
Abstract
To determine the socioeconomic impacts among HIV-infected persons in Sudan and examine whether there are significant variations in coping strategies between infected men and women, a primary survey was conducted among infected persons (n = 555). Discriminant function was used to analyze the data. We found significant variation in the coping strategies (<.001). HIV/AIDS impacts were more critical for women. Infected people have 3 alternatives in coping with the changes in their income and expenditure, that is, borrow, utilize savings, or sell assets. Policy makers should consider economic information in planning health care to mitigate the impacts and remove the gender gap.
Introduction
Coping is defined as handling risk, which is not equally distributed and where people are not equally able to access resources. It is created by individuals from different socioeconomic segments of the society through complex processes of economic, social, and cultural conditions. Livelihood coping strategies are said to be the sum of all the various activities carried out by people in generating income for their livelihood. 1 Deprived households are often the worst strike and more exposed to the long drawn out effects and invisible burden of HIV/AIDS. 2 This results in various coping strategies to cushion the impact of the epidemic. 3 HIV/AIDS is a problem with deep economic roots and potentially serious economic implications. As illustrated by a previous study in Nigeria, 4 significant losses to households and government in terms of income and direct medical care cost were seen. These findings were consistent with other studies from the Canadian AIDS Society, 5,6 which postulated that the major coping strategies faced by people living with HIV/AIDS (PLHIV) included borrowing, sale of assets, and utilization of savings to cope with the out-of-pocket expenditure following HIV infection. Masanjala 7 showed that HIV/AIDS forced households to use their savings, borrow, and engage in debt crisis. Additionally several studies in South Africa have found significant impact of HIV/AIDS on mortality and life expectancy. 3,8,9
In addition, HIV/AIDS affects both the supply and demand for education. For instance, a study in the Central African Republic, about 85% of teachers’ deaths were due to HIV/AIDS, while the corresponding percentage was 70% in Cote d’Ivoire. 10 On the demand side, a survey in South Africa by Oni et al 11 reported that households with HIV/AIDS-infected individuals reduced their spending on education by 7.3%.
HIV/AIDS carries with it huge stigma and discrimination. In Sudan, testing positive for HIV is a death sentence. Older parents of AIDS sufferers are sometimes too frightened of the reaction of their neighbors to disclose that their children are sick or dead due to HIV/AIDS. 12 People living with HIV/AIDS face huge stigma and discrimination, mainly in employment and access to health care and treatment services, which are considered major factors hindering effort for scaling up treatment services. 13,14
Several studies argued that women were rejected by their families because of their HIV status; they have the risk of losing all claims to family assets, facing the burdens of blame and shame. This makes their situation in the society worse than that of men. 15,16
Sudan is a low-income country in the north of Africa with a total population estimated at approximately 35 million. 17 The country’s political instability and internal conflict have increased the level of poverty and deprivation, 18 with the prevalence of poverty at 46%. 19 The first case of AIDS in Sudan was reported in 1986 and since then the number of cases reported annually has increased to a total of 15 000 by the end of 2013. 20 It has been a cause for concern that the number of reported cases do not reflect the real situation of the HIV/AIDS epidemic in Sudan, and a large gap existed between these figures and the estimates provided by Joint United Nations Programme on HIV/AIDS of 49 000 cases of HIV infection. 21 From a comprehensive epidemiological and behavioral review of the HIV and AIDS situation in Sudan, 19 the overall HIV prevalence was estimated at 0.0.2%. The total people living with HIV in 2014 were estimated at 4600 children and 45 000 adults and 3100 deaths.
Objective and Rational for the Study
The medical consequences of HIV infection on the individual and the subsequent interventions including treatment that can mitigate the negative consequences are well studied and understood. 22 However, the socioeconomic impact of being infected with HIV on the individual as well as on his or her family and community is less well studied and understood. Thus, the general objective of this study is to illustrate the socioeconomic impact following HIV infection on PLHIV in Sudan and to what extent it worsens the poverty levels in the country. The specific objectives were to determine the coping strategies among PLHIV and to examine if there is a variation in coping strategies between men and women affected by the disease.
Methods
Research Design
This study builds upon the sustainable livelihood theory to illustrate the impact of HIV/AIDS among PLHIV in Sudan. The utility of the livelihood framework lies in its ability to generate analysis that has positive policy implications. 23 This article adapted the 2-dimensional matrix depicting the possible mix of livelihood strategies open to a rural household in Africa. 7 The framework illustrates the processes of economic change which involves transition between states of economic structure through changes in livelihood strategies. The framework describes the loss of resources in coping with the sickness. This article attempts to illustrate how HIV/AIDS assumes to deplete the household resources and deepen poverty.
The study used quantitative approach to investigate the patterns of survival and living among PLHIV in Sudan. A primary survey was conducted among PLHIV in Sudan between May and September 2011. A structured questionnaire was designed in English and translated to Arabic (the mother tongue of Sudan). The questionnaire included questions on socioeconomic characteristics and status, survival, and coping strategies. In order to protect the privacy and confidentiality of information of the respondents in the survey, their names were not recorded. Thus, the respondents had choice to answer the questions without being subjected to pressure or community norms or expectations.
To generate effective questions, both open- and close-ended questions were used following the recommendations made by Hatch. 24 The questions required personal responses from the respondents.
Pretesting of the Questionnaire
A pilot survey was carried out to test the research instrument, after consultation with the supervisors and the Sudan National AIDS Control Programme authorities. The pilot survey was carried out at the Omdurman Teaching Hospital in Khartoum State mainly at the voluntary counseling and testing and antiretroviral treatment (VCT/ART center). This center was selected, as here a large number of PLHIV come for counseling sessions, treatment, or testing CD4 and viral loads. The pretest for the present study was conducted among a group of 15 PLHIV, which included both male and female individuals.
As a result of the interviews and from the analysis of the findings, several changes were made to the main questionnaire. New questions were developed to replace those where the results from the pretest were not consistent with the theories that explain the study. It was observed that respondents felt comfortable if questions began with the general demographic and economic topics and the transmission topics highlighted later. They also felt at ease in responding to questions in the early morning hours. Hence, it was necessary for most of the interviews to be conducted in the mornings.
Sample Size, Population, and Study Area
The sample size comprised 555 PLHIV. The researcher followed the same method used in health studies. 25 The sample size was calculated according to a formula (n = Z 2 P(1 − P)/d 2), which was used to reflect the certain desired margin of error in the results based on the estimation of the prevalence of HIV in Sudan. Respondents were randomly selected from HIV-infected patients during their regular visits to the VCT/ART centers in Khartoum state (Bashaier, Omdorman, Alban Jadeed, and East Nile centers). Additionally respondents were from VCT/ARTs from Eastern states (Red Sea, Kassala, and Gedarif states) and 2 Western states (South Darfur, West Darfur) and Blue Nile. The study areas were selected due to the high prevalence of HIV (Sudan National Strategic Plan 2010-2014). To be eligible for participation in the survey, respondents were aged 18 years and over and affected by HIV for at least 1 year.
Probability proportional to size was used to select the proper sample from each VCT/ART center within each state targeted in this study. This sampling method is most useful when the sampling units vary considerably in size because it assures that those in larger sites have the same probability of getting into the sample as those in smaller sites and vice versa (see Table 1).
Selection of the Sample Size of PLHIV (Sample Size = 555).a,b

Abbreviations: ART, antiretroviral therapy; PLHIV, people living with HIV/AIDS; VCT, voluntary counseling and testing.
aAdapted from Sudan Central Bureau of Statistics. 34
bNumber of PLHIV registered in each VCT/ART centers (SNAP Annual Surveillance Report 2011). 35
Ethical approval to conduct the study was obtained from the National Health Research Ethics Committee of the Federal Ministry of Health in Sudan. Informed consent was obtained verbally from all respondents separately prior to the interview.
Analysis Method
Data were analyzed using SPSS 18 statistical software (SPSS Inc, Chicago, Illinois, USA). The study used the chi-square test and the discriminant analysis (DA) function to analyze the survey data. The DA function undertakes the same task as multiple linear regressions by predicting an outcome. It is also used when there are more than 2 independent variable categories compared with the logistic regression, which is limited to 2 independent variables. 26
The Empirical Model
The coping strategies among the affected groups were evaluated using the socioeconomic variables which form the discriminant function. The following variables were used to discriminate between the coping strategies based on gender (see Table 2).
Summary of the PLHIV Survey Data “Variables.”a

Abbreviations: NGO, nongovernmental organization; PLHIV, people living with HIV/AIDS.
aSource: PLHIV Survey 2011 Results using SPSS.
The DA helps in making assumptions regarding the best set of discriminate variables through the proportion of the statistical test. The stepwise procedure employed Wilks Lambda λ as a basis to select variables that form the discriminant function. The nonstandardized discriminant function can be calculated according to the following equation:

where Y = discriminate function; V = discriminant coefficient or weight for that variable; X = respondent’s score for that variable; a = constant; and n = number of predictor variables.
The objective of the analysis is to identify the weights of v1 … vn of the first equation that will expand the following equation to explain the coping strategies:

Equation 1 shows a linear combination of the socioeconomic ratio (x1 … xn) for PLHIV in Sudan. The aim is to identify the weight of the variables in the equation by performing this analysis. Based on the equation, the DA was performed by using men and women living with HIV/AIDS as dependent variables and the socioeconomic coping strategies variables identified earlier as independent variables. The variable that decreases the value of Wilks λ, is entered at each step. This stepwise estimation is used to perform the analysis, whilst entering the independent variables. Estimating the discriminant function will help in identifying the minimum discriminant function that provides most of the discrimination power among the different coping strategies for both men and women. The aim is to explain whether there is variation in the coping strategies between the 2 groups.
Results
Demographic and Socioeconomic Characteristics of the Respondents
The results from the descriptive demographic data of PLHIV (see Table 3) show that more than two-third of the respondents were males (60%), while the rest were females (40%). Eighty-one percent of the respondents were Muslims and 19% were Christians, which is due to separation from the republic of South Sudan, as majority of them were not Muslim. Approximately a quarter (25.6%) of the respondents have marginal jobs and 14% were unemployed and 26% housewives. After infection, almost 78% do not have a source of income.
Socioeconomic and Demographic Characteristics of the Respondents.a

Abbreviation: PLHIV, people living with HIV/AIDS.
aSource: PLHIV Survey 2011 Results using SPSS.
The distribution of the respondents according to age shows that PLHIV in Sudan is highly concentrated in the range of 16 to 49 years. More than half (51%) of the respondents had never been to school or received primary education. In addition, 92.7% of the respondents acquired the infection via heterosexual transmission. Close to 50% of the respondents have previously been admitted to a hospital, with the duration of hospitalization ranging between 1 month and 1 year (see Table 4).
Duration and Expenditure on Hospitalization by PLHIV.a,b

Abbreviations: IQR, interquartile range; PLHIV, people living with HIV/AIDS.
aMedian age (IQR): 36 (30-43) of 555 PLHIVs; median income salary (IQR): 99 (99-250) of 555 PLHIV; median hospitalization (IQR): 1 (1-2) of 250 PLHIV; median expenditure per day in hospital (IQR): 99 Sudanese pounds (60-99) of 554 PLHIV.
bSource: PLHIV Survey 2011 Results using SPSS.
The results show that reported expenditure was greater than income for comparison groups, as 77% had no formal source of income and 45% received partial formal income after infection, suggesting that this population is forced to live beyond its economic capability. The findings showed that 88% of the infected persons did not have any savings to deal with increased health expenditures which caused 67.9% of them to sell their assets. This situation is true for those households affected by HIV faced with huge expenditures such as health care and treatment and nutrition. 27 In addition, PLHIV suffered and had to cope with schooling expenses of their children, 45.4% of the respondents could not pay their children’s school fees.
The results showed that neighbors and friends were another source of support to individuals and households in dealing with medical expenses. Close to 50% (49.9%) of the respondents reported receiving financial support from relatives and 36.5% mentioned borrowing from friends.
Distribution of the Respondents by Mode of Transmission
The main mode of HIV transmission in Sudan is sexual intercourse and this accounts for about 97% of transmissions. 11 The survey findings confirmed this, as 93% of the respondents stated that the virus was transmitted to them through sexual contact and only 0.5% mentioned that the virus was transmitted to them through blood transfusion (see Figure 1).

Mode of transmission of HIV. Source: PLHIV Survey 2011 Analysis Results.
Coping with Children’s Education
The negative impacts of HIV/AIDS included children forced to drop out of schools and to take up work to generate extra income. Most of the AIDS patients interviewed reported that their children were not attending school. Table 5 shows that the main reason behind such children dropping out of school was their inability to meet the schooling cost. When the respondents were asked whether their children were still in school after the infection, 56% responded affirmatively, while 44% responded negatively.
Children’s Education.a

Abbreviation: PLHIV, people living with HIV/AIDS.
aSource: PLHIV survey 2011 results using SPSS.
When the respondents were asked about payment of educational expenses, 19.1% mentioned paying the expenses. For those children continuing schooling, 36.4% of the respondents reported that their relatives shoulder the educational expenses. About 4.5% mentioned others and only 2% mentioned government aid. This meant that even the 56% who had their children in school face shortage of income to pay the school expenses and depended on external assistance.
When the respondents were asked the reason why their children were not in school, 65.9% mentioned lack of income,17.5% mentioned that they needed their children to work to generate income to help their families, and 4.8% mentioned that their children take care of sick members of the household. The results indicates that, children were forced to leave school and join the job market due to a decline in the family’s income along with increased health expenses and reduced income for other needs.
The Result of the Empirical Model
The results of the univariate analysis are presented in Table 6. The F test highlighted the significant difference in the coping strategies among the men and women to deal with the impact of the disease. This difference attributed to variables such as salary, cost of education for children, level of education, children continuing schooling after infection, having income after infection, hospital admission, source of income after infection and marital status. Table 6 also shows significant difference in the means between the 2 groups.
Coping Strategies between Infected Men and Women.a

Abbreviations: Afinfech, children still in school after infection; Afexpend, expenditure after infection; Asstinf, still have assets after infection; Contactf, means of transmission of the virus; Educos, Tte burden of education cost; Edulevel, education level; Hospital, admission to the hospital; Hospcost, payment of hospital cost; Infetill, still have income after infection; Maritas, marital status; PLHIV, people living with HIV/AIDS; Sourcinc, source of income; Transmis, mode of transmission of the virus.
aSource: PLHIV Survey 2011 results using discriminant function analysis.
The results show that in terms of keeping children in school after the infection (Afinfecth), women were less able to retain their children and/or wards in school and ensure the continuation of their children’s schooling in relation to their male counterparts (26.21 for women to 55.30 for men) as they faced challenges in sustaining payment of school fees. This significantly shows low earnings and lack of job opportunities on the side of the women owing to prevalent norms related to femininity in most African countries. 28,29
In terms of salary, the findings show that the variation was very high (147.37 for women and 235.52 for men), indicating that higher numbers of men were engaged in formal employment, ensuring a better level of income, which in turn allowed them to cope better with the stress of the disease. For women, they were challenged with low employment rates and low socioeconomic status, rendering them more vulnerable to the negative impact of the disease. Women, especially widowed and divorced, also faced financial constraints due to the loss of their breadwinners. Furthermore, due to cultural unfounded beliefs, women in Sudan have less income because they lack access to some types of jobs, resulting in lack of appropriate health care and affordable health insurance.
With regard to marital status, the findings show that married women infected with the disease (1.86 for women and 1.61 for men) were better able to cope with the psychological impact of the infection in comparison to their male counterparts, reason being that the majority of married women tended to stay at home as housewives (approximately 60% of infected women), therefore having little interaction with persons outside of their community. On the other hand, married men were found to be more commonly engaged in formal employment and were in turn more exposed to stigma and discrimination from fellow workers and colleagues. In addition, the disease can take a greater toll on men due to the role they play as family heads, where in most cases they are the sole breadwinners for the family. The sense of incapacitation and being unable to meet their family needs and commitments increases their stress levels greatly.
In terms of hospitalization, the results indicated that men were able to cope better with the burden of health care costs than women do (7.18 for men to 2.39 for women) due to the differences in income status. In addition, results show that men included in the survey had a higher level of education than women had (2.66 for men to 2.33 for women), hence enabling them to meet the educational costs of their children—the ratio being 64.4 for men to 40.4 for women).
The results further show that in terms of the source of income before the infection (sourcinc) and source of income after infection (infectil), the mean of income for men was larger than that for women (75.05 for men and 51.43 for women and 29.75 for men and 11.33 for women), respectively. This is a strong indication that men have higher income placing them at an advantage and stronger footings, having better coping mechanism to cope with the impact of the disease. This is in line with the documented literature which asserts that men have more access to formal employment as well as income generating activities. 27,30
The remaining variables show no significant differences between the 2 groups in coping with the disease burden. The inference can thus be drawn that men and women who coped with the impact of the disease do not behave differently in terms of variables such as selling of assets, use of personal/household savings, or borrowing money to meet the increasing health service demands which accompany the disease.
Table 7 shows that the first variable entered in the model was the “aftinfech” (children still in school) variable, followed by 4 other variables. It should be noted that Wilks λ statistics decreased as each step was computed. The discriminate variables presented in the table show a high degree of significant variation. It should be further noted that the criteria to enter or remove the variables from the function are based on Wilks λ and the tolerance level of .001. The results show empirical evidence regarding the variations in the coping strategies among men and women, in terms of source(s) of income after the infection, having income after the infection, the costs of schooling for children and hospitalization. Given this method, these variables were important in determining the coping strategies between the 2 groups.
Variables Constitutes the Discriminant Function.a
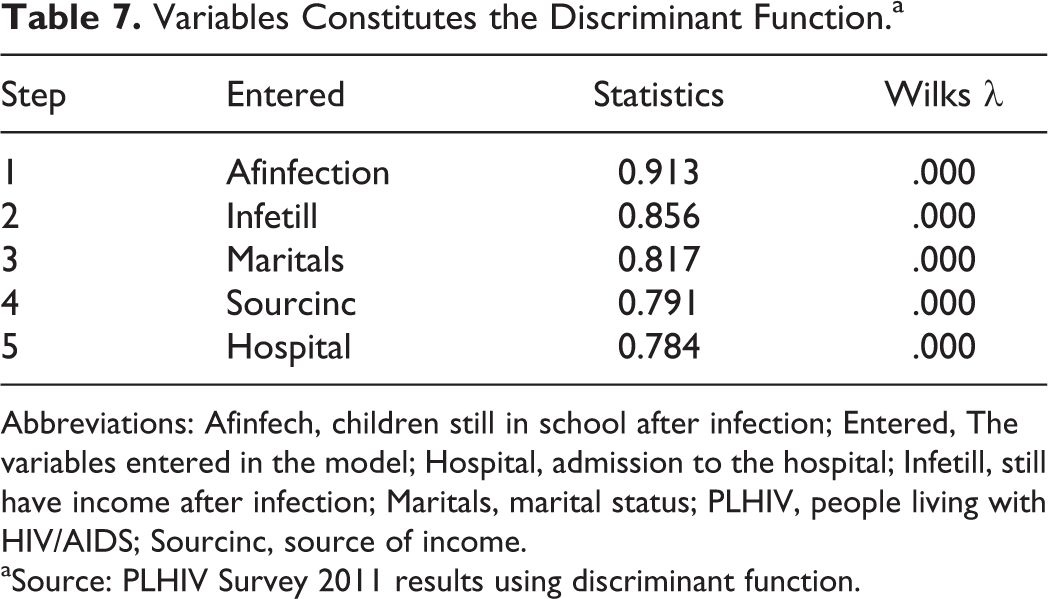
Abbreviations: Afinfech, children still in school after infection; Entered, The variables entered in the model; Hospital, admission to the hospital; Infetill, still have income after infection; Maritals, marital status; PLHIV, people living with HIV/AIDS; Sourcinc, source of income.
aSource: PLHIV Survey 2011 results using discriminant function.
Discussion
The effect of HIV/AIDS is impoverishment, because it leads to higher adult morbidity and mortality, loss of employment, more female household heads, and increasing dependency ratios, deepening the poverty situation. In an attempt to escape the impoverishing effects and deprivation due to poverty, households headed by men or women might adopt different types of action and strategies to cope with this situation such as to alter household composition, draw on savings, sell assets, or use assistance from relatives or other households and from other informal government institutions or nongovernmental organizations to acquire their necessities result from HIV infection. 31
The study showed that PLHIV in Sudan have 3 alternatives in terms of dealing with changes in income and expenditure, that is, to borrow, to utilize savings, or to sell assets. Affected households appeared to first use their savings and assets before they borrow money in an attempt to cope with the financial pressures. This makes sense when considering that the households included in the sample are primarily poorer households with few assets and low income and lacked savings.
The results provide evidence that the impact of HIV/AIDS is more critical on women compared to men. Socioeconomic factors and cultural values place men in a more favorable position for coping with the impact. In their roles as mothers and care providers, women are mainly responsible for taking care of HIV/AIDS patients in the home and for fostering AIDS orphans, in addition to other productive and domestic tasks.
Moreover, the findings suggest that women are more burdened by the economic impact of the disease mainly in terms of income, according to Sudan Household Health Survey, 32 56.9% of household headed by women are below the poverty line, compared to 48.1% of men. It was also found that women are economically dependent on men. 7 According to the findings, it was found that in general women in Sudan are less likely to be employed than men are. According to the available recent data from United Nation Development Programme (UNDP) 18 and in terms of labor force participation, males constitute 38.3% while the share of females stood at 14.1%. Moreover, keeping children in school was found to be a major problem among infected people due to their inability to pay school fees for their children.
Conclusion and Policy Implications
Economic impacts reported by this study combine to create a vicious cycle of poverty and HIV/AIDS in which affected households are grasped up. When productive members of the household become ill and are forced to leave their jobs, their income will decline, children are often forced to drop out of school to assist in caring for the sick or to work so as to create additional source of income. Furthermore, when expenditure on food is reduced due to reduction in income and diverting the resources to cover medical expenses, malnutrition often results, and according to UNDP 18 the nutrition situation in Sudan is characterized by high levels of underweight and chronic malnutrition.
The paper concludes that, 2 major causes of impoverishment are a dramatic increase in spending on health care, which depletes and liquidating savings and, simultaneously, a severe reduction in the incomes of the infected individuals. As the disease progresses and reaches advanced stages, health care cost increased and household resources and savings are diverted for medical treatment. It is recommended that, district-specific microfinance schemes should be promoted to start income-generating activities and informal rotating savings. 33 One way in which this could be done is to provide revolving loans. This requires lending money to someone in need, and when it is repaid, it is again given as loan to another person. This is likely to provide a longer-term source of capital for those involved. The government should use the local and internationally available funds to help in mitigating the impact of HIV/AIDS on food and nutrition. It should also prohibit children from leaving schools and attempting particularly harsh and risky occupations.
There is urgent need to boost the educational and economic opportunities of women and young girls in rural areas. This will reduce HIV transmission by providing alternatives to commercial sex. It will also contribute to sustainable rural development and remarkable improvement in the status of women in the patriarchal society. Advancements on the social variables of education, empowerment of women, and human rights protection are urgent important factors in mitigating the impact of the disease as well and that of women in particular. These are also critical in their own rights.
In the light of the findings of this paper, it is suggested that the government of Sudan considers economic information in planning health care and to mitigate impacts through advocacy on economic protection measures. This paper calls for an economic approach to understanding HIV-infected patients’ access to resources and their families’ present and future security.
Footnotes
Acknowledgments
The authors would like to thank all the PLHIV in Sudan, who participated in this study as well as the health care providers who facilitated data collection and the Federal Ministry of Health for making available the fund.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This research is funded by the World Health Organization Research Fellowship.