
Abstract
Vitamin D plays role in bone health and the regulation of the immune system. A cross-sectional study of serum 25-hydroxyvitamin D (25[OH]D) levels was conducted among HIV-1-infected Thai patients to determine the prevalence and associated factors of low vitamin D levels (25[OH]D <30 ng/mL) in tropical setting. 25-Hydroxyvitamin D was measured by liquid chromatography/tandem mass spectrometry. Of 178 patients, 58% received antiretroviral therapy at median (interquartile range [IQR]) duration of 7.4 (5.9-8.5) years. The prevalence of 25(OH)D deficiency (<20 ng/mL) and insufficiency (20-29.9 ng/mL) was 26.8% and 44.9%, respectively. Multivariate analysis showed that receiving efavirenz (EFV) was significantly associated with low vitamin D status (odds ratio = 3.60; 95% confidence interval, 1.06-12.15, P <.05). The mean (±standard deviation) level of 25(OH)D in patients receiving and not receiving EFV was 22.9 (6.6) and 28.6 (10.7) ng/mL, respectively, (P <.05). Low vitamin D status is common and needs to be assessed among HIV-infected patients including tropical residents especially when EFV is used.
Introduction
Vitamin D is essential for calcium and bone homeostasis. The discovery of vitamin D receptors in many organs of the body has led to a new perspective of vitamin D function. 1 –3 In the past decade, increasing evidences suggest that vitamin D plays an important role in regulating the immune system. 4 –7 In vitro data demonstrated that HIV-1 replication is inhibited by cathelicidin, an antimicrobial peptide that can be activated in macrophages and monocyte by active vitamin D. 8,9 Vitamin D can also regulate the cytokine release from adaptive immunity that involves tropism-specific HIV-1 co-receptor expression. 10 Recent data have demonstrated both higher risk of HIV-1 disease progression and higher mortality in HIV-1-infected pregnant women with low vitamin D status. 11
25-Hydroxyvitamin D (25[OH]D) is currently considered the best indicator of overall vitamin D status. 1,12,13 Parathyroid hormone levels tend to rise when 25(OH)D is less than 30 ng/mL and active calcium absorption is optimal when the level of 25(OH)D is at least 30 ng/mL. 14,15 Therefore, the level of 30 ng/mL or greater is currently considered as the optimal value for calcium homeostasis and healthy bone metabolism. Nowadays, the level of 25(OH)D less than 20 ng/mL is considered deficiency of vitamin D, and the level of 20 to 29 ng/mL indicates a relative insufficiency of vitamin D. The level of 30 ng/mL or greater indicates sufficient vitamin D. 1
Low vitamin D status in HIV-1-infected patients has been described in many studies. 16 –21 However, most of them were conducted in European countries or the United States. Although ethnicity and sun exposure are important factors associated with vitamin D status, 22,23 limited data with regard to vitamin D status in HIV-1-infected patients are available in Asians and populations residing in the tropics. It is therefore the purpose of the present study to assess vitamin D status among HIV-1-infected patients in a tropical setting and to determine factors associated with low vitamin D levels.
Methods
Patients
A cross-sectional study was conducted among HIV-1-infected patients visiting HIV clinic at a university hospital in Bangkok, Thailand. Participants were HIV-1-infected patients aged more than 15 years. For naive patients, we enrolled consecutive cases during the study period. Patients were excluded if they had (1) active granulomatous diseases, (2) liver cirrhosis, (3) chronic kidney disease stages 4 and 5, (4) malignancies, (5) pregnancy, (6) vitamin D supplement, or (7) treatment of low bone mineral density (BMD). Demographic, clinical, history of HIV-1 infection, treatment, and laboratory data were retrieved from medical records. Behavioral data were retrieved from questionnaire. Bone mineral density assessment was performed, and blood samples were collected for measurement of 25(OH)D at the time of enrollment. All participants provided written informed consent. The study was reviewed and approved by the local Institution Review Board.
Measurement of 25(OH)D
Serum 25(OH)D was analyzed by liquid chromatography/tandem mass spectrometry (LC-MS)/MS with an Agilent 1200 Infinity liquid chromatograph (Agilent Technologies, Waldbronn, Germany) coupled to a QTRAP, 5500 tandem mass spectrometer (AB SCIEX, Foster City, California) using a MassChrom, 25-OH-Vitamin D3/D2 diagnostics kit (Chromsystems, Munich, Germany). The inter-assay and intra-assay coefficients of variation of total serum 25(OH)D level were 6.3% and 5.0%, respectively.
A level of less than 20 ng/mL was defined as vitamin D deficiency. Levels between 20 and 29.9 ng/mL were defined as vitamin D insufficiency. Low vitamin D status referred to a level less than 30 ng/mL (vitamin D deficiency or vitamin D insufficiency).
Bone Mineral Density Assessment
Whole-body dual-energy X-ray absorptiometry (DEXA) scans (Hologic Discovery A, version 12.6.1; Hologic) were conducted by radiologists. Scans were performed to assess BMD using T score of lumbar spine and neck of femur. The World Health Organization classification was used for diagnosis purposes. A T score between −1 and −2.5 standard deviation (SD) were defined as osteopenia, and a T score less than −2.5 SD was defined as osteoporosis. Low BMD referred to osteopenia or osteoporosis.
Statistics
Mean (±SD), median (interquartile range [IQR]), and frequencies (percentage) were used to show the patients’ characteristics. Study patients were categorized into 2 groups based on vitamin D status: low vitamin D status group and normal vitamin D status group. The mean values of continuous variables with normal distribution between the 2 groups were compared by Student t test. Mann-Whitney U test was used to compare the median values of continuous variables with nonnormal distribution. Categorical variables were compared by the chi-square test and Fisher exact test as appropriate. Univariate analysis was used to define the factors associated with low vitamin D status. Variables with a P <.2 in univariate analysis were included in the multiple logistic regression model. We used linear regression analysis to define the factors associated with 25(OH)D level. All statistical analyses were performed using SPSS software, version 14.0 (SPSS Inc, Chicago, Illinois). P <.05 was considered statistically significant.
Results
There were 178 patients with mean (±SD) age of 42.1 (±8.5) years and 47.2% of patients were males. Median (IQR) CD4 was 445 (333-524) cells/mm3. Median (IQR) duration of known HIV-1 infection was 6.3 (1.3-9.4) years. Of all, 58% of patients had received antiretroviral therapy (ART) at a median (IQR) duration of 7.4 (5.9-8.5) years and nonnucleoside reverse transcriptase inhibitor (NNRTI)-based ART was the most common regimen (87.5%; Table 1). The prevalence of vitamin D deficiency (25[OH]D <20 ng/mL), insufficiency (25[OH]D = 20-29.9 ng/mL), and low vitamin D status (25[OH]D <30 ng/mL) were 26.8%, 44.9%, and 70.7%, respectively. The mean (±SD) level of 25(OH)D of patients who were naive to ART was 25.0 (±7.8) ng/mL, whereas level of those receiving ART was 26.9 (±9.9) ng/mL (P = .154). There was no statistically significant difference (P >.05) in the prevalence of vitamin D deficiency, insufficiency, and low vitamin D status between the HIV-1-infected patients who were naive or receiving ART.
Baseline Characteristics of 178 HIV-Infected Participants

Abbreviations: BMI, body mass index; HBV, hepatitis B virus; HCV, hepatitis C virus; IQR, interquartile range; ART, antiretroviral therapy; NVP, nevirapine; EFV, efavirenz; PI, protease inhibitor; ZDV, zidovudine; 3TC, lamivudine; d4T, stavudine; TDF, tenofovir; BMD, bone mineral density; SD, standard deviation.
aOnly ART-receiving patients.
bBy Cockcroft-Gault formula.
When the patients were categorized into 2 groups, 126 patients had low vitamin D status and 52 patients had normal vitamin D status. No statistically significant difference (P >.05) with regard to age, gender, body mass index (BMI), CD4 count, duration of known HIV-1 infection, duration of receiving ART, backbone ART regimens, BMD status, creatinine clearance, lipodystrophy, hepatitis coinfection, and behavioral data at the time of enrollment between the 2 groups (Table 1). In univariate analysis, taking efavirenz (EFV)-based regimen, duration of known HIV-1 infection, BMD at lumbar spine, creatinine clearance, and lipodystrophy were the factors that had P <.2 (Table 2). These factors together with the traditional factors associated with vitamin D level (age, gender, and BMI) were considered candidates for the multivariate model to determine the factors associated with low vitamin D status. In multivariate analysis, only taking EFV-based regimen was significantly associated with the occurrence of low vitamin D status (odds ratio 3.60; 95% confidence interval, 1.06-12.15; P = .040; Table 2).
Univariate and Multivariate Analyses of Factors Associated with Low Vitamin D Status

Abbreviations: BMI, body mass index; HBV, hepatitis B virus; HCV, hepatitis C virus; ART, antiretroviral therapy; NVP, nevirapine; EFV, efavirenz; PI, protease inhibitor; ZDV, zidovudine; d4T, stavudine; TDF, tenofovir; BMD, bone mineral density.
aOnly ART-receiving patients.
When we used multiple linear regression model with the same candidate factors as in multiple logistic regression analysis, we found that only taking EFV-based regimen was independently associated with lower levels of 25(OH)D (coefficient = −5.36; standard error 2.19; P = .015; Table 3). The mean (±SD) level of 25(OH)D in patients taking EFV-based regimen was 22.9 (±6.6) ng/mL, while in those not taking EFV-based regimen, it was 28.6 (±10.7) ng/mL (P = .007; Figure 1). There was no correlation between vitamin D level and BMD at lumbar spine and femoral neck (P = .142 and P = .539, respectively.
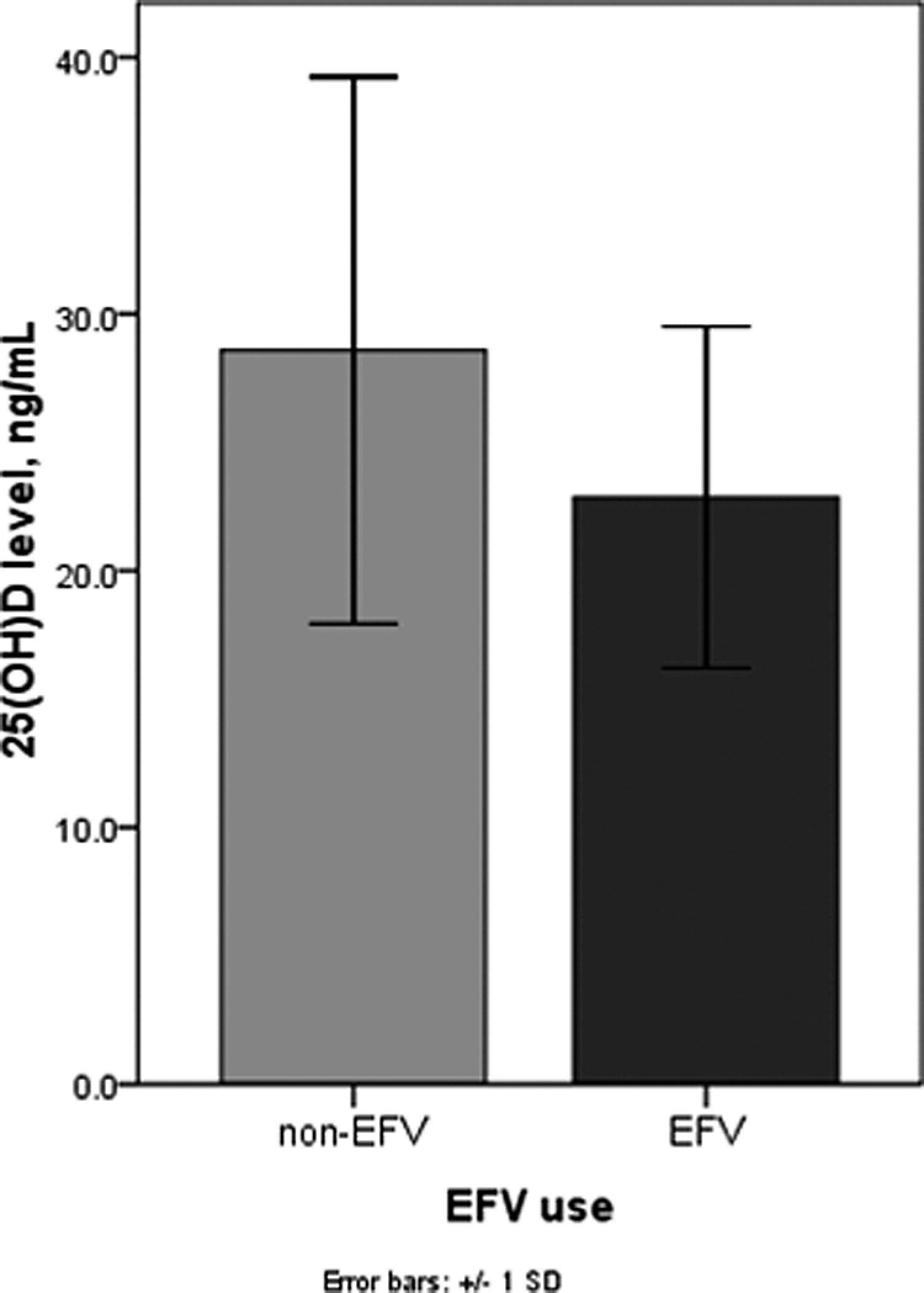
Mean (±standard deviation) level of 25(OH)D between patients taking efavirenz (EFV) and those not taking EFV.
Linear Regression Analysis of Factors Associated with 25(OH)D Levels

Abbreviations: BMD, bone mineral density; EFV, efavirenz.
Discussion
The results from the present study have demonstrated that vitamin D deficiency or insufficiency was highly prevalent among HIV-1-infected adults even in a tropical country such as Thailand. Comparing the general population in Thailand, 24–27 our HIV-1-infected patients had a similar prevalence of vitamin D deficiency or insufficiency. Among our HIV-1-infected patients in the present study, no difference in the prevalence of low vitamin D status was observed between patient naive to ART or receiving ART. In a multivariate analysis, taking EFV-based regimen was found to be the only associated factor of low vitamin D status. In contrast, we did not find an association between taking nevirapine (NVP)-based regimen and low vitamin D status although NVP is also an NNRTI. For protease inhibitor (PI)-based regimen, we observed a lower risk of low vitamin D status only in univariate but not in multivariate analyses. The mean level of 25(OH)D was lower in the patients who took EFV-based regimen as compared to those who were on non-EFV-based regimen.
To our knowledge, the present study is the first report evaluating prevalence and associated factors of low vitamin D status in HIV-1-infected men or women, naive or previously exposed to ART in a tropical setting. We found that the prevalence of vitamin D deficiency or insufficiency in the present study is much higher than a recent report from Brazil 28 but comparable to a study from the United States 21 when using the same definition (25[OH]D <30 ng/mL). A number of studies from European countries have also demonstrated high prevalence of vitamin D deficiency or insufficiency. 16,18,20 These results suggest that inadequate vitamin D status in HIV-1-infected patients is likely to be common regardless of geographic locations or ethnicity. Awareness and monitoring of vitamin D deficiency are warranted when providing long-term care for HIV-1-infected patients.
We found no difference in vitamin D status between HIV-1-infected patients who were naive or exposed to ART. This finding is consistent with studies from Bang et al 18 and Van Den Bout-Van Den Beukel et al. 16 In contrast, some cross-sectional studies have found ART to be associated with lower vitamin D level. 19,21 Efavirenz (EFV) use was found to be the only factor associated with low vitamin D status. It is currently believed that EFV causes lower 25(OH)D by inducing 24 hydroxylase which hydrolyzes 25(OH)D and 1,25(OH)2D to their inactivate form. 29,30 We did not observe this association in NVP users. This finding is consistent with 2 previous reports from Western countries. 19,21 Taken together, this suggests that low vitamin D is not an NNRTI class phenomenon but more likely a specific effect of EFV.
There are some limitations in this study. Due to the cross-sectional nature of the study, we cannot elucidate the causal relationship between HIV-1 infection and vitamin D levels or vice versa. The small number of patients taking PI-based regimen may not have enough statistical power to demonstrate the association of PI use and low vitamin D status. We did not have information on occupation or daily activity related to sun exposure. Since our hospital is located in the middle part of Bangkok, a metropolitan city, our patients can represent tropical HIV-1-infected patients in urban setting.
In conclusion, vitamin D deficiency and insufficiency are highly prevalent among HIV-1-infected patients even in a tropical country such as Thailand. There was no difference in low vitamin D status between patients who were naive or exposed to ART. Use of EFV, which can induce CYP450 enzymes involved in vitamin D metabolism, is significantly associated with low vitamin D status. This suggests that vitamin D status may need to be assessed in HIV-1-infected patients including tropical residents especially when EFV is used. Further studies to define the effect of ART on the metabolism of vitamin D, impact of vitamin D on HIV-1 as well as benefits of vitamin D supplement in HIV-infected patients are needed.
Footnotes
Authors’ Note
Abstract of this study was presented in the Sixth IAS Conference on the HIV Pathogenesis, Treatment, and Prevention, Rome, July 17-20, 2011.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: Research grant of Faculty of Medicine Ramathibodi Hospital, Mahidol University, Bangkok, Thailand.