
Abstract
The objectives of the present study were to evaluate depressive symptoms and coping strategy among HIV-positive women and men. This cross-sectional study was done among 164 newly diagnosed HIV-positive people through a structured questionnaire. Beck Depression Inventory (BDI) scale was used to measure depression. A 16-items coping scale, Coping with AIDS - Fleishman (CWAF) Instrument, was used to assess coping strategy. χ2 test was used to compare proportions. Men had significantly higher mean BDI somatic score. Odds for being depressed were 3.6 times higher among men (P value .001, 95% C.I. 1.64-8.07). Analysis of the coping strategies showed that women had better coping skill. Significant correlation was observed between BDI score and emotion-focused coping score (correlation coefficient −0.258, P value .01). HIV-positive men had more depression. Gender-sensitive strategies needed to provide better care for them.
Keywords
Introduction
HIV infection and AIDS have become a global pandemic posing one of the greatest challenges to global public health. Since its identification in 1981, the HIV/AIDS pandemic has already left millions of children orphaned, has disrupted community life, and has taken a heavy toll on socioeconomic and family structures.
The new 2006 estimates released by the National AIDS Control Organization (NACO), supported by Joint United Nations Programme on HIV/AIDS (UNAIDS) and World Health Organization (WHO), indicate that national adult HIV prevalence in India is approximately 0.36%, which corresponds to an estimated 2 million to 3.1 million people living with HIV in the country. 1 Like many other developing countries, HIV/AIDS has brought new dimensions to some of the already existing complex health issues threatening India.
Acute negative events (eg hospitalization) or persistent adverse circumstances (eg, chronic illness) are related to psychological distress. During past few years, there has been considerable work in the fields of health psychology and psychiatry attempting to explain the variety of individual responses to stresses of illness and to account for these interindividual differences. The concepts of stress, personality types, coping strategies, and defence mechanism can be integrated into a framework that illustrates the complexity of an individual’s behavioral or emotional responses to illness. In any chronic illness, challenges are ongoing and become a part of daily life for the individual.
HIV infection raises the threat of major negative life events and chronic medical conditions. As new technologies extend the lives of people living with HIV/AIDS—it has now become a chronic manageable disease—the survivors have to suffer a great deal of ongoing stress that give rise to affective and behavioural changes. Reported coping responses are defined in terms of actions on cognitions, which the individual employs to address stressful events or problems. AIDS-related grief creates significant mental health needs among people living with HIV/AIDS (PLWHA). This appears to persist even in the context of advances in medical treatment. Coping interventions are needed to reduce psychological distress among PLWHA. 2 The coping strategy differs among patients. Problems in coping with illness have been shown to be a frequent reason for psychiatric consultation. The relationship between coping behaviors and affective responses (eg, depression) among the HIV population is very much crucial to understand the disease dynamics and impact of care and support program. Although depressive symptoms are common in people living with HIV/AIDS, their reported prevalence varies greatly across HIV-positive populations, ranging from 21% to 97%. 3
India is a country of diversity in ethnic origin, social customs, languages, etc. There is very limited research in India to understand correlation of coping strategy and depression among HIV/AIDS population and especially in women. Studies of coping strategy and depression among HIV-positive women may enable a wider scope in the analysis of impact of sickness and complex therapeutic strategies used, permitting us to evaluate which dimension of partner’s life are most affected and to establish association with different clinical, therapeutic, and psychosocial factors. This information may help the policy makers to implement effective preventive and control strategies to combat this epidemic.
Aims and Objectives
The objective of the present study was to evaluate depressive symptoms and coping strategy among HIV-positive men and women in clinical care. An attempt was also made to get the answers of the questions that whether there are any important differences in the coping skills among HIV-positive women as compared to HIV-positive men as well as what may be the characteristics associated with the likelihood of depression among HIV population. The importance of the sociodemographic characteristics in coping skill among HIV-positive population was also searched in the present study.
Materials and Methods
Study Design
This was a cross-sectional (group comparison) study comparing prevalence of depression and coping strategy between HIV-positive women and men in Kolkata, India. Prevalence of depression and coping strategy were explored through a structured questionnaire interview process. The study was conducted at out patients department for HIV-positive people in an HIV clinic of a tertiary government hospital of Kolkata, India. The study was conducted during the year of 2008-2009. Ethical committee of that institution approved the study.
Study Populations
The inclusion criteria for recruiting participants in the present study were recently diagnosed HIV-positive cases (within 2 months), aged between 18 and 50 years, and able to understand Bengali. Indoor admitted cases were excluded with the assumption that they would be depressed and not in a position to recall their status when they were diagnosed as HIV cases. It has been documented from studies that cancer is a predictor of depression so, to avoid confounding, we excluded HIV-positive cases having coexistence of cancer. Similarly, past history of psychiatric illness might also influence the depression severity and were also excluded.
Sample Size and Scheme
Consecutive 85 positive women and positive men were recruited for the study, but 1 woman and 3 men could not complete the whole study procedure. Finally, research work was done among 84 HIV-positive women and 82 HIV-positive men.
Data Sources and Collection
A questionnaire was developed in local language, which was a structured, close-ended, instrument meant to be administered in a face-to-face interview. The questionnaire was intended to capture information on 4 major aspects such as (a) participants' socioeconomic and demographic characteristics, (b) mode of transmission, WHO HIV staging, treatment information of the individuals, (c) their coping strategies, and (d) depression level. Questionnaire was pilot-tested and validated before using at this study.
Depression was diagnosed according to Diagnostic and Statistical Manual of Mental Disorders (Fourth Edition; DSM IV) criteria. 4 Beck Depression Inventory (BDI) scale 5 was used in this study to measure depressive symptoms, because BDI scale is a self-reporting instrument. The strength of BDI includes its brevity and lack of clinician/staff time required for administration. Beck Depression Inventory contain 14 cognitive/affective items and 7 somatic items. Individuals are asked to rate themselves on a 0 to 3 spectrum (0 = least, 3 = most) with a score rage of 0 to 63, total score is a sum of all items. Grouping of coping responses vary in applied research; however, several investigations have employed 3 broad categorizations, active (or approach) coping, avoidant coping (disengagement, avoidance, denial), and support coping (seeking on utilizing support measures). A set of 16 items coping scale, Coping with AIDS - Fleishman (CWAF) Instrument, 6 with dichotomous responses were used to assess coping strategy. Coping was measured by having respondents indicate how they reacted in the month after they first learned that they were infected with HIV. This 16-items scale was first used by John A. Fleishman, Barry Fogel in their study. 7 They selected these 16 items from items developed in prior studies by Folkman et al. 8 Later, this scale was used by other investigators to address coping strategy in different scenario.2,9–12 Coping strategies were assessed in 2 methods; firstly, according to Folkman and Lazarus, 13 which comprises “Problem” and “Emotion” focused coping dimensions and the other is according to Fleishman JA and Fogel B, 7 which includes “Positive coping,” “Avoidance coping,” and “Seeking social support.” This 16-items scale were translated in Bengali and validated before administering in our study population.
Data Management
All collected data were double-entered into Microsoft Excel spreadsheet and subsequently analyzed by SAS program. Before analysis, data were cleaned using validity and consistency checks.
Data Analysis
Analyses were conducted with the SAS program (SAS version 9.1.1, SAS Institute Inc. Cary, North Carolina). Descriptive analyses of all variables were done, using proportions and means where applicable. Then the association of important sociodemographic factors with depression and coping status were explored. A χ2 test was used to compare proportions that were considered significant if the P value was less than .05. Finally, logistic regression analyses were performed to detect predictors of depression.
Ethics
This study was approved by Ethical Committee of Medical College Kolkata.
Results
Majority of the study participants (53.6% of women and 63.4% of men) were from the rural areas. The mean age of the study population was lesser in positive women, 29.4 years (SD 6.1) in comparison to 35 years (SD 6.9) in positive men, but the difference was not statistically significant (P > .05). The mean income of the family, in cases of positive women, was Rs 2211 (minimum Rs 2014 and maximum Rs 12 000); in cases of positive men was Rs 2776 (minimum Rs 600 and maximum Rs 12 000). The average number of family members was 4 in the positive women group and 3 among the positive men. The other relevant sociodemographic criteria are shown in Table 1 , which is comparable between the men and women. Among the participants, 95.2% of women and 94% of men had acquired the HIV infection via sexual transmission.
Sociodemographic Characteristics of the Study Population

Figure 1 shows the comparison of the WHO HIV staging of positive men and women, which clearly depicts that most of the recruited women were in Stage 2 of the infection, whereas, men were mostly in the Stage 4 of the disease. Opportunistic infection was present in 46.4% of positive women and 74.4% of positive men. Among the participants, 27 (32.1%) women and 49 (59.8%) men were receiving antiretroviral therapy (ART). The mean CD4 count (cells/mm3) was 375 in positive women (min 19, max 912) and 163 in men (min 17, max 780).
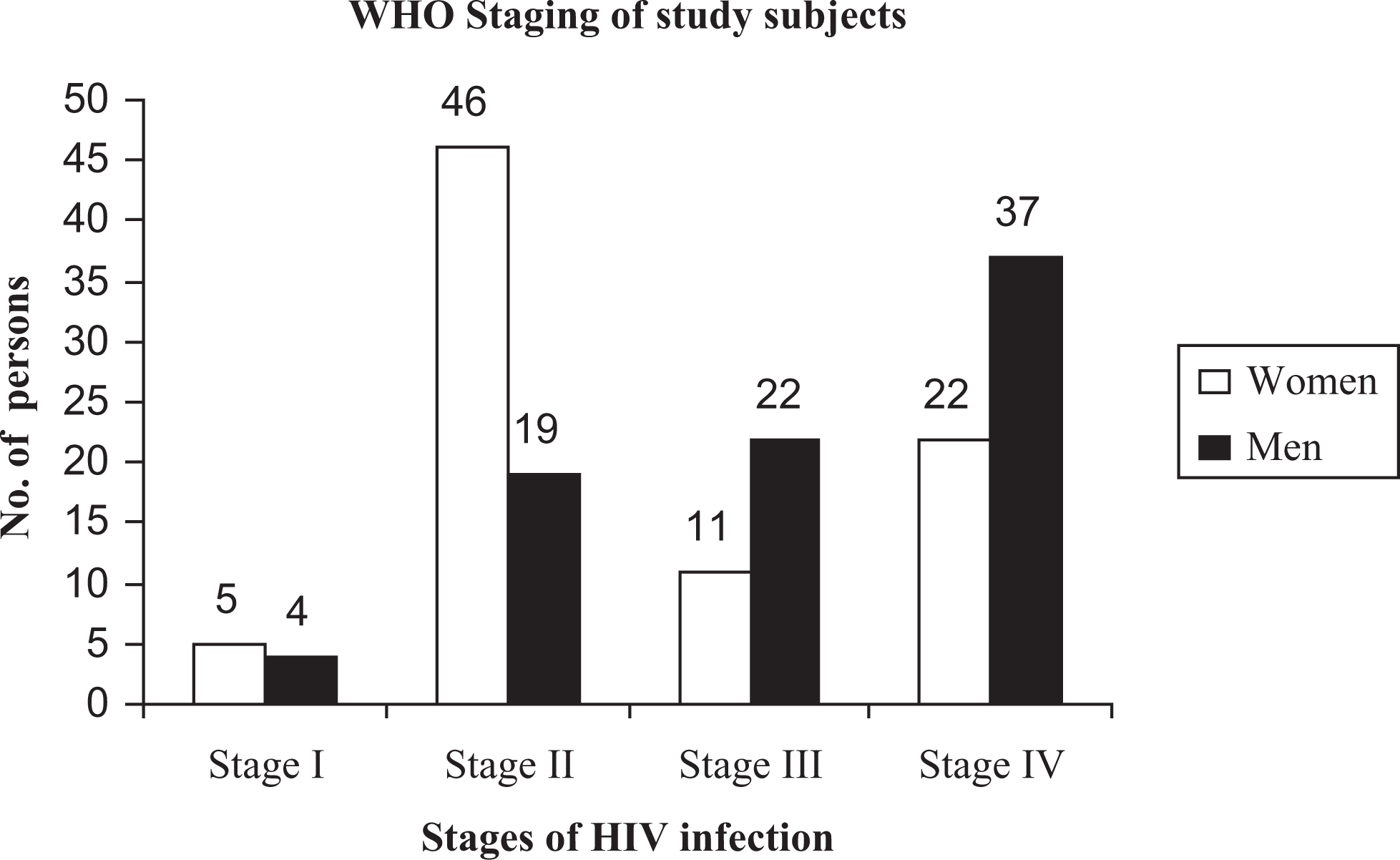
World Health Organization (WHO) staging of the study participants.
Mean score of 7 of BDI items namely “sadness,” “discouraged about future,” “dissatisfaction,” “crying,” “loss of interest in people,” “difficulty with decisions,” and “libido” were higher in women than men in this study, but none was statistically significant. But there were significant higher mean score in 5 items of the rest 14 items while comparing item-wise mean scores of BDI between positive women and men, as shown in Table 2 .
Comparison of Mean Scores of Beck Depression Inventory (BDI) Items

Figure 2 depicts the comparison of depression among positive women and men. Here, BDI score ≥14 is noted as depression; it is found that 50 positive women (59.5%) and 69 positive men (84.1%) are found to have depression. Odds for being depressed were 3.6 times higher among men comparing to women, which was found to be statistically significant (P value .001, 95% CI 1.64-8.07). Mean BDU score of men (24) were higher than women (21.3), but that was not statistically significant (P = .26). On further analysis, it was revealed that men had significantly higher mean BDI somatic score than women (men—13.1 and women—9.6). It was also observed that mean BDI cognitive score of women (11.7) was higher than that of men (10.9) but not statistically significant. The coping strategies are compared in Table 3 in 2 ways. Both analyses showed that women had better coping skills. Women can significantly cope with problem. Women had also more positive coping skills.

Comparison of depression among HIV-positive women and men.
Comparison of Coping Strategy Between Women and Men

Significant correlation was observed between BDI score and emotion-focused coping score. Correlation coefficient was −0.258. (Negative coefficient because emotional scoring were calculated in reverse way that is those who cannot cope would get higher scoring). P value for this correlation was .01. It suggested that those who cannot cope up emotional factors suffered from depression.
Discussion
The socioeconomic and HIV-infection-related parameters of positive men and women are more or less comparable in our study, but it is to be noted that most of the women recruited for the study was in Stage 2 of the disease, where as, men were mostly in the Stage 4. Male persons attended the clinic when they become ill, but women were diagnosed as a part of spouse screening procedure adopted in our clinic.
This study revealed depression is widely prevalent in both groups and more than two-third men were depressed while diagnosed as HIV positive. Studies in other countries also showed prevalence of depression varying from 20% to 60%. A study 14 with 297 PLWHA showed that depression was widespread (54.2%) and largely unrelated to demographic characteristics, but associated with diminished health status, health-related quality-of-life, and coping strategies.
Results of our study showed that HIV-positive women have more positive coping, that is, problem-focused coping, and they are seeking more social support. Study findings suggested that there is statistically significant problem-focused coping in HIV-positive women. Emotion-focused coping showed no statistically significant difference between men and women. However, finding of the study is not consistent with others.14–17 Other studies showed that gender distinctions in AIDS-related bereavement currently exists as evidenced by HIV-positive women exhibiting more distress on several grief dimension when compared to men. Bereaved women have unresolved grief, increased risk for generalized anxiety, and overall depressed anxious mood symptomatology than their male counterparts. Women scored significantly worse than men on depression. Here, men were more depressed than women.
The instruments used are self rated by the concerned participants, but score obtained from the individual is expected to be reliable. Both these instruments met psychometric requirement of having study reliability as measured by interrater reliability, test–retest reliability during the process of validation of these instruments in local language. The choice of an appropriate coping response to stressors is believed to involve consideration of the level of resources available. Empirical investigations have shown that individuals with higher levels of perceived control are more likely to engage in problem-focussed or active-coping responses. Further, in some investigations, perceived control has been related to effectiveness of coping responses in ameliorating distress. After controlling resources, different coping responses may be associated with different psychological outcomes.
There may be a few explanations why this study result differs significantly from other study conducted among HIV-positive people. Our sociocultural norms and aspect are different from western developed countries. In our country, most of the HIV transmission is heterosexual in nature and women in almost all cases contract their disease from men (mostly from their husband). In BDI score, men showed higher “feeling guilty” and “being punished” than women. In these 2 items of cognitive affective subscale, P value is significant between men and women. In our sociocultural setup, men are dominant members of the family and in most case the only earning member of the family. His wife, children, and in few cases old parents are totally dependant on him. In this setup, when men contracts the disease like HIV—which has no cure—the family structure is broken, there is financial crisis and hopes are shattered. This affects the male patient to a severe degree. He has to endure everything helplessly—coming to the hospital, taking medicines, becoming jobless, seeing his sweet home shattered, family being socially ostracized. He becomes dependant on others for his family. Loss of employment or closure of business is really devastating to a man who was in full swing even a few months back. Being jobless or failing in business after contracting the illness create a mental agony among men as they are the sole earning member in most of the families. As stigma and discrimination is prevailing with HIV/AIDS, it is difficult for the men to disclose his sero-positive status to others as he is the source of spreading the disease to his family. Greater substance abuse especially alcohol and cannabis may be another predictor of depression in male as significant number of male were abusing substance for a long period of time. In contrast, substance abuse is very negligible among women participants.
HIV-infected persons generally shows avoidant coping (escape avoidant, self blame, confrontation, distancing) instead of active coping (problem solving, seeking social support, accepting responsibility, positive reappraisal). Avoidant coping is associated with greater depression, anxiety, maladjustment to HIV. Coping strategy is a strong predictor of greater AIDS-related grief reaction and psychological distress including depressive symptoms. The 16-item coping scale shows significant relation with depressive symptoms. In longitudinal study, positive coping is related to reduction in depressive symptoms.
To our knowledge, this was the first study in India comparing a group of women with positive men at clinical setup. Because of inherent limitations of retrospective self-report assessments, reporting bias could have occurred in this study. Other limitation of this study include the recruitment of a convenience sample with possible limits to generalizability of the findings and also other stressful life events, and related coping strategies past or present were not assessed or accounted for in this study. In addition, inherent to the cross-sectional nature of the study, it is expected to have certain limitations regarding reliability and validity of the study like selection bias, measurement error. To minimize this error, experienced interviewers were engaged and rechecking of responses was followed before completion of individual interview procedure.
Despite the problems and limitations as mentioned above, the study generated adequate relevant information as discussed. This study indicated that low status in society and family, and economic and social barriers such as poverty are some of the primary issues that facilitate a woman coping with the disease process. Less coping skill of men might adversely affect in ART adherence and increasing psychiatric morbidity.
Further study on depression and coping strategies throughout all classes of Indian society is important, to ensure proper attention of multiple social barriers. Also, increased dissemination of research results throughout global community is important, to ensure that severity of current problem is acknowledged and remains a global priority.
Conclusion
The present study has turned up evidence that sero-positive men have more depression than sero-positive women in our society. This calls for further investigation of gender differentials with a view to mounting gender-sensitive strategies aimed at providing better care for the men. The results of this study could help making appropriate and rational policies and developing effective intervention and prevention.
Footnotes
This work has been attributed to Medical College Kolkata, India.
Acknowledgement
We acknowledge support of Dr SK Guha, Dr Prathama Guha, and Mrs Soma Roy Chowdhury for data collection and manuscript preparation.
The author(s) declared no conflicts of interest with respect to the authorship and/or publication of this article.
The author(s) received no financial support for the research and/or authorship of this article.