
Abstract
Objective:
To analyze the epidemiology and outcome for patients with HIV coinfected with hepatitis in comparison with monoinfected patients.
Methods:
At the First Affiliated Hospital at Xinjiang Medical University in Urumqi, China, 395 patients were diagnosed with HIV between 2001 and 2010. The main routes of transmission were sexual (30%) and intravenous drug use (33%). The patient records were studied retrospectively.
Results:
A total of 135 patients had markers of viral hepatitis (34.2%). Abnormal liver function was seen among 48.9% of these patients. Hepatitis B surface antigen was positive in 24 patients (6.1%), with 15 (3.8%) being hepatitis B virus (HBV)-DNA positive, none on tenofovir treatment, because it is still not provided free in Xinjiang. Hepatitis C antibodies were found in 98 patients (24.8%), 46 (11.6%) were hepatitis C virus (HCV)-RNA positive. Only 1 patient had been treated with interferon and ribavirin. Both HBV and HCV were found in 13 (3.3%) of the patients.
Conclusions:
Nearly half of the HIV patients in Urumqi had markers of hepatitis. Only antiretroviral treatment is provided free, and most of the patients cannot afford the hepatitis treatment they need, which has to be addressed in the treatment programs.
Introduction
HIV, hepatitis B virus (HBV), and hepatitis C virus (HCV) have the same main routes of transmission: intravenous drug use (IVDU), sexual intercourse, blood transfusion, and mother-to-child transmission. After the introduction of highly active antiretroviral therapy (HAART), the mortality of the HIV-positive patients has decreased, but the survival of the patients coinfected with hepatitis is still low.
HIV infection accelerates the course of HCV-related liver damage to cirrhosis, end-stage liver disease, and death. 1 –9 Consequently, compensated and decompensated liver cirrhosis are common in these patients. The evolution of compensated HCV-related cirrhosis in monoinfected patients is slow in most patients but can be accelerated by alcohol abuse, HBV infection, and metabolic disorders. 10 –12 Therapy to treat HCV can delay the development of liver-related clinical events. 13
Although the outcome of decompensated cirrhosis in HIV-HCV-coinfected participants is well known, 6 –8,14 the few reported studies on compensated cirrhosis have low sample sizes or have dealt only slightly with predictors of clinical outcome. 15
Materials and Methods
This was a retrospective study of the 395 consecutive HIV-positive patients registered at the First Affiliated Hospital of Xinjiang Medical University, Urumqi, China, during 2001 to 2010. The sex distribution and ethnic groups are presented in Table 1.
Sex Distribution by Ethnic Group.

The patients were followed from registration to December 2010. The mean time of follow-up was 68.4 months.
Mean age of the patients was 36.8 years. The mean age with HIV monoinfection was 34.8 years, with HIV + HBV was 38.2 years, with HIV + HCV was 30.5 years, and with HIV + HBV + HCV was 35.7 years.
Appointments were scheduled at least every 6 months. Clinical, virological, immunological, and biochemical evaluations were performed at every appointment. Liver disease was managed primarily by specialists in infectious diseases, in accordance with the protocols described elsewhere. 6,7 Liver dysfunction was classified according to the Child-Pugh criteria. 16
Antibodies to HCV were analyzed with enzyme-linked immunosorbent assay ([ELISA] WC-3196, Company of Beijing Wantai [Zhongguancun Life Science Park in Beijing, China]). Both HBV-DNA and HCV-RNA were tested with FQ-PCR provided by DAAN Gene Co, Ltd (Sun Yat-sen University, Guangzhou, China). The level of detection of the positive HBV-DNA was 102 copies/mL, and for positive HCV-RNA it was 103 copies/mL.
Results
Among the 395 HIV-positive patients, 329 were HIV positive and 66 were asymptomatic with CD4 count >350/μL, and 370 patients were on antiretroviral therapy (ART).
Hepatitis B surface antigen (HBsAg) was positive in 24 patients (6.1%), with 15 (3.8%) being HBV-DNA positive. None of the patients were on ART, including tenofovir (TDF). Hepatitis C antibodies were found in 98 patients (24.8%), and 46 (11.6%) were HCV-RNA positive. Only 1 patient had been treated with interferon and ribavirin. Both HBV and HCV were found in 13 (3.3%) of the patients.
The prevalence of coinfections with hepatitis B and/or hepatitis C is presented in relation to ethnic group and sex in Table 2.
Coinfections with Hepatitis B and C by Sex and Ethnic Group.

Abbreviations: HBV, hepatitis B virus; HCV, hepatitis C virus.
The proportion of the patients with liver dysfunction is presented in Table 3. Among the patients with positive HBsAg, 6% had liver dysfunction; those with positive HCV-RNA, 70% had liver dysfunction; and among patients with both hepatitis B and C, 39% had impaired liver function. One patient with hepatitis B and C died of liver failure. The proportion with liver function impairment was 23 (44%) of 52 among the HCV antibody positive patients with negative HCV-RNA.
Liver Function of HIV + Hepatitis Coinfected Patients.
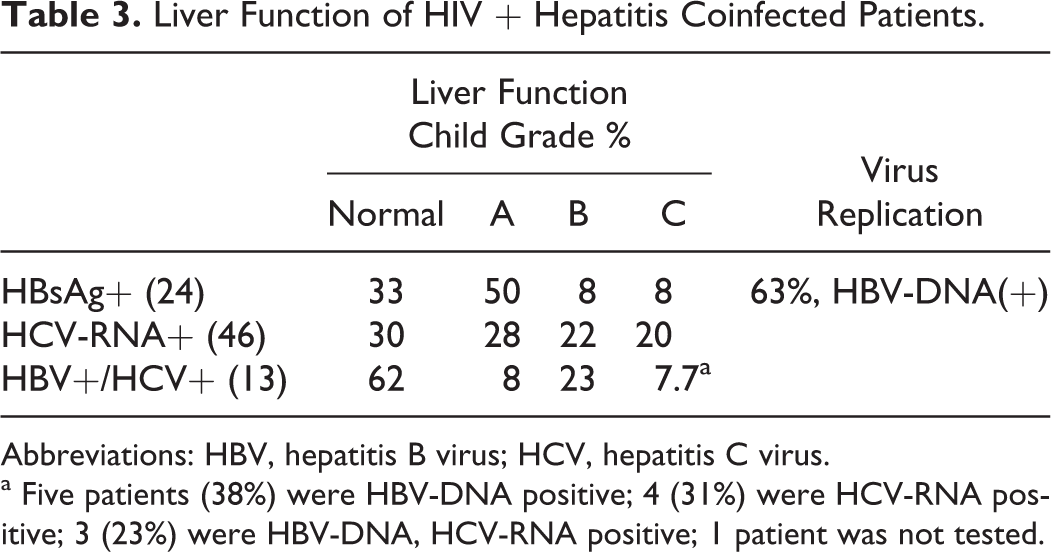
Abbreviations: HBV, hepatitis B virus; HCV, hepatitis C virus.
a Five patients (38%) were HBV-DNA positive; 4 (31%) were HCV-RNA positive; 3 (23%) were HBV-DNA, HCV-RNA positive; 1 patient was not tested.
The reported routes of transmission are presented in Table 4. For patients with hepatitis C coinfection, IVDU was the dominant route of transmission, and for those with hepatitis B coinfection sexual route was the most common route. For patients with HIV monoinfection, both sexual and intravenous drug transmissions were equally common.
Routes of Transmission of HIV Patients Coinfected with Hepatitis.a

Abbreviations: HBV, hepatitis B virus; HCV, hepatitis C virus; IVDU, intravenous drug use.
a R × C contingency tables with imprecise probability method: P = .007. There is a statistically significant difference between hepatitis B and hepatitis C regarding routes of transmission.
Discussion
In our study, 6.1% of the HIV-positive patients had positive HBsAg. In addition, patients with positive antibody to hepatitis B core antigen may have active hepatitis B, but HBV-DNA was not tested in this group. It has been reported that patients with hepatitis B coinfection have 3.5 times higher incidence of decreased liver function than HIV-positive patients without HBV coinfection. 17 The immunodeficiency caused by HIV can result in a false low prevalence of HBV if HBV-DNA is not analyzed. After HAART, the immunity improves and the HBV serum markers can change. 18 Patients with HIV/AIDS with HBsAg positivity can be cured of their hepatitis B infection, become HBV-DNA negative, and produce anti-HBs. 19 Studies of HIV/HBV-coinfected patients and some preliminary clinical data on monoinfected patients suggest the importance of TDF treatment because of its high potency and low risk of resistance profile. Tenofovir is a superior anti-HBV agent compared to lamivudine (3TC). 20 –22 In the treatment of HIV/HBV coinfection, a combination of TDF with emtricitabine or 3TC is recommended, but emtricitabine is not available in Xinjiang. Tenofovir is available in Xinjiang, but none of the patients in our retrospective analyses received this treatment, because it has not been offered free of charge. HIV patients without HBV should be vaccinated with HBV vaccine. Patients with advanced HIV with low CD4 count, however, respond poorly to the HBV vaccine. 17
In our study, the HCV prevalence was 35.8%, thus much higher than that in the general population in China, which is 3.2%. 23 One patient with HCV and 1 with both HBV and HCV died. The relative risk of death in HIV-HCV-coinfected patients with decompensated cirrhosis has been reported to be 2.26 (95% confidence interval, 1.51-3.38), in relation to HCV-monoinfected patients. 6 HIV patients coinfected with HBV/HCV can have accelerated HBV/HCV virus replication, which in turn accelerates liver disease progression and speeds up the cirrhosis, resulting in increased mortality. 24,25 Because of the frequency of IVDU in our province, many of our HIV-positive patients are coinfected with HCV. Intravenous drug use increases the frequency of both HIV and HCV. 24,26 The main route of HIV transmission among all patients was IVDU (33%). We found liver function impairment among 70% of the HCV-RNA-positive patients, but in most cases it was mild. Only 1 of the 110 patients coinfected with HCV, in our study, had received interferon and ribavirin treatment in addition to ART and the patient also responded well. It has been shown that starting anti-HCV treatment when the CD4 count is high is considered most effective. 27
HIV patients coinfected with both HBV and HCV may develop severe liver damage. 28 Patients with HIV who are coinfected with hepatitis B and C must be treated for their hepatitis together with the ART to achieve good long-term survival and low morbidity. Several studies are ongoing to determine the optimal treatment program. Because many HIV-positive patients are coinfected with HBV and HCV from IVDU, and there is no free treatment for HBV/HCV, treatment is a challenge, as so many of these patients are infected through IVDU.
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.