
Abstract
Objective
Hospital-based, cross-sectional study to determine whether exposure to hepatitis B virus (HBV) has an independent effect on the risk of developing chronic kidney disease (CKD).
Methods
Han Chinese adults undergoing routine physical examinations were recruited. Blood was tested for the presence of hepatitis C virus (HCV) antibodies, HBV surface antigen, and antibodies against HBV core antigen and hepatitis B surface antigen (HBsAg). CKD was defined as estimated glomerular filtration rate (eGFR) <60 ml/min per 1.73 m2 or presence of albuminuria.
Results
The prevalence of HBV exposure was 42.1% (6 418/15 259 participants). There were no significant associations between HBV or HCV status and CKD, low eGFR or albuminuria.
Conclusion
There was no association between exposure to HBV and the risk of developing CKD in this Chinese study population.
Introduction
Hepatitis B virus (HBV) infection is a major global public health problem with a widely varying prevalence.1,2 In mainland China the prevalence of HBV surface antigen (HBsAg) was found to be 7.2% in the general population and 1.1% in children aged <5 years. 3 Both HBV and hepatitis C virus (HCV) are significantly associated with end-stage liver diseases including hepatocellular carcinoma (HCC) and cholangiocarcinoma. 4 In addition, hepatitis is a systemic infectious process, and HBV can travel through the bloodstream and be deposited in the kidney. 5 Glomerular deposition of HBV antigens has been observed in long-term HBV carriers with different glomerulonephritis entities, although the aetiological role of HBV is uncertain. 6
A cross-sectional survey from China showed that the prevalence of chronic kidney disease (CKD) is 10.8%, equivalent to a total of 119.5 million adults. 7 Factors associated with CKD include hypertension, diabetes, older age, nephrotoxic medication use and high-density lipoprotein-cholesterol (HDL-C) concentration.7–11 It is also known that uric acid induces small-vessel disease in the kidney, and that a low serum albumin level is a significant predictor for progression of renal function via an inflammatory mechanism.12–14
Clinically, it has been observed that HBV infection is associated with nephropathy, 15 but the association between CKD and HBV infection remains unclear. HCV infection, but not HBV infection, has been significantly associated with the prevalence and disease severity of CKD in HBV and HCV endemic areas in Taiwan, 16 but others found no association between HCV and risk of CKD. 17 It has been shown that HBV infection with elevated alanine aminotransferase is significantly associated with reduced renal function in Chinese adults aged 30–75 years. 18 However, these studies analysed HBsAg data, rather than patients who had recovered from acute or chronic HBV infection. To the best of our knowledge, there have been no studies to determine the association between CKD and prior exposure to HBV. The aim of the present large sample study was to evaluate whether or not previous exposure to HBV is associated with CKD.
Patients and methods
Study population
This hospital-based, cross-sectional study recruited 15 600 subjects aged ≥18 years, undergoing physical examinations at the Chinese PLA General Hospital, Beijing, China, between December 2009 and June 2012. Subjects with severe hepatic disease or incomplete HBsAg/HCV data were excluded. Data regarding age, sex, diabetes mellitus, hypertension, height, weight and blood pressure were collected using standard methods as part of the health examination procedure.
The study was approved by the hospital’s Institutional Review Board and Ethics Committee, and participants provided written informed consent.
Laboratory analyses
Venous blood (5 ml) was collected after an overnight fast (≥12 h) for quantification of biochemical parameters. Serum was separated by leaving the whole-blood sample to stand at room temperature for 4 h, then centrifuging at 2500
Serum total cholesterol, low-density lipoprotein cholesterol (LDL-C), high-density lipoprotein cholesterol (HDL-C), triglycerides and uric acid were measured using commercially available reagents (Roche Diagnostics).
Urinalysis was performed with spontaneously voided clean-catch midstream fresh urine collected in the morning and stored at 4°C for <1 week. Albumin was quantified via immunoturbidimetry (Turbox Microalbuminuria; Orion Diagnostica Oy, Espoo, Finland). Creatinine was quantified using Jaffe’s kinetic method. 19 Urinary albumin-to-creatinine ratio (ACR; mg/g creatinine) was calculated.
Study definitions
Chronic HBV infection was defined as the presence of HBsAg. Resolved acute/chronic HBV infection was defined as absence of HBsAg and presence of anti-HBs antibodies.16,17 Subjects positive for anti-HBc antibodies but negative for HBsAg and anti-HBs antibodies were defined as having being exposed to HBV and possibly harbouring persistent HBV infection. 20 Individuals positive for anti-HCV antibodies were defined as having chronic HCV infection. 21
Diabetes mellitus was defined as fasting plasma glucose >7.1 mmol/l, history of diabetes mellitus, or current hypoglycaemic drugs or insulin use. Hypertension was defined as systolic blood pressure >140 mmHg, diastolic blood pressure >90 mmHg, history of hypertension, or current antihypertensive drug use.
Albuminuria was defined as ACR >30 mg/g. The estimated glomerular filtration rate (eGFR) was calculated using an equation developed by adapting the Modification of Diet in Renal Disease equation on the basis of data from Chinese CKD patients, 22 and CKD was defined as eGFR <60 ml/min per 1.73 m2 or the presence of albuminuria. Chronic kidney disease was staged according to Kidney Disease Outcome Quality Initiative guidelines, 23 with stage 3 further classified as stage 3a or 3b using eGFR 45 ml/min per 1.73 m2 as the cutoff.
Statistical analyses
Data were presented as mean ± SD for continuous variables and frequencies (%) for categorical variables. Differences among viral hepatitis groups were compared using one-way analysis of variance or χ2-test, as appropriate. Univariate and multivariate logistic binary regression analyses were used to study crude and adjusted associations with CKD, with adjustment of covariates to include potential confounders, including age group by quartile (<51, 51–61, 62–69, and ≥70 years), sex, body mass index, albumin, lipid, uric acid, hypertension and diabetes mellitus. The same multivariate model was used to test the association between viral hepatitis and eGFR. P-values <0.05 were considered to be statistically significant. SAS® version 9 (SAS Institute Inc., www.sas.com) was used for all statistical analyses.
Results
A total of 15 600 participants completed the adult health examination during the study period. After excluding 16 participants with cirrhosis (including two patients with cirrhosis and ascites) and 35 with no HBV results, 15 549 individuals were included in the final analysis (10509 [67.6%] male/5040 [32.4%] female; mean age 49.2 ± 9.3 years; age range 18–89 years). The study population mainly originated from northern China, with the majority being of the Han ethnic group. HBV data were unavailable for 290 subjects (1.9%).
Demographic and clinical data from subjects included in a study to investigate the relationship between viral hepatitis and chronic kidney disease (CKD), stratified according to hepatitis B virus (HBV) and hepatitis C virus (HCV) status.
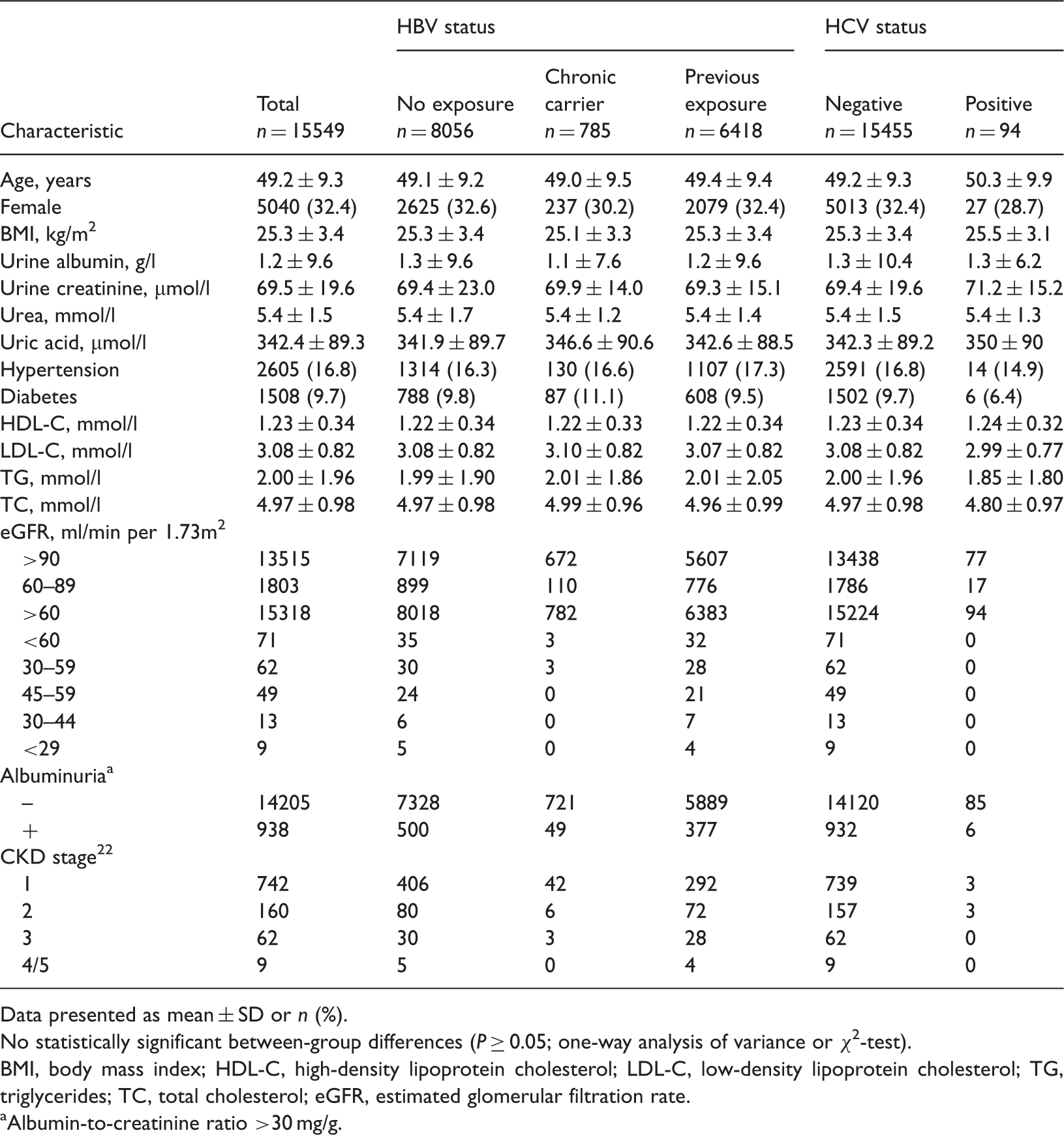
Data presented as mean ± SD or n (%).
No statistically significant between-group differences (P ≥ 0.05; one-way analysis of variance or χ2-test).
BMI, body mass index; HDL-C, high-density lipoprotein cholesterol; LDL-C, low-density lipoprotein cholesterol; TG, triglycerides; TC, total cholesterol; eGFR, estimated glomerular filtration rate.
Albumin-to-creatinine ratio >30 mg/g.
Univariate and multivariate logistic regression analyses of factors associated with chronic kidney disease in Chinese adults (n = 15 549).

Data presented as odds ratios (95% confidence intervals).
Statistically significant (P-values < 0.05).
CI: confidence interval; HBV: hepatitis B virus; HCV: hepatitis C virus; BMI: body mass index; HDL, high-density lipoprotein cholesterol; LDL, low-density lipoprotein cholesterol; TG, triglycerides; TC, total cholesterol.
Multivariate logistic regression analysis for the association between viral hepatitis and low estimated glomerular filtration rate (eGFR) or albuminuria in Chinese adults (n = 15 549).

Data presented as odds ratios (95% confidence intervals).
Multivariate logistic regression analysis adjusted for age, sex, body mass index, albumin, hypertension, diabetic mellitus, total cholesterol, triglyceride, and low-density lipoprotein cholesterol.
HBV: hepatitis B virus; HCV: hepatitis C virus.
<60 ml/min per 1.73 m2.
Discussion
The present large-scale population study confirmed that there is no association between prior exposure to HBV and the risk of CKD, after controlling for known CKD risk factors. In addition, there were no significant associations between HBV status and low eGFR or albuminuria.
The absence of any association between HBV exposure and CKD in the present study is unsurprising for two reasons. First, it has been documented that men with HBV have higher morbidity and mortality than women in terms of HCC and cirrhosis. 24 The participants in the current study had a mean age of nearly 50 years, with 67% being male. The high viral load required for HBV to accelerate kidney damage would also affect liver function and increase mortality, therefore such individuals were excluded from the present study. Secondly, the immune response to HBV is present only in patients with active hepatitis B, and this response plays a role in both hepatitis B and HBV-associated nephropathy. HBV replication may accelerate apoptosis of renal tubular cells and subsequently contribute to deterioration in renal function.25,26
The present study had several strengths. Our analysis was conducted in a large, demographically diverse group that was a close reflection of the general population seen in outpatient clinics across China. In addition, the mean age for patients with HBV and the distribution of CKD in our cohort were similar to those found in analyses of National Health and Nutrition Examination Survey data.3,7 The reliance on a positive test to identify patients with past exposure to HBV minimized any ascertainment bias in classifying patients with HBV. Access to a broad array of data sources allowed us to capture and adjust for a wide range of patient-level variables that may have affected the development of CKD. Finally, our finding that diabetes, hypertension and age-related risk factors were correlated with CKD is in accordance with the results of others.10,18
Our study had some limitations. Since people with prior exposure to HBV were diagnosed during a physical examination, liver tissue was not available for HBV DNA analysis and we cannot rule out the possibility of selection bias due to low-grade viral replication in HBc-positive patients. Moreover, no kidney damage was demonstrated during the routine health examinations of HBsAg-positive patients, who have a much higher risk of substantial viral replication and potential immune reactions that can also affect the kidney (cryoglobulins, Ag deposition in the glomeruli, and deposition of viral particles).
In conclusion, there was no association between exposure to HBV and the risk of developing CKD in a Han Chinese population. It is possible that the combined effects of risk factors such as HCV, HBV, hypertension and diabetes, might increase susceptibility to chronic inflammation, DNA damage and development of CKD.
Footnotes
Declaration of conflicting interest
The authors declare that there are no conflicts of interest.
Funding
This work was supported in part by a grant from the State Science and Technology Support Program (No. 2012BAI37B04).