
Abstract
Background. Sideways reaching with the unaffected arm while seated is a component of everyday activities and can be a challenging task early after stroke. Kinematic analysis of a lateral reach task may provide potential rehabilitation strategies. Objective. The authors examined the difference between people with stroke and healthy controls in the movement sequence of head, trunk, and pelvis, as well as the difference in angle at maximum reach and peak velocity for each body segment during reach and return. Methods. Twenty-four people within 12 weeks of a stroke and 20 healthy subjects performed a standardized lateral reach. Using CODAmotion, movement sequence was determined and angles and peak velocities were calculated. Results. When reaching, people with stroke moved their pelvis first, followed by the trunk and head, whereas healthy controls started with their head and then moved their trunk and pelvis. Patients achieved significantly smaller angles at maximum reach compared with healthy subjects for all body segments and lower peak velocities during the reach (for head, trunk, and pelvis) and the return (for head and trunk). Conclusions. Lateral reaching to the unaffected side early after stroke revealed a different pattern than normal and patients reached less far and moved at a slower speed. Specific training strategies to improve reaching are needed.
Introduction
Disability persists in more than 75% of people after stroke, leading to dependency in daily activities. 1 For people after stroke to successfully execute activities of daily living, postural control is crucial. Early sitting balance is an independent predictor of motor and functional outcome. 2-4 During several activities of daily living, sitting balance is necessary to reach laterally with the unaffected upper hand, for example, to grasp the salt holder from the other side of the table.
The biomechanical analysis of sitting balance in people after stroke has usually been examined by a force platform to report center of pressure displacements and velocities. Patients require greater center-of-pressure displacements and increased velocities when compared with healthy controls. 5 Greater lateral displacement when reaching forward and less lateral displacement when reaching sideways to the affected side has also been reported. 6 In addition, lateral sitting balance control was more impaired after stroke than balance in the anterioposterior direction, and lateral sitting balance showed the strongest association with the Berg Balance Scale score. 7 Lateral balance in a sitting position, then, ought to be targeted for rehabilitation. 7
Only a few studies addressed the kinematics of a lateral reach after stroke. Katz-Leurer et al 8 found that during sideward reaching, patients reached significantly less far when compared with healthy controls. Campbell et al 9 investigated the speed, distance reached, and angular movement of the head and pelvis in a lateral reaching task in healthy subjects and 5 patients after stroke. The latter reached shorter distances at lower speed, but these differences were not significant. 9 Additional kinematic analysis on a larger sample of people after stroke that includes the trunk, head, and pelvis may increase our understanding of balance and lateral reach and provide potential rehabilitation strategies.
To assess differences in kinematics of a lateral reach task between people with stroke and healthy controls, a cross-sectional study was designed. We examined the difference in movement sequence of head, trunk, and pelvis, as well as the difference in angle at maximum reach and peak velocities during reach and return for each body segment. We hypothesized that people early after stroke would have an altered movement sequence in comparison with healthy controls and that angles of lateral displacement and velocity of movement of head, trunk, and pelvis would be less in comparison with healthy controls. Analysis of preliminary data of angular displacement of the trunk showed the lateral reach paradigm (Figure 1) in which 4 phases were identified when performing a lateral reach: initiation, reach, return, and recovery. 10,11 In an additional exploratory analysis, we examined whether this paradigm could also be applied to the head and pelvis and if there was a difference between people with stroke and healthy subjects. Duration of the phases was compared between both groups, as well as the angles and velocities during initiation and recovery. These latter phases could be of further interest when performing a lateral reach, as they might indicate preparation (initiation) or relaxation (recovery) of postural setting by means of postural adjustments prior to a reach or after a return, respectively. 12
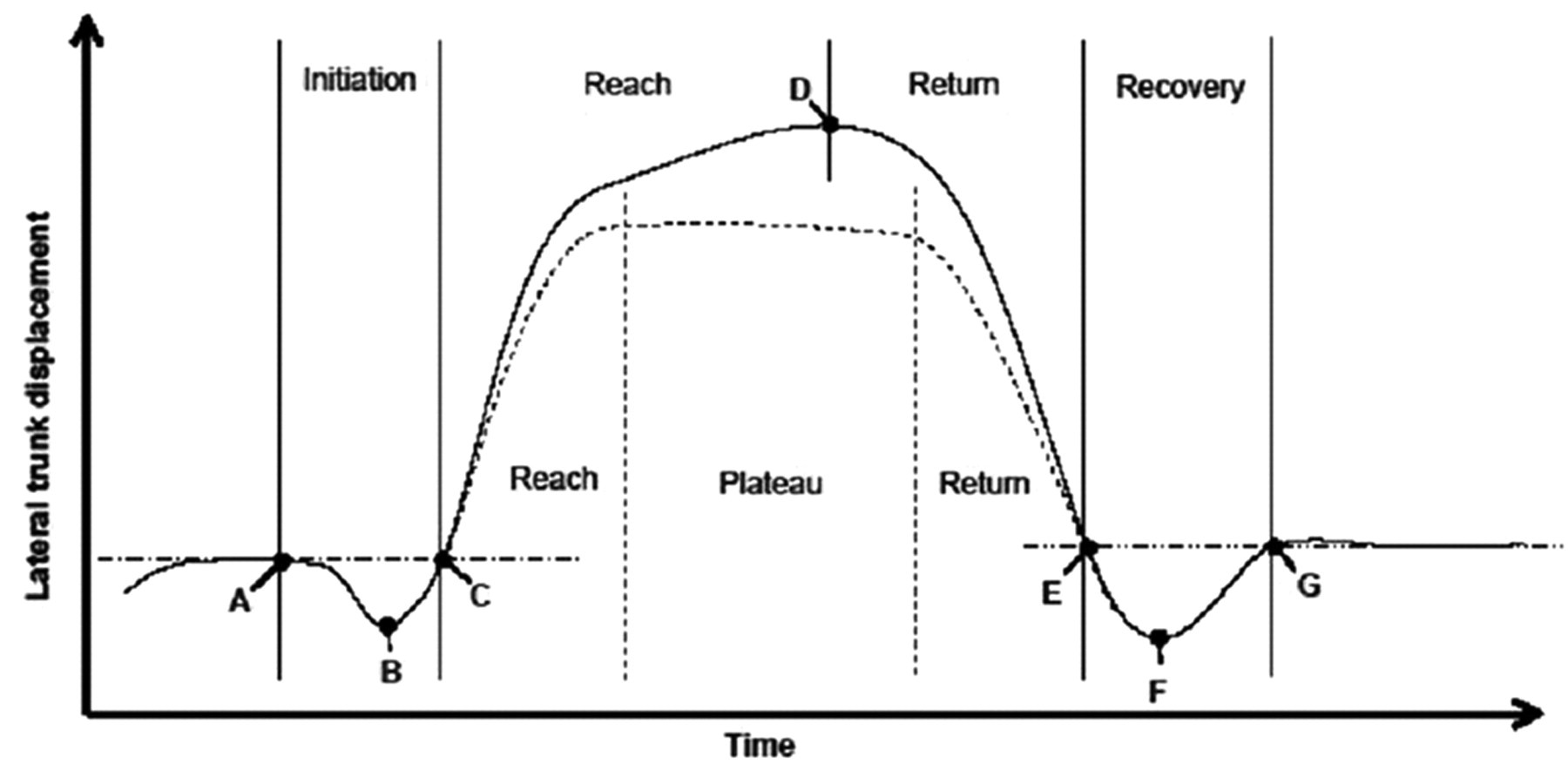
Lateral reach paradigm of the trunk. The paradigm based on preliminary results of angular displacement of the trunk, showing 4 phases of lateral reach: initiation, reach, return, and recovery. Some subjects showed a plateau phase from the point of maximum reach. A, Start of initiation. B, Peak of initiation. C, End of initiation/start of reach. D, Maximum reach. E, End of return/start of recovery. F, Peak of recovery. G, End of recovery.
Methods
Subjects
A total of 25 people with a first-ever stroke according to the World Health Organization definition 13 were included in this study. They had to be independently mobile prior to the stroke event. Exclusion criteria were history of other neurological impairment and other factors such as impaired vision, uncontrolled hearing, musculoskeletal and vestibular deficits, or other balance disorders. They were assessed within 12 weeks after stroke.
Twenty healthy adults volunteered as a control, age-matched sample. They were all aged 60 years and older. Volunteers were excluded if there was a presence of neurological conditions, history of stroke, impaired vision, uncontrolled hearing, musculoskeletal and vestibular deficits, or other balance disorders.
The protocol was approved by the Isle of Wight, Portsmouth & South East Hampshire Local Research Ethics Committee. All participants provided informed consent.
Procedure
Baseline data were obtained from participants and from medical records (Table 1) and included age and gender and for people with stroke the type of stroke, side of lesion, Rivermead Motor Assessment, 14 and Motricity Index. 15
Demographics a
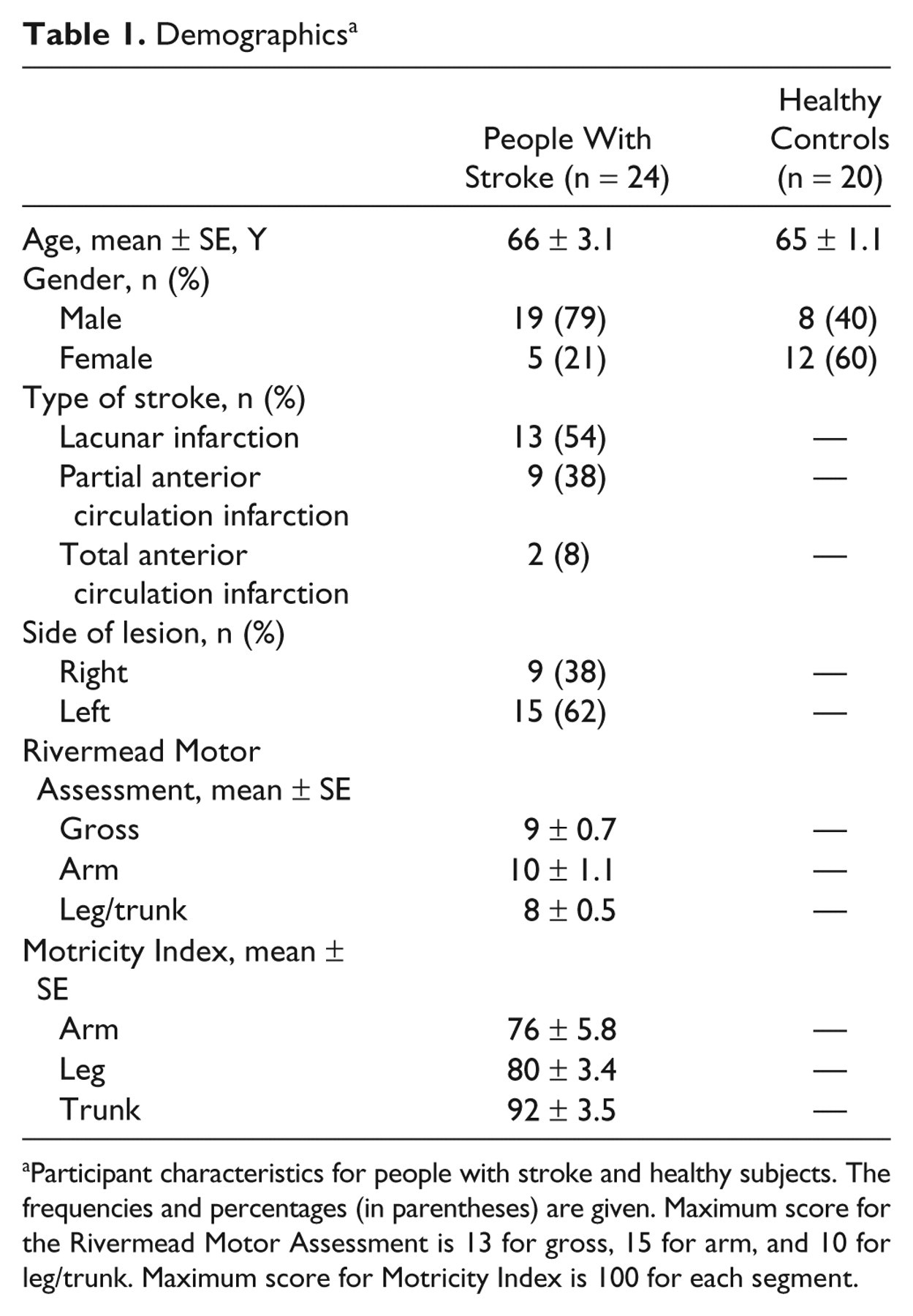
Participant characteristics for people with stroke and healthy subjects. The frequencies and percentages (in parentheses) are given. Maximum score for the Rivermead Motor Assessment is 13 for gross, 15 for arm, and 10 for leg/trunk. Maximum score for Motricity Index is 100 for each segment.
A lateral reach task was performed as follows (Figure 2). When sitting without back and arm support, people after stroke were asked to reach with the unaffected hand to the unaffected side as far as comfortably possible. Healthy controls reached to a randomly determined side and used the same strategy and received the same command. Both groups were asked to focus on a fixed point directly in front of them to minimize any rotational component of head and shoulders. Subjects were allowed to tilt their pelvis while reaching and to use the contralateral leg as a counterbalance. Subjects were seated on a height-adjustable plinth, so that hip and knees were at 90 flexion. They were asked to perform the task 3 times. The lateral reach task was recorded using CODAmotion (Charnwood Dynamics Ltd, Leicester, UK), a 3-dimensional movement analysis system. This system is noninvasive and uses up to 24 light emitting diodes to record joint angle and time/distance factors. For our current set up, we used 2 markers on the face; 1 marker between the eyes, and 1 marker on the chin. We also used a marker on the top of the sternum and 1 marker on each anterior superior iliac spine (ASIS).
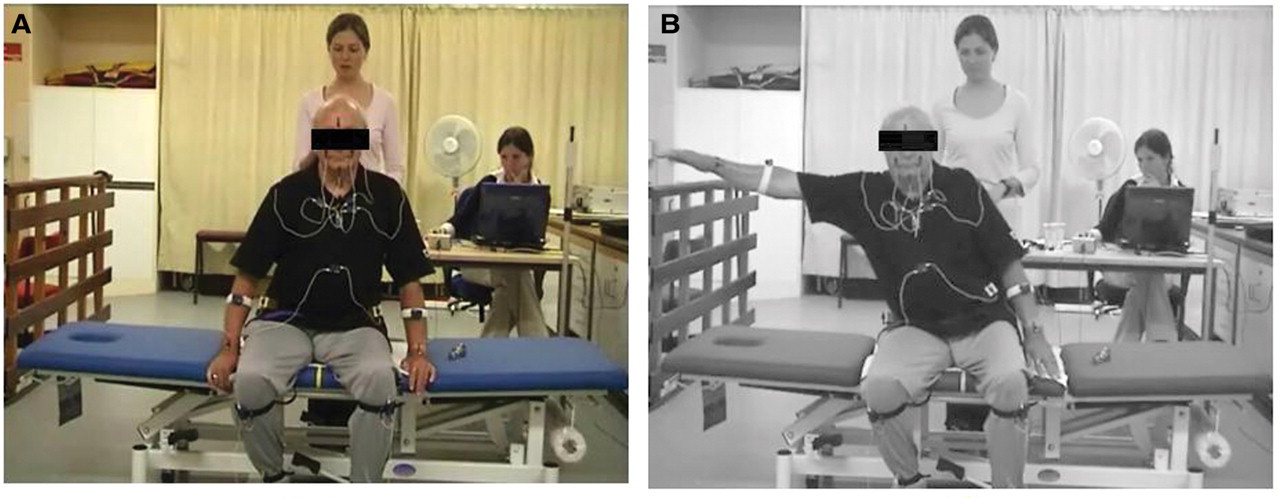
Lateral reach task. Participants were instructed, from the starting position (A), to reach to the side with their ipsilateral hand as far as comfortably possible (B). For people with stroke, this was done to their unaffected side; for healthy controls, to a randomly determined side.
Data Collection
Based on preliminary results of lateral trunk movements, a paradigm was created (Figure 1). This paradigm showed lateral movement of the trunk when performing a lateral reach. Before starting with the actual reach, participants showed an initiation phase in the opposite direction of the reach. Then we noted the reach phase when reaching out and the return phase when coming back to the starting position. After the return phase, we observed a recovery phase with again a trunk movement in the opposite direction of the reach. Some of our participants showed from the point of maximal reach a stable plateau, before starting with the return.
Using the CODAmotion analysis system, angles of head and trunk displacement were calculated relative to the vertical plane. We connected the 2 CODAmotion markers on the face to construct the vertical face reference. The vertical trunk reference was created by connecting the sternum marker with the middle of the 2 ASIS markers. Angles of pelvis displacement were calculated relative to the horizontal plane; the horizontal pelvis reference was constructed by connecting the 2 ASIS markers. Using graphs of lateral displacement of the angles, outcome measures were calculated. For each segment, first the baseline angle and time were determined (point A in Figure 1). A mean was calculated for the angles of the movement before the actual reach began. If there was an initiation phase, the peak angle of the initiation (B) and time of the end of the initiation (ie, start of reach; C) was noted. In addition, the time and angle of maximum reach (D) were determined. The start of return was defined as the point of maximum reach or the end of the plateau (see Figure 1). The final time and angle (G) were calculated similarly to those of the baseline. For files with a recovery, the peak time and angle (F) and the start of recovery (ie, end of return; E) were noted. This was done for all subjects, for all 3 attempts after which a mean was calculated for each variable per subject. To calculate moving sequence of head, trunk, and pelvis, we used the initial start of head movement in the lateral plane as the starting point for calculating start of the reach and return of head, trunk, and pelvis.
Statistical Analysis
First, we visually examined the movement sequence for the reach and the return by means of plotting bar charts of start of head, trunk, and pelvis movement for people after stroke and healthy controls separately. We examined whether differences between people with stroke and healthy controls as well as within-group movement sequences were significant by means of independent and paired t tests, respectively. Second, angles of maximum reach for head, trunk, and pelvis and peak velocity of head, trunk, and pelvis during reach and return were compared between groups by means of independent t tests. Third, we calculated time of each phase as percentages and compared these normalized durations of initiation, reach, return, and recovery for head, trunk, and pelvis between our 2 groups by means of independent t tests. Fourth, we noted for how many people after stroke and healthy controls there were initiation and recovery phases according to our lateral reach paradigm for head, trunk, and pelvis. Finally, we examined whether there were differences in peak angle and velocity in the initiation and recovery phases between people after stroke and healthy controls by using independent t tests. We reported mean ± standard error for all continuous variables. All analyses were performed using SPSS statistics (version 17.0 IBM; Somers, New York). The alpha level was set at .05.
Results
For 1 of our 25 people after stroke, data were corrupted and had to be excluded. For all other participants, CODAmotion analysis could successfully be executed. Overall, people after stroke took longer to perform the total lateral reach task in comparison with healthy controls (12.98 ± 0.65 vs 9.88 ± 0.71 seconds, respectively; P = .003).
Movement Sequence
Figure 3 shows the movement sequence for the start of lateral reach. People with stroke relatively moved the pelvis first, followed by the trunk and head. In contrast, healthy subjects started the lateral reach with the head, followed by trunk and pelvis. Start of head and trunk movement for the reach was significantly later in people after stroke in comparison with healthy controls (head: 1.15 ± 0.27 vs 0.09 ± 0.25 seconds, P = .007; trunk: 0.9 ± 0.30 vs 0.14 ± 0.12 seconds, P = .026). There were no significant differences between the body segments within both groups.
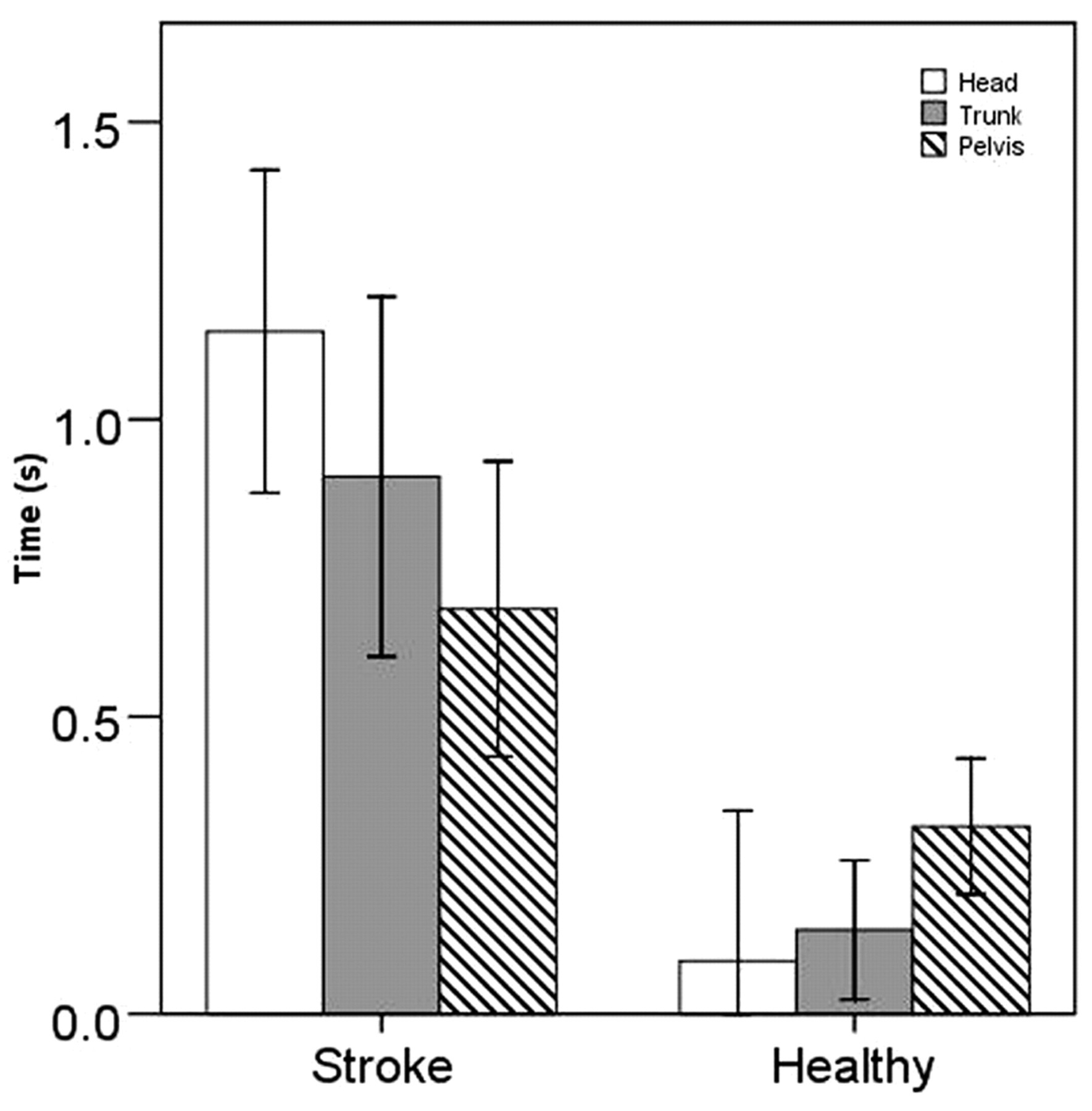
Movement sequence reach. Mean (±1 SE) start of reach (seconds) of head (white), trunk (grey), and pelvis (striped pattern) for people with stroke and healthy controls.
Start of movement of the different body segments for the return is shown in Figure 4. No clear sequence could be observed. Start of head, trunk, and pelvis movement for the return was significantly later in people after stroke in comparison with healthy controls (head: 8.89 ± 0.67 vs 5.45 ± 0.45 seconds, P < .01; trunk: 8.28 ± 0.60 vs 5.32 ± 0.49 seconds, P < .01; pelvis: 8.45 ± 0.62 vs 5.48 ± 0.45 seconds, P < .01). There were no significant differences between the body segments within both groups.
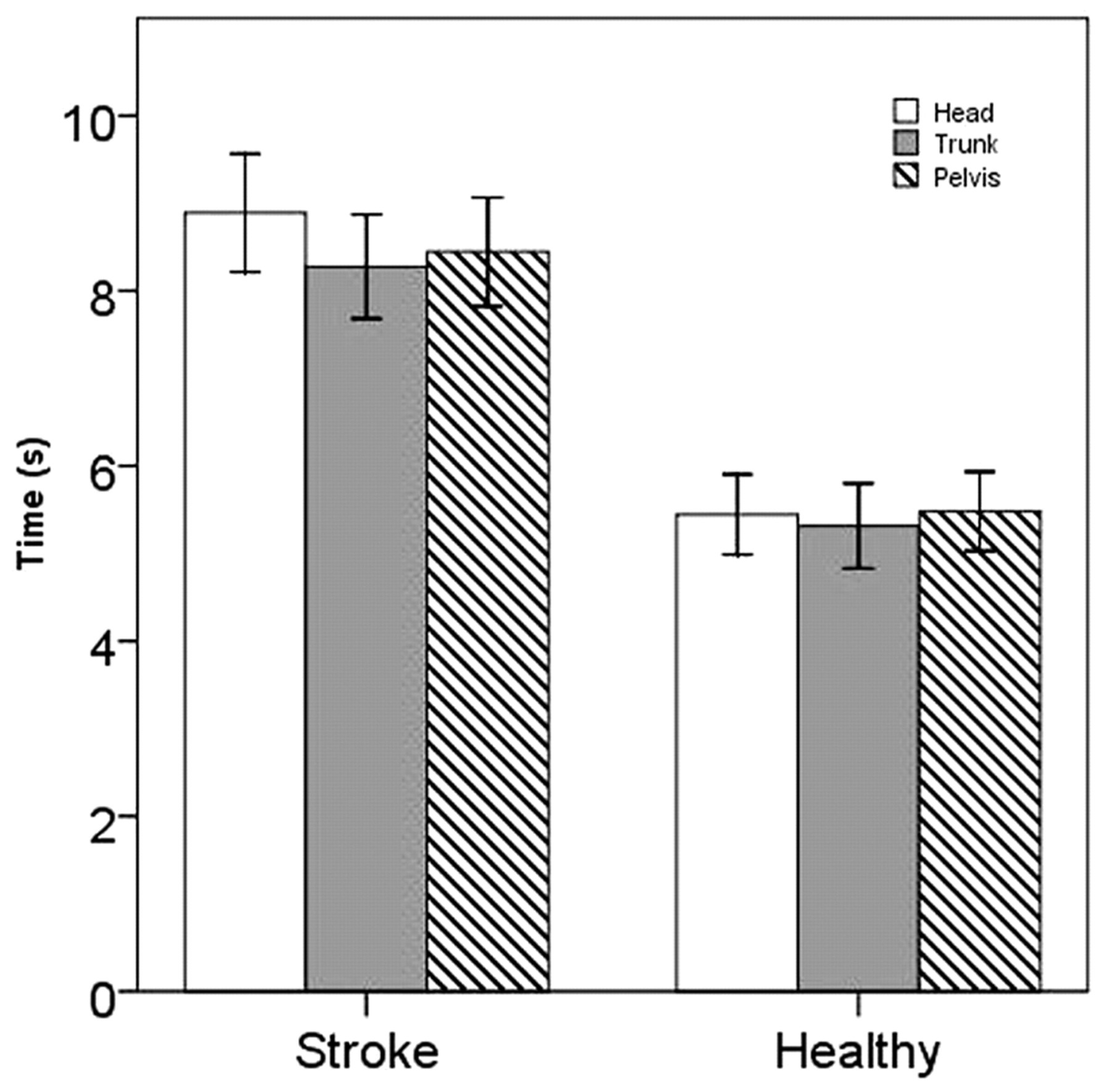
Movement sequence return. Mean (±1 SE) start of return (seconds) of head (white), trunk (gray), and pelvis (striped pattern) for people with stroke and healthy controls.
Reach and Return
People with stroke showed significantly smaller angles for head, trunk, and pelvis position at the point of maximum reach when compared with healthy controls (Table 2). Normalized durations of the reach and return phases for people with stroke were not significantly different in comparison with healthy controls, neither for head, trunk, or pelvis (Table 2).
Angles, Normalized Durations, and Velocities of a Lateral Reach a
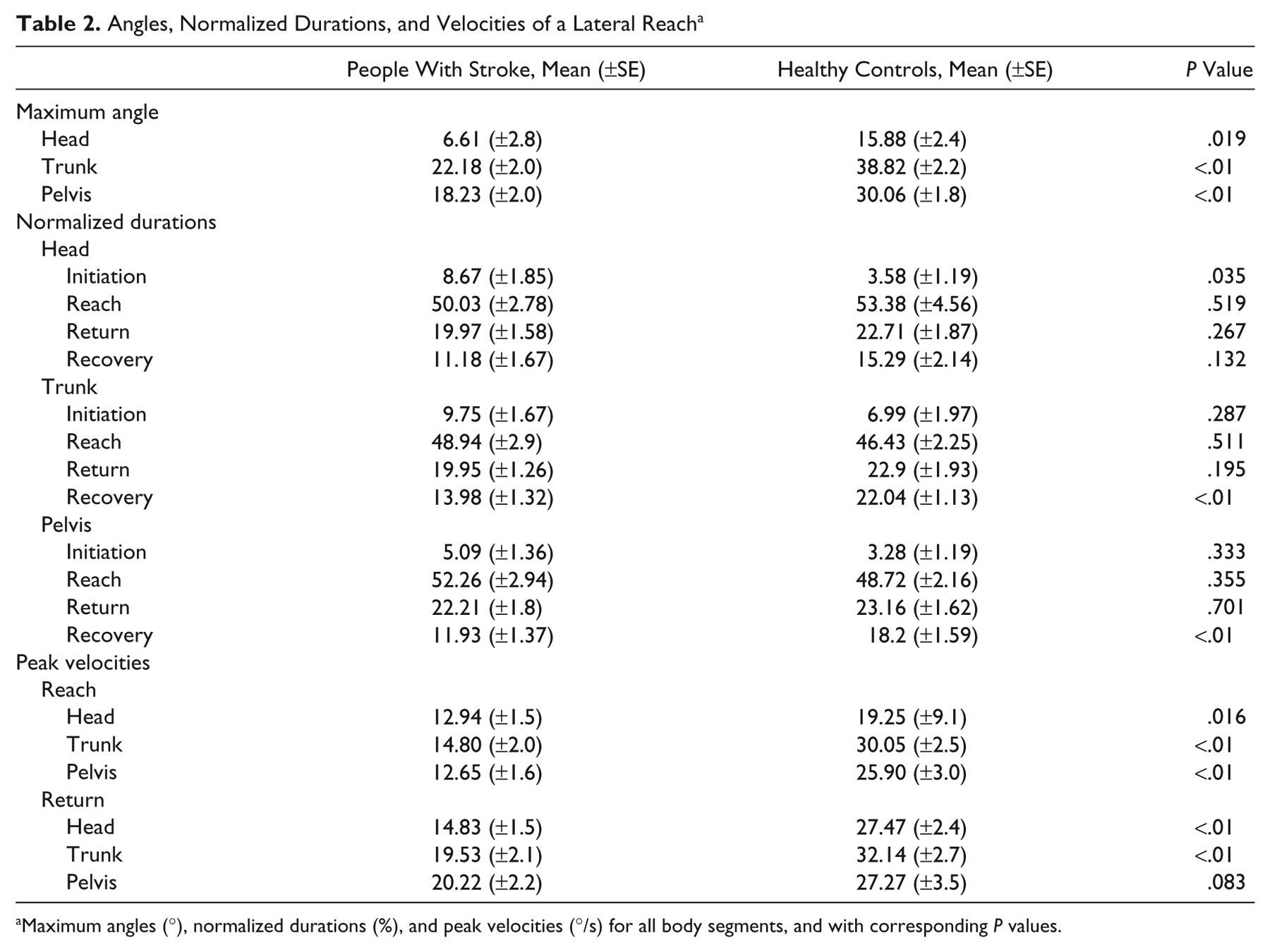
Maximum angles (°), normalized durations (%), and peak velocities (°/s) for all body segments, and with corresponding P values.
Peak velocities for all body segments indicated that people after stroke were clearly slower, both when reaching and returning (Table 2). This was significantly different in all body segments for the reach. For the return, this was significantly different for peak head and trunk velocity.
Initiation and Recovery
For the head, an initiation was seen in 50% of people after stroke and 25% of healthy controls, a recovery was seen in 75% and 85%, respectively. More initiations were observed in the trunk, 67% in people after stroke and 80% in healthy controls. This was also the case for recovery of the trunk, 92% and 95%, respectively. Fewer initiations were noted for pelvis movement in people after stroke (46%) and healthy controls (35%), whereas the incidence of recovery was similar to that of the trunk (92% and 95% for people after stroke and healthy controls, respectively).
In people after stroke, there was a significantly longer duration of the initiation of head movement in comparison with healthy controls (Table 2). For people with stroke, we also found a shorter recovery for trunk and pelvis movement compared with healthy controls (Table 2).
For those participants who showed an initiation or recovery, no differences in peak angle of head, trunk, and pelvis position were seen between both groups. We only noted smaller peak velocities in people after stroke for the second part of trunk initiation (6.27 ± 0.92°/s vs 12.09 ± 1.58°/s; P = .002) and the first part of trunk recovery (13.75 ± 1.22°/s vs 21.06 ± 1.91°/s; P = .003) in comparison with healthy controls.
Discussion
The aim of this study was to conduct a kinematic analysis of the lateral reach, a frequently used clinical task in stroke rehabilitation, wherein participants are in a sitting position and reach to the side as far as comfortably possible and subsequently return to the starting position. We were interested in the sequence of movement as well as the lateral displacement and velocity of head, trunk, and pelvis during a lateral reach, and we hypothesized that people after stroke would have an altered sequence of movement and that our kinematic parameters would be decreased in people after stroke in comparison with healthy controls.
Our results with regard to movement sequence at the onset of reach did show an altered pattern of movement. People after stroke had a relatively contrary movement sequence in comparison with healthy controls with significantly longer onset latencies of head and trunk movement in the lateral plane. We observed a relative top-to-bottom movement sequence in healthy controls; the head moved before the trunk and the trunk before the pelvis. This might be as one expects and is in line with the top-to-bottom movement sequence presented in the literature examining whole-body coordination while turning in healthy controls. 16 Our relatively contrary results for people early after stroke indicated that the pelvis moved first followed by the trunk and head. In our study, movement was defined as a deviation from the horizontal room axis in the case of the pelvis and from the vertical room axis in the case of trunk and head. This means that our sample of people after stroke started to move from the pelvis but they kept the trunk and head aligned in their original position when reaching sideways, which suggests an “en bloc” movement. The point where the trunk and head then started to move away from the vertical room axis was found to be significantly delayed when compared with healthy controls. Reisman and Scholz 17 examined surface force production during lateral seated reaching and found a delayed onset of mediolateral seat force, which seems to be in line with our present findings.
Our results for the movement sequence of the return showed very similar patterns for both groups, but people after stroke started to move their head, trunk, and pelvis significantly later than healthy controls. It is important to be cautious when interpreting these results, because the onset of the movement of the body segments for the return are relative to the initial lateral head movement of the reach. Nevertheless, it is noteworthy that for healthy controls and people after stroke, the movement sequence was very comparable and in this prospect different from the result from the reach. This difference could be explained in several ways. When reaching sideways, away from the base of support, muscles have to work concentrically and the person is moving to a more unstable position. On the return, muscles have to work eccentrically and control the descent toward the starting position, thus one is moving toward a safer position. It might be the case that the assistance of gravity in the return phase of the lateral reach is a less challenging task and facilitates a movement pattern more closely related to that seen in healthy controls. To the best of our knowledge, this movement sequence has not been described in the literature before and is of interest for clinical practice. The fact that onset latencies for head, trunk, and pelvis movement in the return phase were delayed in people with stroke in comparison with healthy controls can be explained by the result of a post hoc analysis using the raw times, indicating that the time it took to achieve the point of maximum reach was significantly longer for people after stroke in comparison with healthy controls. However, this difference was not significant in the normalized times that we presented here (Table 2). We decided to present normalized times based on the fact that overall times for the lateral reach were significantly different between both groups. Furthermore, one should note that not only peak velocities were significantly decreased for people after stroke but also maximum angles. These 2 variables combined could also explain the discrepancy found between significant delay of onset latency for the return and nonsignificant normalized durations of the reach and return phases.
At the point of maximum reach, angles of the head, trunk, and pelvis were significantly lower for people after stroke in comparison with healthy controls, which confirms the findings of other researchers. 6-9 Our study contributes to the body of knowledge of kinematics of the lateral reach in people after stroke, and more specifically, we were able to confirm the findings of Campbell et al, 9 who suggested that people after stroke reached less far and had lower speed of movement when reaching to the side. Their study included a limited sample of people after stroke (n = 5), and they only observed head and pelvis movement. In our study, we were able to recruit a larger number of participants and included head, trunk, and pelvis measurements during the reach as well as the return. We found significant differences for peak velocity for all segments during the reach and for the head and trunk during the return. Further studies could investigate how these findings progress during the recovery from the very early stage after stroke until the chronic phase, as well as the relation with motor and functional outcome after stroke. Further research into this area seems justified based on our results as well as from previous literature looking into the clinical measurement of a lateral reach.
Among the standardized clinical assessments of lateral trunk control, a simple lateral functional reach test 8 had high reliability and significantly correlated with Balance Master measures, indicating validity. The dynamic sitting balance subscale of the Trunk Impairment Scale 18,19 also examines lateral trunk control; small controlled trials have found that trunk exercise improves selective performance of lateral flexion of the trunk after stroke. 20 Task practice to prevent compensatory trunk motion may improve reaching kinematics. 21,22
We examined in more depth our original paradigm of lateral trunk movement (Figure 1) during the lateral reach with 4 phases: initiation, reach, return, and recovery. We proposed that this paradigm could also be applied to lateral movements of the head and pelvis and, by utilizing the 4 phases, to describe angles and velocities throughout the movement cycle. The recovery phase at the end of the return was of particular interest in our study. Some of our participants demonstrated an adjustment of body position following an overshoot. We believe this relates to the fact that peak velocities for the return were relatively higher than for the reach—for all segments and for both groups. Bringing a body segment back to its starting position and controlling the eccentric descent apparently involves obtaining control over an overshoot of this body segment after the return phase. We also noted a significantly shorter duration of recovery for trunk and pelvis in people after stroke. We believe this could relate to the fact that people after stroke reached significantly less far than healthy controls and, therefore, less eccentric trunk and pelvis movement was needed. We believe this also explains the smaller peak trunk velocity found in the first part of trunk recovery.
Limitations and Directions for Future Research
Our sample was relatively small and only mildly impaired. Replication is needed on a group of very acute people with stroke with more severe impairments. Furthermore, we evaluated lateral reach only to the unaffected side. This was based on (a) the fact that our task was part of a larger protocol that included different clinical tasks as well as 3-dimensional observations and (b) people after stroke in our study generally had an upper limb impairment and could not bring their arm in the standardized position to perform a lateral reach task. In addition, we focused on lateral displacements in our analysis and acknowledge that there might be a rotational component as well as a displacement in the sagittal plane when reaching to the side. By asking our subjects to focus on a visual target in front, we believe we have minimized these additional movements to obtain optimal standardization of our clinically important task. Finally, further suggestions for future studies could include the use of 3 markers to determine the center of the pelvis: the kinematic analysis of the upper (shoulders) and lower part of the trunk (pelvis) separately, and the inclusion of a biomechanical analysis of the supporting role of thighs and feet.
Conclusion
Our cross-sectional study of the kinematic analysis of the lateral reach in people after stroke showed clear deficits of head, trunk, and pelvis movement in the different phases of the lateral reach. Reduced peak angles and velocities of head, trunk, and pelvis movement indicated that people after stroke with mild motor impairments have kinematic impairments when performing a lateral reach. These findings can inform clinical practice as a lateral reach is a common activity in rehabilitation and everyday life. Therapists and people with stroke should be alerted to the reduced movement and the tendency to move en bloc, which suggests less freedom to move or to respond to disturbances of stability. It could be argued that the emphasis in rehabilitation should be on providing opportunities to facilitate total body movement and movement at the different sections of the body during functional tasks such as reaching. Speed of movement should be monitored and trained, with emphasis on the control of eccentric descent during lateral reach.
Footnotes
Acknowledgements
The authors acknowledge the expert discussions with Robert Allen, Neil Shepard and Denise Taylor, and the other investigators, researchers and contributors of The Stroke Association Rehabilitation Research Centre; Jane Burridge, Pamela Crawford, Giles Durward, Caroline Ellis-Hill, Carolyn Fitton, Damian Jenkinson, Joseph Kwan, Kath McPherson, Anna Orpen, Hugh Perry, Ruth Pickering, Helen Roberts, Judy Robison, and Rose Wiles.
The author(s) declared no potential conflicts of interest with respect to the authorship and/or publication of this article.
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This study forms part of a larger programme of research funded by The Stroke Association (UK).