
Abstract
Background. Coverage policy ultimately determines the delivery of services. This article summarizes the authors’ effort to ascertain the extent of publically available information on coverage for neurorehabilitation services internationally. Objective. Present available data on neurorehabilitation coverage and examine the needs for further research in this area. Methods. Review of published literature, review of government Web sites, survey of World Federation of NeuroRehabilitation (WFNR) program chairs, and attendees of the 2010 World Congress of NeuroRehabilitation. Results. A wide variation in coverage was found internationally. Data are not routinely accessible. Conclusions. Informed policy requires current data. There is an opportunity for the WFNR to provide leadership in policy for neurorehabilitation services by assembling and maintaining current data on coverage policy internationally.
Introduction
Government and other third-party coverage and reimbursement policies largely determine which neurorehabilitation services will be available to our patients. Scientific evidence can determine which interventions are efficacious in clinical practice and what is effective in the community; however, which services receive reimbursement ultimately determines what services will be delivered. Because of this compelling importance, coverage and financing policy was identified as a discussion topic for the 2010 World Federation of Neurorehabilitation Congress in Austria. In preparation, an extensive literature search and a small survey was undertaken to assess variation in contemporary coverage and financing policy for neurorehabilitation services internationally. This article will review what was learned and discuss trends in policy as well as needs for future research.
Methods
Our approach to data collection included an extensive literature review, supplemented by a survey administered to the program chairs for the World Federation of NeuroRehabilitation (WFNR) and feedback obtained from country experts after a presentation of the findings at the WFNR meeting. We supplemented information from government sources with published literature and this convenience sample of practitioners and experts, since the situation in reality can be significantly different than the stated policies of the government or other third-party payers (see, eg, services provided for traumatic brain injury [TBI] in Ireland). 1
Our literature review included the medical literature through PubMed and surveys of government Web sites. PubMed searches on “neurorehabilitation” AND “coverage policy” retrieved 10 articles, none of which were relevant to the present discussion; “rehabilitation” AND “health policy” retrieved 4391 articles and 650 reviews. Few of these appeared relevant so this strategy was abandoned. More productive were searches on “stroke” AND “country or region” AND “services or policy” yielding 12 relevant articles; “spinal cord injury (SCI) AND “country or region” AND “services or policy” yielding 4 relevant articles; “traumatic brain injury (TBI) AND “country or region” AND “services or policy” yielding 8 relevant articles; and “health policy” AND “country or region” AND “rehabilitation” yielding 8 relevant articles. Country experts and reference lists from the retrieved articles led us to retrieve additional articles. We were especially fortunate to have available a recent report on neurorehabilitation policy in the European Union prepared for the Belgian government. 2 Wikipedia 3 provides useful quick overviews of health systems organization by country.
Results
Coverage for Neurorehabilitation
Table 1 presents the summary findings of the literature review. As is apparent, the detail in the published literature on neurorehabilitation services and coverage for most countries is very limited. A total of 35% of the burden of disease in Europe is due currently to disorders of the central nervous system. In terms of years of life lost and disability-adjusted life years lost, stroke, dementia, and injuries are in the top 10 disease categories. 42 Throughout the European Union, rehabilitation is considered part of the package of medically necessary services. However, admission criteria for inpatient rehabilitation vary widely across Europe. For example, availability of social networks, home support, premorbid disabilities, and cognitive function are important for determining admission to inpatient rehabilitation in Germany, Switzerland, and Belgium, whereas the United Kingdom does not consider level of function prior to the onset of illness or injury as a criterion for admission to inpatient rehabilitation. 43 Despite the official government positions on the value of rehabilitation services, physicians in these countries perceive that rehabilitation services can be difficult to obtain for their patients. In a recent survey, 57% of physicians in Italy, 53% in Norway, 23% in Switzerland, and 44% in the United Kingdom reported scarcity in rehabilitation services for stroke survivors. 44 Despite (or perhaps because of) this scarcity, innovative efforts to improve access are underway, as for example, the Adaptive Physical Activity (APA) program for chronic stroke in Tuscany, Italy. 16
Summary Findings of the Literature Review
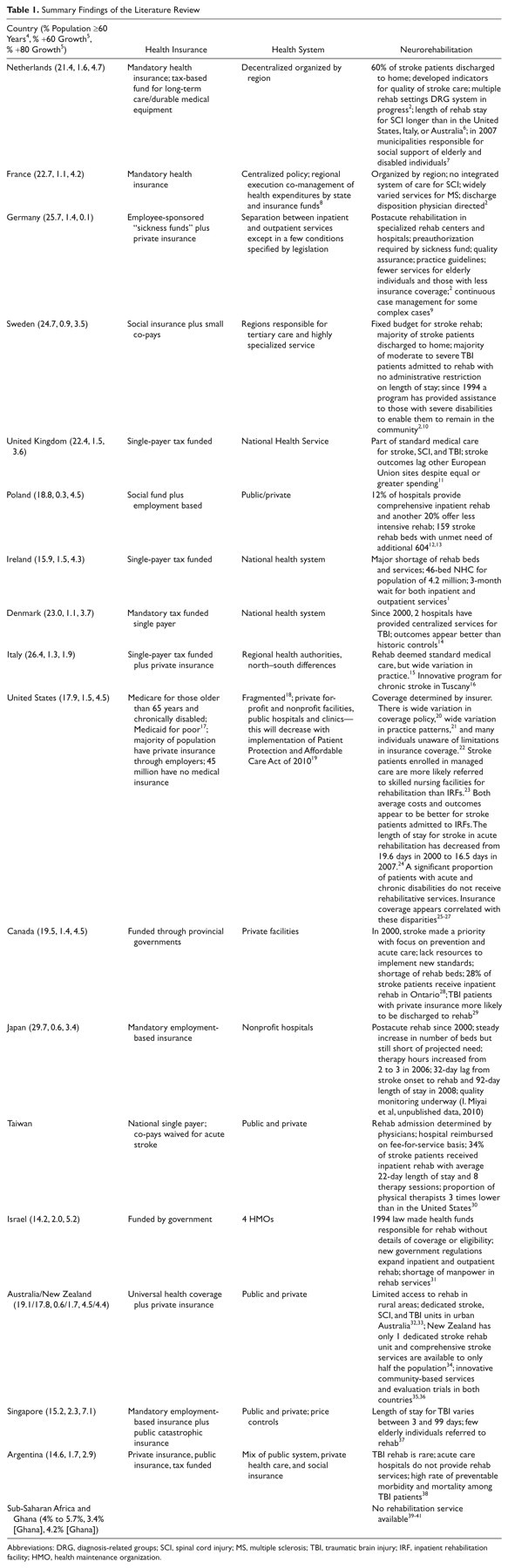
Abbreviations: DRG, diagnosis-related groups; SCI, spinal cord injury; MS, multiple sclerosis; TBI, traumatic brain injury; IRF, inpatient rehabilitation facility; HMO, health maintenance organization.
In the United States, access to neurorehabilitation services is influenced by insurance coverage as well as geographic variation in the availability of services. The recently enacted Patient Protection and Affordable Care Act of 2010 (ACA) is expected to reduce inequities associated with lack of insurance coverage. 19 Type of insurance also affects access—stroke patients enrolled in managed care are more likely to be referred to skilled nursing facilities than inpatient rehabilitation facilities (IRFs) for rehabilitation, although both average costs and outcomes appear to be better for stroke patients admitted to IRFs. 23
Outside of Europe and the United States, coverage for and access to neurorehabilitation is highly variable. For example, Australia provides well-developed systems in urban centers with more limited rural access. 32,33 Japan has provided coverage for postacute rehabilitation since 2000; efforts to expand access and quality of services are ongoing (I. Miyai et al, unpublished data, 2010). In sub-Saharan Africa and Ghana, no rehabilitation services are available. 39-41
General Observations
Two general observations regarding neurorehabilitation emerged in the cross-country comparisons. First, discontinuities in funding and responsibility lead to inefficiencies in care. Examples include Sweden, where acute care is funded by regions, and postacute care is funded by municipalities. This situation leads to conflicting incentives for transfer of patients to the most appropriate setting. In Germany, rigid separation between inpatient care and outpatient care has led to documented inefficiencies, 45 although changes enacted in 2007 have improved the situation for some specific diseases, for example, multiple sclerosis. Second, demography is straining budgets everywhere, leading to cost control as a major priority. Government documents across the globe emphasize cost containment, 8,46 an increased emphasis on competition as a cost control mechanism, and a desire to build “an evidence-based approach.” 2 To help place the issues around population growth and cost containment in context, Table 1 provides 2009 data 4 on the proportion of individuals in each country 60 years or older as well as the annual growth rates projected for the period 2025-2030 for the proportion of the population 60 years and older, and for the proportion 80 years and older. Even countries with already large proportions of their populations older than 60 years, such as France and Japan, are facing very large increases in their population older than 80 years. This trend is even greater in the less developed nations, for example, Singapore. 5
Neurorehabilitation faces a number of special challenges. It comprises only a small proportion of medical costs and the number of patients served is small as compared with the general population. Denial may result in some underestimation by the public of their risks of stroke and other disabling conditions, 47 although risk factor education can potentially correct these misperceptions. 48 Interestingly, a recent study demonstrates that the price elasticity for rehabilitation is approximately equal to that of acute care, suggesting that the patients value rehabilitation as much as acute interventions. 49 Many of the patients with significant neurological disabilities have other comorbidities. Stroke patients, for example, are at high risk for other cardiovascular events, and they also have an increased prevalence of hypertension, diabetes, metabolic syndrome, and deconditioning. 50 Effective care of the whole patient, including these comorbidities, is made that much more complex. Medical care of patients with neurological disabilities also intersects with larger economic and social realities. Presence or absence of spousal support, accessible housing and transportation, and financial resources can be at least as important as neurological function in determining stroke survivors’ abilities to maintain living in their communities.
Recent Trends in Policy
The history of a country’s health policy decisions reflects a myriad of political, economic, and cultural influences. Decisions occur at a variety of levels, from the deliberations of parliaments and ministries, to rules established by insurers, to individual decisions made by providers and consumers. In recent years, scientific evidence appears to be playing an increasingly important role in shaping these decisions. For example, in the United Kingdom, the National Health Service’s allocation of resources is increasingly following recommendations of the National Institute for Health and Clinical Excellence (NICE). 51 Stroke rehabilitation guidelines are in progress, with a target delivery date in 2012 (acute stroke care and critical illness rehabilitation guidelines are already issued). 52 The NICE process includes meetings with stakeholders and public comment. The current financial benchmark for medical interventions is that the cost per quality-adjusted life year saved should not exceed £30 000. Similar efforts are in play across the European Union, including major efforts in quality management in Germany, Belgium, France, and the Netherlands. Variations in stroke mortality and disability across Europe are under study. 53 The Collaborative Evaluation of Rehabilitation in Stroke across Europe (CERISE), funded by the European Union, seeks to compare process, outcomes, and costs of stroke rehabilitation. 54 Comparative effectiveness research has been a new major priority for the Obama administration 55 and the Patient Protection and Affordable Care Act of 2010 contains several provisions that direct the Centers for Medicare and Medicaid Services to implement demonstration projects to improve postacute care services. 19
Limitations of the Data
There were several major limitations in collecting the data. Data on coverage policy and statistics regarding access to rehabilitation services were often minor parts of the articles reviewed, and statistics were often incomplete. Government policies enunciated in official documents did not always reflect services actually delivered. Attention to issues regarding policies and costs of acute care and pharmaceuticals usually dwarfed those regarding rehabilitation. For example, in the OECD 2003 report “A Disease-Based Comparison of Health Systems,” 56 a 363-page report, there is 1 chapter on stroke, focused entirely on 7-day and 30-day mortality, and no mention of rehabilitation in the entire report. We were not able to obtain statistics and detailed information on coverage of neurorehabilitation services in several countries with outstanding health systems, for example, Switzerland 57 and Austria.
Discussion and Conclusions
What research would be helpful in providing the evidence base needed to drive public policy toward greater provision of neurorehabilitation services? First, it would be helpful to have reliable, current tables of neurorehabilitation services covered and available across countries. As the scattershot data in this article illustrate, it is currently very difficult to assemble this information from the published literature and Internet searches. The WFNR could play a key role in creating and maintaining such a database. This resource could play a vital role in helping policy makers understand the importance of neurorehabilitation and options for implementation of services. The investment necessary would be modest if WFNR members and regional societies would gather the information relevant to their countries on an annual basis. Reliable, current information across countries on covered neurorehabilitation services would inform policy makers and public alike, and would provide a basis for discussions on accepted medical practice and equity. As the organization and delivery of care varies widely internationally, 58 we suggest that rather than focusing on site of service, for example, acute care, acute inpatient rehabilitation, and/or subacute care, that data collection be organized around diagnoses, time from onset, and services actually delivered.
Second, although neurorehabilitation comprises only a small proportion of medical costs, our patients are among the most costly when total annual per capital medical costs are measured. 59 Studies on the integration of rehabilitation services, new technologies, pharmaceuticals, community exercise programs, and chronic disease management for people with neurological impairments have the potential to demonstrate ways to improve outcomes while reducing costs. Recent estimates indicate that if current trends continue, the United States will be spending 38% of GDP on health care by 2075, 60 echoing the overarching concern with costs observed across countries in our literature review. These economic conditions, although cause for alarm, also provide a window of opportunity for the field. To take advantage of this window, we need to be informed about international variation in coverage and to develop research that is responsive to the real need for coverage policies that provide high-quality, cost-effective services for people with neurological impairments.
In this regard, there is no substitute for randomized clinical trials (RCTs) in evaluating the efficacy of new interventions. 61 RCTs must be properly designed, 62 and they are time-consuming and expensive to mount. Moreover, RCTs conducted in rigorous, academic settings on homogenous populations of carefully selected patients do not tell us how well these interventions will work when translated widely into the community setting. New technologies offer the potential for new measurement strategies in community settings. For example, remote motion sensing may provide the means for accurate measurements of patient activities in their communities, leading to a new level of ecological validity in rehabilitation trials 63 and may accelerate the development of large, “simple” trials to determine best practices in rehabilitation. 64
Finally, there also is a need for good observational, cohort studies to generate research hypotheses, and to observe effects in community settings. These methods have provided some evidence for the cost-efficiency of temporary home attendant care for elderly individuals recovering from acute medical episodes 65 and for longer stay rehabilitation programs for patients with traumatic brain injuries. 66 Our questions must be expanded to include not only “Does it work?” but also “How can we make it better, faster, cheaper?” For example, modern anesthesia practice has reduced the operative death rates from anesthetics by a factor of 10 over the past 3 decades. Much of this work was accomplished through quality improvement studies rather than RCTs. 67 An emerging area of opportunity for cohort studies in neurorehabilitation is the incorporation of functional outcome data into administrative databases. 68
Footnotes
Acknowledgements
We thank Drs Michael Barnes, Andrew Frank, Gert Kwakkel, David Johnson, Ben Marosszeky, Leonardi Matilde, Jozef Opara, Koen Putman, and Pam Enderby for feedback and suggestions.
The author(s) declared no conflicts of interest with respect to the authorship and/or publication of this article.
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: Dr Weinrich performed some of the research for this article in the performance of his official duties and received travel support from the WFNR to present this work.