
Abstract
Objective
Many studies have shown that vitamin D deficiency is associated with insulin resistance and metabolic syndrome. However, few studies have shown independent associations between vitamin D deficiency and the metabolic characteristics of prediabetes. We aimed to evaluate the relationship between serum vitamin D concentration and metabolic risk factors in adults with prediabetes.
Methods
We enrolled 161 patients aged 25 to 75 years in a cross-sectional study and collected clinical and biochemical data, including 25-hydroxyvitamin D (25[OH]D) status and fasting glucose concentration. Vitamin D status was defined as follows: deficiency (25[OH]D <49.9 ng/mL), insufficiency (49.9 to 74.9 nmol/L) or sufficiency (>74.9 nmol/L). Prediabetes was defined using fasting plasma glucose concentrations of 5.55 to 6.49 mmol/L.
Results
The prevalences of vitamin D deficiency and insufficiency were 49.7% and 24.8%, respectively. Participants with vitamin D deficiency had a higher prevalence of prediabetes than those without (53.8% vs. 32.1%), and there was a significant relationship between female sex and vitamin D status (odds ratio: 1.382; 95% confidence interval: 0.335–5.693).
Conclusion
Vitamin D deficiency is more closely associated with a high prevalence of prediabetes in women than in men. Further studies are needed to elucidate the explanation for this association.
Introduction
The link between vitamin D deficiency and the development of metabolic syndrome has been a focus of recent study. Vitamin D has received widespread attention for its numerous non-skeletal effects, such as on pancreatic insulin release and insulin sensitivity. 1 The principal biological role of vitamin D is conventionally thought to be related to bone health, but it may also have important and more general effects on the regulation of metabolism and inflammation. 2 Furthermore, vitamin D deficiency is associated with higher risks of cancer, cardiovascular disease and metabolic syndrome. 3
Many studies have shown that vitamin D deficiency is associated with type 2 diabetes and metabolic syndrome.4,5 Furthermore, vitamin D supplementation may prevent type 2 diabetes or improve insulin release and sensitivity.6,7 However, randomised clinical trials in humans have not generated consistent results regarding the relationship between vitamin D and diabetes.8,9 Although a defect in insulin secretion and insulin resistance are both important in the progression of euglycemia to prediabetes and type 2 diabetes, the role of vitamin D in the development of prediabetes and type 2 diabetes remains unclear. 10
The purposes of the present study were to evaluate the relationships between the serum 25-hydroxyvitamin D [25(OH)D] concentration and metabolic risk factors in adults with prediabetes, and between vitamin D deficiency and sex in adults with prediabetes.
Materials and methods
Participants and study design
We conducted a cross-sectional study between January 2016 and November 2017, in which we consecutively recruited patients aged 25 to 75 years who presented at the hospital with fatigue, dizziness and generalised oedema. The exclusion criteria were as follows: (1) heavy alcohol consumption that would affect the liver or vitamin D status, (2) missing data, and (3) a history of vitamin D supplementation.
The medical history of each participant was obtained from their medical records and the height, body mass and blood pressure of each were measured. Blood samples were collected for the evaluation of fasting glucose concentration, lipid profile, thyroid function, and serum 25(OH)D concentration. Serum 25(OH)D concentration was measured using liquid chromatography-tandem mass spectrometry (LC-MS/MS; PerkinElmer, Waltham, MA, USA). We measured thyroid-stimulating hormone (TSH) concentration using electrochemiluminescence immunoassay (Roche Diagnostics, Mannheim, Germany) and HbA1c using a turbidimetric immunoassay (COBAS Integra 800, Roche, Mannheim, Germany). To evaluate vitamin D status, we used the guidelines of the Endocrine Society, which define vitamin D deficiency using a 25(OH)D concentration of <49.9 nmol/L, vitamin D insufficiency using a 25(OH)D concentration between 49.9 and 74.9 nmol/L, and vitamin D sufficiency using a 25(OH)D concentration of >74.9 nmol/L. 11
On the basis of the criteria of the American Diabetes Association, we defined prediabetes using a fasting plasma glucose concentration of >5.55 mmol/L and <6.99 mmol/L. 12 The International Diabetes Federation criteria were used to define hypertension and dyslipidaemia. 13 Hypertension was defined using a systolic blood pressure ≥130 mmHg, diastolic blood pressure ≥85 mmHg or the ongoing treatment of previously diagnosed hypertension. Obesity was defined as a large waist circumference (≥90 cm in men and ≥80 cm in women). Dyslipidaemia was defined as hypertriglyceridaemia (triglyceride concentration >1.69 mmol/L), low high-density lipoprotein-cholesterol concentration (HDL-C; <1.03 mmol/L) or the ongoing treatment of previously diagnosed dyslipidaemia.
In clinical practice, adiposity is assessed using body mass index (BMI). Adult obesity is defined using a BMI ≥25 kg/m2 in Eastern populations, 14 and this definition was used in the present study.
TSH concentration was categorised as follows: hyperthyroidism, TSH <0.35 µIU/mL; euthyroidism, TSH 0.35 to 5.50 µIU/mL; and hypothyroidism, TSH >5.50 µIU/mL.
We defined non-alcoholic fatty liver disease (NAFLD) using the identification of hepatic steatosis by two well-trained radiologists.
Clinical and laboratory measurements
Height and body mass were measured with shoes removed. To determine vitamin D status, we measured serum 25(OH)D concentration using liquid chromatography-tandem mass spectrometry (LC-MS/MS), which is considered the gold-standard method, as previously described. 15 The participants were allocated to a deficiency [25(OH)D <49.9 nmol/L], insufficiency (49.9 to 74.9 nmol/L) or sufficiency (>74.9 nmol/L) group.
NAFLD was diagnosed using abdominal ultrasonography when liver parenchymal brightness and high liver-to-kidney contrast were identified.
Statistical analysis
Statistical analysis was performed using SPSS version 18.0 (SPSS Inc, Chicago, IL, USA). The baseline characteristics of the groups are presented using percentages. Differences between categorical data were identified using the chi-squared or Fisher’s exact test, as appropriate. P ≤ 0.05 was accepted as indicating statistical significance. After adjustment for age and other confounding factors, multiple linear regression analysis was used to evaluate the relationship between serum 25(OH)D concentration and metabolic risk factors in the participants with prediabetes.
Ethics
The study was performed according to the principles of the Declaration of Helsinki. The study protocol was reviewed and received an exemption from the need for approval by the institutional review board, because of its retrospective nature. We obtained the written informed consent of all the study participants. We have de-identified all the participants’ details. The reporting of this study conforms to the Strengthening the Reporting of Observational Studies in Epidemiology (STROBE) statement.
We confirm that fellow researchers may reproduce our methodology from the description provided.
Results
After applying the exclusion criteria, data from 161 out of 203 patients were analysed. Table 1 shows the characteristics of the participants, categorised according to vitamin D concentration. Their mean age was 51.2 years (SD 10.14) and 88.2% (n = 142) were women. The prevalences of vitamin D deficiency and insufficiency were 49.7% and 24.8%, respectively. The majority (74.5%) had a serum 25(OH)D concentration <74.9 nmol/L and approximately half of the participants were considered to be vitamin D-deficient (<49.9 nmol/L).
Characteristics of the participants, categorised according to vitamin D status.
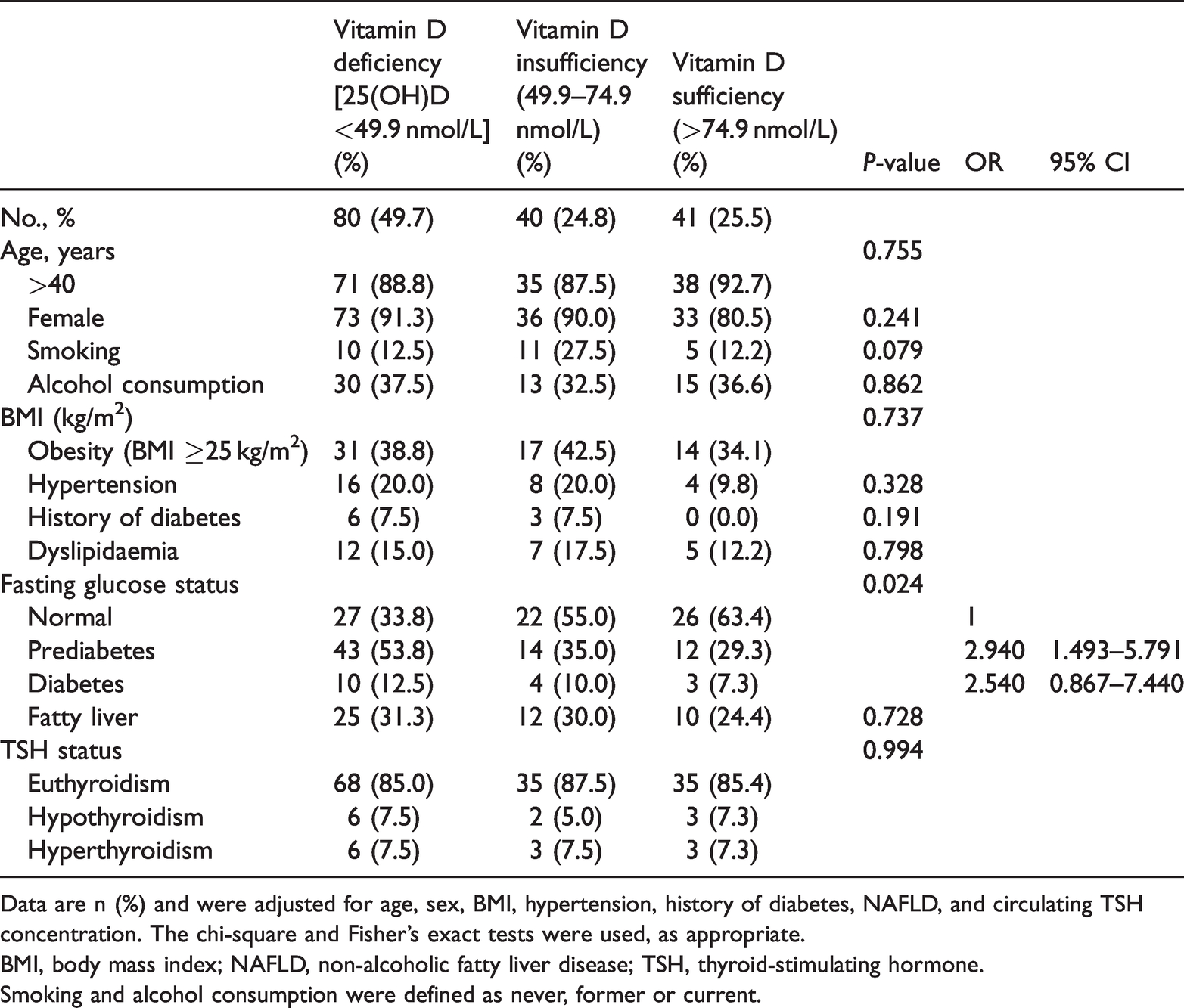
Data are n (%) and were adjusted for age, sex, BMI, hypertension, history of diabetes, NAFLD, and circulating TSH concentration. The chi-square and Fisher’s exact tests were used, as appropriate.
BMI, body mass index; NAFLD, non-alcoholic fatty liver disease; TSH, thyroid-stimulating hormone.
Smoking and alcohol consumption were defined as never, former or current.
Multiple linear regression analysis was performed to identify parameters that were independently associated with prediabetes. After adjustment for age, sex, BMI, hypertension, a history of diabetes, NAFLD, and the TSH concentration, the odds ratio (OR) for the relationship between vitamin D deficiency and prediabetes was 2.940 (95% confidence interval [CI]: 1.493 to 5.791; P = 0.024). Therefore, a larger proportion of participants with prediabetes were in the vitamin D deficiency group than in the other groups. In the participants with a history of diabetes, the mean haemoglobin A1c was 7.83%, and none of these participants were in the vitamin D sufficiency group, but there was no significant difference in HbA1c between the vitamin D deficiency and sufficiency groups. Furthermore, there were no differences in the prevalences of obesity, NAFLD or thyroid dysfunction among the groups.
Table 2 shows the characteristics of the participants with prediabetes, categorised according to their vitamin D concentration. Of the 69 participants with prediabetes, 9 were men and 60 were women, and the majority (92.8%) were aged ≥40 years. Women were significantly more likely to have poor vitamin D status (OR: 1.382; 95% CI: 0.335 to 5.693; P=0.035). However, hypertension and dyslipidaemia were not associated with vitamin D status. In addition, there were no differences in the prevalences of obesity, NAFLD or thyroid dysfunction between these groups.
Characteristics of the participants with prediabetes, categorised according to vitamin D status.

Data are n (%). P-values were derived from multiple linear regression analysis.
BMI, body mass index; NAFLD, non-alcoholic fatty liver disease; TSH, thyroid-stimulating hormone.
Discussion
The prevalences of type 2 diabetes and prediabetes have increased significantly worldwide in recent years.16,17 Prediabetes is defined by the presence of insulin resistance and impaired insulin secretion, and can eventually lead to the development of type 2 diabetes. Research interest in the role of vitamin D in prediabetes and type 2 diabetes has been growing. However, few studies have evaluated the relationships between serum vitamin D concentration and metabolic risk factors in adults with prediabetes. In the present study, we found that vitamin D deficiency is associated with prediabetes, and is more prevalent in women.
Because many previous studies have shown that vitamin D deficiency is associated with autoimmune thyroid disease, we might presume that it would also be associated with thyroid dysfunction. However, in the present cross-sectional study, the 25(OH)D concentration was not associated with thyroid function. Although vitamin D may modulate the immune response in the thyroid, there have been few studies of this relationship. 18 Therefore, further randomised controlled trials are needed to investigate the relationship between vitamin D deficiency and the pathogenesis of thyroid dysfunction.
In the present study, we have shown that vitamin D deficiency is associated with a high prevalence of prediabetes, which implies that vitamin D deficiency may be involved in the development of prediabetes. Because prediabetes can progress to diabetes, it is a critical phase of the pathogenesis. 19 Several previous studies have shown that impaired insulin secretion is associated with vitamin D deficiency,20,21 and the results of another study have suggested that vitamin D supplementation could improve insulin secretion. 22 Therefore, a low serum 25(OH)D concentration may be present before the onset of diabetes.
The role of vitamin D in insulin signalling has been debated. Previous studies have shown that pancreatic vitamin D receptors bind circulating vitamin D, 23 and that vitamin D regulates insulin secretion, calcium flux within β cells, and β-cell survival. Furthermore, vitamin D deficiency has been shown to impair insulin secretion in pancreatic β cells, while vitamin D supplementation restores secretion. 24 Furthermore, vitamin D increases the expression of the insulin receptor, thereby increasing insulin sensitivity and glucose uptake. Therefore, vitamin D deficiency may result in insulin resistance, leading to the development of prediabetes 25 . Other studies have shown an inverse association between serum 25(OH)D concentration and the prevalence of diabetes, and that vitamin D deficiency is a biomarker of diabetes risk. 26
We also identified an inverse relationship between the serum concentration of 25(OH)D and female sex in the participants with prediabetes. Poor vitamin D status in Korean women may be the result of low exposure to sunshine, a lack of dietary supplementation and/or low circulating oestrogen concentration. Exposure to sunlight plays an important role in vitamin D production. 3 Although Korea is a country with ample sunshine, most women tend to limit their exposure to sunlight by using sunblock or maintaining an indoor lifestyle. Furthermore, the consumption of fortified food and vitamin D supplements is low.27,28 Although daily supplementation with 1000 IU of vitamin D for 3 to 4 months is needed to increase serum 25(OH)D concentration by 25 nmol/L, it is difficult to achieve vitamin D sufficiency for various reasons, one of which is insufficient circulating oestrogen. In the present study, the majority of participants with prediabetes were women of >40 years of age. This finding is consistent with those of previous studies that have shown a significant association between low circulating oestrogen concentration and vitamin D deficiency.29,30 Oestrogen is the primary female sex hormone and is associated with the biosynthesis of vitamin D. Specifically, it increases vitamin D 25-hydroxylase activity in the liver and increases the circulating concentration of vitamin D-binding protein.31,32
There were several limitations to the present study. First, it had a cross-sectional design; therefore, several parameters affected vitamin D status. Therefore, a prospective study should be conducted to confirm the findings. Second, the study sample was relatively small and the majority of the enrolled patients were women. Approximately 80% of women in Korea are vitamin D-deficient. 33 For this reason, we cannot generalise our results to populations of other ethnicities, and therefore large prospective studies in other localities are needed to confirm the findings. Third, the consumption of fortified foods and vitamin D supplements increases the serum 25(OH)D concentration. 34 In addition, sunlight exposure is lower in winter than in other seasons in Korea. 35 However, we did not quantify the dietary intake of vitamin D or the seasonal variation in serum 25(OH)D concentration. Finally, we diagnosed diabetes using the fasting glucose concentration, rather than using haemoglobin A1c (HbA1c). The HbA1c level reflects the mean blood glucose concentration over the preceding 3 months, whereas the fasting blood glucose concentration is quite variable. 36 However, despite its limitations, this study has demonstrated associations between vitamin D status and metabolic risk factors in individuals with prediabetes.
In conclusion, many previous studies have shown that vitamin D deficiency is associated with several diseases, as well as metabolic syndrome. We aimed to identify factors related to vitamin D deficiency, and found that vitamin D deficiency is associated with a high prevalence of prediabetes in women. However, the reason for this relationship is not clear; therefore, further studies are needed to elucidate the explanation for this association.
Supplemental Material
sj-pdf-1-imr-10.1177_03000605211033384 - Supplemental material for A high prevalence of prediabetes and vitamin D deficiency are more closely associated in women: results of a cross-sectional study
Supplemental material, sj-pdf-1-imr-10.1177_03000605211033384 for A high prevalence of prediabetes and vitamin D deficiency are more closely associated in women: results of a cross-sectional study by Jeonghun Lee, Young Joo Lee and Youngsun Kim in Journal of International Medical Research
Supplemental Material
sj-pdf-2-imr-10.1177_03000605211033384 - Supplemental material for A high prevalence of prediabetes and vitamin D deficiency are more closely associated in women: results of a cross-sectional study
Supplemental material, sj-pdf-2-imr-10.1177_03000605211033384 for A high prevalence of prediabetes and vitamin D deficiency are more closely associated in women: results of a cross-sectional study by Jeonghun Lee, Young Joo Lee and Youngsun Kim in Journal of International Medical Research
Supplemental Material
sj-pdf-3-imr-10.1177_03000605211033384 - Supplemental material for A high prevalence of prediabetes and vitamin D deficiency are more closely associated in women: results of a cross-sectional study
Supplemental material, sj-pdf-3-imr-10.1177_03000605211033384 for A high prevalence of prediabetes and vitamin D deficiency are more closely associated in women: results of a cross-sectional study by Jeonghun Lee, Young Joo Lee and Youngsun Kim in Journal of International Medical Research
Footnotes
Declaration of conflicting interest
The authors declare that there is no conflict of interest.
Funding
This research received no specific grant from any funding agency in the public, commercial, or not-for-profit sectors.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.