
Abstract
Self-managing type 2 diabetes (T2D) is critical but often presents a challenge among African American men. Stress may exacerbate both mental and physical problems, which can lead to poor self-management; however, the evidence is sparse. The purpose of this manuscript is to examine the relationship the role of stress in type 2 diabetes management among a prospective group of African American men living in the southern United States. Nineteen African American men with T2D were recruited from barbershops and churches. Interviews were conducted using a semi structured interview guide. Transcripts were analyzed using a phenomenological approach and focused on identifying common themes describing the responses regarding any stress that the participants have pertaining to living with and managing T2D. The themes that emerged from the participant responses are: (a) experiencing less stress, (b) stress not attributed from diabetes, (c) avoid thinking about stress, and (d) some stress is prevalent. Overall, participants expressed either that diabetes was not attributing to the stress that they have or that they have less stress than they did prior to being diagnosed with T2D. In this sample of African American men, stress became a factor for some participants when considering the complications that can occur from diabetes. These findings suggest the need for key considerations to only incorporate general information about diabetes and stress management, but should be gender and culturally relevant to African American men.
Introduction
Stress is a feeling that is formed when an individual responds to particular actions or situations (Ullah, Khan, & Khan, 2016). It is the body’s way of heightening to a challenge and preparing to meet a vigorous situation with attention, power, endurance, and concentration (Ullah et al., 2016). The situations that incite stress are called stressors, and they cover a wide range of situations including physical stressors such as an illness or trauma (Loghmani, 2005). However, stressors can also be mental, such as in a person’s occupation, marriage, personal health and wellness, or finances (Loghmani, 2005). The human body braces itself to react in turn to distress or stressors, often referred to as the fight or flight response. In the fight or flight response, levels of several hormones such as cortisol and growth hormones escalate (Mitra, 2008). The long-term effect is to produce an adequate amount of stored energy, glucose, and adipose tissue available to cells. Insulin is not always able to allow the extra energy into the cells, so glucose accumulates in the blood (Matough, Budin, Hamid, Alwahaibi, & Mohamed, 2012). These results intensify the propensity of various diseases, and diabetes may be an outcome of stress, which can further spiral into a vicious cycle of a stress–diabetes relationship (Matough et al., 2012).
More and more individuals are living with diabetes; in fact, there are more than 30 million individuals diagnosed with type 2 diabetes living within the United States (Sherman & Williams, 2018). Of these, approximately 15 million are men (Hawkins et al., 2017; Sherman & Williams, 2018). Regrettably, diabetes is more prevalent among minority men (Hawkins et al., 2013; Sherman, Jones-McKyer, Singer, Larke, & Guidry, 2014). Between 1997 and 2010, Latino men (Mexican) experienced increased rates of diabetes of 52%, while African American men had increased rates of 143% (Hawkins et al., 2013). Along with having diabetes comes the possibility of experiencing diabetes complications including diabetic retinopathy, daily stress, and the worry of diabetes complications (Samuel-Hodge, Watkins, Rowell, & Hooten, 2008). African American men have increased rates of blindness and twice as many amputations associated with diabetes as European American men (Sherman et al., 2014; Two Feathers et al., 2005). In addition, mortality rates related to diabetes are the highest among African American men (Thorpe, Wilson-Frederick, Bowie, Coa, Clay, LaVeist, & Whitfield, 2013).
Among adults, the effects of stress on people with diabetes vary in accordance with a patient’s coping ability. There is scant research on how African Americans with diabetes cope with life’s challenges (Samuel-Hodge et al., 2008). The relationship between stress and diabetes has been investigated extensively among the general population of adults, yet there remains a limited amount of published research related to the stress levels of African American men living with and managing type 2 diabetes.
Diabetes is a complex, demanding disease that can induce serious psychological stress, which in turn can inhibit one’s ability to self-manage the condition (Lloyd, Smith, & Weinger, 2005). In addition, distress related to diabetes may be indicative of whether individuals achieve their daily self-care behaviors (Lloyd et al., 2005). Stress also disrupts glycemic control through its effects on stress hormones such as catecholamine and cortisol (Surwit & Schneider, 1993). Living with diabetes can be very stressful, and at times, stress can advance the disease (Seawell, Hurt, & Shirley, 2016). It is important for individuals with diabetes to learn to mitigate and cope with any negative stress reactions, especially because some stressors are a part of daily life (Lloyd et al., 2005).
African American men are more likely to state having a higher rate of stress than White men (Seawell et al., 2016). Sources of stress experienced by African American men may not stem from caring for their diabetes, per se, but from other situations such as the ability to adequately care for family (Mathew, Gucciardi, De Melo, & Barata, 2012; Seawell et al., 2016). Another source of stress for African American men with diabetes is seeing a number of people, whether family or friends, developing diabetes and suffering diabetes complications (Seawell et al., 2016). The purpose of our study was to examine the role of stress in type 2 diabetes management among a prospective group of African American men living in the southern United States.
Phenomenological Methodology
This study utilized a qualitative research design, specifically, a phenomenological research method. According to Patton (1990, p. 71), the focus of a phenomenological study lies in the “descriptions of what people experience and how it is that they experience.” The goal is to identify the essence of the shared experience that underlies all the variations in this particular learning experience. Although none of the participants were related in any way, they all share the same phenomenon which is type 2 diabetes. Essence is viewed as commonalties in the human experiences (Creswell, 2007). This type of research methodology is used to study areas in which there is little knowledge (Donalek, 2004). The original study’s primary focus was to gain a stronger understanding of the essence and lived experiences of African American men living with type 2 diabetes.
Setting and Selection of Participants
Participant Demographics.
These initial subjects serve as seeds, through which Wave 1 subject is recruited; Wave 1 subject in turn recruits Wave 2 subjects; and the sample consequently expands wave by wave like a snowball growing in size as it rolls down a hill (Heckathorn, 2015). The inclusion criteria for the study were as follows: (a) participant self-identified as African American, (b) age 18 to 70 years, and (c) physician-diagnosed type 2 diabetes. The final sample consisted of 19 African American men, most (68.4%) of whom were older than 55 years. About 12 participants (66.0%) had lived with diabetes for 10 years or less. Additional details regarding participant recruitment can be found in the publication by Sherman and Williams (2018).
Instruments and Data Collection
After reviewing published literature centered on diabetes management among non-Hispanic Black men, the interview guide was developed based on the current gap of information missing from published studies. Guide criterion validity was established via review and consultation by two experts: (a) a qualitative methodologist with expertise specific to non-Hispanic Black men and (b) a chronic disease and health inequities researcher. The guide concentrated on eliciting data from six areas: (a) diabetes self-management practices, (b) knowledge and beliefs about diabetes, (c) perceived barriers to diabetes self-management, (d) social support, (e) symptoms, and (f) personal versus interpersonal feelings about diabetes self-management.
Semistructured Interview Guide.

Data Analysis and Member Checking
Narrative analyses have been used to explore life experiences of individuals with diabetes (Stuckey, 2013). Fidelity to the phenomenon as it is lived means capturing and understanding it as perceived through the person living the situation (Moustakas, 1990). Participants in this study told their unique story of how they prefer to manage and treat their type 2 diabetes. Therefore, excerpts from their transcripts were not edited or corrected and are presented in their unique voice as originally recorded. To establish the validity of the interview data, member checking was done after all 19 interviews were completed. Lincoln and Guba (1985) posit that member checking is the most crucial technique for establishing credibility. Member checking is when data, analytic categories, interpretations, and conclusions are tested with the members of those groups from whom the data were originally obtained (Creswell, 1998).
The transcript of the first interview foregrounds the second interview during which the researcher focuses on confirmation, modification, and verification of the interview transcript (Birt, Scott, Cavers, Campbell, & Walter, 2016). The outcome of this process was to ensure that the transcripts that were typed and presented resonated with the participants and that their responses to the interview questions were captured correctly. Participants were given an opportunity to remove and add to their responses, but the only feedback that was provided to the researcher was grammatical corrections that they pointed out on their transcripts. No additional comments were provided by any of the participants who pertained to or elaborated on the interview questions.
Results
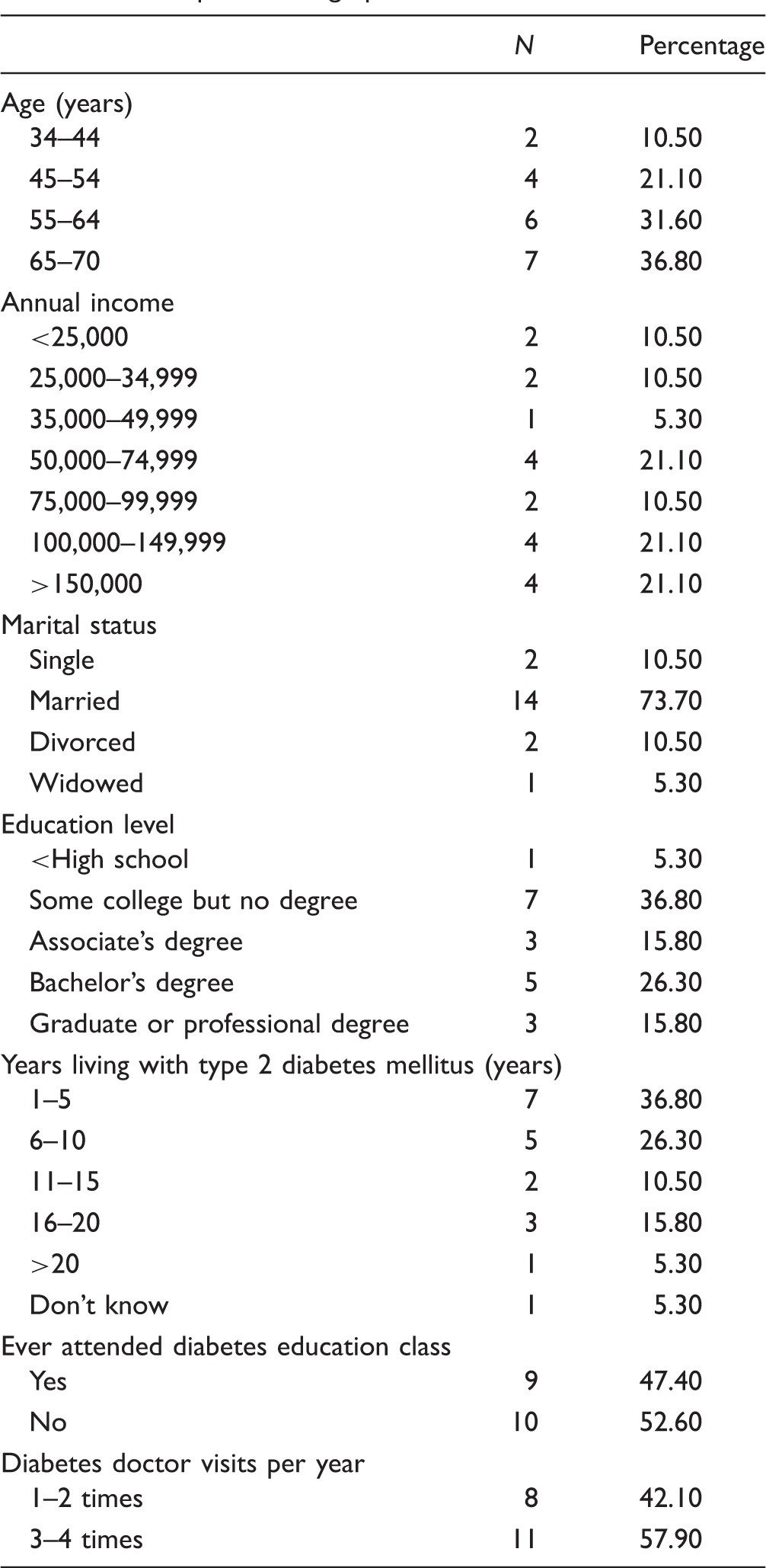
Table 1 shows the sample characteristics of the men who participated in the study. The final sample consisted of 19 non-Hispanic Black men, of whom 68.4% were older than 55 years. Approximately 66% had diabetes for 10 years or less, 42% reported an annual income of $100,000 or higher, 74% were married, and 37% had some college but no degree, while 26% had a bachelor’s degree. Table 2 shows the interview guide used during each semi-structured interview. The participants shared a variety of responses reflecting on any stress that they have pertaining to them living with type 2 diabetes. In their responses, a few participants indicated experiencing stress, although their stress was not attributed to diabetes, but from other aspects of their lives such as their jobs and family responsibilities.
A few other participants indicated that their stress was self-induced and that they try to avoid thinking about particular stressors. Overall, participants either expressed that their diabetes was not attributing to the stress that they have or that they have less stress than they did prior to being diagnosed with type 2 diabetes. Interestingly, only two participants in the sample stated that they have stress due to living with type 2 diabetes. Themes emerging from participant responses included: (a) experiencing less stress, (b) stress not attributing from diabetes, (c) avoid thinking about stress, and (d) some stress is prevalent.
Experiencing Less Stress
Seven of the 19 participants stated that they have little to no stress at all after being diagnosed with type 2 diabetes. The comments that were provided centered on their stress levels being low due to being retired, becoming more knowledgeable about diabetes management, changes in behavior and lifestyle choices, and overcoming the challenges of living with diabetes. During his interview, a 62-year-old retired postal worker commented on how his previous job caused stress in his life and that after he retired, he noticed a reduction in his stress levels, which correlated to a reduction in diabetes-related stress. This participant responded as follows: I’ve been retired now for four years and I was in a stressful job in management and dealing with people. Life is less stressful for me and I think that has helped me more since I retired. I don’t have the everyday thing of working and budgets, and you know … dealing with a lot stressful things so … since my stress level is down, that’s probably why I don’t have a lot of effects with my diabetes. I don’t think there’s more stress. It’s just the behavior pattern that you have to adapt to … and try to do the best you can to work with what you have to work with and work on, but I don’t say it’s more stress. I would say that it’s good in a way because I’m more knowledgeable now … things I took for granted about eating a lot better, now you are trying to do better and manage things. You have to really govern yourself and have to be disciplined … that’s all … they key word is disciplined about what you’re eating and how much you’re eating and all that so basically, that’s it. No! Less stress since I’ve learned how to deal with it. Again, information and knowledge are paramount in dealing with this condition. Coaches, boxers, athletes, study film of their opponents. And that better enables them to prepare themselves for the upcoming game or event. It’s the same with this diabetes … the more I learned about it, the more I read, the more knowledgeable I became, to this point I now, I’m the best diabetic patient that I know! Because the results of the medicine that I’m taking, the knowledge that I have about it has given me the confidence in going by my everyday routine without any stress, without any apprehension about having this in the first place because it can be managed, and you can live with this condition if you follow the instructions. Something else might kill me, but it won’t be the diabetes. No. I think it’s just a matter of accepting that you have it and right now there’s no cure for it. But they do have some guidelines that you can follow to maintain it … to keep it in check. So what I try to do is to stay as close to it as I possibly can. Like I said, sometimes I fall off the wagon, but when you fall off, you realize, hey, I kinda strayed away and you try to come back on course … get back on track. I feel stress free, I’m just putting it like that. I don’t let nothing worry me, I don’t care about what people say. I just go about my day, that’s it. Because if you worrying about what people say, that has an effect on how you’re managing your lifestyle. But my mind is made up and that’s it. No, I don’t look at it as being negative stress. It’s something that I have to look at and deal with but as far a real negative situation, no, I think we can look at it and take something positive from this and that’s diet and exercise and eating properly and letting somebody else know about it.
Stress Not Attributed From Diabetes
Six of the participants in the study indicated that although they do have stress in their lives, the stress is not primarily attributed to living with diabetes. Rather, the stress is due to their jobs, finances, personal responsibilities, and daily time management. A high school teacher/assistant football coach shared a response that focused on how his stress stems from roles and responsibilities that are not directly aligned with managing diabetes. His response was as follows: Well … I don’t think the stress comes from diabetes. I guess the older you get, the more responsibilities you know. You see I got a whole campus and all of my responsibilities as a husband, father, grandfather, educator, and coach fall into one. So it’s hard to divide your time … I guess that’s the way of the world. Our philosophy at my school is that football is your wife and life from June to Christmas. We go seven days a week. So the stress is from my job and my environment, regardless of the diabetes. I have a lot of stress, but I don’t think it’s because of diabetes. Diabetes might be a part of it, but I don’t think it’s that high of a level because of diabetes. I have a lot of other things in that’s been in my life that make my stress more. The diabetes has nothing to do with the stress, unfortunately. I guess that’s a good thing that the diabetes didn’t have anything to do with the stress. The stress in my life comes from typical things, bills, even my job. Like I said, I work pretty much for myself and my job-related productivity and everything is fine. The most stress is work! And in my job, I try to resolve conflict in the workplace. And listening to others and making recommendations and trying to resolve those issues at work at times can be overwhelming. But as far as type 2 diabetes, in the beginning it did because it was that fear. But with education and the support, I am not stressed.
Avoid Thinking About Stressors
Three participants had very interesting perspectives when asked if they have experienced more stress in their lives as they were diagnosed with diabetes. The response they each provided hinted at stress being nonexistent because they try not to think about their stressors. A 54-year-old construction company supervisor responded as follows: No. I don’t even try to thank about it. I just go ahead and do what I gotta do and live my life. When it’s time to go, it’s time to go. Not really. The stress I probably do have is what I caused myself. As long as worry about it, that’s what keeping me stressed. As long as I somewhat pretend in my mind that it’s not there, it’s not bothering me, then I’m living me own life. I’m not sure if the stress is from my job or … I’ve been taking on more responsibilities at my job lately but, I don’t think the disease really stresses me out more. I pretty much still do everything I want to do. I guess maybe it should, but I never really thought about it.
Some Stress Is Prevalent
Two participants in this sample indicated that they experience stress as a result of living with diabetes. A retired Vietnam veteran responded as follows: Yes I do. I’m stressed because seeing people with limbs removed due to complications. You know that … that causes me to stress to the extent that I was discovered to have diabetes, the VA signed me up for a Veterans support group and I went there for counseling for probably six months. And in that counseling, they were telling us what we should do, what we shouldn’t do and that we could have a productive life with diabetes and that there are people living that have had diabetes for 25 years and 30 years if they did the right thing and had God on their side. So I’m definitely stressed. I do. You see all of the gray hairs on head and neck popping out? All of these gray hairs just popping out of nowhere. They say it’s from stress, I’m sweating now. Yeah it’s a lot of stress but I have to make sure that is stay on my ABC’s like I said.
Discussion
Investigators conducted semistructured interviews to examine how African American men experience stress while dealing with the diagnosis and self-management of diabetes. Some participants indicated that they experienced less stress after the diagnosis of diabetes and that stress is related to issues outside of diabetes management. Study participants identified with being the primary provider for their families and sources of stress were related to family obligations and commitments at their places of employment. Results of other studies with African American men echo these findings and indicate family relationships can help to cope with the realities of diabetes. On the other hand, family and financial demands can be a source of stress (Seawell et al., 2016). Seawell et al. (2016) conducted focus groups among African American men diagnosed with diabetes, and a paradox was uncovered of how Black men feel like king of the castle but have little control over food choices in the home and the need to provide financial assistance to adult children. Additionally, the need to make ends meet extends to stress in the workplace where African American men have pressure to keep steady employment. Within our study, one participant mentioned how his job was stressful, but stress levels decreased once he retired. It is important to note that almost 70% of participants in this study were aged 55 years or older and were experienced within their jobs. The fact that some participants were either retired or planning for retirement may have contributed to thoughts of less stress after learning about the diagnosis of diabetes in this population.
There was a variety of responses regarding stress after learning of the diagnosis of diabetes among study participants. Stress became a factor for some participants when considering the complications that can occur from diabetes. One participant mentioned how fear set in after thinking about others who had limbs removed because of the disease. Other men commented that they avoid thinking about diabetes and stress altogether. Among those who avoid thinking about stress, there were thoughts that there was nothing they could do about the disease and they should just let it run its course. The notion of fatalism has been identified in other research within this population (Breland, McAndrew, Gross, Leventhal, & Horowitz, 2013). Other research works confirm that African American men deal with the stress of diabetes differently, which include avoid thinking about it all together, eating unhealthy, or drinking alcohol excessively (Seawell et al., 2016). Although these men are not thinking about it, the disease process will advance, and efforts should be made to educate men on strategies to mitigate the progression of diabetes.
Of participants who experienced less stress after the diagnosis of diabetes, acquiring more knowledge about the disease was a key factor. Hurt, Seawell, and O'Connor (2015) conducted focus groups among Black men who discussed developing diabetes programming specific for Black men to help cope with the disease. Based on this work, key considerations should not only incorporate general information about diabetes but should also be gender and culturally relevant to African American men. That would include providing information on how diabetes affects one’s ability to be a primary provider in the home. As discussed by study participants, the majority of stress comes from family and financial commitments. Providing a program that specifically addresses those concerns can empower African American men to perform self-care and manage their disease, which may reduce stress. In addition, programming should be easily accessible to African American men at low cost. If possible, education sessions should be facilitated by Black men to encourage fellowship and create a social support system in the community (Hurt et al., 2015).
Conclusion
Most participants of this study did not feel stressed after learning about their diagnosis of diabetes. A major factor that mitigated thoughts of stress was education and strategies on how to manage diabetes. After becoming educated on how to self-manage the disease, many of the men felt relieved and even less stressed about the situation. Factors that contributed to stress seemed unrelated to diabetes and included jobs, finances, and family circumstances. Older and retired participants mentioned that they experienced less stress since leaving the job. A few men reported some level of stress, which was due to thoughts of long-term complications of diabetes.
Recognizing how African American men react to stress is essential for understanding and addressing their immensely high proportions of stress-related chronic disease and untimely mortality. It is imperative to examine how stress and coping frameworks relate to men's health, in general, but specifically in African American men. Interceding to enhance stress-related health for African American men will require a multilevel approach that is cognizant of men’s identities, characteristics, and social and physical environments, and how these help frame the ways that men manage stress. Cultivating theories and interventions that evolve from recognizing the familiar and exclusive issues that influence stress and coping among African American men may have a more significant impact on enhancing the lives of this underrepresented population.
Limitations
This study has some limitations. This was a qualitative study, which involved 19 participants. As a result, the study findings are not generalizable to all African American men who are living with type 2 diabetes. Because this was a qualitative study, a very large sample size was not needed as one would need for a quantitative study. The results of this study are presented to raise awareness as well as to pose important questions for further investigation in this area. None of the participants stated in their responses that they have ever had an opportunity to express their concerns regarding their fears of type 2 diabetes (see Table 2). An argument can be made that participants recruited from a different setting, such as a recurring diabetes educational seminar, intervention program, or past participants from a previous diabetes management study, may have had an opportunity to reveal which treatment methods and preferences have aided them most in managing type 2 diabetes.
Footnotes
Authors’ Contributions
Ledric D. Sherman obtained funding for the study, acquired the data, and designed the study. Ledric D. Sherman, DeLawnia Comer-Hagans, and Anthony J. Pattin analyzed and interpreted the data, drafted the article, and critically revised the manuscript for important intellectual content. All three authors approved the final manuscript.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This study was funded, in part, by the Transdisciplinary Center for Health Equity Research (TCHER). TCHER is housed in the Department of Health and Kinesiology, College of Education and Human Development at Texas A&M University.