
Abstract
The purpose of this descriptive study is to highlight the physical and mental health symptoms of 68 rural women living with AIDS (WLA) in India, their compliance to antiretroviral therapy (ART) medication, and barriers to accessing health care within the past 6 months. Physical and mental health status was obtained by self-report, administered by questionnaire and physician-determined clinical assessment, as well as selected objective parameters. Findings revealed that while rural WLA had been on antiretroviral therapy for just under 2 years, they self-reported a high prevalence of physical symptoms, and more than half reported high levels of depressive symptoms and major barriers to accessing health care. CD4 levels, body weight, and basal metabolic rate were also low. While the rural and urban WLA faced similar health care challenges, the demographic characteristics of the rural women may make them more vulnerable, as they are less adherent to ART and slimmer than their urban counterparts.
Introduction
Today, in India, nearly half of the HIV-infected population live in rural areas and have a poor public health infrastructure which has management challenges, poor quality service, and lack of funding. 1 Treatment centers for HIV/AIDS are mostly located in urban areas and monthly collection of antiretroviral therapy (ART) is particularly problematic for rural women living with AIDS (WLA) who bear the brunt of stigma, lack autonomy or decision-making power, are illiterate and rarely employed, 2 and lack basic knowledge of HIV transmission. 3,4 Moreover, they face profound challenges in following treatment regimens, modifying health risk behaviors, caring for family members, and maintaining positive mental health status. 5
While there is some literature that details the HIV/AIDS epidemic in urban India, there is a paucity of literature that depicts the health of rural WLA. The purpose of this study is to describe the physical and mental health symptoms experienced by rural WLA, their compliance to ART medication, and the barriers to accessing health care sites during the past 6 months. These findings will be discussed in relation to comparisons with populations of urban women in India.
A prospective secondary analysis of persons diagnosed with AIDS in South India revealed that patients with a baseline CD4 count less than 100 cells/mm3 had an 85% probability of survival at 12 months, while those with a baseline CD4 count between 100 and 199 cells/mm3 had a 96% probability of survival.
6
While we are not able to consider rural versus urban differences, CD4 counts among urban women in Bangalore
7
averaged 367 cells/mm3 compared to women in rural Chhattisgarh,
8
where 17% had a CD4 count
In terms of opportunistic infections (OIs), tuberculosis (TB) remains the most prominent in both urban and rural areas. Among 457 persons living with HIV in urban Pune, India, TB was the most commonly reported OI affecting 15.4 per 100 person-years. 10 In a cohort study of 90 HIV-positive patients in rural Chhattisgarh, India, the most common OI was also TB (23%), followed by oropharyngeal candidiasis (17%), onychomycosis (15.5%), and bacterial pneumonia (5.5%). 11 Among the 594 urban counterparts residing in urban Chennai, the 3 most common AIDS-defining illnesses were pulmonary TB (49%), extrapulmonary TB (11.0%), and Pneumocystis carinii pneumonia (6%). 12 In terms of other HIV symptoms, among HIV-positive adults in eastern India, the most prevalent HIV-associated symptom was fever, followed by weight loss (71% and 53%, respectively). 13 Furthermore, an assessment of the clinical profile of people living with HIV/AIDS (PLWHA) at a tertiary care center in urban Kashmir revealed the predominant physical symptoms experienced by HIV-infected adults included fever, asthenia, and weight loss. 14
Among individuals with AIDS, adherence is arguably one of the most important predictors of both the long-term success of first-line ART regimens and the development of drug resistance. Nevertheless, numerous barriers exist. In a qualitative study with 60 HIV-positive adults living in urban Chennai, barriers to adherence included (a) cost; (b) social support/stigma concerns; and (c) perceived benefits of nonadherence. 15 Comparatively, WLA residing in rural Andhra Pradesh reportedly faced several barriers to adherence which included worsening AIDS symptoms, side effects to medications, psychological sequelae of having AIDS, and social barriers such as lack of finances to travel to district hospitals, lack of accompaniment, and child care. 16 In fact, current literature suggests that rural Indian women face the compounded effects of lack of knowledge, poverty, gender inequality, financial constraints, perceived lack of benefits of treatment, fear of disclosure, lack of social support, and geographical isolation which may affect ART adherence. 15,17
Barriers in accessing care also impact adherence to ART as well as overall health care. Lack of education has been implicated as a major barrier to accessing adequate medical care. In India, WLA lack information about HIV disease progression, ways of seeking treatment or dealing with ART side effects, and strategies to promote a less stressful life. 18 In relation to rural versus urban differences, 1 76% of women in rural Andhra Pradesh heard of AIDS compared to 87% in urban India. 19 Among urban women living in Andhra Pradesh, about one quarter had comprehensive knowledge of AIDS compared to 17% of those in the rural region. 19 Rural women are also more likely to experience lack of access to care compared with urban women. 20,21 Specifically, rural WLA cite barriers to care such as lack of transportation, lack of finances, inability to seek child care support, and for caring for a sick spouse. 22 Stigma is yet another major barrier preventing HIV-positive patients from getting adequate medical care. 23 In a qualitative study conducted in an urban nongovernmental organization (NGO) in Chennai, 15 barriers to ART adherence were somewhat similar to rural areas and included low disclosure of HIV status, lack of social support, fears about stigma, and privacy concerns. 15
In India, WLA face serious social, psychological, and economic problems; these include coping with stigma from in-laws, disclosing their diagnoses to their families, caring for ill husbands, providing income to their families if the husbands are ill or deceased, and caring for ill children. 16,24,25 While little is known of urban versus rural distribution of mental health disorders, in general depression is the most common psychiatric condition reported by persons with HIV. 26 One study found that among 51 persons with AIDS in urban South India, 40% were depressed. 27
Depression is also one of the major barriers related to noncompliance to ART. 28 ,29 Among HIV-positive persons in urban Pune and New Delhi, India, severe depression was associated with lower adherence rates to ART. 28 A survey of people living with AIDS (PLWA) in urban South India demonstrated that enacted, felt, and internalized stigma were associated with higher levels of depression. 30 Specifically, perceptions of felt stigma encouraged people to avoid disclosing HIV status. 30
Methods
Design
This study reports findings from a cross-sectional baseline questionnaire administered to 68 WLA who were enrolled into a 2-arm prospective, randomized clinical trial. This article focuses on baseline physical and mental health indices relevant to PLWA. Human Subjects Protection Committee clearances were obtained both in the United States and in India.
Sample and Setting
Women were invited to participate if they met 4 criteria: (a) were living with AIDS; (b) were between the ages of 16 and 45 years; (c) had received ART for at least 3 months; and (d) had not participated in an earlier qualitative study. Patients were excluded if they were not cognitively intact, as assessed by the research staff, or had current CD4 counts less than 100 cells/mm3. The research settings included 2 high-prevalence HIV/AIDS villages in rural Andhra Pradesh that were randomly selected from a pool of 16 demographically similar sites served by a Public Health Center (PHC).
Screening Procedures
Potential participants were made aware of the study by flyers posted in the PHCs of the participating villages. After the participants expressed interest, research staff contacted them and provided a description of the study in a private setting in the PHC. After all questions had been answered, interested WLA signed the first informed consent. Immediately thereafter, a brief screening questionnaire was administered by the research staff, which elicited eligibility information about HIV and ART status and age. Subsequently, blood was drawn to assess the current CD4 counts. After CD4 results had been provided about 1 week later, eligible WLA who wished to participate then completed a second informed consent procedure and were enrolled in the study. Administration of the baseline questionnaire by a trained interviewer followed immediately thereafter.
Measures
Several of the instruments have been previously tested with WLA in the United States 31,32 and in India. 33 All instruments were translated into the native language, Telugu, and back translated to assure semantic equivalence. Sociodemographic information, collected by a structured questionnaire, included age, sex, birthday, education, religion, employment status, marital status, and number of children.
Health history was collected by self-reported HIV- and TB-related physical symptom questions, as well as the history of OIs and other illnesses as assessed by a licensed physician. We also assessed the history of health care access and utilization. Number of pills left in medication bottles was also checked at baseline by the interviewer at the time of baseline administration. This calculation of adherence was based on the month of the year the baseline was conducted.
CD4 counts were assessed during screening. Blood samples were sent to the district hospital laboratory for CD4 count determination by flow cytometry.
The Center for Epidemiologic Studies–Depression Scale (CES-D) is a 20-item scale that measures frequency and severity of depressive symptoms on a 4-point continuum. The CES-D has well-established reliability and validity. 34 Scores on the CES-D range from 0 to 60, with higher scores representing greater depressive symptomatology. Internal consistency for this scale in the present sample was .94. Depressive symptoms were dichotomous at the suggested cut point of 16, indicating a need for psychiatric evaluation.
Data Analysis
Categorical sociodemographic and health care characteristics, HIV symptoms, OIs, and barriers to clinic visits were described with frequencies and percentages. Standard deviations and medians, if appropriate, were reported.
Results
Sociodemographic Factors
A total of 68 WLA were enrolled in the study and completed the baseline structured questionnaire. The mean age was 31.2 years (SD, 5.3 years), and the women reported a mean of 1.6 children (SD 1.0; Table 1). The majority of the women had received less than a high school education (94%); about three quarters reported employment. Slightly over half of the women were married and over 40% were widowed. Nearly two thirds reported being Hindu and more than three quarters lived with children.
Sample Characteristics.a

a N = 68.
Abbreviation: SD, standard deviation.
Physical Health
The most prevalent HIV symptoms reported by our WLA included fevers and fatigue (84%; Table 2). At least three quarters of the women reported dizziness, frequent headaches, and changes in body shape. Over half of the women reported gastrointestinal symptoms and stomach pain, difficulty sleeping and skin rashes, followed by depression/mood swings. Least prevalent symptoms included mouth ulcers (31%). Over 54% reported experiencing depressive symptoms.
Self-Reported HIV Symptoms in the Past 6 Months.a

a N = 68.
Abbreviation: CES-D, Center for Epidemiologic Studies–Depression Scale.
In terms of objective measures (data not shown), the mean CD4 count was extremely low at baseline (mean 443, SD 26), with a range of 127 to 1071, and the median value was 363.5. Regarding the body weight parameters, average values suggestive of a thin phenotype at baseline were observed among WLA. Lean weight was 32.7 kg (SD, 5.3 kg; median, 33.5 kg), with a range of 22.1 to 46.2 kg. Basal metabolic rate (BMR) revealed a mean of 994.3 (SD 160.7; median 1017), with a range of 671.0 to 1403.0.
Health Care
Opportunistic infections and clinician-determined assessment of illness
Over the last 6 months prior to entry into the study, women were unaware of the OIs they had experienced. However, Table 3 reveals a clinician-determined assessment of illnesses described by the WLA at baseline assessment. These most prevalent illnesses included pyrexia of unknown origin and skin rashes (97%), followed by wasting, oral candida, and amebiasis (nearly 80% and higher).
Illness-Related Clinical History Determination by Licensed Physician.

Abbreviations: TB, tuberculosis; LGV, lymphogranuloma venereum.
In terms of health care utilization, WLA on average had been receiving ART for just under 2 years (about 22 months). About one third had been tested for HIV because they had experienced persistent severe illness or had a spouse who was HIV positive (Table 4). At baseline, adherence to ART averaged 54%; range was 27% to 88% (data not shown). The mean number of visits made to health care providers was 7.5 over the past 3 months. Providers included health care staff at the government hospital (100%), followed by pharmacists (68%), primary health center staff (65%), and medical assistants (52%). Fewer WLA reported making visits to an NGO/voluntary testing and counseling (VTC) site (15%) or private practitioner (40%).
Health Care Utilization and Treatments.a

a N = 68.
Abbreviations: SD, standard deviation; ART, antiretroviral therapy; PHC, primary health center; NGO, nongovernmental organization; VCT, voluntary counseling and testing.
Barriers to Access to Care
Table 5 depicts major barriers to clinic visits. These included long wait times at the clinic or hospital (71%), followed by difficulties with, or lack of, transportation (65%) and need to work (63%). Lack of child care was also cited by more than half of the women.
Barriers to Clinic Visits.a
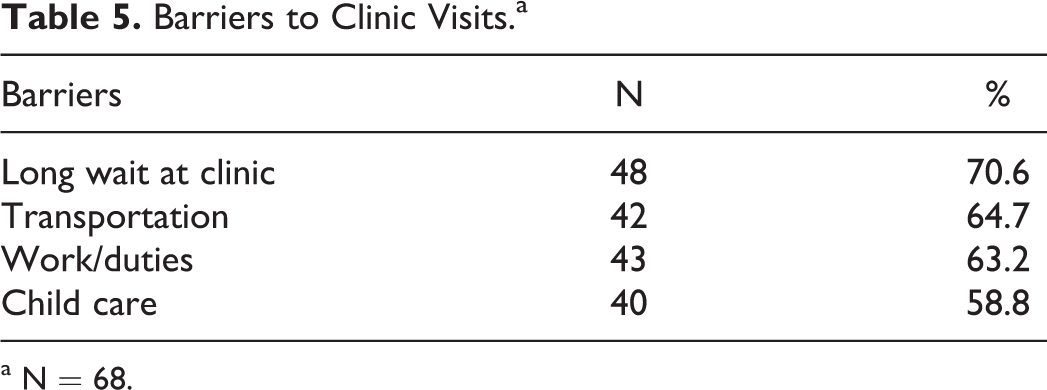
a N = 68.
Discussion
This article is a novel contribution that provides a basis for understanding the physical, mental health problems, and access to health care issues faced by rural WLA, living in Andhra Pradesh, India, and how our data compare with existing literature among their urban counterparts. Demographically, rural women in our study were quite distinct from urban areas. For example, we found that 94% of our participants received less than high school education compared to about 85% of mixed urban/rural counterparts in Kolkata, India 35 ; being married favored the urban group (89% urban vs 52% rural).
Our rural participants were not aware of the name of the OIs validated in the hospital settings. Based on self-report, our WLA revealed fever, fatigue, dizziness, and frequent headaches over the past 6 months. Over 50% reported difficulty sleeping. Moreover, our study physician reported high rates of pyrexia of unknown origin, skin rashes, wasting, oral candida, and amebiasis. In another rural study, the most common presenting complaints among PLWHA were pyrexia of unknown origin, diarrhea, and weight loss. 11 These urban findings are somewhat higher in frequency as compared with urban study investigators. 13,14 New health care policies should be considered in rural areas where medical information in the form of documentation of OIs, dates of diagnosis, and medication provided is readily available to patients in order to optimize the continuity of care.
Adherence to ART was poor among our participants as the average adherence rate at baseline was 54%. In a study of a primarily urban setting, 20% of participants reported less than 95% adherence at baseline. 33 We also revealed that 75% of WLA experienced changes in body shape within the past 6 months. Mean body weight and BMR reflected a lean body composition; lean weight (mean = 32.7 kg) and BMR (mean = 994.3). Saghayam et al 9 studied weight and body shape changes among persons on ART in urban Chennai. Both men and women (N = 190) averaged a mean of 56 kg at baseline. Interestingly, these authors likewise report CD4 counts at baseline with a mean of 175 (SD, 102), 9 which was lower than our mean baseline CD4 count of 443. A true comparative study of rural versus urban WLA is warranted to fully understand the dynamics occurring among these populations.
Interestingly, we found that 54% of WLA reported severe depressive symptoms. However, in a study of depression and coping skills among PLWHA in urban Kolkata, nearly 60% of women had depression based on the Beck Depression Scale. 35 Studies have also found that depression has been associated with caregiver burden, stigma, 36 and poorer health care. 26 Among widows of injection drug users (IDUs) in rural Manipur and Nagaland, some of whom were HIV positive, 70% experienced depression and anxiety. 37 Among WLA, self-reported and clinical depression, anxiety, and suicidal ideation need to be further explored. Understanding psychiatric morbidity can provide future mental health education and treatment for WLA.
Equally important, our findings revealed WLA reported specific barriers to accessing care which included long wait times, lack of transportation, work/duties, and child care. Similar findings were reported in other studies of primarily urban WLA. 15,22
Limitations
The small sample size limits generalizability of the findings. Thus, more research is needed to determine whether the WLA in this study are representative of WLA in other rural areas of India. As Andhra Pradesh is a large rural state, the results of the study should relate to a substantial proportion of rural WLA. In addition, while self-reported health history may suffer from recall bias, engagement of a licensed physician to elicit health information mitigated the bias somewhat.
Conclusion
When compared to urban WLA, rural WLA revealed similar challenges which negatively impacted access to health care and reported similar physical and mental health symptoms. However, the demographics of the rural women may make them more vulnerable, particularly as these WLA appear to be less adherent to ART and are slimmer than their urban counterparts. Our data strengthen the need for culturally tailored interventions that more clearly focus on improving access to care among rural WLA and strategies to support adherence to ART. Our findings also provide a foundation for intervention, wherein a comprehensive team of health care providers, ranging from HIV-oriented lay village women to community nurses and physicians, can ensure consistent and high-quality health care. Additional research is needed to provide a prospective design to better understand the behavioral and biological symptoms and the demographics of rural WLA versus urban women with the goal of improving quality of life.
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This study was funded by the National Institute of Mental Health, Grant #MH082662.