
Abstract
Background. Functional electrical stimulation therapy (FET) has a potential to improve voluntary grasping among individuals with tetraplegia secondary to traumatic spinal cord injury (SCI). Objective. This single-site, randomized controlled trial examined the efficacy of 40 hours of FET with conventional occupational therapy (COT) compared with COT alone to improve grasping. Methods. Twenty-four subjects with subacute traumatic incomplete SCI (C4-C7, AIS B-D) consented to participate in 40 hours of therapy over 8 weeks, beyond the conventional rehabilitation program. Subjects were randomized to receive FET + COT (n = 9) or COT (n = 12). The key outcomes were changes in Functional Independence Measure (FIM) self-care subscores, Spinal Cord Independence Measure (SCIM) self-care subscores, and Toronto Rehabilitation Institute Hand Function Test (TRI-HFT) performed at baseline and follow-up. Results. At the end of the treatments, the change in mean FIM self-care subscore for the FET + COT group was 20.1 versus 10 (P = .015) for the COT group. Subjects randomized to FET + COT also had greater improvements in the SCIM and TRI-HFT. No longer term follow-up was feasible. Conclusion. FET significantly reduced disability and improved voluntary grasping beyond the effects of considerable conventional upper extremity therapy in individuals with tetraplegia.
Keywords
Introduction
Among persons with cervical spinal cord injury (SCI), restoration of hand function is a key priority. 1 Various therapies, surgical interventions, and devices have been proposed to improve hand function in individuals with C4-C7 tetraplegia. Among these interventions, functional electrical stimulation (FES) devices have shown promising results. 2 Some FES systems for grasping, also known as neuroprostheses for grasping, have been successfully commercialized and are typically intended for routine daily use. 3,4 During a power grasp, the object is held in a clamp formed by partly flexed fingers and the palm; counterpressure is applied by the thumb lying more or less in the plane of the palm. 5 Precision grip of small objects is generated by flexing the fingers and opposing the thumb. 5
Anecdotal accounts over the past 30 years have reported that individuals with C4-C7 tetraplegia who frequently use their FES systems for grasping may have experienced improved carryover in function that persists even when the device is not in use. 6-10 Neurological mechanisms for the carryover effect were proposed by Rushton in 2003. 11 We published the results of a phase I randomized controlled trial that examined this carryover effect. 12 Although that study was not powered to determine treatment efficacy, its results suggested that short-term use of FES therapy (FET) for grasping has the potential to improve hand function in individuals with both complete and incomplete subacute C4-C7 SCI.
The objective of this study was to determine if FET is an effective means of improving voluntary hand function in adults with incomplete subacute (<6 months postinjury) tetraplegia (C4-C7, AIS B-D). We hypothesized that individuals with tetraplegia who undergo FET may have greater improvements in voluntary hand function, in particular grasping, when compared with individuals who receive a similar volume and duration of conventional occupational therapy (COT) during subacute rehabilitation.
Methods
Consenting adult subjects who met inclusion criteria were randomized to either the control group or the intervention group. They received either 1 hour of COT plus 1 hour of FET daily (intervention group) or 2 hours of COT (control group) on weekdays, for a total of 10 hours of therapy per week for 8 weeks. Outcome assessments were performed by staff blinded to the study intervention and group allocation. The study was approved by Toronto Rehabilitation Institute’s research ethics board and registered on www.clinicaltrials.gov (ClinicalTrials.gov ID NCT00221117). We certify that all criteria for the ethical conduct of clinical trials were met.
Subjects
Eligible subjects were identified through staff referrals, poster campaign, and local advertisements during their initial inpatient rehabilitation following traumatic SCI.
Inclusion criteria
(a) Individuals who had sustained a traumatic incomplete SCI between C4 and C7, AIS B, C, or D, less than 6 months prior to the baseline assessment; (b) individuals 18 years of age or older; and (c) individuals unable to grasp and manipulate various objects either unilaterally or bilaterally, to allow independent performance of activities of daily living (ie, eating, dressing, grooming).
Exclusion criteria
(a) Individuals who had contraindications for FES, such as a cardiac pacemaker, skin lesions, or a rash at a potential electrode site; (b) individuals who suffered from cardiovascular conditions such as uncontrolled hypertension or autonomic dysreflexia requiring medication; or (c) individuals with denervated muscles (ie, individuals who beside SCI also sustained partial or complete damage of the peripheral nerves that were innervating muscles of interest).
Study Protocol and Randomization
Subjects were randomized using 2 sets of sealed envelopes. Each unmarked envelope contained a single sheet of paper with a printed number in the range of 1 to 40. A second set of envelopes was marked with numbers from 1 to 40 and contained a single sheet specifying the group allocation. The randomization schedule was done using the randperm function in Matlab (The Mathworks Inc, Natick, Massachusetts) seeded with an arbitrary clock value. After the subject selected a random number from the set of unmarked envelopes, the corresponding marked envelope was opened, revealing the group allocation. The allocation sequence was generated by the principal investigator (MRP) as he was not involved in any subject assessments or treatment sessions. Subject screening and consent was carried out by the research coordinator who was not involved in providing the treatment, performing the outcome assessments, or performing the data analysis. The randomization allocation ratio was 1:1.
Interventions
Conventional occupational therapy
COT pertaining to hand function 12 represents the current best practice activities against which the FET was compared. The COT included the following: (a) muscle facilitation exercises emphasizing the neurodevelopmental treatment approach; (b) task-specific, repetitive functional training; (c) strengthening and motor control training using resistance to available arm motion to increase strength; (d) stretching exercises; (e) electrical stimulation applied primarily for muscle strengthening (this was neither FES nor FET, but electro muscular stimulation); (f) practice of activities of daily living (ADLs) including self-care where the upper extremities were used as appropriate; and (g) caregiver training.
FES therapy
The FET began by designing stimulation protocols to generate power (circular grip and lateral pinch) and precision (opposition with 2 and 3 fingers) grasps on demand. The stimulation sequence (protocol) for power and precision grasps was developed for each patient individually using the Compex Motion electric stimulator. Compex Motion is a fully programmable transcutaneous (surface) stimulator that uses self-adhesive surface electrodes. 13
The power grasp was used for grasping bigger and heavier objects such as water bottles and coffee mugs (see Figure 1). Lateral pinch was used for grasping smaller and thinner objects such as keys and paper. Precision grip was used for grasping smaller objects such as dice and popcorn. Power grasp was generated by partly flexing the fingers and the thumb in flexion and slight opposition. Lateral pinch was generated by fully flexing the fingers followed by the thumb flexion. Precision grip was generated by first forming opposition between the thumb and the palm, which was followed by index finger and thumb flexion. Muscles that were stimulated during therapy were the following: wrist flexors—flexor carpi radialis and flexor carpi ulnaris; wrist extensors—extensor carpi radialis longus and brevis, and extensor carpi ulnaris; finger flexors—flexor digitorum superficialis and flexor digitorum profundus; finger extensors—extensor digitorum; thumb abductors—median nerve or abductor pollicis brevis and abductor pollicis longus; thumb flexors—flexor pollicis brevis and flexor pollicis longus; and thumb oppositors—opponens pollicis. Of note, not all the aforementioned muscles were stimulated in every subject. The individuals with SCI often have some of the muscles partially or completely denervated, that is, they cannot be contracted using electrical stimulation. To overcome this problem the practitioners are encouraged to try stimulating different muscle group combinations (when this is possible) to generate the desired hand movement. Hence, all muscles listed above have been stimulated during the study, but not in a single subject. Each subject had customized stimulation protocol that was applied to some of the muscles listed above. Furthermore, stimulation of flexor pollicis longus muscle using surface stimulation technology is not a trivial exercise, as this muscle can be contracted using surface electrical stimulation only in 1 out of 4 individuals. During therapy, the command for activating the stimulation sequence was issued with a pushbutton. More detailed information regarding the Compex Motion stimulator and the hand stimulation protocols used may be found in the works by Popovic and colleagues. 13,14
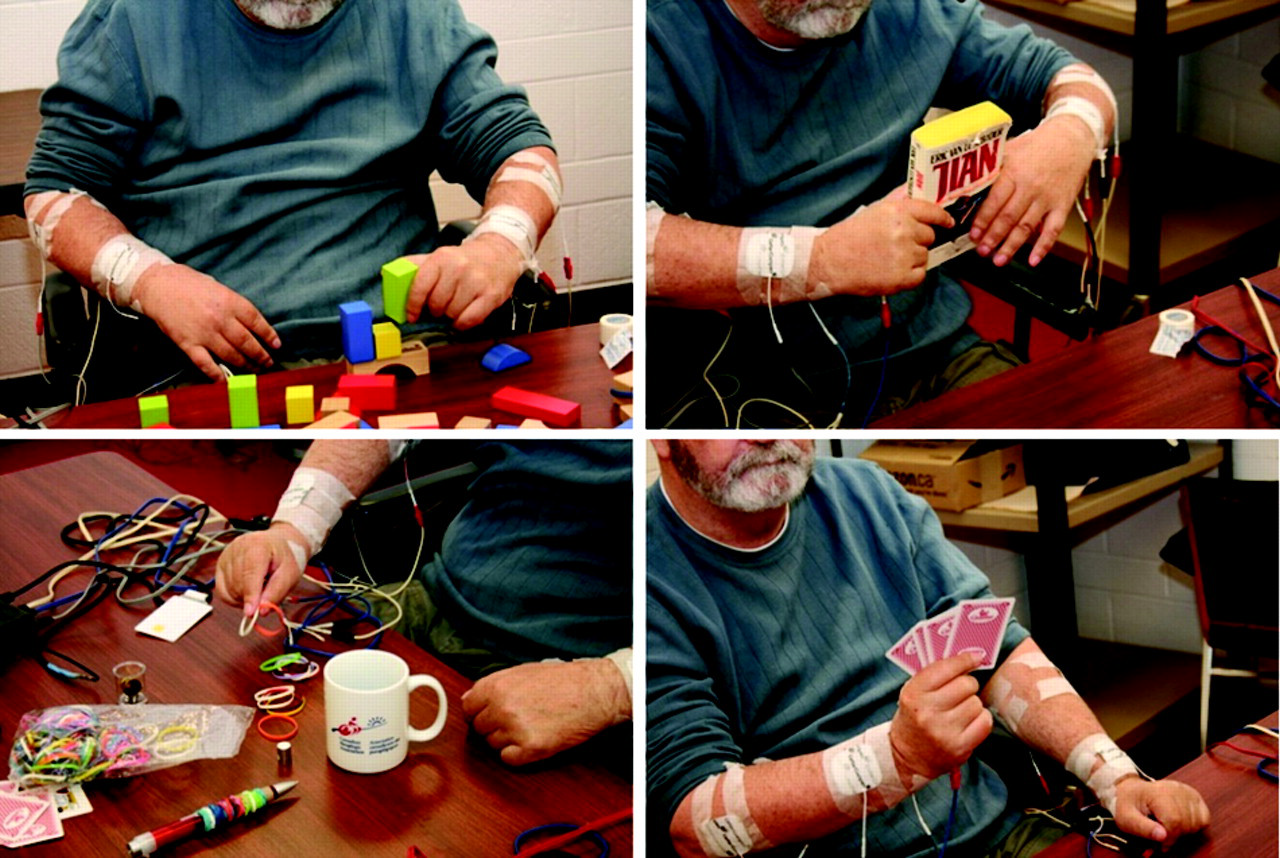
Examples of object manipulation during the functional electrical stimulation therapy.
The FET protocol used in this study allowed individuals who did not have any voluntary movement or contraction in the wrist and fingers to be included. This factor makes FET unique when compared with alternative therapy forms. In the early stages of FET all the movements were performed with the help of FES. Subjects were asked to imagine a particular movement and then try to execute it voluntarily. The occupational therapist would allow the subject to struggle while trying to perform the desired movement. Ten to 20 seconds after attempting a desired task, the therapist activated the FES sequence and helped the subject perform the desired movement. As soon as an individual showed signs of recovery of either voluntary extension or flexion in a stimulated muscle group, he/she was encouraged to make an effort to produce the movement voluntarily, which was previously facilitated by FES. As the subject demonstrated improved strength and range of motion, the FES for those muscle groups were phased out and refocused on other muscle groups that were still weak and needed to be “reactivated.” The order in which muscle groups were sequentially “reactivated” was subject dependent. In later phases of FET the use of FES was reduced considerably and was used only to help a subject carry out particular components of the movement that he/she was still unable to do.
In all cases FET was delivered while the individual was performing functional tasks, such as grasping a mug, writing his/her name, playing table tennis, and so on. Use of FET as part of a functional training was an essential component of this therapy. FET was not used for muscle strengthening; instead, it was used to retrain the neuromuscular system to execute tasks it was previously unable to carry out voluntarily. Movements were performed against gravity and sometimes against light manual resistance. The number of repetitions was determined based on subject’s strength and endurance. In general, the subject spent at least 45 minutes out of the 60 minutes of daily FET performing various tasks common in ADLs while being assisted by FES system for grasping. In the later stages of therapy the therapists allowed the subject to control the triggering of the stimulation sequences. The key element in this therapy, besides FES, is that the subject was fully engaged in the therapy process and that he/she paid attention to the tasks being performed. That is why the focus of our FET was execution of as many diverse functional tasks as possible during the therapy sessions.
The stimulation parameters used were the following: (a) balanced, biphasic, current regulated electrical pulses; (b) pulse amplitude from 8 to 50 mA (typical values 15-30 mA); (c) pulse width 250 µs; and (d) pulse frequency 40 Hz. During the intervention, the occupational therapist adjusted the placement of electrodes and guided the hand movements. The occupational therapist ensured that all movements were functional, efficient, and used normal movement patterns. An independent hand-strengthening and -stretching program was provided as needed to facilitate normal hand function.
Therapy Dose
All subjects received therapy daily, 5 days per week, for the duration of 8 weeks (total of 40 sessions). On “therapy days” all subjects received a total of 1 hour of COT between the right and left hands and 1 hour of either FET (intervention group) or additional 1 hour of COT (control group) between the right and left hands. The 2 hours of therapy were performed with at least a 2-hour break in between. Both groups received 1 dose of COT irrespective of their group allocation to ensure that they received the best practice upper limb therapy for tetraplegic patients available at the time of this study within the medical rehabilitation program at Toronto Rehab. Subjects in the control and intervention arms of the study received equal amount of therapy and attention.
Outcome Measures
Primary outcome measure
The Functional Independence Measure (FIM) 15 was employed to measure the degree of disability for daily self-care.
Secondary outcome measures
The Spinal Cord Independence Measure (SCIM) 16 is a disability scale that has been specifically developed to evaluate the degree of disability in patients with traumatic and nontraumatic SCI. The SCIM assesses function in 3 core areas: (a) self-care, which includes feeding, bathing, dressing, and grooming, and is scored in a range of 0 to 20; (b) respiration and sphincter management are scored in a range of 0 to 40; and (c) mobility, also scored in a range of 0 to 40.
The Toronto Rehabilitation Institute Hand Function Test (TRI-HFT) 17 evaluates gross motor function of unilateral grasp (also referred to as the Rehabilitation Engineering Laboratory Hand Function Test). Hand functions that are assessed with TRI-HFT include the following: lateral or pulp pinch and palmar grasp. The TRI-HFT consists of 3 components. The first evaluates the power grasp, the lateral pinch, and precision grip, whereas the second and third components evaluate the strength of both power and lateral grasps. The scoring system for TRI-HFT (scale 0-7) is as follows:
0 = No movement elicited, that is, subject unable to reach for the object
1 = Subject able to reach for the object but unable to grasp the object
2 = Subject able to reach and grasp (using passive grasp) but unable to lift the object successfully off the supporting surface
3 = Subject able to reach and grasp (using active grasp) but unable to lift the object successfully off the supporting surface
4 = Subject able to reach, grasp, and lift the object (using passive grasp) but unable to manipulate the object
5 = Subject able to reach, grasp, and lift the object (using active grasp) but unable to manipulate the object
6 = Subject able to reach, grasp, lift, and manipulate the object (using passive grasp) appropriately
7 = Subject able to reach, grasp, lift, and manipulate the object (using active grasp) appropriately
This scoring system was developed specifically for individuals with SCI in distinction to another system 12,17,18 for stroke.
Statistical Analysis
The subject’s impairment and demographic characteristics were analyzed using descriptive statistics for parametric and nonparametric data. The baseline outcome data of the intervention and control groups were compared using Fisher exact test (for categorical variables) and Mann–Whitney U test (for continuous variables). Comparisons between the intervention and control groups were carried out using linear regression analysis adjusted for the baseline degree of disability (baseline AIS). 19 In each analysis the posttreatment score (SCIM or FIM) was adjusted by its respective baseline (pretreatment SCIM or FIM, respectively). All data analyses were carried out using SAS program version 9.1 (SAS Institute Inc, Cary, North Carolina). Significance was determined at P < .05.
Results
Figure 2 shows the CONSORT diagram for screening and entries. One subject in the intervention group and 1 control dropped out. Data for 1 subject in the intervention group was corrupted before the analysis was preformed, which left 21 subjects (9 in the intervention group and 12 in the control group) with full baseline and therapy completion data. Demographics and neurological descriptors are shown in Table 1. Out of these 21 subjects who successfully completed the therapy and had complete data sets at baseline and therapy completion, only 5 were willing and able to participate in the 6-month follow-up assessment session (4 in the intervention group and 1 in the control group). Because of very poor response of the subjects in taking part in the 6-month follow-up assessment session, only data collected at baseline and therapy completion phases of the study were analyzed.
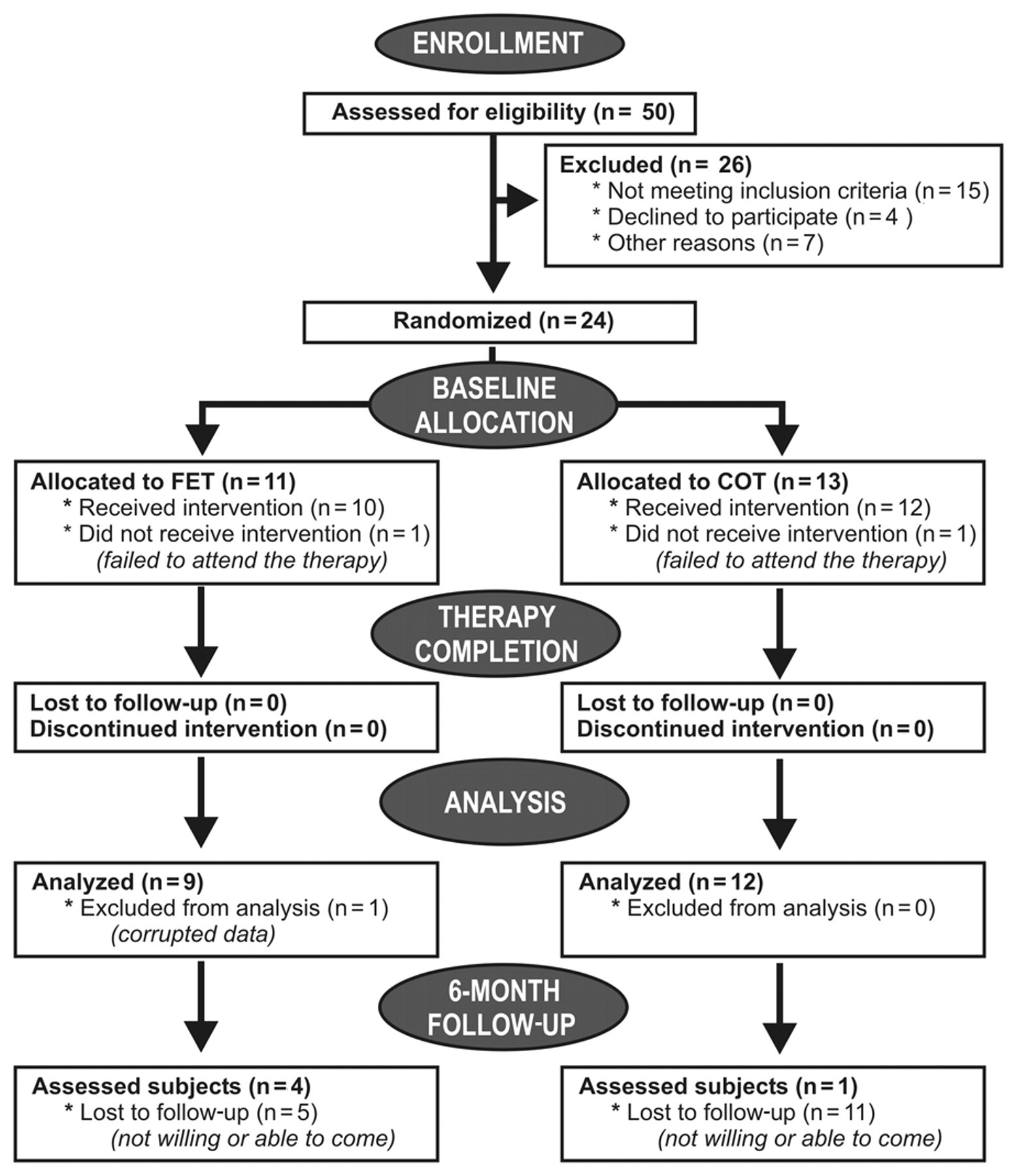
CONSORT diagram showing the recruitment process and the recruitment numbers Abbreviations: FET, functional electrical stimulation therapy; COT, conventional occupational therapy.
Subjects’ Demographic and Neurological Data
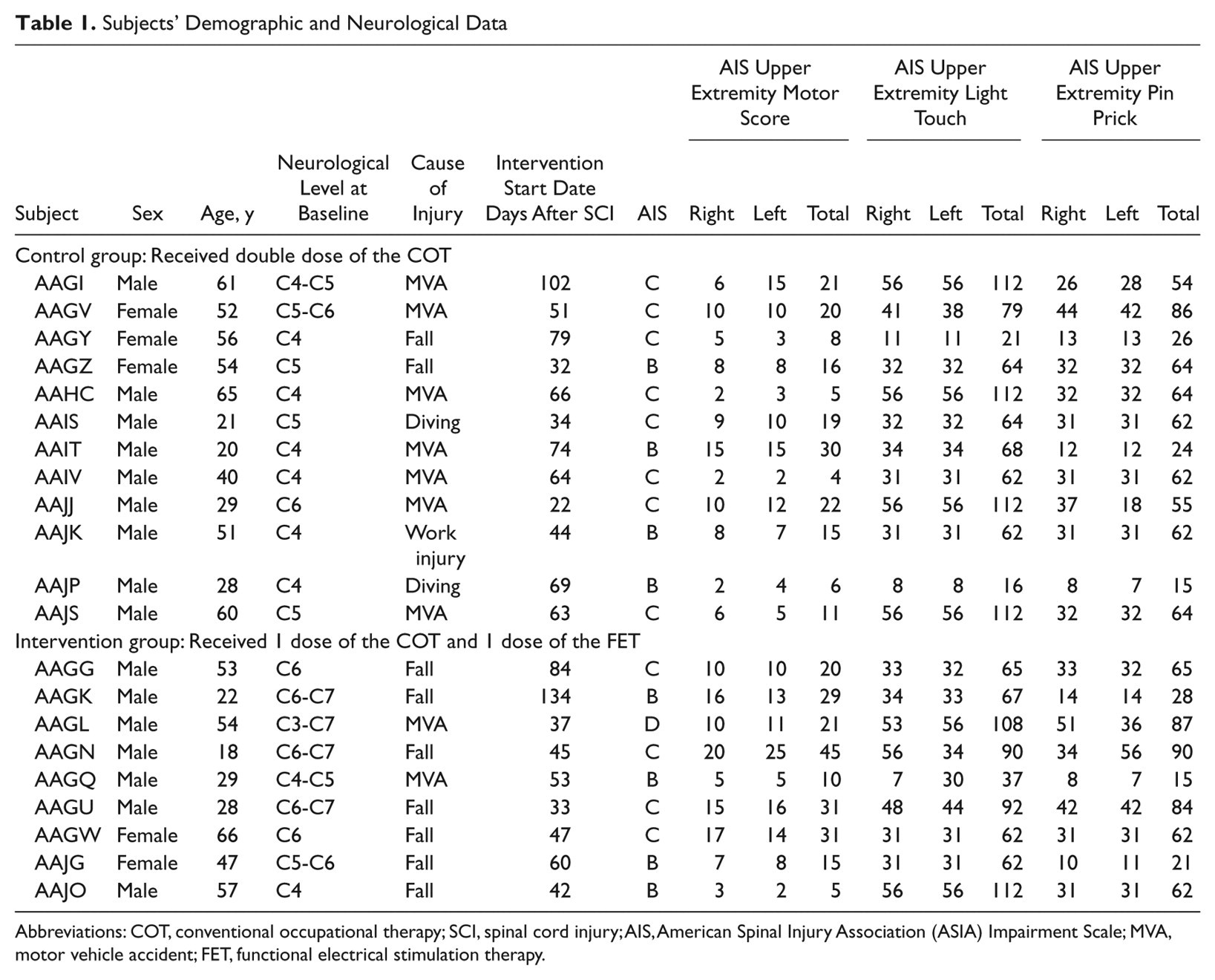
Abbreviations: COT, conventional occupational therapy; SCI, spinal cord injury; AIS, American Spinal Injury Association (ASIA) Impairment Scale; MVA, motor vehicle accident; FET, functional electrical stimulation therapy.
At baseline there was no clinically significant difference between the groups (Table 2). At completion, both intervention and control groups improved (Table 3 and Figure 3). However, the FET group improved more (Table 4). Statistically significant improvements were observed in FIM self-care subscores, SCIM self-care subscores, TRI-HFT instrumented cylinder scores, and TRI-HFT credit card scores (Figures 4 and 5). Trends with repeated-measures testing were found for the TRI-HFT total score for manipulation of objects 1 to 10 12,17,18 (P = .054) and the TRI-HFT wooden bar test score (P = .0652). No statistically significant difference between the intervention and control groups was found for the TRI-HFT 9 rectangular blocks test.
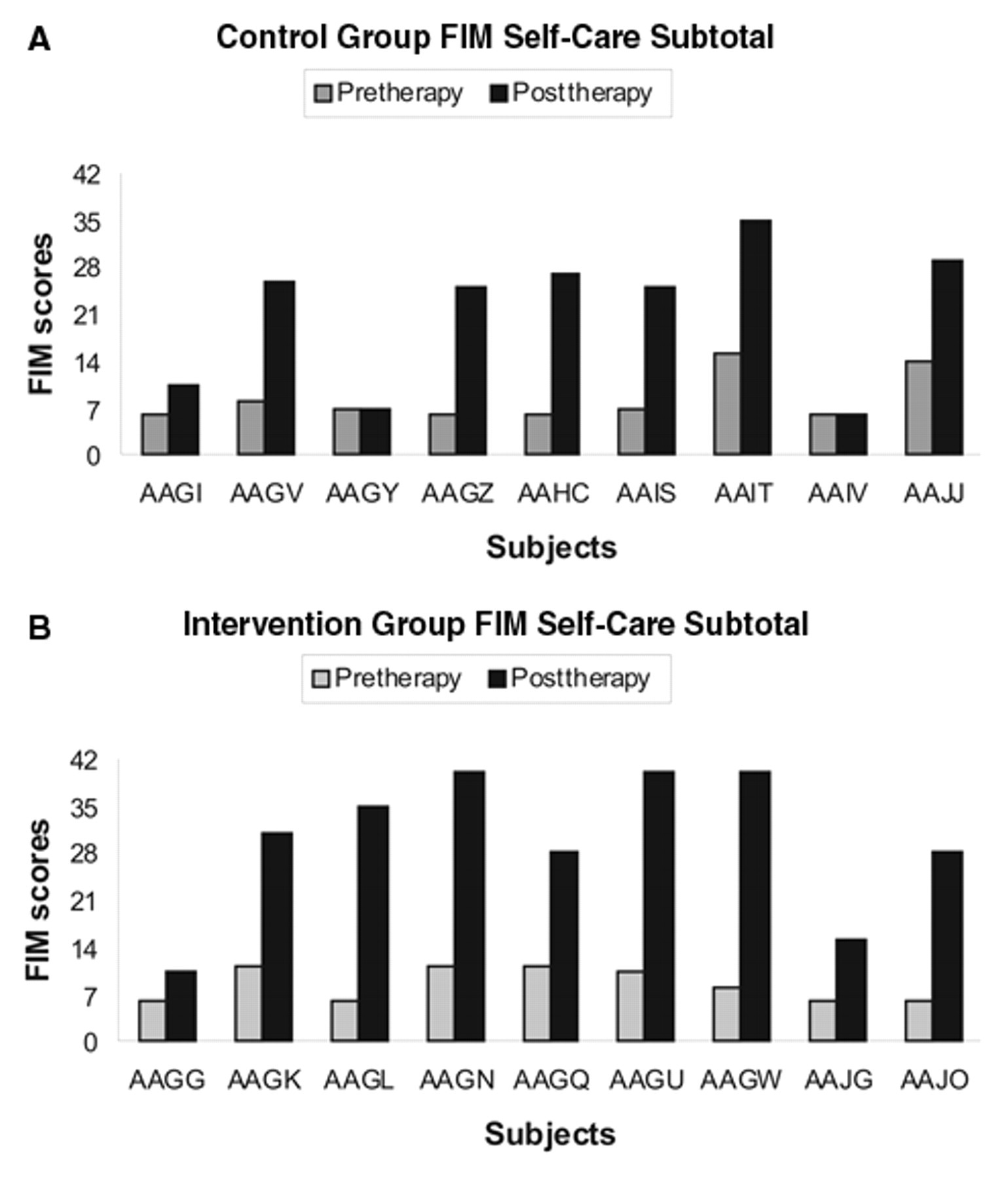
(A) Subjects’ Functional Independence Measure (FIM) Self-Care subscore before and after therapy for the control group. (B) Subjects’ FIM Self-Care subscore before and after therapy for the intervention group.
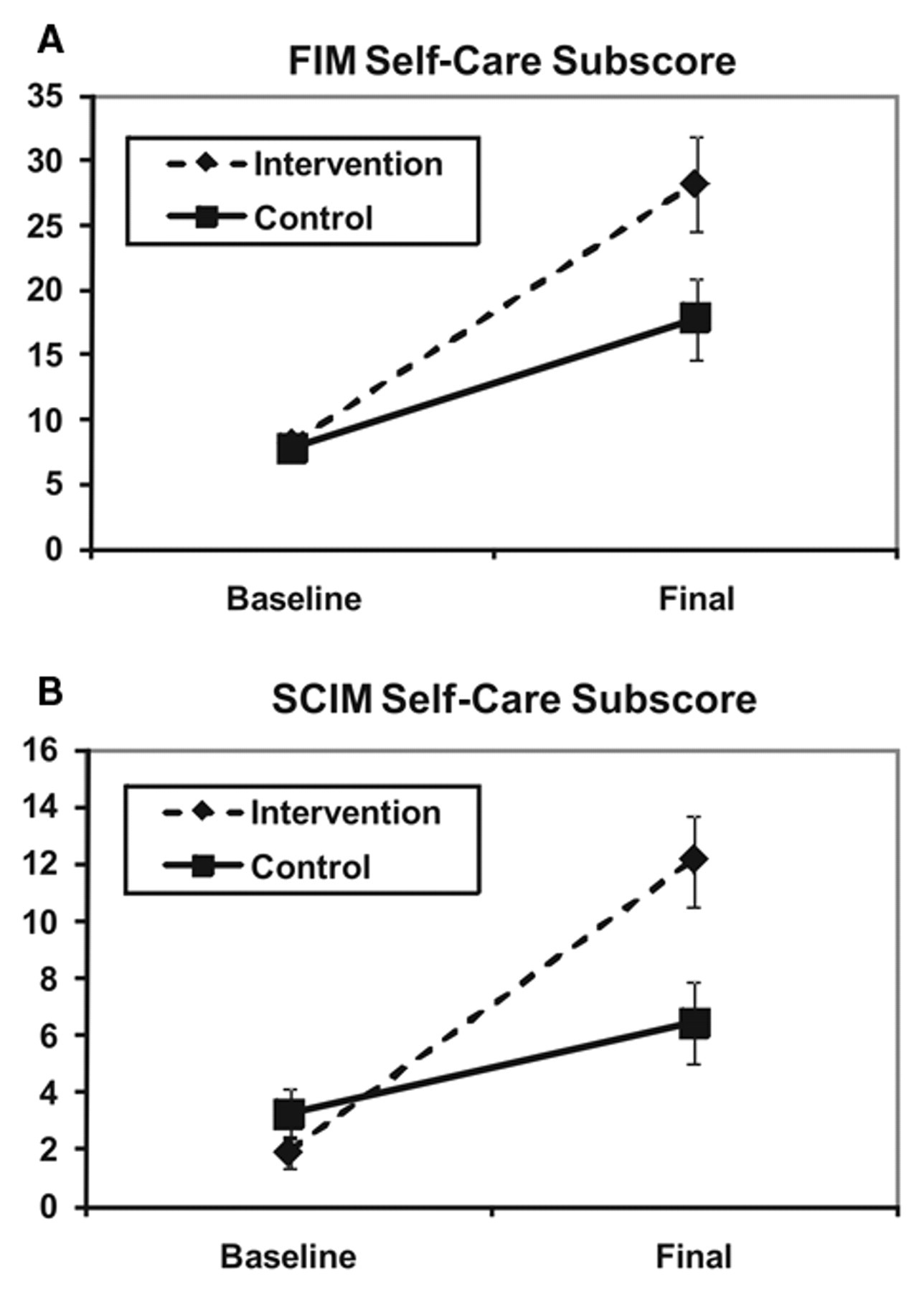
(A) Functional Independence Measure 9FIM) self-care subscores at baseline and after therapy completion for the controland intervention groups (mean ± standard error of mean). (B) Spinal Cord Independence Measure (SCIM) self-care sub-scores at baseline and after the therapy completion for the control and intervention groups (mean ± standard error of mean).
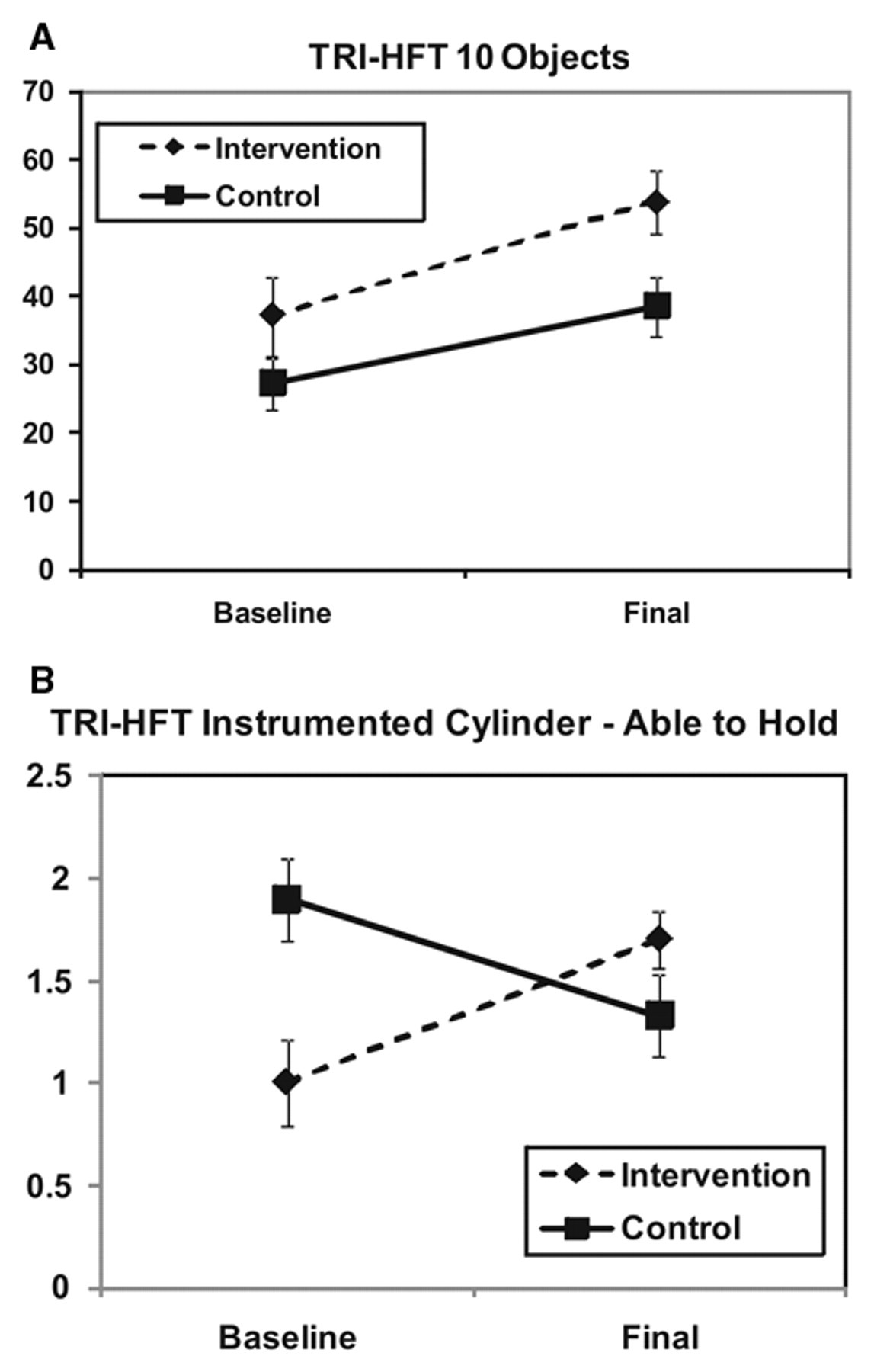
Toronto Rehabilitation Institute Hand Function Test (TRI-HFT) 10 objects (objects 1 to 10 in Refs [12, 17, 18]) total score at baseline and after therapy completion for the control and intervention groups (mean ± standard error of mean). (B) TRI-HFT Instrumented Cylinder—Able to Hold (object 12 in Refs [12, 17, 18]) score at baseline and after therapy completion for the control and intervention groups (mean ± standard error of mean)
Baseline Data Comparisons Between Control and Intervention Groups
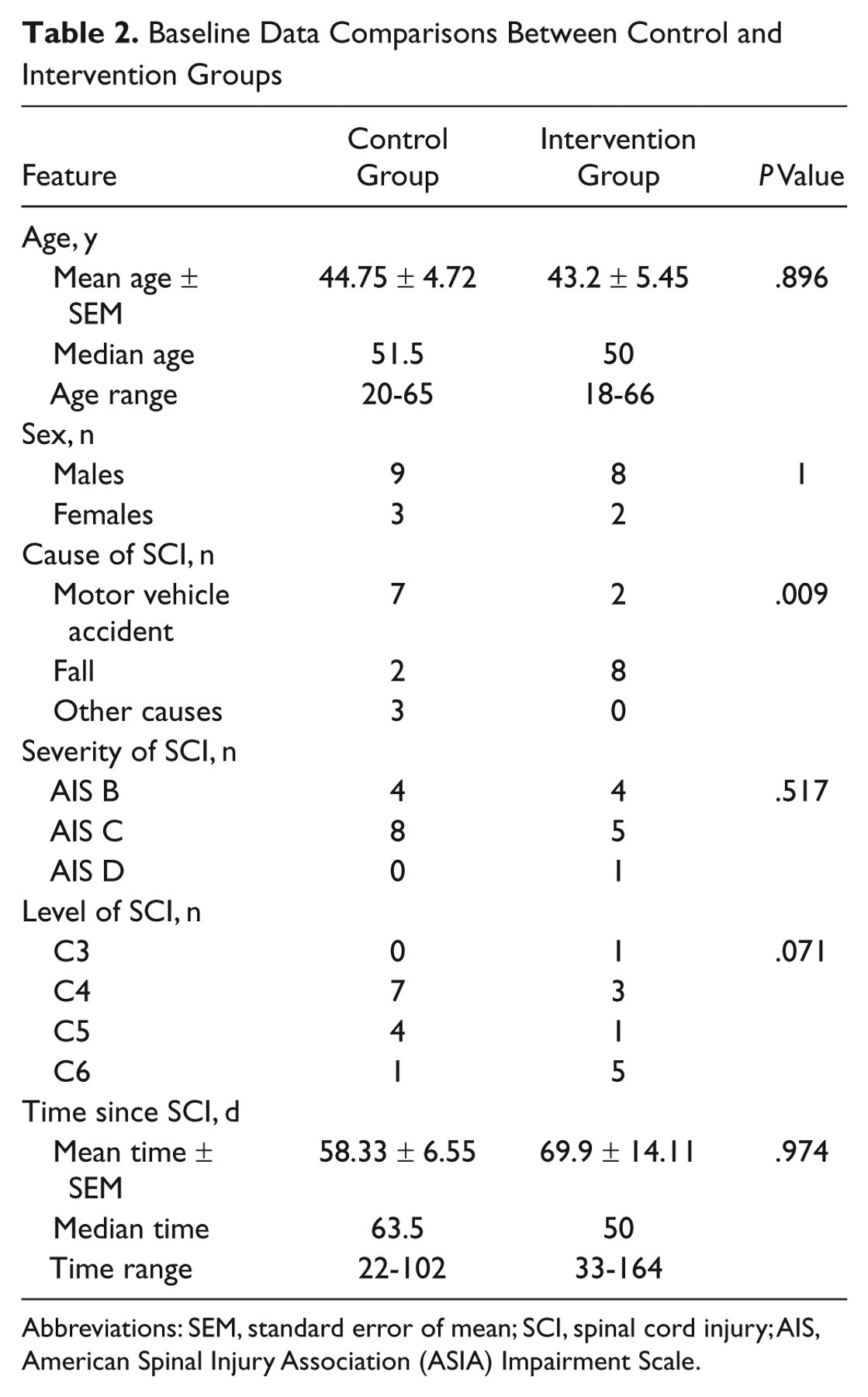
Abbreviations: SEM, standard error of mean; SCI, spinal cord injury; AIS, American Spinal Injury Association (ASIA) Impairment Scale.
Individual Subjects’ FIM Self-Care, Sphincter Control, and Motor Subscores for the Intervention and Control Groups
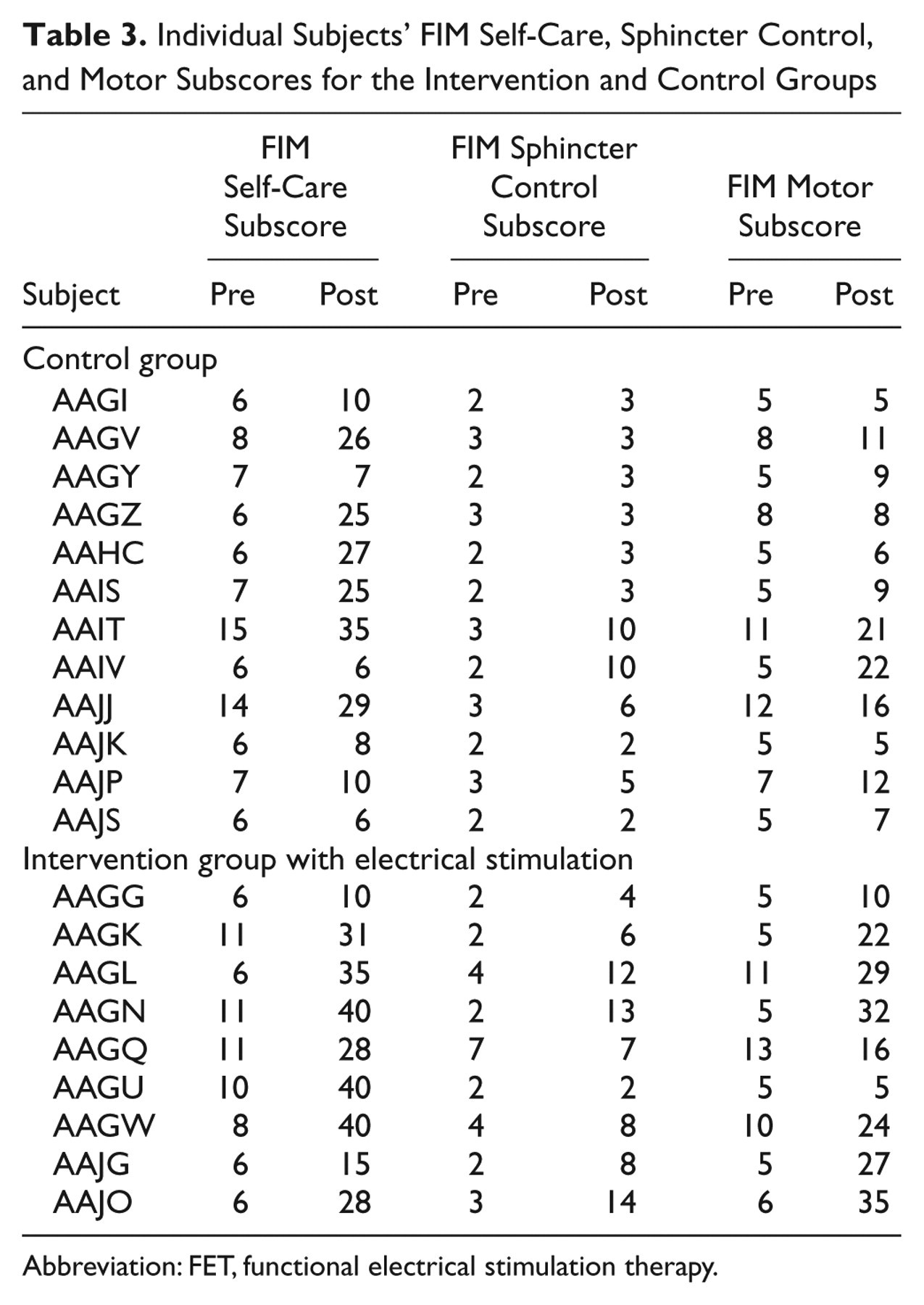
Abbreviation: FET, functional electrical stimulation therapy.
Summary of the Mean Test Results for the Control and Intervention Groups at Baseline (Before) and on Completion of the Therapy (After), With Corresponding P Values a
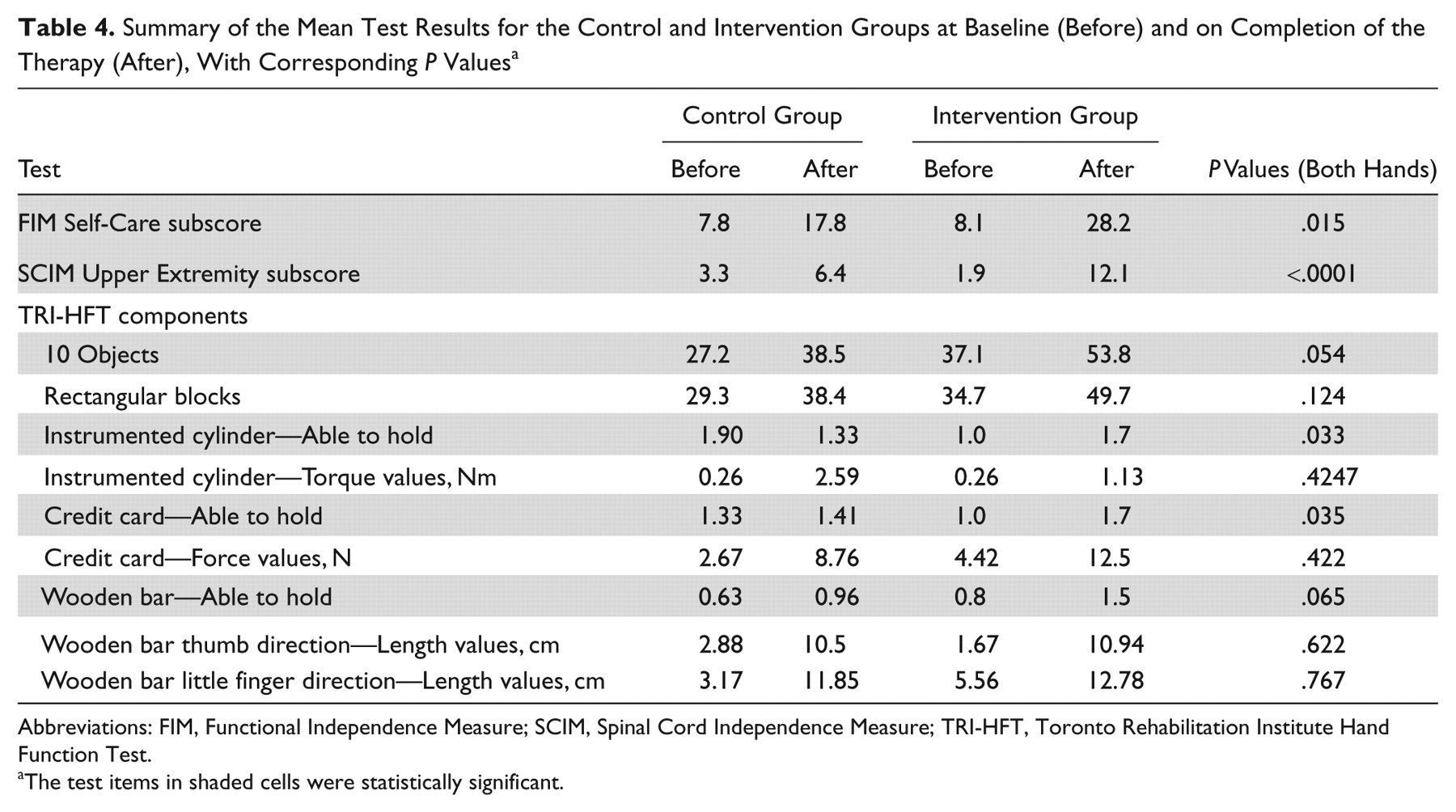
Abbreviations: FIM, Functional Independence Measure; SCIM, Spinal Cord Independence Measure; TRI-HFT, Toronto Rehabilitation Institute Hand Function Test.
The test items in shaded cells were statistically significant.
Discussion
This is the first randomized controlled trial evaluating the efficacy of FET in individuals with subacute incomplete tetraplegia after SCI. Statistically significant differences in hand function were found in favor of the FET intervention despite a small sample size (12 in the control group and 9 in the intervention group) and large variability.
The results suggest the efficacy of a surface FET intervention that can be tailored and adjusted to patients’ needs on a daily basis and can evolve as patients improve their function. Furthermore, our findings suggest that if a subject who attempts to execute a grasping task is assisted with the FET to carry out that task, he/she is effectively voluntarily generating the motor command. FET is providing afferent feedback (system’s output), indicating that the command was executed successfully. We hypothesize that by providing both the command input and system’s output to the central nervous system repetitively over enough time, this type of treatment may facilitate functional reorganization within the sensorimotor network. It is important to add that during the intervention the subjects were performing grasping tasks repetitively. We believe that the combination of performing diverse and meaningful tasks with high repetition and subject’s persistent active engagement (ie, all subjects had to devote 100% of their attention to the tasks performed) may have played a critical role in retraining voluntary grasping functions. These strategies are fully in tune with recent findings in the field of neuroplasticity 20 and suggest that the proposed FET is potentially another effective method that can be used to retrain the neuromuscular system.
The results are quite different from those reported in the study where FET was applied to patients with severe hemiplegia. 17,18 Stroke subjects did not experience dramatic improvements in FIM scores. This finding is explained by the typical bilateral disability of persons with SCI, which is not the case in individuals with hemiplegia. Individuals with hemiplegia, with time and intensive therapy, learn how to reach and grasp objects using the least affected arm, without engaging the more affected arm in ADLs. Hence, in these subjects, improving the function in the disabled arm does not produce significant changes in FIM scores. However, in the individuals with SCI, who typically have bilateral disability, even small improvements in hand function may produce measurable improvements in the FIM and SCIM scores. The results suggest that FET applied to hand function in individuals with SCI positively affects performance in ADLs and increases independence measured by the FIM and SCIM.
What is unique about this study is that we provided 1 dose of COT (1 hour of therapy) daily to both the intervention and control groups, followed by 1 dose of either COT or FET. The study design intentionally put FET in a possibly less favorable position compared with the double dose of the task-related COT.
A limitation of this study is that despite considerable effort we failed to attract the subjects to take part in a 6-month follow-up assessment. This can be explained by the fact that the majority of the subjects were discharged home or to long-term care facilities that were far from the study site.
The positive results, as well as results of our preceding study, 12 suggest that individuals with SCI would benefit from FET for grasping and voluntary hand function. We recommend at least 40 one-hour sessions of FET to try to improve upper limb function. Only after the patient has not shown signs of improvement should other invasive procedures be considered, such as implanted neuroprostheses for grasping and tendon transfers.
We have trained more than 30 occupational therapists, physiotherapists, and biomedical engineers to administer the FET. Most of the physiotherapists and occupational therapists already knew how to use electrical stimulation systems, so minimal additional training, up to 2 hours, was needed. Donning and doffing the system requires no more than 5 minutes. From a logistics perspective, FET may be easily integrated into existing occupational therapy programs without requiring additional treatment hours or funds beyond those needed to purchase a programmable FES system.
Footnotes
Acknowledgements
The authors would like to acknowledge the valuable assistance of Kieva Richards, Jennifer Holmes, Suzanne Iafolla, Tamara Schultz, Melanie Alappat, Farhana Jaffer, Grant Murray, Sylvia Haycock, and Abdul Kadir Bulsen, who helped with delivering the therapy and performing the assessments.
The author(s) declared no potential conflicts of interest with respect to the authorship and/or publication of this article.
The author(s) disclosed receipt of the following financial support for the research and/or authorship of this article: The work presented in this article was supported by grants from The Physicians’ Services Incorporated Foundation (PSI Grant #05-06) and Christopher and Dana Reeve Foundation (TA1-0706-2). Additional financial support for this study was received from the Toronto Rehabilitation Institute and Ontario Ministry of Health and Long-Term Care.