
Abstract
Objectives:
The aim of this study is to empirically examine a full pathway model of health literacy, and health and well-being outcomes among patients with type 2 diabetes.
Methods:
A three-wave longitudinal survey was administered to 148 patients with diabetes. Covariance structure analysis was conducted to create a path diagram, with health literacy and burden of medical expenses included as independent variables and with psychosocial factors, behaviors, and health and well-being outcomes included as dependent variables.
Results:
The model fit indices showed a comparative fit index of 0.985 at baseline, 0.959 after 3 months, and 0.948 after 6 months, with a root mean square error of approximation of 0.040 at baseline, 0.079 after 3 months, and 0.085 after 6 months. There were 14 significant paths across the three time points between health literacy and understanding of diabetes care, self-efficacy, communication with doctors, and medication adherence.
Conclusion:
The model fitness index showed an adequate result. Health literacy was significantly positively associated with understanding of diabetes care, self-efficacy, communication with doctors, and medication adherence. Health literacy had a direct positive influence on medication adherence and possibly an indirect positive influence on exercise/diet via self-efficacy. The results were generally consistent across the three time points, suggesting good reliability of the models. Improving health literacy may lead to better self-management of diabetes and favorable health outcomes.
Introduction
The number of people with diabetes worldwide is rapidly increasing, and those with type 2 diabetes account for the majority of these cases. In Japan, there are about 10 million people either diagnosed with diabetes or strongly suspected of having diabetes (HbA1c (National Glycohemoglobin Standardization Program [NGSP]) > 6.5%), and the percentage currently receiving treatment increased from 45.0% in 2007 to 76.6% in 2016. 1 Globally, US$825 billion is spent annually on medical expenses for diabetes; in Japan, these expenses amount to approximately US$37 billion, and Japan ranks seventh in the world in terms of diabetes spending. 2
People with type 2 diabetes are greatly influenced by lifestyle and self-care behaviors such as diet and exercise, and they are susceptible to psychological problems, including anxiety and depression. 3 Depression can affect self-care behavior and therapeutic adherence, leading to problematic glycemic control and deteriorated quality of life (QOL).4,5 Patients’ emotional burden should therefore be considered to have a strong influence on self-management behavior and glycemic control,6,7 both globally and in Japan.
It is imperative to improve disease management for patients with type 2 diabetes and to increase efforts to prevent disease progression. To this end, self-management—including a healthy diet, exercise, and a medication regimen—is required on a daily basis. For self-management of chronic diseases, patients need to understand their illness and the necessity of treatment, and they need to implement self-management in daily life. The empowerment approach, aimed at effective decision making, patient participation in treatment, and clarifying the patient’s goals, values, and motivations, has become a focus of attention.8,9
Schulz and Nakamoto 10 noted that, for patients to be empowered, in addition to receiving knowledge, they need to be able to appropriately use their knowledge and information (i.e. health literacy). Health literacy has been defined as “the cognitive and social skills which determine the motivation and ability of individuals to gain access, understand and use information in ways which promote and maintain good health.” 11 The empowerment approach focuses mainly on enabling psychological aspects, such as motivation—the power to independently make decisions and cause actions. However, health literacy goes beyond this, encompassing both the knowledge necessary to maintain and improve health outcomes and the ability and skills to use this knowledge. Psychological empowerment and improved health literacy need to be encouraged to facilitate patients’ effective self-management.
The active involvement of patients and diverse types of support from health care providers are also required in the self-management of diabetes, and collaborative relationships between these groups are needed.12–15 For this purpose, good communication between the patients and health care providers is essential. Patients who can communicate well with their primary doctors have confidence in their own ability to acquire the information necessary for their treatment and for self-management, and to understand and use this information effectively. 16
Previous studies17,18 have proposed causal pathways between health literacy and health outcomes. These have covered topics, including access to and use of health care, provider–patient interaction, and self-care. Based on a review of previous studies on health literacy and diabetes self-management, Fransen et al. 19 developed a framework for health literacy and health outcomes. This framework, which is shown in Figure 1, suggests that health literacy is related to psychosocial factors (e.g. knowledge, understanding, and self-efficacy), behavior (e.g. quality of patient–provider communication and diabetes self-management, including diet, exercise, and medication), and health outcomes (e.g. glycemic control measured with HbA1c and diabetic complications).

Conceptual diagram of Fransen et al.’s 19 health literacy framework.
Regarding psychosocial factors, self-efficacy has been shown to be strongly related to diabetes-related knowledge and self-management.20,21 Health literacy increases patients’ self-efficacy 20 and knowledge about diabetes 22 and thereby improves self-management of diabetes. 23
Effective self-management of diabetes also requires considering the patient’s psychological burden. Previous studies have examined the associations of both degree of emotional burden6,7 and depression 24 with the self-management of diabetes. In terms of the influence of health literacy on psychological burden, no link has been found between health literacy and the prevention of depressive symptoms, 25 but interventions to improve health literacy have been found to improve suffering from diabetes. 26 However, this association remains unclear. Medical expenses such as those for external factors and psychological effects have also been noted, 19 although their association is also somewhat unclear.
Regarding the relationship of health literacy with health outcomes, patients with diabetes with low health literacy may have poor control of their blood glucose level, 27 a high prevalence of diabetic retinopathy, 28 and other complications. 29 Many studies have treated HbA1c as a direct outcome, but one study has reported an association between health literacy and HbA1c.28,30 Other studies testing the association between health literacy and HbA1c have reported that these variables are unrelated,22,23,25,31–33 and there is still no consensus among scholars regarding this potential association. 19 In Japan, one study found no association between HbA1c and health literacy, 34 and another study found that HbA1c levels were low when communicative health literacy was high. 35
Factors such as satisfaction and QOL with regard to patient treatment and self-management may also be important for patients with diabetes and for outcomes such as HbA1c. Research has been conducted on aspects of QOL such as self-efficacy and satisfaction with treatment.36,37 However, no work has yet clarified how diabetes treatment, self-management, QOL, and health literacy relate to satisfaction.
The previous findings summarized above indicate that improving health literacy may increase individual patients’ adherence to required treatments. Health literacy thus may be a pertinent factor for changing behavior and decision making regarding the implementation of self-management and sound daily health habits. However, no studies have yet verified Fransen et al.’s 19 entire model. The present study aimed to empirically examine a full pathway model of health literacy, and health and well-being outcomes among patients with type 2 diabetes. The examined model was based on Fransen et al.’s 19 framework and focused on psychosocial factors, diabetes knowledge, self-efficacy, communication with doctors, and self-management behavior.
Methods
Participants in this study were patients with type 2 diabetes who visited the outpatient internal medicine department for diabetes metabolism at a university-affiliated hospital in Tokyo. The inclusion criteria were having type 2 diabetes, being aged ⩾20 years, and requiring periodic medication. Exclusion criteria were not using diabetes medication, having dementia, or being judged unsuitable by the attending doctor. Patients who were eligible for recruitment were randomly selected from the appointment logs of the study physicians. From October to November 2013, 193 potential participants were identified. These patients were approached in the waiting room after they had attended a consultation, and they were given an explanation of the study purpose and procedures. A total of 153 patients provided written consent to participate in the study and to complete the questionnaire.
A longitudinal study was carried out at three time points: baseline (T1), 3 months after baseline (T2), and 6 months after baseline (T3). The questionnaire responses were kept confidential. Patients were asked to give their name, address, and contact telephone number on the consent form at the time of the first survey. The consent form was linked to the questionnaire by an ID number. The baseline sample of 148 patients introduced by the attending doctor, excluding five patients who were found to be ineligible because of the exclusion criteria, provided consent before the T1 survey. They were asked to complete a self-administered multiple-choice questionnaire at each time point at the hospital or to return the questionnaire by mail from January to March 2014 (T2) and from April to July 2014 (T3). The most common reasons for refusal to participate were a lack of time and poor physical condition on the day of the survey. The study was conducted with the approval of the Ethical Review Committee of the Graduate School of Medicine and Faculty of Medicine, The University of Tokyo.
Measures
Health literacy
Health literacy was measured using the health literacy scale developed by Ishikawa et al. 35 The reliability and validity of this scale have been confirmed. 35 The scale includes 14 items: 5 assessing functional health literacy, 5 gauging communicative health literacy, and 4 measuring critical health literacy. All items are rated on a four-point scale, with higher scores indicating higher health literacy levels.
Psychosocial factors
Understanding of diabetes care
Inoue et al. 34 created a Japanese version of the measurement tool for understanding diabetes care, which was developed by Heisler et al. 38 Items on this scale are rated on a five-point scale, with higher scores indicating higher understanding of diabetes care.
Self-efficacy
Fitzgerald et al. 39 developed a measurement tool for self-efficacy in diabetes management. Items on this scale are rated on a five-point scale, with higher scores indicating higher self-efficacy in diabetes management.
Emotional burden (Problem Areas in Diabetes scale)
To measure the emotional burden associated with diabetes, Ishii et al. 6 created a Japanese version of the Problem Areas in Diabetes (PAID) scale, which was developed by Polonsky et al. 7 The reliability and validity of the Japanese version of the PAID scale have been verified previously. 6 From among the scale’s 20 items, the present study used five reliable and valid items from the PAID-5 shortened version. 40 Each of these items is rated on a five-point scale, with higher scores indicating a higher degree of emotional burden.
Burden of medical expenses for diabetes
The burden of medical expenses related to the treatment of diabetes was scored on a five-step range from “none” to “high,” with higher scores indicating a higher burden.
Behavior
Communication with doctors
We used a scale developed by Clayman et al. 41 to assess communication with doctors and in a clinical setting: The Ask, Understand, Remember Assessment (AURA) comprises four items measuring self-efficacy in collecting, understanding, remembering, and evaluating medical information. We created a Japanese version of the scale after receiving the original authors’ approval, and we performed a reverse translation of the content for verification. All items on the AURA are rated on a four-point scale ranging from agree or disagree with a statement “a little” or “a lot.” Higher scores reflect a higher sense of self-efficacy regarding communication in a clinical setting.
Self-management
Medication adherence
Medication adherence was measured using a 12-item version of the Medication Adherence Scale developed by Ueno et al. 42 for patients with chronic diseases. This scale comprises four subscales. The first contains three items on medication compliance, the second has three items on collaboration with health care providers, the third has three items on willingness to access and use information about medication, and the fourth has three items on acceptance to take medication and how taking medication fits patient’s lifestyle. These items are rated on a five-point scale ranging from 1 (“never”) to 5 (“always”). Higher scores indicate higher medication adherence.
Exercise/diet
Regarding exercise and dietary habits related to diabetes treatment, patients were asked to what extent they followed the instructions of their health care providers, with response options of 1 = “I have received no instructions,” 2 = “I have received some instructions but am not sure what to do,” 3 = “I know what I should do but rarely follow the instructions,” 4 = “I usually follow the instructions,” and 5 = “I almost always follow the instructions.” Higher scores indicate greater adherence to these instructions.
Health and well-being outcomes
Diabetes Therapy-Related QOL: satisfaction with treatment subscale
The Diabetes Therapy-Related QOL (DTR-QOL) questionnaire, developed by Ishii, 43 addresses four areas of diabetes treatment: burden on social activities and daily activities (13 items), anxiety and dissatisfaction with treatment (8 items), hypoglycemia (4 items), and satisfaction with treatment (4 items). The present study included the four items from the “satisfaction with treatment” subscale. These items are rated on a seven-point Likert-type scale (1 = “strongly agree” to 7 = “strongly disagree”). For each item, a score of 1 represents the highest level of satisfaction with the treatment.
Glycemic control (HbA1c)
HbA1c level at the time of each survey was extracted from the patient’s medical chart. The test results of HbA1c were measured on the same day as the questionnaire was administered at T1. For T2 and T3, the test results of the dates around 3 and 6 months after baseline (T1) were extracted from the patient’s chart, respectively.
Basic characteristics
Sex and age were identified from the patients’ medical records. Data on highest level of education, marital status, living with someone else, and working for income were collected from the questionnaires.
Characteristics related to treatment of diabetes and current physical condition
Number of years since being diagnosed with type 2 diabetes, presence of diabetes-related complications, and type of medicine taken for diabetes were determined from medical records, and body mass index was indicated on the questionnaires.
Statistical analysis
All data analyses were performed using SPSS, Version 21.0 (IBM SPSS Japan, Inc., Tokyo, Japan), except for the covariance structure analysis, which was performed using AMOS, Version 21.0 (IBM SPSS Japan, Inc.). Covariance structure analysis is a statistical technique in which a theoretical model, or a covariance structure, is constructed, and the covariance values predicted by the theoretical model are compared with those of the observed data. The adequacy of the model in reproducing the sample covariance values is reflected by estimates of the parameters of the model and measures indicating the goodness of fit. 44
Results
Sample characteristics
Table 1 shows the characteristics of the 148 participants at T1. The average age was 67.9 (range: 32–87) years, and roughly 67% were men and 33% were women. More than 70% were married, 83.1% were living with someone else (i.e. immediate family, relatives, partners, or roommates, irrespective of marital status), 48% had a high level of education (technical college, junior college, or university graduates), and 43.9% were engaged in income-generating work.
Demographic and clinical characteristics of participants (N = 148).

Data are presented as mean ± standard deviation (range), or as n (%).
The mean disease duration of diabetes was 12.0 (range: <1–45) years, mean HbA1c was 7.0% (range: 5.1%–12.6%), and 30.4% of the participants were using insulin injections. Complications were seen in retinopathy (28.4%), nephropathy (51.4%), and neuropathy (32.4%). Some participants had multiple complications. The average body mass index was 24.4 (range: 16.0–51.4) kg/m2.
The final sample at baseline comprised 148 patients. Six of these patients dropped out at T2 (n = 142), and another two dropped out at T3 (n = 140). The drop-out rate was very low (5.4%).
We performed a sample size calculation with a 5% significance level for the test of close fit, with 0.05 as the null value of the root mean square error of approximation (RMSEA) and 0.08 as the alternative value of RMSEA. For the test of not-close fit, 0.05 was the null value of RMSEA and 0.01 was the alternative value of RMSEA. 45 This yielded a minimum target sample size of 95 to 152 participants and a power estimate 0.50 to 0.75. A total of 148 patients with diabetes participated in this study.
Relationships of health literacy at T1 with psychosocial factors, behavior (communication with doctors and self-management), and health and well-being outcomes at T1, T2, and T3
Figures 2–4 show the results of the covariance structure analysis, presented as path diagrams for T1 (n = 148), T2 (n = 142), and T3 (n = 140), respectively. Health literacy and the burden of medical expenses were included as independent variables, and psychosocial factors (understanding of diabetes care, self-efficacy, and emotional burden), behaviors related to communication with doctors and self-management (medication adherence, exercise/diet), and health and well-being outcomes (satisfaction with treatment and HbA1c) were included as dependent variables. When adjusting for educational background, age, and sex, the model fit index decreased. We therefore refer to the results of the models where these attributes were not adjusted. The model fitness indices showed χ2 to degrees of freedom ratios of 1.237 (T1), 1.876 (T2), and 2.011 (T3); comparative fit index values of 0.985 (T1), 0.959 (T2), and 0.948 (T3); and RMSEA values of 0.040 (T1), 0.079 (T2), and 0.085 (T3).

Relationships of health literacy at baseline (T1) with psychosocial factors, behavior (communication with doctors and self-management), and health and well-being outcomes at T1.

Relationships of health literacy at baseline (T1) with psychosocial factors, behavior (communication with doctors and self-management), and health and well-being outcomes after 3 months (T2).
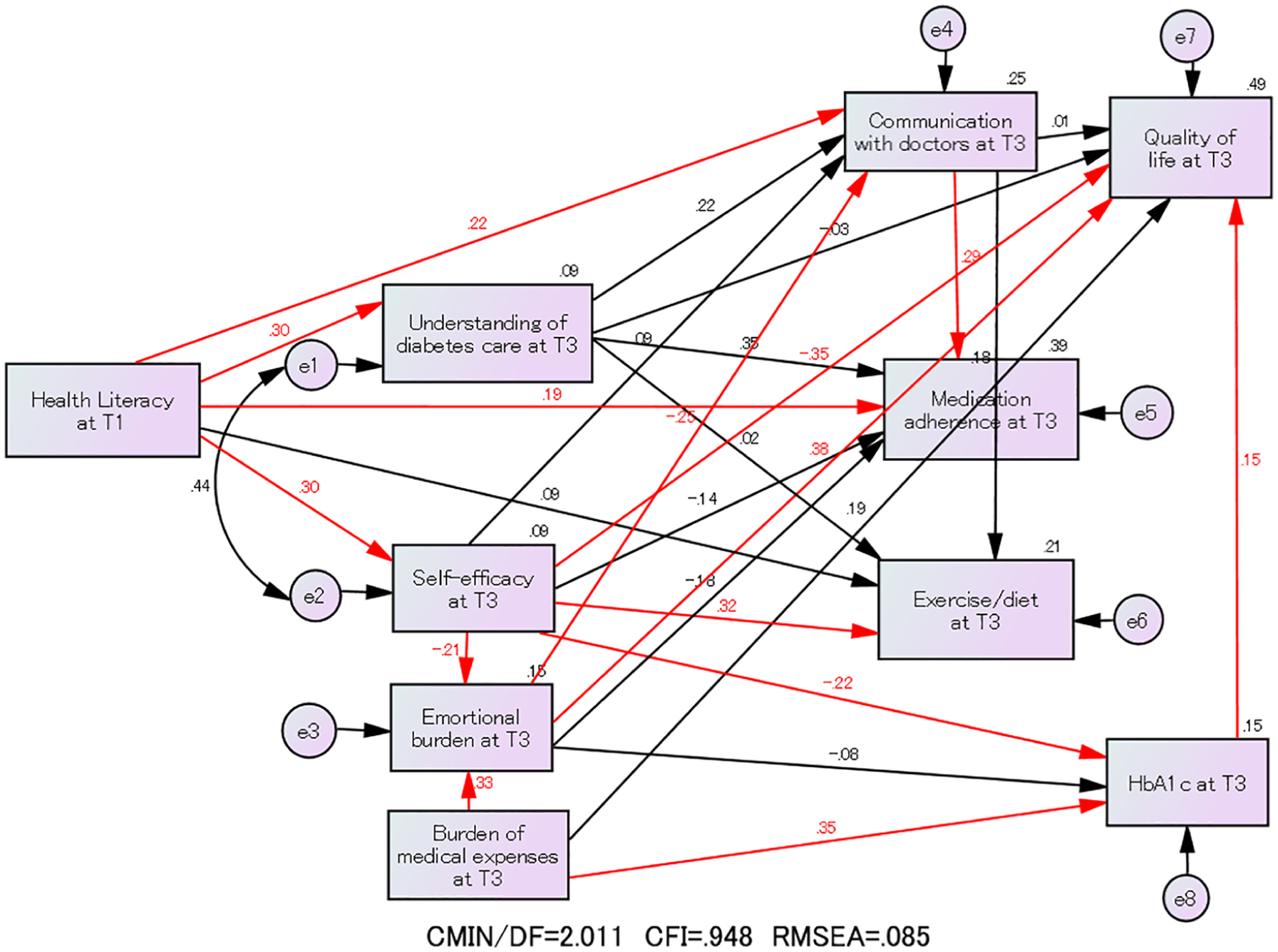
Relationships of health literacy at baseline (T1) with psychosocial factors, behavior (communication with doctors and self-management), and health and well-being outcomes after 6 months (T3).
Fourteen paths were significant at the 5% level (red arrows) at T1, T2, and T3: from health literacy to understanding of diabetes care, self-efficacy, communication with doctors, and medication adherence; from burden of medical expenses to emotional burden and HbA1c; from self-efficacy to emotional burden, exercise/diet, HbA1c, and satisfaction with treatment; from emotional burden to communication with doctors and satisfaction with treatment; from communication with doctors to medication adherence; and from HbA1c to satisfaction with treatment.
Regarding the relationships between health literacy and psychosocial factors, a positive path that was significant at the 5% level was found from health literacy results at T1 to understanding of diabetes care and self-efficacy at all three time points.
Regarding the relationship between health literacy and behavior, there was a significant positive path from health literacy at T1 to communication with doctors at all three time points. In terms of the relationship between health literacy and self-management, there was a significant positive path between health literacy at T1 and medication adherence at all three time points.
Discussion
The present study aimed to examine a pathway model based on the framework proposed by Fransen et al., 19 linking health literacy to health and well-being outcomes among patients with type 2 diabetes. This study was the first to empirically examine a conceptual framework linking health literacy, psychosocial factors, communication with doctors, self-management behavior, and health and well-being outcomes among patients with type 2 diabetes.
The model fit index was highest at T1. Although it slightly declined at T2 and T3 with a decrease in sample size, the relationships among the variables in the model were generally comparable across the three time points.
In terms of the relationship between health literacy and psychosocial factors, there were significant positive paths from health literacy at T1 to understanding of diabetes care and self-efficacy at all three time points. A similar positive association between health literacy and understanding of diabetes care has been shown in previous studies, 20 suggesting that higher levels of health literacy correspond to higher degrees of understanding. 22
Regarding the relationship between health literacy and behavior, there was a significant positive path from health literacy at T1 to communication with doctors at all three time points. Similar results have been reported in previous studies, 21 suggesting that health literacy is an important factor in successful communication in doctors’ examinations. This suggests that the ability to properly collect and exchange information such as health literacy leads to a high level of communication ability such as the exchange of information with doctors. 21 In addition, it is thought that good relationships with doctors will lead to further improvement in communication, as it will also lead to patients participating proactively in treatment and decision making. 46 However, the effect of health literacy for a particular patient depends on the complexity of the health information provided to him or her. 47 In addition to their efforts to improve patients’ health literacy, medical personnel should also communicate health information in a way that is easy for their patients to understand.
Concerning the relationship between health literacy at T1 and self-management, there was a significant positive link between health literacy and medication adherence at all three time points. This finding is consistent with previous studies that have examined the association between patient health literacy and medication adherence.48,49 Health literacy is important in improving education and communication, which can increase patients’ understanding of medication adherence. 48 Our findings suggest that improving health literacy may increase medication adherence among patients with diabetes. However, health literacy at T1 was not a statistically significant predictor of exercise/diet at any of the three time points. Previous studies have also indicated that there is no direct relationship between health literacy and adherence to diet and/or exercise therapy,20,22,23,25,31 but that there is a direct relationship between health literacy and drug therapy.48,49
We found a significant strong positive association between burden of medical expenses and degree of emotional burden at all three time points. This suggests that a high economic burden of medical expenses for treating diabetes increases the degree of emotional burden among patients with diabetes—a conclusion that can also be found in previous studies. 19
Regarding the relation between burden of medical expenses and the examined health outcomes, there was no strong relation between burden of medical expenses and medical satisfaction; however, there was a significant positive association between burden of medical expenses and HbA1c at all three time points. Our findings suggest that, if the burden of medical expenses is high, HbA1c also tends to be high. However, careful attention should be paid to the interpretation here because high HbA1c can lead to morbidity and complications and therefore to a high burden of medical expenses (e.g. for treatment and medicine).
An increased level of health literacy may directly improve medication adherence, and health literacy may indirectly influence exercise and diet behaviors by improving self-efficacy. Self-efficacy has a positive effect on self-management for many chronic health conditions.50,51 Self-efficacy theory states that perceived self-efficacy refers to the belief in one’s capabilities to organize and execute the courses of actions required to produce given attainments. 50
It is argued that motivation for behavior change can be attained by enhancing self-efficacy, so that actions such as exercising and eating a healthy diet can be achieved. Furthermore, actions can be maintained by successful experiences of these actions.50,51 A previous study found high self-efficacy to be associated with high levels of self-care behavior, such as exercise and diet, among diabetic patients. 20 The rationale for this association is that the improvement of the sense of self-efficacy is thought to lead to the implementation of actual exercise/dietary behavior changes. We observed a significant positive effect of health literacy on understanding of diabetes care, self-efficacy, communication with doctors, and medication adherence at all three time points. Health literacy might also have had a positive influence on exercise/diet through self-efficacy at the three time points.
The significant effects of health literacy found in this study suggest that efforts to increase proactive behavior on the part of patients will lead to positive self-management behavior,21,30 including medication adherence48,49 and effective exercise and dietary practices, by improving self-efficacy. 20 In addition, improving communication with doctors can increase patients’ ability to collect and exchange high-quality information, which can, in turn, lead to patients’ greater involvement in decision making regarding their treatment.10,12,15,16,38,49
A limitation of this research is that the survey was conducted at only one university hospital in Tokyo. Compared with patients with diabetes who visit general hospitals and clinics in outlying areas, there is a possibility of bias because the participants in the present study represent more serious cases and have higher levels of education. It would be desirable for future studies to consider including larger numbers of facilities and patients. In addition, all indicators used in the survey in this study were based on self-report, which may have resulted in measurement error because of bias in the response tendencies of participants. It would therefore be desirable to conduct future studies using more objective indicators. Finally, although we observed relationships between health literacy and self-efficacy and between self-efficacy and exercise/diet, this does not mean that health literacy has a positive effect on exercise/diet through self-efficacy, because there are other variables that we have not measured that may independently affect both self-efficacy and exercise/diet.
Conclusion
The present research empirically examined the pathway model linking health literacy to health and well-being outcomes among patients with diabetes, based on a theoretical model proposed in a previous study. Our results suggest that health literacy may be indirectly related to patient health and well-being outcomes through psychosocial factors, communication with doctors, and self-management behaviors. The relationships among the variables in the model were generally comparable across the three time points. Further research is needed to investigate whether the results and models of this study can be applied to patients with other chronic diseases that require self-management.
We found significant positive effects of health literacy on understanding of diabetes care, self-efficacy, communication with doctors, and medication adherence. In addition, health literacy might have a positive influence on exercise/diet through self-efficacy. Improving health literacy may lead to better self-management and improved health and well-being outcomes, although the impact of improvements in health literacy may be determined by the relationship between a patient’s health literacy level and the understandability of the information provided. 47 Educational programs focusing on health literacy52,53 should be considered in the future as a means of improving health and well-being outcomes.
Footnotes
Acknowledgements
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Ethical approval
The study was conducted with the approval of the Ethical Review Committee of the Graduate School of Medicine and Faculty of Medicine, The University of Tokyo (No. 10240-(3)).
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This study was supported by JSPS KAKENHI (Grants-in-Aid for Scientific Research: grant number 24390163).
Informed consent
Written informed consent was obtained from all subjects before the study.