment period was 3.1 ± 2.9 for the CCFES group and 5.6 ± 3.8 for the cyclic NMES group.
The baseline-adjusted outcomes were more favorable for the CCFES group than the cyclic NMES group at every posttreatment time point and for every outcome measure. Table 2 lists for each outcome measure the mean baseline scores across both groups, the baseline-adjusted scores for each group at EOT, 1 month, and 3 months, and the estimated group differences (treatment effect). The treatment effect for all 5 outcome measures is in the direction supporting CCFES superiority. The outcome measure showing the largest treatment effect (having more than 90% of its 95% confidence interval favoring CCFES) was maximum voluntary finger extension, with the CCFES group having 28° more finger extension on average across the posttreatment time points than the cyclic NMES group and an upper 95% confidence limit of 59°. The mean baseline-adjusted scores for maximum finger extension are plotted in Figure 3 to depict the group differences, and the distribution of changes in maximum finger extension for both groups is shown in Figure 4.
Adjusted Means ± Standard Errors and 95% CIs for Treatment Effect
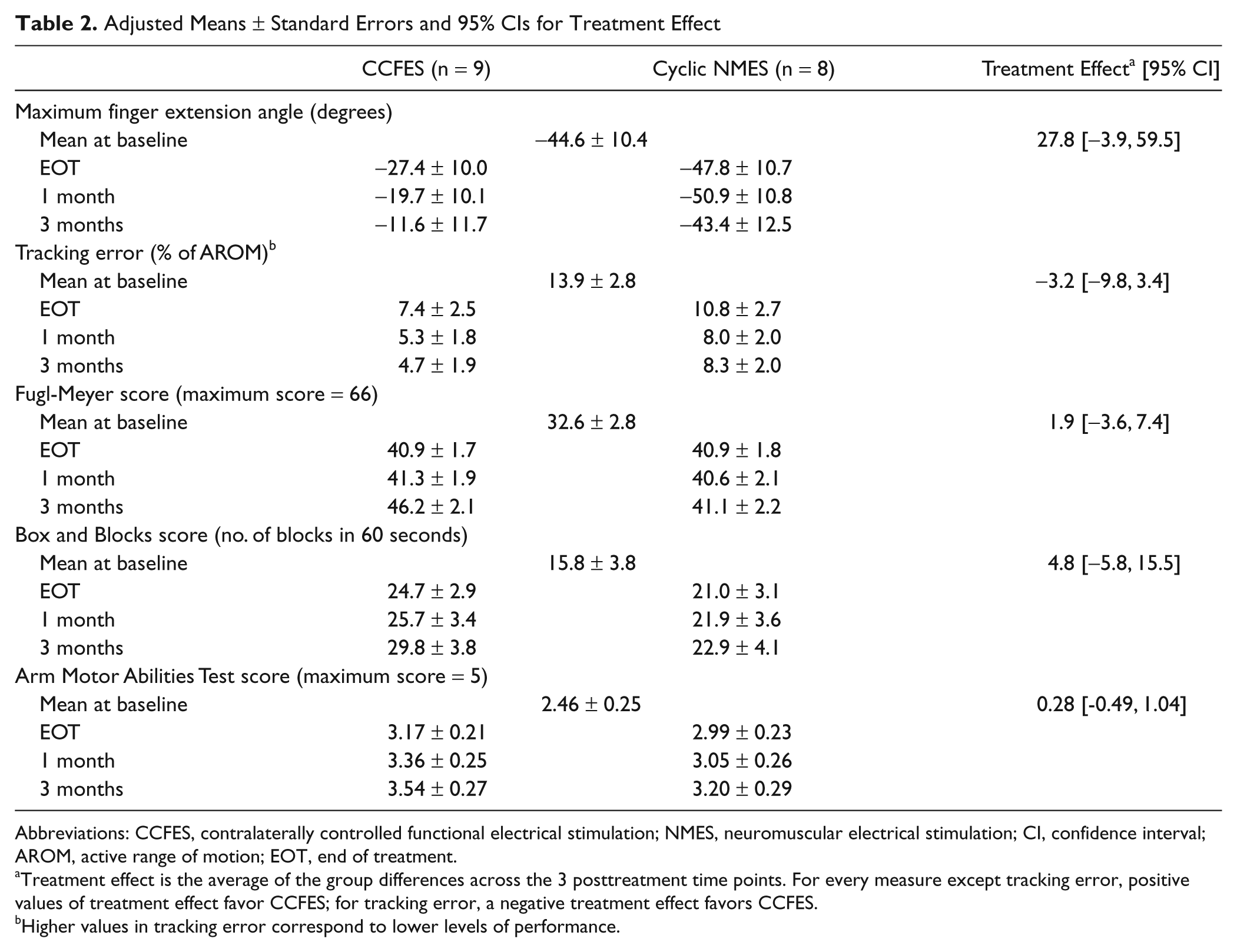
Abbreviations: CCFES, contralaterally controlled functional electrical stimulation; NMES, neuromuscular electrical stimulation; CI, confidence interval; AROM, active range of motion; EOT, end of treatment.
Treatment effect is the average of the group differences across the 3 posttreatment time points. For every measure except tracking error, positive values of treatment effect favor CCFES; for tracking error, a negative treatment effect favors CCFES.
Higher values in tracking error correspond to lower levels of performance.
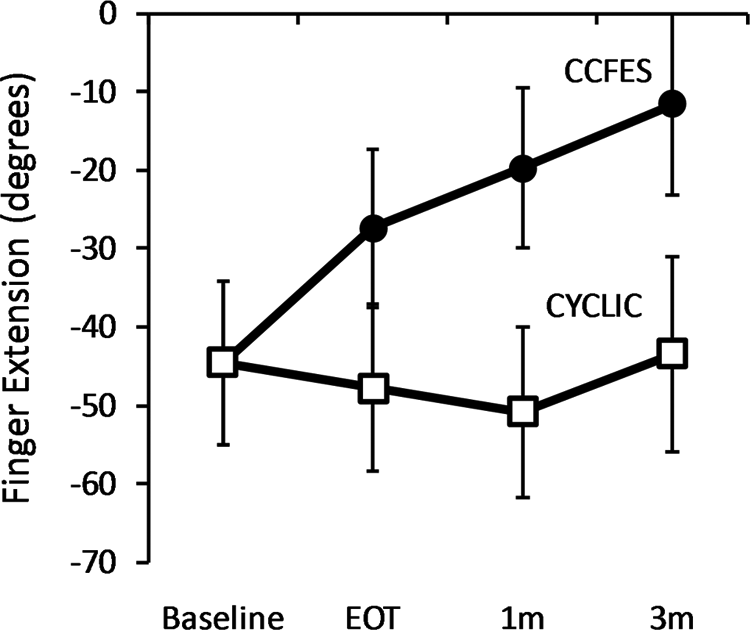
Maximum voluntary finger extension angle means and standard errors. Baseline value is the mean across subjects from both groups. Values at EOT, 1m, and 3m are baseline-adjusted scores
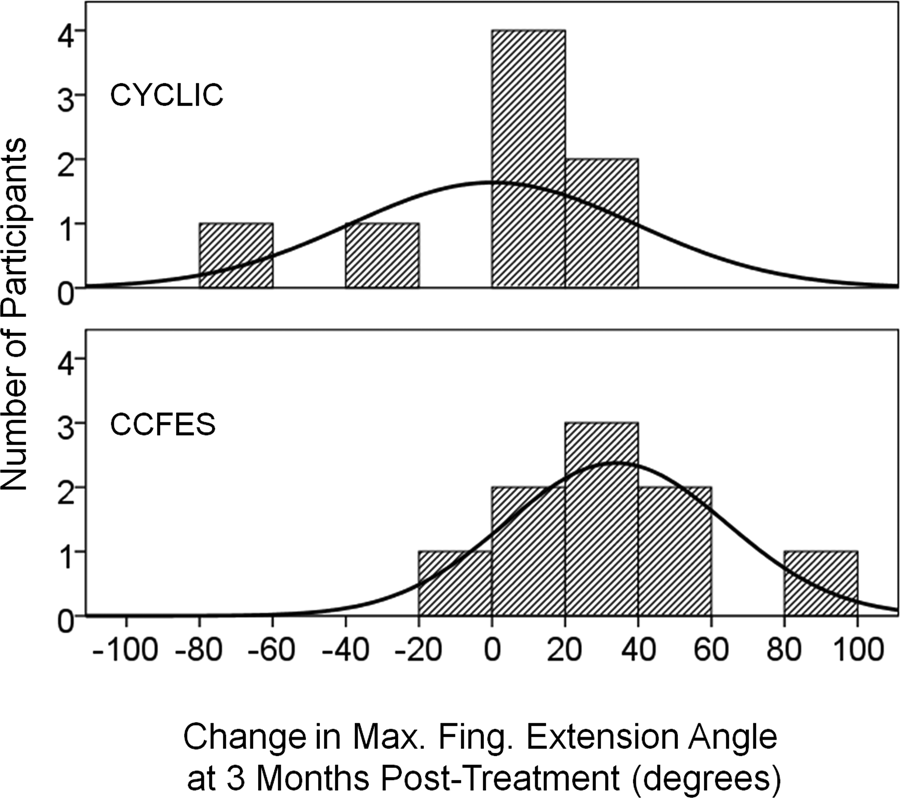
Distribution of maximum voluntary finger extension angle changes for cyclic NMES (top) and CCFES (bottom) participants
Discussion
This was the first randomized clinical trial of CCFES, a preliminary investigation of the hypothesis that CCFES is more effective than cyclic NMES in reducing hand impairment and activity limitation. Though an early-phase study, the results support this hypothesis. For every outcome measure the CCFES group experienced greater improvement than the cyclic NMES group (Table 2).
The largest treatment difference was seen with maximum voluntary finger extension, with 94% of its confidence interval favoring CCFES. This is not surprising, because this measure (of the 5 we used) captures the most fundamental level of hand motor impairment and therefore is expected to be most impacted by a treatment that emphasizes repeated active hand opening. The size of the treatment effect on maximum voluntary finger extension was 28°, an increase in finger extension at the MP and PIP joints that exceeds 10% of the total range of the scale, a criterion that has been suggested to define the minimal clinically significant difference. 27 For maximum voluntary finger extension, the total range of the scale would be approximately 200° (the maximum sum of MP and PIP angles) 28 and minimal clinically significant difference would be 20°. Although the other outcome measures also showed treatment effects in favor of CCFES, the sizes of those effects were not as large (a lesser proportion of the confidence interval was >0), probably because those measures require more global upper limb motor recovery. The treatment effects for the finger movement tracking error and the Box and Blocks Test each had ~74% of its confidence interval in favor of CCFES. Effect sizes of 3.2% and 4.8 blocks for these 2 measures, respectively, are approaching clinical relevance. The treatment effects for the Fugl-Meyer motor assessment and AMAT each had ~68% of its confidence interval in favor of CCFES. Treatment effects of 1.9 and 0.28 for these 2 measures, respectively, are not clinically relevant. Perhaps a longer treatment duration and further treatment optimization would produce changes large enough to reach statistical and clinical significance on all of these outcome measures.
The imbalance between groups in the degree of impairment at baseline made it imperative to adjust for baseline scores. Without adjustment, the cyclic NMES group had better pretreatment and posttreatment scores than the CCFES group. However, the CCFES group had greater average gains from their baseline scores than the cyclic NMES group (Figure 4). The greater gains achieved by the CCFES group may in part be because the cyclic NMES group was more mildly impaired than the CCFES group at baseline and therefore may have had less room to improve (ie, ceiling effect) on some outcome measures (eg, maximum voluntary finger extension). Adaptive randomization will be used in future studies to minimize group imbalances on key patient characteristics such as severity of impairment.29,30
Given the small sample size and exploratory nature of this study, there was no expectation of demonstrating statistical significance, and indeed the 95% confidence intervals around the mean differences included zero for every outcome measure, even when not accounting for multiple comparisons. However, if this particular sample of subjects had been tripled in size (eg, n = 27 per group), we would have been able to detect a true treatment effect size of 0.5 on the AMAT (minimal clinically significant difference) with probability (power) of .80 and α = .05 (type I error rate). Thus, the data generated in this study have allowed us to estimate effect sizes and determine the sample size needed to properly power a future randomized clinical trial.
This study has several limitations. The heterogeneity of the sample likely increased the variance in the outcomes and diluted the power to detect differences between the 2 treatment groups. We did not monitor whether the CCFES participants indeed exerted effort to open both hands in response to the cues, or ensure that cyclic NMES participants neither exerted effort to open the paretic hand in synchrony with the stimulation nor opened their contralateral unaffected hand in synchrony with the stimulation. In spite of major sources of potential bias, the finding that CCFES was superior to cyclic NMES suggests that we need to optimize the CCFES treatment and confirm the preliminary findings here in a properly powered trial.
Footnotes
Acknowledgements
We gratefully acknowledge Kristine Hansen, PT, and Maureen T. Hennessey, PT, for their assistance with outcomes assessment. The NMES stimulators used in this study were developed by the Technical Development Laboratory of the Cleveland FES Center.
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article:
This work was supported by the National Institutes of Health (NIH) National Institute of Child Health and Human Development (NICHD), Grant No. R21HD054749.
*
Cyclic NMES: 15 min/set × 4 sets × (2 sets/d × 5 d/wk + 1 set/d × 2 d/wk) = 12 h/wk. CCFES: 15 min/set × 3 sets × (2 sets/d × 5 d/wk + 1 set/d × 2 d/wk) + 90 min/lab × 2 labs/wk = 12 h/wk.