
Abstract
Mexican Americans have the highest prevalence of type 2 diabetes (T2DM) within the U.S. Hispanic community with 14.4% affected, and are disproportionately affected by diabetes-related comorbidities (“Center for Disease Control and Prevention” [CDC], 2023; Haw et al., 2021; National Center for Health Statistics, 2022). Engaging in diabetes self-care behaviors, including exercise, monitoring blood glucose levels, and following a healthy diet, is vital for adequate diabetes management (“American Diabetes Association” [ADA], 2022). However, Hispanics encounter barriers to engage in adequate diabetes self-care behaviors which contribute to worse health outcomes (Aguayo-Mazzucato et al., 2019). Implemented diabetes self-education programs have been found to increase knowledge of diabetes self-care behaviors and improve glycosylated hemoglobin (A1C) (ADA, 2022).
Diabetes self-management education can be significantly impacted by family support (McEwen et al., 2019). Often, family members improve a patient's well-being, ability to follow up with medical treatments, and adherence to positive lifestyle changes by way of their expressed thoughts and attitudes, similar to findings by Fort et al. (2020). However, at times, family's nonsupportive behaviors can intensify the stressors that come with managing a disease (Mayberry et al., 2019), and can be associated with being less adherent to one's diabetes medication regimen and having poorer glucose control (Mayberry et al., 2014).
Culturally tailored interventions that incorporate family (Ingram et al., 2007) have led to statistically significant increases in diabetes self-care behaviors in Mexican Americans in the U.S. border region (Teufel-Shone et al., 2005). However, in the Mexican American population, few studies have qualitatively explored how family supports and hinders diabetes self-management, which is concerning given worse complications seen in this subgroup compared to other Hispanic American adults (CDC, 2023). Some recent studies have gathered perspectives on the relationship between Mexican Americans with T2DM and their children and in rural populations, but few have been done within the family unit or in other geographic areas with a high concentration of Mexican Americans (McEwen & Murdaugh, 2014; McEwen et al., 2017; Rascón et al., 2022).
Chicago, Illinois’ Hispanic population is largely Mexican American (“2020 Census Hispanic”, 2020), with this population experiencing higher rates of T2DM (16.7%) than Chicago's general Hispanic population (13.2%) (“Adult Diabetes Rate”, 2021). Despite its reported benefits, the effects of family on diabetes self-management behaviors have not been qualitatively described in this urban setting that is home to a significant proportion of Mexican Americans. Through qualitative analysis, the purpose of this study was to identify how family influences diabetes self-care management in Mexican Americans, and how family without T2DM is impacted by the disease.
Methods
Study design
This qualitative study used data from two separate research studies and one additional dataset (Baig et al., 2012, 2014, 2015, 2016). The current study design uses the qualitative research method of modified template analysis to explore diabetes self-care management behaviors in the Mexican American community using previously transcribed data. Complete details regarding study design, data collection, and data analyses of the prior datasets can be found in Table 1.
Description of Previously Collected Study Data.
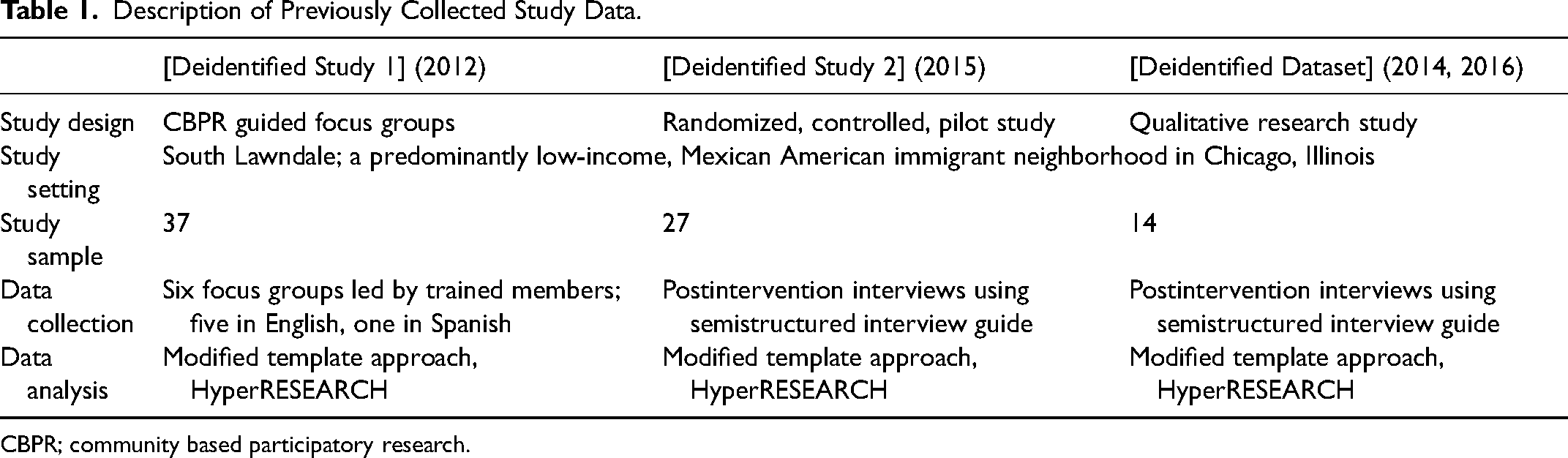
CBPR; community based participatory research.
In the first study, participants were recruited to elicit solutions of how to address T2DM disparities in the Hispanic community (Baig et al., 2012). This study was conducted in partnership with community members at two predominantly Mexican American churches and used community-based participatory research (CBPR) methods, a research methodology that focuses on collaborating with community members throughout the research process (Wells & Jones, 2009), to elicit ideas of effective diabetes interventions (group vs. one-on-one) that might happen in a church setting. The second study (Baig et al., 2015) was a randomized, controlled pilot study to improve diabetes self-management in the Hispanic population. The intervention arm included eight weekly 90-min group classes that were conducted by lay members who encouraged using intrinsic motivators to elicit behavioral change; in the control arm, participants were invited to a 90-min lecture on diabetes self-management by a bilingual community health educator. In this study, all participants could opt to take pictures that represented or were related to their T2DM and management; semi-structured interviews were conducted to inform subsequent research in creating a culturally-tailored diabetes intervention (Baig et al., 2014, 2016).
The final dataset used randomly selected participants from the second study described. These data were used in a culturally-competent training for healthcare providers that included direct patient audio narratives describing the importance of chosen photographs (Baig et al., 2014, 2016). An objective of the interviews was to explore beliefs, behaviors, and challenges to diabetes self-management.
Setting
All study subjects were recruited in a predominantly low-income, Mexican American immigrant neighborhood in Chicago, Illinois in which many risk factors exist that lead to poor health and higher diabetes-related mortality (Community Snapshot: South Lawndale, 2016). The research team recruited participants through posted flyers at churches, verbal referral at health fairs and church events, and word-of-mouth in the community.
Data collection
The first study was conducted between February and April 2009. Six focus groups were conducted with 37 adults diagnosed with T2DM or who had a family member with T2DM. These groups were led by a trained bilingual community member. Interviewers followed a semi-structured questioning guide that was intended to elicit opinions on proposed interventions and to elicit perceived community needs and barriers to diabetes self-management (Appendix A). Five groups were conducted in English, and one in Spanish that was translated into English by a professional translation service. The sessions lasted approximately 90 min each and were audio recorded and transcribed verbatim using professional software.
For the randomized pilot study, 100 participants were recruited from May 2011 to June 2012. Of this study's 100 participants, 30 were contacted to complete post-study interviews between July 2012 and February 2013 to gather personal experiences and social support as it relates to diabetes self-management and study participation. Interviewers followed a question guide that included two family-focused questions that asked if the program helped to involve family in diabetes management and if they would recommend the program to a family member (Appendix B). These interviews were conducted by trained research assistants in a private room at a local health center, lasted 45–60 min each, and were led by a trained bilingual interviewer. Interviews were transcribed verbatim using professional software; three were not transcribed due to administrative error.
For the final dataset, an additional fourteen interviews were conducted with participants from the randomized study; seven of these participants had not previously been interviewed. Interviews were completed between June 2013 and August 2013, lasted approximately 30 min each, and were audio-recorded and transcribed in a similar fashion to the prior studies described. Trained research staff led participant interviews that discussed the rationale for taking the photographs, and worries, challenges, motivators, and successes that the photo represented. The potential role of family in diabetes management for each participant was discussed in the interview (Appendix C).
Data analysis
One researcher grouped representative quotations into themes using inductive and deductive analysis and developed an initial codebook. Data were then analyzed using a modified template approach and code reports were generated in HyperRESEARCH. This researcher further used hierarchical coding to identify sub-themes and representative quotes. A second researcher independently reviewed code hierarchies and reviewed subthemes in collaboration with the first researcher. The first researcher subsequently refined subthemes based on the discussion and coded representative quotations into a list that was finalized in discussion with the second researcher (Morse, 1995).
Ethical considerations
All studies from which the current study's data were derived were approved by the Institutional Review Board at The University of Chicago. All participants provided written informed consent.
Results
Data were collected from a total of 71 participants (37 from focus groups, 34 from one-on-one interviews). Participants had a mean (SD) age of 55 (11) years and 80% were female. Eighty-nine percent self-identified as Hispanic, and the majority of participants reported being of Mexican descent (86%) and born in Mexico (72%). Fifty-eight participants (82%) reported a diagnosis of T2DM and 13 (18%) noted having an immediate family member with T2DM. Seventy-seven percent of participants were born outside of the United States. Spanish was the primary language spoken at home for 82% of participants.
Quotations were grouped into four categories. The first three categories pertained to participants with T2DM, and the fourth included perspectives from family members of those with the disease.
Family-Related Facilitators to Participants’ Diabetes Self-Management (Table 2)
Provides support
Family as a source of support for diabetes management was expressed by 39 (55%) of 71 participants. Twenty-two participants mentioned that family provided instrumental support in providing healthy food, medication adherence, and transportation to doctor's appointments. Several mentioned families were accommodating to their needs, and a couple stated family was involved in day-to-day management of their diabetes. Some participants also discussed how family members provided informational support by giving advice, recommendations, and reminders to assist with diabetes management as well as emotional and companionship support. One noted:
“My daughter bought some little boxes like this … she arranges everything for me so that … I don’t forget [to take my medication].”
Family-Related Facilitators to Participant's Diabetes Self-Management.
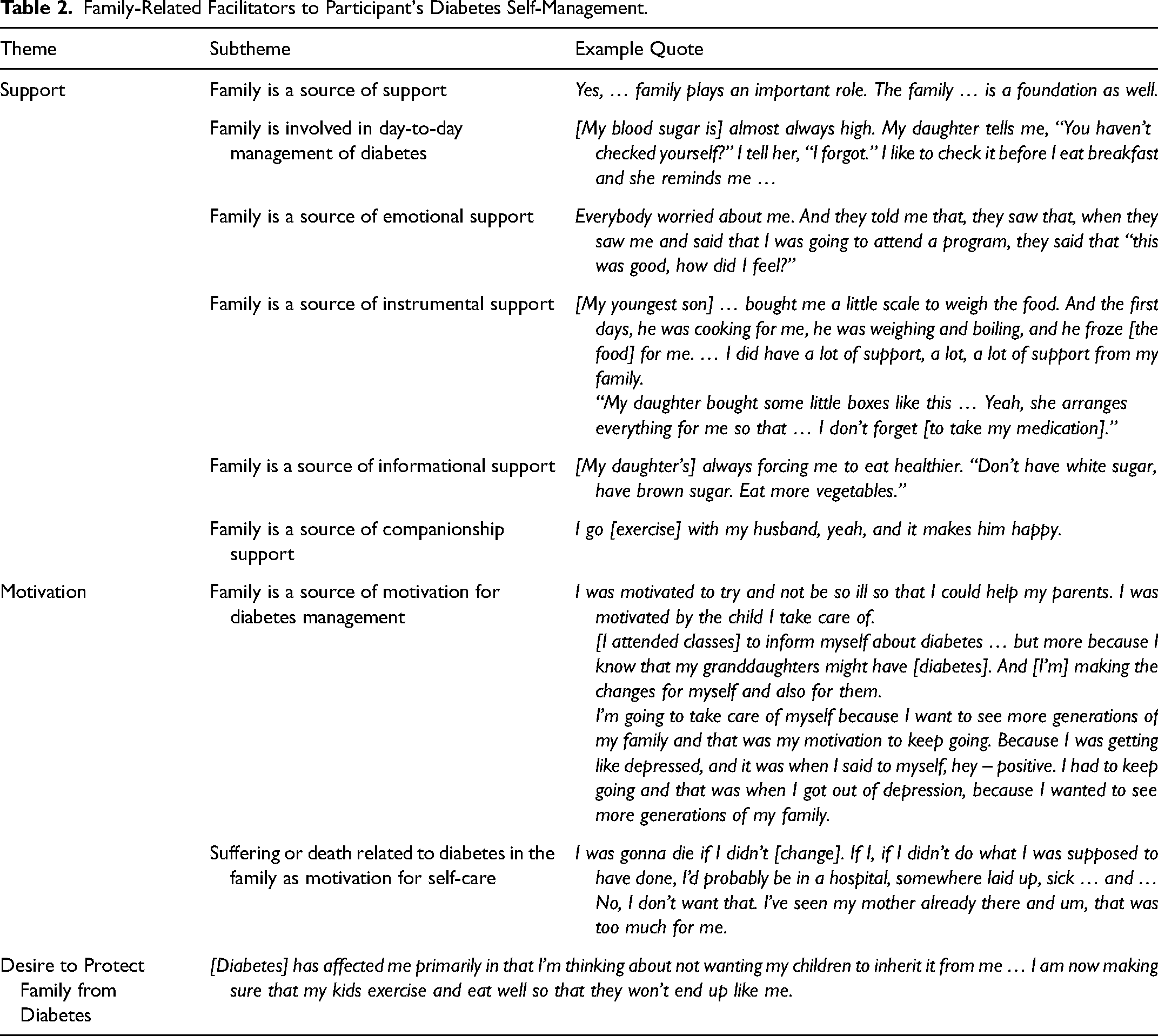
Provides motivation
Family as a motivator for participating in diabetes self-care behaviors was expressed by 24 (34%) of 71 participants (Table 2). Being able to support family members in the future and enjoy life with grandchildren were frequently mentioned as motivation to improve self-care. Many of these participants said family members who had already suffered from diabetes complications provided motivation to maintain their own health. Many (20%) of the participants mentioned having brothers, sisters, parents, and grandparents with diabetes, whereas only one participant spoke of having no history of diabetes in her family. One participant shared:
“… If I didn’t do what I was supposed to have done, I’d probably be in a hospital, somewhere laid up, sick … No, I don’t want that. I’ve seen my mother already there and um, that was too much for me.”
Desire to protect family from diabetes
Twenty-one (30%) of all participants reported wanting to be more informed about diabetes in order to prevent diabetes in family members and protect them from its complications. One participant stated:
“[Diabetes] has affected me primarily in that I’m thinking about not wanting my children to inherit it from me … I am now making sure that my kids exercise and eat well so that they won’t end up like me.”
Family-Related Challenges to Participants’ Diabetes Self-Care (Table 3)
Lack of support
Lack of social support from family was expressed by 15 (21%) of 71 participants. Some participants mentioned they did not have family members around or who cared about their diabetes management with one stating:
“I am here by myself. In other words, I am here with my four kids, no one else. So, I don’t have any relatives and my children, well they want to be taken care of, not the other way around.”
Family-Related Challenges to Participant's Diabetes Self-Management.
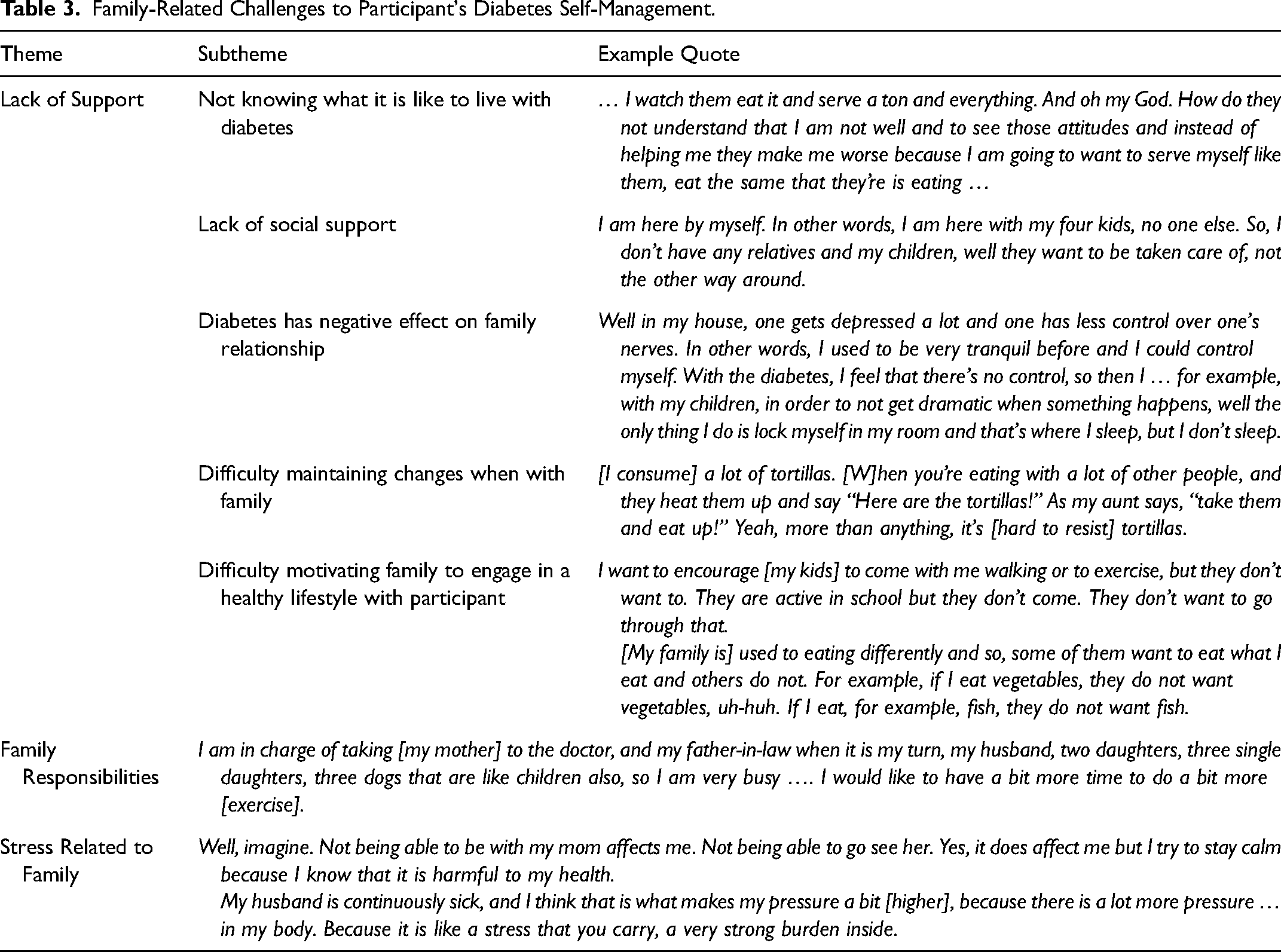
Nine participants noted that family members did not understand what is it like to live with diabetes.
Fifteen (21%) of 71 participants stated they had difficulty engaging family in a healthy lifestyle with respect to exercise and food. Some participants explained that they had difficulty maintaining healthy lifestyle behaviors when with family, such as resisting unhealthy foods, and at times felt wearied by their family members’ unhealthy behaviors:
“[I consume] a lot of tortillas. When you’re eating with a lot of other people, and they heat them up and say ‘Here are the tortillas!’ As my aunt says, ‘take them and eat up!’ Yeah, more than anything, it's [hard to resist] tortillas.”
However, one participant mentioned she had little difficulty changing their own eating habits with regards to appropriate food portions. Another participant did not live with any family, which made it easier to adhere to a healthy diet.
Seven participants (10%) expressed that diabetes had negatively affected their relationships with family members.
Family responsibilities
Of all participants, 16 (23%) were routinely busy taking children to and from school or taking family members to appointments, which competed with their ability to provide self-care. Two participants had difficult family environments that interfered with management behaviors. One participant noted:
I am in charge of taking [my mother] to the doctor, and my father-in-law when it is my turn, my husband, two daughters, three single daughters, three dogs that are like children also, so I am very busy. I would like to have a bit more time to do a bit more [exercise].”
Stress related to family
Seven participants (10%) with diabetes mentioned stress from family as negatively affecting their self-care, citing sick family members, issues coping with family stress, and the stress of living separately from family members.
Impact of Diabetes Education Information on Family (Table 4)
Sharing information
Of all participants, 16 (23%) reported they disseminated information to family members, with many sharing healthy eating tips and materials from the study intervention:
“My 18-year old nephew who I took care of when he was young, tells me “Godmother, you know, ever since you have been giving my mom the handouts, she has had everyone on a diet.” And he has lost a lot of weight. He says, “My mom only wants to feed us lettuce like rabbits.”
Impact of Diabetes Education Information on Family.
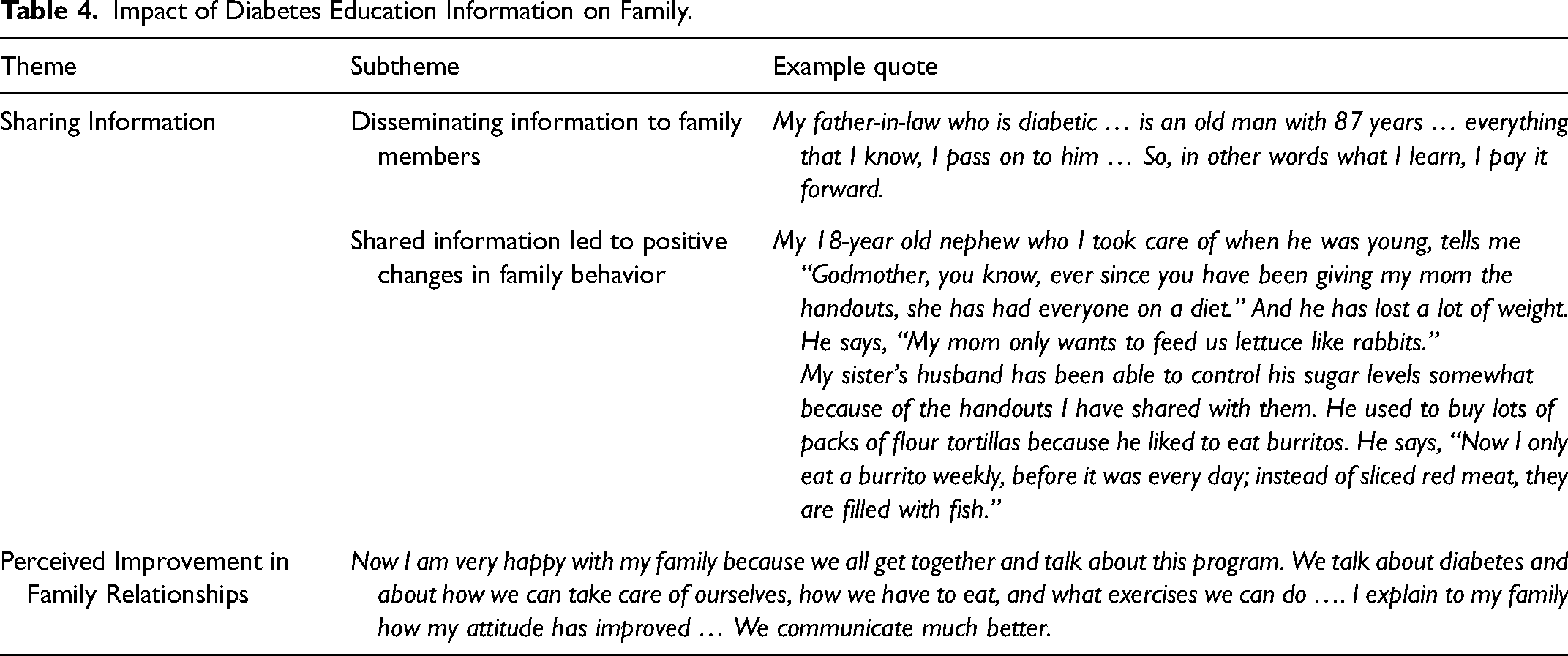
Some participants encountered family tension when sharing diabetes information, but most (23%) said that the knowledge they shared with family led to a positive impact on family behavior, especially regarding diet.
Multiple participants mentioned the desire to include family members, especially children, in diabetes education programs to prevent the disease in future generations.
Perceived improvement in family relationships
Four participants noted that sharing diabetes knowledge with family helped involve them in their diabetes management, improved communication within the family, and allowed them to share their feelings about diabetes:
“Now I am very happy with my family because we all get together and talk about … diabetes and about how we can take care of ourselves, how we have to eat, and what exercises we can do … We communicate much better.”
Family Member Perspectives on Diabetes Management (Table 5)
Family does not know how to help
Of 13 family members, 11 (85%) also expressed a desire to be more educated about diabetes or have more education provided to family members. One family member stated family responsibilities interfered with providing more support. One participant expressed her issues providing support in the context of their cultural upbringing:
“You need to deal with customs and traditions. You need to find out the best way to educate yourself … ”
Family Member Perspectives on Diabetes Management.
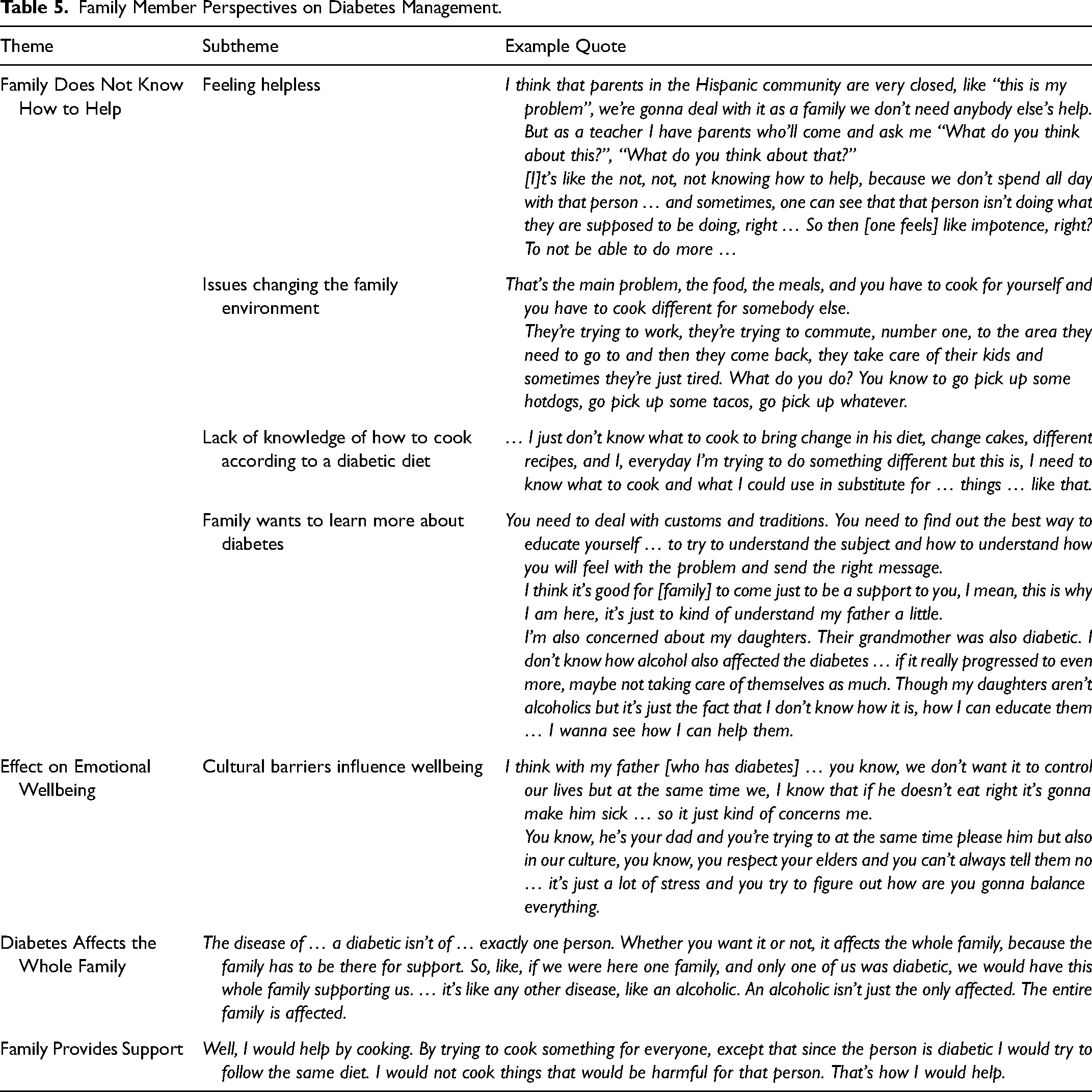
Some expressed feeling helpless, had difficulty changing the family environment to support healthy behaviors, and lacked knowledge of how to cook according to a diabetic diet:
“That's the main problem, the food, the meals, and you have to cook for yourself and you have to cook different for somebody else.”
One participant noted getting support from other community members:
“I think that parents in the Hispanic community are very closed, like ‘this is my problem’, we’re gonna deal with it as a family we don’t need anybody else's help. But as a teacher I have parents who’ll come and ask me ‘What do you think about this?’”
Effect on emotional wellbeing
Six (46%) of all family members of someone with diabetes reported that diabetes had affected their emotions, inciting worry, stress, and anger. One participant stated cultural traditions of respecting elders contributed to stress when helping manage their loved one's diabetes:
“You know, he's your dad and you’re trying to at the same time please him but also in our culture … you respect your elders and you can’t always tell them no … it's just a lot of stress and you try to figure out how are you gonna balance everything.”
Diabetes affects the whole family
Four family members of participants with diabetes reported that diabetes affected the entire family.
“Whether you want it or not, it (diabetes) affects the whole family, because the family has to be there for support.”
Family provides support
Five family members expressed they did provide support for those with diabetes.
Discussion
This study outlines various key themes regarding the family role in diabetes self-management among Mexican American adults, including perspectives from family members. This relationship has been investigated, but previous qualitative studies have focused on Mexican Americans in different geographic areas or pairs (Hu et al., 2013; McEwen et al., 2017) and, to our knowledge, this is the only study in recent years that categorizes this relationship in an urban city with a majority Mexican American Hispanic population.
These results emphasize that family provides varying types of support for diabetes self-care behaviors, and often is a motivator to improving self-management behaviors. Similar studies have noted grandchildren, spouses, and other family members as motivation (Hu et al., 2013; Perez-Brescia et al., 2022; Rascón et al., 2022; Schmittdiel et al., 2018). Despite this knowledge, the proportion of Mexican Americans with poorly controlled T2DM (Hemoglobin A1C > 9%) remains almost double that of non-Hispanic whites (CDC, 2023). Our study provides detailed evidence on the struggles those with diabetes face and how we can ameliorate them in Mexican American families.
Our research enforces that diet and T2DM are inextricably linked. Dietary changes hold a complex role in self-management behaviors. Often, conflict within families centered around lack of support for healthy eating and poor food choices by family members, which is similar to qualitative research results by Toney et al. (2023). Our study highlights the complexities of this theme within the Mexican American community, and future directions should encourage dietary recommendations that are culturally adaptable in Mexican American families.
Participants often shared diabetes education information within the family unit which led to positive behavioral changes in family members. There are increased odds of unrecognized prediabetes in the Hispanic population (Cowie et al., 2018). Research on non-Hispanic adults has shown that family members of those newly diagnosed with T2DM often implement significant changes in health-related behaviors both consciously and subconsciously (Schmittdiel et al., 2018). In research performed by Reininger et al. (2020), involving family in a diabetes intervention led to improved A1C at a 12-month interval, which suggests a longer intervention period may be more beneficial in populations who experience more social or cultural barriers to health. To address shortcomings in preventative health, diabetes interventions could be more effective by including family, perhaps with a focus on shareable resources and hands-on demonstrations to encourage the exponential spread of health benefits to at-risk family members.
The interference of family responsibilities and family-related stress with diabetes self-management noted amongst our study participants has also been found in other studies including Mexican Americans, (Hu et al., 2013) and reflects how the existing healthcare system structure is intertwined with social determinants of health. Revising policies to expand transportation access and utilization may unload that burden off of caregivers, and also may address limited transportation options to healthy foods if they are further from grocery stores than convenience stores. We corroborate with existing literature that policies should focus on improving systematic support to ensure that interventions shown to improve diabetes outcomes can be translated effectively into the real world (Marquez et al., 2019).
Many family members in this study felt helpless due their lack of knowledge of how to best be a support person for one with diabetes. Prior studies have noted similar findings among family members of Mexican American patients (Hu et al., 2013; McEwen et al., 2017) with one intervention that involved teaching family how to best provide positive social and emotional support leading to clinically significant weight loss (Rosas et al., 2020). There is evidence that inclusion of a family member in a group support intervention can lead to statistically significant improvements in fasting blood sugar levels and diabetes knowledge in a rural Mexican American population and improvements in diabetes outcomes
These results show that family members often sought other trusted community members outside of the family unit, such as teachers, to guide behaviors. Using community health workers, or promotoras (lay community-based health outreach partner) has led to improved lifestyle management in interventional studies (Flores-Luevano et al., 2020). While not directly family, extending the familial relationship to trustworthy citizens and forming interventions that utilize these members could help close the disparities gap.
Generally, our findings are similar to those found in other ethnic minorities. In certain East Asian groups, family is a motivator but also presents dietary challenges, (Liu et al., 2022; Nguyen & Jones, 2021), with an added pressure has been noted to improve self-care to avoid becoming a burden to family as they age (Yoon et al., 2022). Park et al. (2022) found that patients with T2DM trusted health information when explained by family members more than providers, which may be why promotoras previously described have improved diabetes self-management. Similar thoughts on barriers and motivators regarding family and diabetes self-management have been described in qualitative literature focusing on black and South Asian communities (Deol et al., 2022; Lee et al., 2019; Rao et al., 2021). This suggests the desires expressed in our study are generalizable to other ethnic minorities facing health disparities.
Limitations of this study included that it was completed in an urban, Midwestern city with a large Mexican American population, and our findings may not be generalizable to all Hispanic populations. Furthermore, the study population was chosen by convenience sampling and collected on a volunteer basis, which may not match a general population, but our results are consistent with other studies with Mexican Americans with diabetes (Hu et al., 2013; McEwen & Murdaugh, 2014). Our study population also consisted of mostly women, so results may not be applicable for Mexican American men. Since our study design analyzed interviews retrospectively and was exploratory in nature, our data may not capture the entire breadth of opinions and beliefs of the family role for Mexican American adults with T2DM, although it is similar to findings in other ethnic groups.
Conclusion
We found that while lack of social support, family responsibilities, and stress from family can undermine successful diabetes management, many participants with diabetes had family available to support their diabetes management but wanted them to provide more social support. Seeing family members suffer with diabetes and preventing diabetes in future generations were noted as motivators. Diabetes knowledge was shared within the family unit, and family members had a desire to learn more about the disease, but didn’t know how to best support at times due to conflict from cultural family norms. Further research should use our findings to inform culturally-tailored diabetes education efforts in order to improve healthcare disparities in the Hispanic community.
Supplemental Material
sj-doc-2-hci-10.1177_15404153231206086 - Supplemental material for The Role of Family in Diabetes Management for Mexican American Adults
Supplemental material, sj-doc-2-hci-10.1177_15404153231206086 for The Role of Family in Diabetes Management for Mexican American Adults by Olivia J. Jordan, Amanda Benitez and Deborah L. Burnet, Michael T. Quinn, Arshiya A. Baig in Hispanic Health Care International
Supplemental Material
sj-docx-3-hci-10.1177_15404153231206086 - Supplemental material for The Role of Family in Diabetes Management for Mexican American Adults
Supplemental material, sj-docx-3-hci-10.1177_15404153231206086 for The Role of Family in Diabetes Management for Mexican American Adults by Olivia J. Jordan, Amanda Benitez and Deborah L. Burnet, Michael T. Quinn, Arshiya A. Baig in Hispanic Health Care International
Supplemental Material
sj-docx-4-hci-10.1177_15404153231206086 - Supplemental material for The Role of Family in Diabetes Management for Mexican American Adults
Supplemental material, sj-docx-4-hci-10.1177_15404153231206086 for The Role of Family in Diabetes Management for Mexican American Adults by Olivia J. Jordan, Amanda Benitez and Deborah L. Burnet, Michael T. Quinn, Arshiya A. Baig in Hispanic Health Care International
Supplemental Material
sj-docx-5-hci-10.1177_15404153231206086 - Supplemental material for The Role of Family in Diabetes Management for Mexican American Adults
Supplemental material, sj-docx-5-hci-10.1177_15404153231206086 for The Role of Family in Diabetes Management for Mexican American Adults by Olivia J. Jordan, Amanda Benitez and Deborah L. Burnet, Michael T. Quinn, Arshiya A. Baig in Hispanic Health Care International
Footnotes
Acknowledgements
This project was funded by the 2017 Summer Research Program at The University of Chicago Pritzker School of Medicine. This research was supported by grants from the University of Chicago Clinical and Translational Science Award (UL1RR024999), the National Institute of Diabetes and Digestive and Kidney Diseases Diabetes Research and Training Center (P60 DK20595) and the Chicago Center for Diabetes Translation Research (P30 DK092949). Dr. Baig was supported by a NIDDK Mentored Patient-Oriented Career Development Award (K23 DK087903-01A1). Acknowledgements are made to the Little Village Community Advisory Board for their feedback and collaboration and Erin Staab, MPH for their help with this study. We have no conflict of interest to disclose.
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Supplemental material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.