
Abstract
Proprioception is a vital aspect of motor control and when degraded or lost can have a profound impact on function in diverse clinical populations. This systematic review aimed to identify clinically related tools to measure proprioceptive acuity, to classify the construct(s) underpinning the tools, and to report on the clinimetric properties of the tools. We searched key databases with the pertinent search terms, and from an initial list of 935 articles, we identified 57 of relevance. These articles described 32 different tools or methods to quantify proprioception. There was wide variation in methods, the joints able to be tested, and the populations sampled. The predominant construct was active or passive joint position detection, followed by passive motion detection and motion direction discrimination. The clinimetric properties were mostly poorly evaluated or reported. The Rivermead Assessment of Somatosensory Perception was generally considered to be a valid and reliable tool but with low precision; other tools with higher precision are potentially not clinically feasible. Clinicians and clinical researchers can use the summary tables to make more informed decisions about which tool to use to match their predominant requirements. Further discussion and research is needed to produce measures of proprioception that have improved validity and utility.
Introduction
What Is Proprioception: Ambiguity Leading to Confusion
In the early 1830s, Sir Charles Bell described the sixth sense, referring to the sense of position and action of the limbs. 1 Proprioception was further discussed by Sherrington in his seminal text and lecture series some 70 years later. 2 Since then the term has been used to describe a variety of senses and therefore has become somewhat ambiguous. The word proprioception comes from the Latin proprius, meaning “one’s own,” combined with the concept of perception: thus a literal translation is that of “perceiving one’s own self.” This notion of self-perception reflects one’s ability to have both a sense of body orientation and position as well as a sense of body and limb motion. Accordingly, words often used interchangeably with proprioception are (joint) position sense, kinesthesia, movement sense, body position in space, sense of effort, or sense of force. The confusing and inconsistent application of these terms, particularly in the clinical domain, reflects the slowly emerging understanding of the nature of how we sense ourselves.
Berthoz 3 classically defines kinesthesia as the sense of movement, of which proprioception (sense of position and of velocity) is a part, along with cutaneous receptors, and the vestibular and visual systems. Conversely, other authors cite proprioception as having 3 submodalities: kinesthesia, joint position sense, and sensation of force (see, eg, Niessen et al 4 ). Others again add body segment static position, displacement, velocity, acceleration, and muscular sense of force, effort, or heaviness (see Ogard 5 or Proske and Gandevia 6 ) to the list of proprioceptive constructs. In this review, we will refer to proprioception as a collective term for these “subsenses,” unless the evidence only pertains to one in which case we will refer to that subsense individually.
Finally, proprioception can be considered one of the subsystems within the somatosensory system (along with pain, touch, and thermal sensation) and has also been considered interoceptive in that the sensory information is derived from changes within internal structures. This classification is in distinction to exteroception where the stimulus originates from outside the body such as external heat for thermoreception or light stimuli for vision.
Proprioceptive Receptors
Proprioception, or proprioceptive acuity, is a complex system that involves both peripheral and central systems. The evidence for the prime proprioceptive receptor favors muscle afferent input, 6 in particular muscle spindles. These receptors are specialized fibers within the muscle that detect change in muscle length and also the velocity of contraction 7 (or body part motion as the first derivative of length, ie, the rate of the change in length). If a passive lengthening is applied to a muscle, spindle exafferent signals are produced and interpreted as a sensation of movement, with increasing velocities causing an increasing response. 6 The spindle system has the capacity to anticipate length change because it can detect velocity as well as length (which changes more quickly). 3 Furthermore, motion direction can be perceived relative to which particular muscle has shortening or lengthening activity, and presumably by comparison between agonist and antagonist activity ratios, joint position can be perceived. The muscle spindle is also under fusimotor control (the gamma system), during contractions, which has the capacity to alter the calibration or sensitivity of the receptor by altering its internal length. 8 This modulation allows adaptation of the receptors during action and also allows simulation in the absence of real action. 3 Related to the sensitivity of the spindle is the role of thixotrophy—the phenomenon that demonstrates a relationship between a muscle’s properties and its immediate history of contracting/lengthening. It is a property of muscle (and muscle spindles) and influences proprioception—that is to say proprioception (spindle sensitivity) can be altered, dependent on whether the muscle has recently contracted or not (see Proske and Gandevia 6 )
Proske and Gandevia 6 summarize the evidence that receptors in the skin (cutaneous receptors) also contribute to joint position and motion sense, for example, as skin strain, particularly at the digits, elbow, and knee. Receptors analogous to the cutaneous receptors also exist in joint structures. For example, the more superficial Ruffini endings in the joint capsule, ligaments, and menisci are slow adapting mechanoreceptors. This allows detection of static joint position, intra-articular pressure, and possibly joint motion in terms of amplitude and velocity. 8 Pacinian corpuscles are deeper in these joint connective tissues with a lower mechanical threshold and are faster adapting—allowing them to be more responsive to changes in velocity, that is, acceleration and deceleration. Lephart and Fu 8 also describe free nerve endings widely distributed in articular structures and which may play a role in detecting severe mechanical deformation or inflammatory changes. However, it is now accepted that these mostly mechanical receptors predominate at extreme angles of joint position and motion and are relatively silent midrange.6,9 Golgi tendon organ-like receptors are also found in cruciate and collateral ligaments and menisci; like the mechanoreceptors listed, it is reported that they are useful at extremes of range as limit detectors. 8 This then leaves the muscle spindles to provide most information in the middle region of joint action. 6
Effort-based signals, that is, the efferent commands to muscles, have a role in proprioception (particularly sense of force and/or position sense). These signals are distinct from the traditional kinesthetic senses in that they are based on motor commands and therefore not experienced in a passive limb. However, Gandevia et al 10 investigated paralyzed and anesthetized upper limbs to demonstrate an alteration in position sense at the wrist joint, relative to the effort of attempting to produce a contraction in the paralyzed muscle(s), concluding there is a definitive role for “outflow” (efferent) signals in proprioception.
In summary, proprioception is based on an ensemble of sensory inputs that serve sensing, producing, predicting, and simulating joint position, joint motion (velocity and direction), and force specification. 3 There is considerable specificity and sensitivity in this ensemble arrangement as well as redundancy, particularly when proprioception is converged with the visual and vestibular systems in detecting motion and spatial orientation (from visual- and gravity-referenced coordinates).3,11 The most basic of postural control tasks, such as standing in regular environments, 12 is contingent on the coordination of these processes.
Clinical Implications of Proprioception
In motor control, proprioception, along with the other senses, is important in both feedback and feedforward operations and can be used in combination or in the absence of other sensory systems. Proprioceptors have a role in motor planning (feedforward for anticipation, preparation, and response planning) as well as rapid wiring into adaptation mechanisms to effect performance changes during task execution (feedback). Clinical scenarios where proprioception is lost or degraded classically result in loss of movement control where the person must then rely on visual input for feedforward and feedback processes. This may result in difficulty in learning novel movement, and also difficulty in improving the quality of movement or maintaining quality over a series of repetitions because of the absence of feedback for adaptation and skill refinement. 12 Not only are dexterous tasks affected but also balance and locomotion despite the high degree of redundancy with vision and vestibular input for these activities. Age has an impact on proprioception 13 ; proprioception lags somewhat behind vision in an infant’s development and then declines with age, particularly beyond 50 years.
Clinically, reduced proprioception has been most obviously implicated in stroke, 14 age-related falls, 13 and peripheral neuropathy 15 and also in movement disorders such as Parkinson’s disease, Huntington’s disease, and focal dystonia. 16 There has also been a lot of interest in the role of suboptimal proprioception in the etiology and/or rehabilitation of orthopaedic 17 and sporting injuries. 18 Poor proprioception has been reported in pain states such as chronic low back 19 and in persistent whiplash and associated disorders, 20 and in other diverse conditions such as developmental coordination disorder, 21 hypermobility syndrome 22 and Asperger syndrome. 23
Measuring Proprioception
There is clearly no single measure of proprioception due to the complexity of the neurophysiological processes that encompass proprioception described above.
In order to investigate the impact of a loss of proprioception on function, or the degree of loss from pathology, clinicians and researchers have developed many ways to capture proprioceptive acuity. More recently this has been driven by inquiry into the capacity of the proprioceptive senses to be improved through sensory-specific training or upregulation via afferent stimulation. 24
Tests have differentiated between the 2 main proprioceptive functions—detection of static position and detection of motion. The latter is further broken down into the threshold of motion detection, that is, the threshold amount/speed of motion required for detection to occur, and second, the direction of motion (eg, flexion or extension), which is considered a discrimination task. These 2 tests are usually performed passively and clinically and are administered to the great toe in a nonstandardized fashion. Detection of position has been performed by position copying or position matching tasks that can be done actively or passively. In order to further refine testing, attempts are often also made to reduce cutaneous stimulation during motion or position detection. However, given the multiplicity of constructs attributed to proprioception and the array of physiological processes, such tests often raise more queries than answers.
We embarked on this review systematically as the first stage in clarifying the ambiguities discussed above. We chose a systematic approach to cover the greatest breadth and depth of the literature. As such the aims of this systematic review were to
Identify the reported methods of assessing proprioception in healthy and pathological populations Classify the subsenses of proprioception they purport to measure (external validity) Report the clinimetric properties investigated for each tool (internal validity)
The overall objective was to provide clinicians and clinical researchers with a summary document of tools to enhance selection relative to need, with an explanation of the limitations or issues in the identified current approaches.
Methods
To identify proprioception assessment tools, a systematic search of the literature was conducted. The search strategy involved 2 steps. First, a comprehensive electronic database search was conducted. Then a secondary search was conducted looking at the reference lists from articles that were reviewed in full-text from the database search.
The databases searched included EBSCO, Journals@OVID, AMED, EMBASE, Medline, Ovid Medline, Science Direct, SportDiscus, E-journal, Ageline, CINAHL, and Highwire Press. Dates were from database inception and the searches were completed in December 2013. Search terms used included combinations of proprioception, kinesthesia or joint position, joint motion, with terms such as tests, clinical measures, clinical examinations, diagnostic accuracy, predictive value, sensitivity or specificity.
Articles identified in the database search were then evaluated by a team of researchers to ensure the research article and tools of proprioception assessment met the following inclusion criteria:
Explicitly described and employed a tool or tools to measure proprioception (or allied terms) In any human population Written in English
Two researchers (SH and a research assistant) agreed on eligibility for inclusion. There was no attempt to critically appraise the quality of the individual articles as they were of various study designs not necessarily related to the use of the tool itself. For example, the primary article may have been a randomized controlled trial using the tool as an outcome measure or it may have been a single case study using the same measure. We determined the level of study design itself did not offer any indication of the robustness or utility of the tool itself and therefore was not relevant.
The articles were then collated into similar tools with similar targeted subsenses (relative to aim 2) and data extracted to describe the joints measured, the construct, and the broad method of testing. Further data regarding population tested, equipment, and procedures were also extracted. The subsense or construct clusters were identified as
Joint position detection—active/instantaneous position or passive (AJPD or PJPD) (acknowledging the position is enacted AT the joint, not necessarily detected BY the joint) Passive motion detection threshold (PMDT) Passive motion direction discrimination (PMDD)
To fulfil aim 3, further data were extracted from the articles retrieved (and from the reference lists) to record relevant clinimetric properties, based on the process used by Slater et al.
25
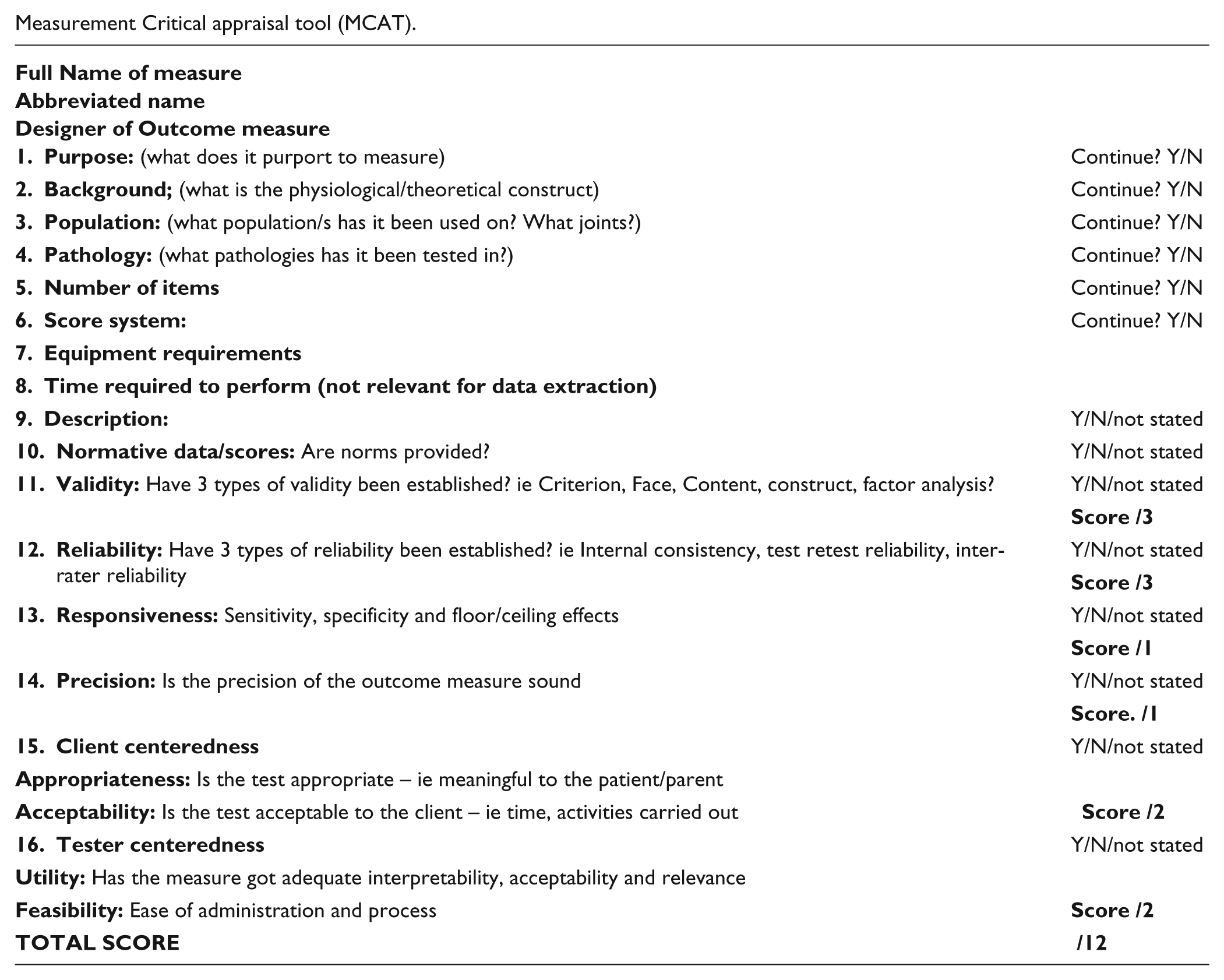
See Appendix 1 for an example of the data extraction pro forma. The properties scrutinized were the following:
Reliability: test–retest, reproducibility, intra- and interrater and internal consistency Validity: face, criterion, content, construct, concurrent, or factor analysis Responsiveness: sensitivity, specificity, floor and ceiling effects, discrimination Precision: accuracy, standard error
To further inform potential readers of the clinical features of the tool (also aim 3), we also considered subjectively
Client-centered attributes: appropriate, meaningful, acceptable Tester-centered attributes: feasibility and clinical utility—ease of use, clinically meaningful, ease of interpretation, normative scores
Two researchers completed this data extraction phase and crosschecks occurred on a random audit basis.
Results
We will first report the results of the search and then results relative to the 3 aims of the study.
Step 1, which involved the database search, ultimately yielded 40 articles from the initial database search list of 935, with the full process of inclusions and exclusions detailed in Figure 1. Step 2, which involved pearling the reference lists of the articles retrieved for full-text review, revealed a further 17 articles to be retained for final inclusion, giving a total of 57 articles.
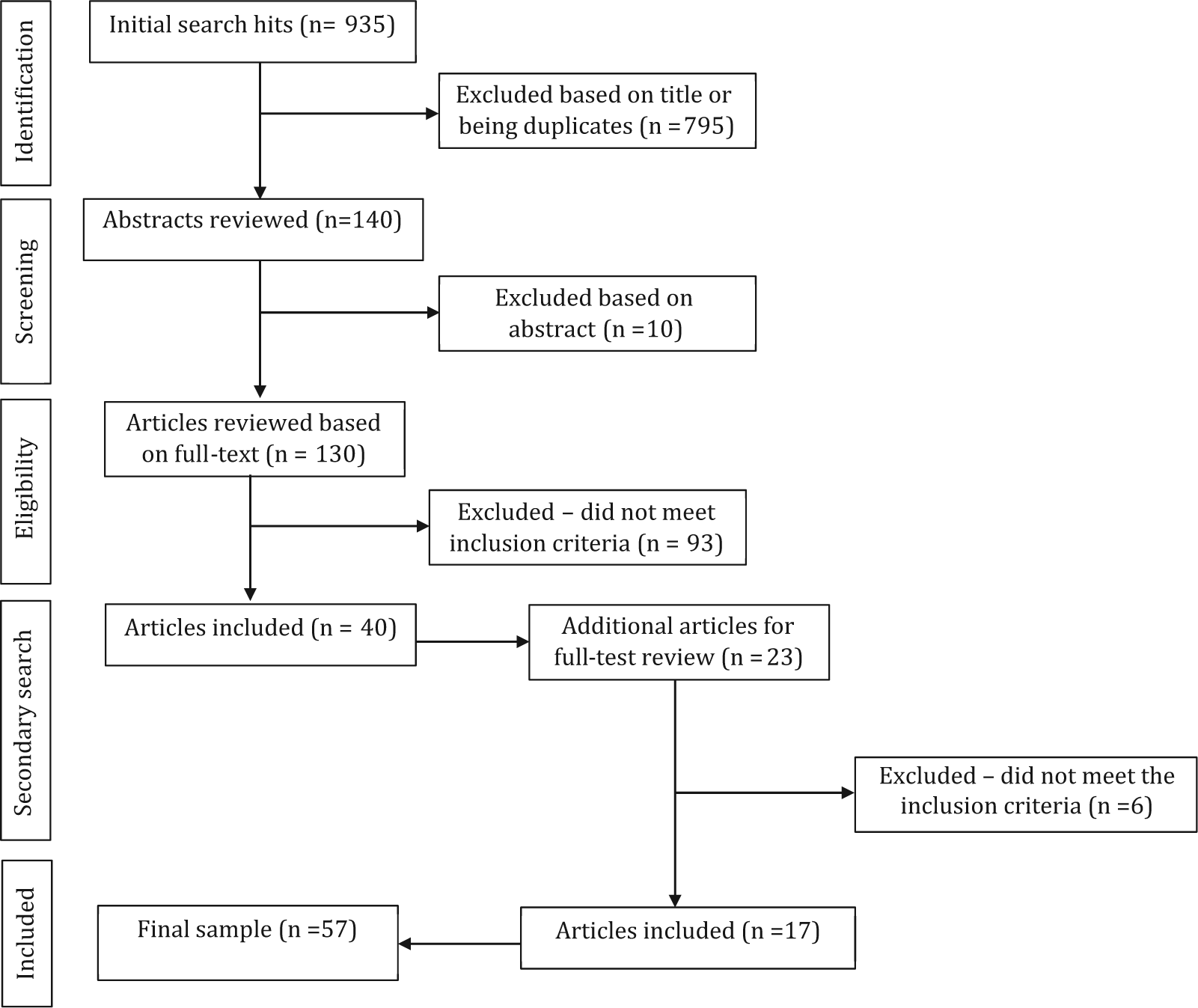
PRSIMA flow chart of article selection.
Identification of Tests
Table 1 summarizes the 57 research articles included in this review. From these 32 tests of proprioception were identified (that appeared to be sufficiently distinct in relation to purported constructs, administration, and/or joints) and data extracted as detailed in the methods.
Summary of Identified Proprioception Tests.

Abbreviations: AJPD, active joint position detection; PJPD, passive joint position detection; PMDT, passive motion detection threshold; PMDD, passive motion direction discrimination; L or Lx, lumbar; WB, weight bearing; Cx, cervical; GH, gleno-humeral; flex, flexion; ext, extension; ACL, anterior cruciate ligament; OA, osteoarthritis; WADS, whiplash and associated disorders; NWB, non–weight bearing; MS, multiple sclerosis; MCP, metacarpophalangeal joint.
The body part most commonly measured was the knee (11) followed by 4 tests identified for the lower trunk or back, 4 for the ankle, and 2 distinct protocols for the cervical spine. Other areas were often tested as a composite (eg, hip and knee and ankle in weight-bearing), or targeted distal joints of upper and lower limbs (eg, toes and fingers/thumb).
The tests were used on widely varied populations. The majority were with healthy adults or used healthy adults as a control. Three looked at populations of athletes (gymnasts and tennis and basketball players), a specific profession (firefighters with and without lower back injuries), or the influence of age (children, adults, and elderly). The majority of pathological populations had musculoskeletal issues such as anterior cruciate ligament deficiency (ACL; 4), osteoarthritis (5), or pain (4). Postsurgical comparisons were also featured, for example, pre- and post-ACL reconstruction (3), shoulder arthroplasty, or knee replacement. Neurological pathologies were less well featured with 4 tests described in stroke and 1 each for Parkinson’s disease, traumatic brain injury, cerebral palsy, peripheral neuropathy, and anesthetized limbs.
Proprioceptive Subsenses Tested
Table 2 summarizes the tests in relation to what they test (the subsenses or constructs). The majority of tests assessed joint position detection either actively or passively (AJPD or PJPD) through recognition or reproduction tasks with the measurement being joint angle error (JAE; ie, the difference between the true target angle and the reproduced angle or angle at which recognition occurred). There was variation in how the target angles were demonstrated (on the limb itself, or the contralateral limb, using an angled lever) and whether the JAE was measured via motion capture equipment, electro-inclinometry, photographic capture, Perspex protractor grading, or goniometry (electric or manual). Various means were used to produce the passive motion for PJPD from motorized apparatus or robotics, to modified splints moved by the tester to simply the tester moving the body part. Where the task was active reproduction of the target angle, it was mostly reproduced on the ipsilateral side, but in the more manual-based tests it was reproduced on the contralateral side or on a sheet of paper, a goniometer, or a simulated limb.
Proprioceptive Tools Clustered Within 4 Identified Subsenses.
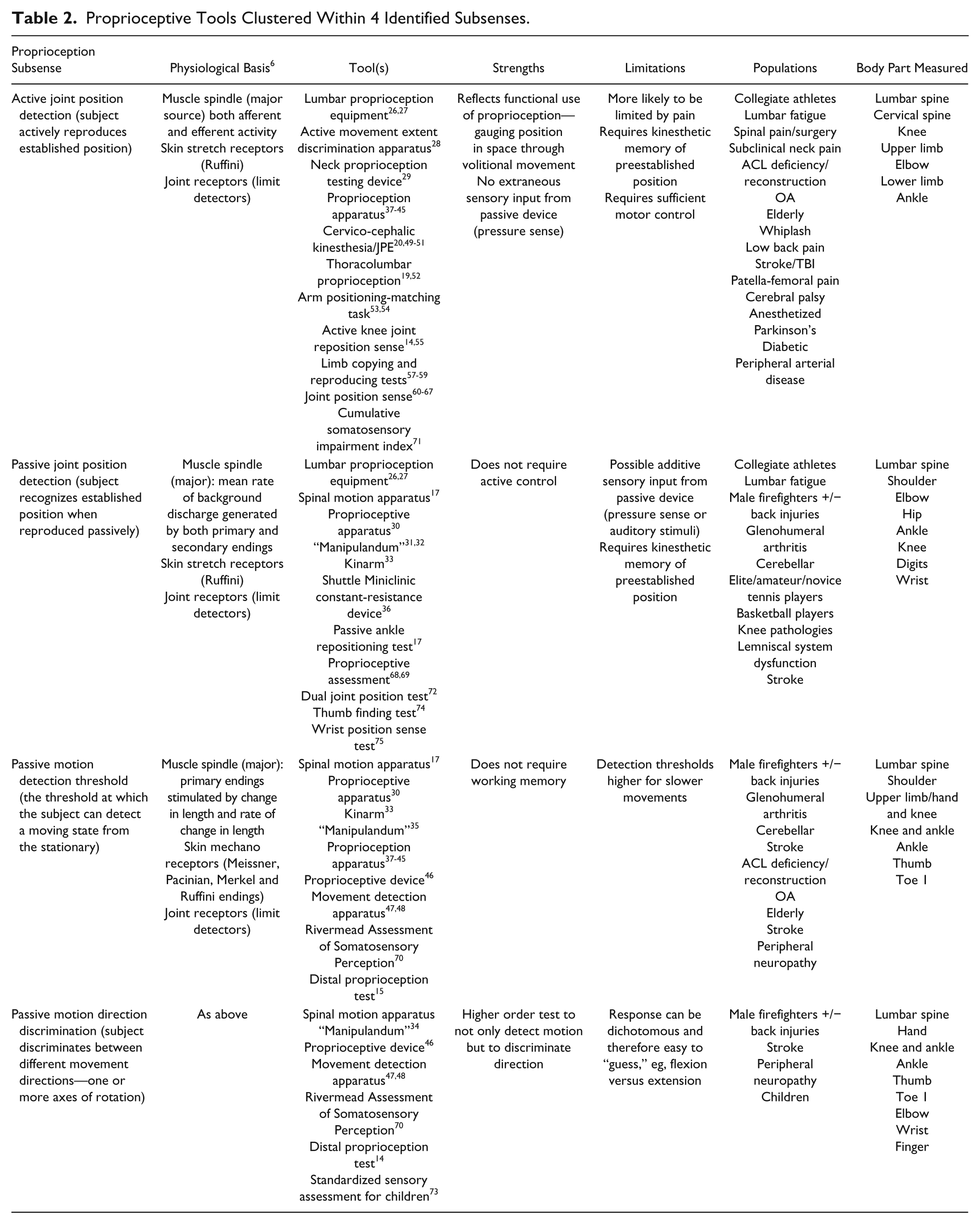
Ten tests15,17,30,33,35,37,45-48,70 measured the threshold for detecting motion (PJMD) again using a variety of ways to produce the passive motion as described above. The most common measure was the error between the angle of actual commencement of motion and the detection angle. However, the more simple clinical tests simply required the person to detect motion compared to static position and were scored dichotomously for 5 to 10 trials.
Six tests15,34,46,48,70,73 also incorporated the direction of motion discrimination task (PMDD) by requiring the person to indicate whether the limb moved in a positive or negative direction relative to the defined plane of motion. Generally, the planes of motion were restricted to one but a few tests did incorporate up to 3 planes and one used “pathways,” that is, tilting or curved.
In all examples found, some attempt was made to reduce the influence of confounding senses though the degree to which this was attempted also varied, for example, all tests excluded vision while the most elaborate tests produced passive motion with pneumatic splints so that there was no discernment of pressure to imply motion or motion direction (via cutaneous receptors) or even used background white noise to cancel out any clues to motion commencement from the sound of the motor (see Table 2 for limitations).
Clinimetric Properties
Generally, the clinimetric properties for the identified tools were poorly evaluated or reported. Table 3 summarizes each test and the reported properties we were able to find, as well as our judgments on the user- and client-centered aspects. Six tests29,30,31,32,34,46,74,75 had no recorded properties tested. For the others, the main data available related to the discriminant ability of the test, that is, to differentiate between 2 groups (one normal and one pathological for example). The Rivermead Assessment of Somatosensory Perception (RASP) 70 had the most reported properties and achieved “good” or higher in the evaluations. Furthermore, this test can be applied with no equipment to 5 different joints for greater clinical utility; however, it was not considered precise in that the scoring for each test move is only dichotomous and there is the confounder of the tester manually moving the body part with cutaneous input. The Modified Thomas splint with Pearson knee flexion piece68,69 has been used and tested more widely with high values for test–retest and concurrent validity and ability to discriminate between different pathological groups and age ranges. The equipment requirements are not onerous but this device only assesses the knee.
Clinimetrics of Proprioception Tests From Published Literature.

Abbreviations: AJPD, active joint position detection; PJPD, passive joint position detection; PMDT, passive motion detection threshold; PMDD, passive motion direction discrimination; ICC, intraclass correlation; CI, confidence intervals; ACL, anterior cruciate ligament; OA, osteoarthritis; PF, plantar flexion; WADS, whiplash and associated disorders; LBP, low back pain; ADL, activities of daily living; Dom, dominant; Ndom, nondominant; SEM, standard error of measurement; ant, anterior; KR, knee replacement; PCL, posterior cruciate ligament; JPA, joint position awareness; MS, multiple sclerosis; TD, typically developing; WB, weight bearing; NWB, non–weight bearing.
Discussion
We have conducted a thorough search of the literature to identify the most commonly used tools for the measurement of proprioception in humans. Not surprisingly, we found a plethora of different tools, and the variations came with respect to
Measuring different proprioceptive subsenses (active versus passive position, motion detection, or direction discrimination) Measuring different joints The use of different types of equipment and values Differing populations.
Given the complexity of proprioception and the multifacetted aspects of kinesthesia and position sense as identified in the introduction, it is not surprising that the tests are so seemingly disparate. By highlighting this issue we hope that future clinicians and researchers are aware of the variations in terminology and practice and that some consensus can be reached about the definition and assessment of proprioception.
It is interesting to contemplate the influence of current understandings in the physiology of proprioception on the testing of position and motion. We did not find strong indications that there was any clear incorporation or acknowledgement of the primary role of muscle spindle activity, nor was the influence of thixotrophy consistently acknowledged (controlling for muscle activity prior to testing). There was little acknowledgement of the differentiation of individual proprioceptive senses, with most tests not controlling for efferent influences (via electromyography for example). Therefore, both the muscle afferents and efferents may contribute to proprioception in the so-called passive tests. Well-described examples of test procedures exist in the experimental literature that do control for these factors (ie, thixotrophy, muscle effort, force feedback; see Gandevia et al 10 ), and we encourage clinicians to familiarize themselves with these procedures. Most tests were conducted in mid-ranges and therefore not engaging the joint receptors as limit detectors, highlighting the emphasis of tests for muscle spindle afferent activity.
In considering the active tests there are also questions to be considered. Bevan et al 31 reported that the joint angle may be less accurate than the angular distance travelled by the limb, especially given the latter has more functional meaning. Gandevia and Burke 9 originally suggested that repositioning or relocating after active positions or motions may rely on central motor programs rather than a memory of proprioceptive coordinates. Some tests (eg, Kristjansson et al 49 ) attempted to overcome this by increasing the complexity of the active motion; however, this was for head motion and they clearly could not control for vestibular input into the relocation/repositioning response so the specificity of the test for neck proprioceptors is not clear.
Tests for the sense of force or effort are still not routinely conducted in clinical settings; therefore, they were not available to be included in the review. We are aware of clinical researchers using various means to evaluate the sense of heaviness (see Konczak et al 78 ) but there seems to be no consistent uptake of these constructs in rehabilitation settings as yet. Clear dialogue between researchers and clinicians is required to further robust investigations into the clinical import of these constructs in rehabilitation and recovery.
Some authors did attempt to reproduce more applied tests such as weight-bearing or through more functional arcs of motion rather than anatomical single planes of action. We were unable to determine if these are any more accurate or valid beyond an element of face validity in terms of relevance to daily life. Further to this it has been questioned how functional these point-in-time measures are. First, they do not take into account the role of fatigue on proprioception. Fatigue has been reported to influence proprioception whereby exercise-induced fatigue can produce inaccuracies of proprioception, 6 such as errors in matching torque, 79 movement, or position.80,81 Furthermore, clinical fatigue (from conditions such as chronic fatigue syndrome) may be associated with kinesiophobia and other sensor-motor impairment. Second, the tests only test conscious proprioception, whereas it is clear that mostly we are reliant on subconscious proprioception in daily activities. Further issues include potential learning effects and the role of attention levels. Some measures did attempt to control for confounding alternate sensory inputs but others did not.
Some of the tests predate current proprioceptive understanding—it may be considered a limitation of this review that we did not exclude tests devised before the 1970s. However, we could not be confident that tests produced in more recent times in fact do take into account current theories; therefore, we have included all tests found and leave it to the readers to evaluate for themselves the relative validity of the tests.
We summarized the reported clinimetric properties for each identified test and found that very few had a full suite of properties evaluated and/or reported. Therefore, there is a question mark over many in terms of robustness, believability, and utility in the clinical setting. There is a clear trade-off between more research-oriented measures and those used clinically. The former measures should be more precise, accurate, and valid (particularly in terms of controlling for input other than proprioceptive); however, these techniques may be beyond the scope of a general clinical environment. In contrast, the clinically friendly tests are arguably more for “screening” given their lack of precision. We advise readers to carefully consider the constructs they wish to test, the individual joints, and with what precision. For example, if high precision is needed to evaluate the impact of interventions for lowered proprioception, then the expense of the more research-oriented tools may be warranted. Certainly it has been our experience that an easy to conduct, clinically based tool such as the distal proprioception test is not useful in clinical trials (see Lynch et al 82 ). However, if the use is for a clinical screen to simply identify that there is a proprioceptive impairment that may be affecting function in the clinical setting, then the RASP 70 certainly seems to offer a useful means to standardize the conduct and reporting of such an impairment. Subsequently, it is then up to the clinician to establish an association between the sensory impairment and the loss of function. Some tests have established an overall concurrent validity with aspects of functional performance, for example, the cervico-cephalic kinasthesia tests correlate with reduced balance and smooth pursuit in people with whiplash 20 ; the knee test using a modified Thomas splint correlated with function and with patient satisfaction 69 ; and proprioceptive tests within the RASP correlated with scores for motricity and activities of daily livings. 70
We recommend collaborations between neurophysiologists, conducting precise proprioceptive testing, and clinicians, interested in understanding the influence of impaired proprioception. This would further a more universal appreciation of the interdependent nature of the various facets of proprioception and motor function, clarify confusion around terminology, and serve to identify and standardize tests that have validity and utility for clinical populations in their rehabilitation. Facets of proprioception missing from clinical practice such as measures of sense of force, effort, motion speed, and so forth, are areas we wish to particularly highlight for further collaboration.
Conclusion
In summary, the information provided by this review should be directly useful to clinicians and researchers alike to compare and contrast their testing needs and therefore select the most appropriate tool for the job at hand. We have identified that whatever the need, proprioceptive tools are generally poorly evaluated in clinical settings and further research is required to establish reliability and validity as a starting point in the existing tests. Current understandings of proprioception from the research literature need to be applied in clinical practice to further implement evidence-based assessment and therefore rehabilitation.
Footnotes
Appendix 1
Measurement Critical appraisal tool (MCAT).
|
|
|
|
|
|
|
|
|
| Continue? Y/N | |
| Continue? Y/N | |
| Continue? Y/N | |
| Continue? Y/N | |
|
|
Continue? Y/N |
|
|
Continue? Y/N |
|
|
|
|
|
|
|
|
Y/N/not stated |
| Y/N/not stated | |
| Y/N/not stated | |
|
|
|
| Y/N/not stated | |
|
|
|
| Y/N/not stated | |
|
|
|
| Y/N/not stated | |
|
|
|
|
|
Y/N/not stated |
|
|
|
|
|
Y/N/not stated |
|
|
|
|
|
|
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: Financial assistance was provided by the Director, International Centre for Allied Health Evidence. Research assistance was provided by Valentin Dones and Anthea Worley.