
Abstract
Objectives:
Studies of social support in diabetes have focused on the effects of support on the person with type 2 diabetes. We explored diabetes prevention effects of a culturally tailored diabetes self-management intervention in individuals without diabetes who were supporters of intervention participants.
Methods:
This is a secondary analysis of data from a randomized clinical trial that involved 256 Mexican Americans with diabetes. Each study participant designated a supporter—spouse, relative, friend—who attended intervention sessions and assisted participants in attaining effective diabetes self-management. Supporter’s glycosylated hemoglobin (A1C) data were tracked for 1 year to determine diabetes conversion rates in supporters without diabetes at baseline.
Results:
Fewer individuals in the intervention group (n = 9) converted to an A1C above the 7% threshold, compared to the 1-year wait-listed control group (n = 16). We found a statistically significant difference (p = .021) at 12 months in the number of individuals whose A1C was ⩽8%, with fewer supporters above threshold in the intervention group (reduction of 48%). Supporters in the intervention group with prediabetes, based on baseline A1C, experienced a slight reduction in A1C, while control group supporters with prediabetes experienced an increase.
Discussion:
The results suggest that there are potential benefits for family members and other supporters of persons with diabetes who participated in diabetes self-management programs.
Introduction
Hispanics comprise 17% of the US population and are estimated to constitute 28.6% of the nation’s population by 2060, making them the largest minority group. 1 Obesity, the primary precursor of type 2 diabetes (T2DM), is at epidemic levels in the United States, particularly among Mexican Americans, the largest Hispanic subgroup. Among Mexican Americans who reside on the Texas–Mexico border, higher rates of overweight/obesity and lower rates of physical activity have been documented.2,3 “Overnutrition” and a sedentary lifestyle are modifiable risk factors of T2DM as well as for diabetes-related co-morbidities, such as cardiovascular disease.4–6 Culturally tailored diabetes self-management education (DSME) has been successful in improving the health of high-risk minority populations.7–10
Previous studies on social support in diabetes generally have focused on the effects of family support on the person with T2DM. Persons with T2DM who perceive that they have the support of their family members, or at least report fewer obstructive family behaviors, show better medication adherence, weight loss, and glycemic control.11–13 In the case of DSME interventions, supporters who may be family members or friends attend intervention sessions and may be charged with assisting the person with T2DM in recommended lifestyle changes. The health benefits, however, of being a supporter of a family member or friend with T2DM are unclear. Does incorporating supporters into DSME programs prevent or delay diabetes onset in the support persons, who do not yet have T2DM but who are at high risk of developing it?
Since the late 1980s, we have developed and tested DSME interventions culturally tailored for Spanish-speaking Mexican Americans who resided in Starr County, a Texas–Mexico border community that is the poorest county in Texas and one of the poorest in the United States. 14 The interventions, although designed for individuals already diagnosed with T2DM, were similar in some respects to the Diabetes Prevention Program (DPP), which targeted individuals with impaired glucose tolerance (IGT).15,16 In the DPP, the lifestyle arm involved moderate levels of physical activity and a reduced caloric intake; these lifestyle changes resulted in a 58% reduction in diabetes risk. The primary targets of Starr County intervention studies were adult Mexican American residents of Starr County who were already diagnosed with T2DM for at least 1 year. Each study participant was required to recruit his or her spouse, other family member, or close friend to attend intervention sessions and provide support for the behavioral changes required for effective diabetes self-management. Approximately 70% of the support people did not have diabetes but attended intervention sessions with their family members or friends diagnosed with T2DM.
Here, we report the results of a secondary analysis of Starr County data to explore the question of whether DSME has any serendipitous health effects on, or lowers the diabetes risks for, family member or friend supporters who do not have T2DM. The specific purpose of these secondary analyses was to compare experimental and control groups on baseline and 12-month A1C levels of the supporters without diabetes to determine 1-year rates of conversion to T2DM in these individuals who did not have diabetes at baseline but who were at high risk of developing it. This secondary analysis is similar in nature to the DPP study in which persons with IGT were followed for 3 years to determine rates of conversion to diabetes. 15 However, in these secondary analyses, we examined the 1-year conversion rates, a time frame that is adequate for providing information on trends in the data and guidance on whether examining DSME effects on supporters is an important focus for future research and clinical practice. The specific research questions that guided these analyses were as follows:
What were the characteristics (e.g. gender, age, and relationship to the study participant) of the individuals without diabetes who were designated to serve as supporters of DSME study participants?
What were the 1-year diabetes conversion rates, based on A1C, of supporters without diabetes at baseline, comparing experimental and control participants of a community-based, culturally tailored DSME intervention?
Methods
Study design
The Starr County studies involved testing of a culturally competent, community-based DSME intervention designed for Spanish-speaking Mexican Americans diagnosed with T2DM. We used a randomized study design with a 1-year wait-listed control (WLC) group. Due to the fact that the community did not provide any DSME programs at the time, we felt compelled to provide the full DSME intervention for the WLC group, beginning after the 12-month measurement point. In total, 256 individuals were recruited and assigned to one of 32 groups of 8 participants; half of the groups were randomly assigned to begin the intervention and half were wait-listed for 1 year (control). The aims were to examine intervention effects on the primary outcomes of metabolic control (glycosylated hemoglobin (A1C)), fasting blood glucose (FBG)), knowledge, health beliefs, lipids, and body mass index (BMI) at 3, 6, 12, 24, and 36 months. Hispanics value close familial and social relationships, so we emphasized social support by family members, close friends, other members of the individuals’ study group, and members of the intervention teams (nurses and dietitians), as well as the “promotoras” assigned to each group. 17
Community setting
Since 1980, Hanis et al. have conducted investigations in Starr County on the epidemiology and genetics of diabetes and related complications, providing valuable cross-cultural experience and longitudinal data that guided the development of our DSME intervention projects. The research infrastructure that had been in place for many years provided an advantage for conducting intervention studies. Entrance into border communities for research purposes can be difficult to attain and building trust with the community may require many years. A Research Field Office in Rio Grande City, the county seat, was staffed by local residents who were extensively trained for their roles: data collection, communicating with local physicians and their staff, managing intervention logistics, maintaining the on-site clinical laboratory, and collecting clinical specimens. We arranged intervention sites throughout Starr County, for example, Rio Grande City, Roma, La Grulla, and the nearby “colonia,” Las Lomas. “Colonias” are unincorporated communities characterized by poverty and lack of basic resources, such as water and electricity. All of these border communities are similar, with high poverty and diabetes rates and lack of health care access.
Participant recruitment/allocation
The recruitment process has been described in detail elsewhere. 8 In brief, we recruited 502 individuals from lists of the ongoing genetic studies in Starr County, Texas. Half of these individuals (n = 256) were participants diagnosed with T2DM and half (n = 256) were supporters, for example, spouses, adult children, who agreed to participate to support their family members with diabetes. To control for group contamination, subjects were constituted according to the area of the county in which they lived and then were randomized by group to either the experimental or WLC group. A convenient time for intervention sessions was negotiated with each experimental group and project staff provided transportation and childcare, when required. We had high levels of recruitment success; 95% of the invitees participated.
The DSME intervention
The DSME intervention involved 12 weekly educational sessions, followed by 14 bi-weekly support group sessions designed to assist people with overcoming personal and environmental barriers to recommended behavioral changes. The primary lifestyle recommendations involved (1) diets reduced by 500 to 1000 calories per day through portion control, as well as reductions in saturated fat and sodium intake, as prescribed by a dietitian; (2) physical activity of ⩾150 min of brisk walking per week. The intervention also involved guidance on home glucose monitoring, accurate medication self-administration, and community resources available for individuals with limited personal resources. The challenge when fostering healthy eating and increased physical activity in Mexican American populations is to adapt guidelines to cultural norms in order to be effective with this population. The approach we used was culturally competent for language, diet, social emphasis, family participation when possible, and incorporation of cultural health beliefs. 18 Study participants embraced the practical learning activities, such as grocery shopping and food preparation demonstrations directed by dietitians.
Role of supporters in intervention activities
All Starr County interventions targeted family members for support as part of the culturally competent efforts, thereby addressing the major cultural value of a strong interdependence with family. Our previous focus group interviews held in this community indicated that individuals consistently wanted family members involved in order to engender their support for the changes in health behaviors that are required to manage diabetes. We asked each study participant to designate preferably a spouse or first-degree relative who would attend intervention sessions along with the participant. If a family member was not available or willing to participate, a close friend was allowed to serve as a substitute. The only requirement for support persons was that they were 21 years of age or older.
The intervention curriculum involved instruction at each session on how supporters could assist and motivate their family members to improve health behaviors. In total, 30% of the supporters were diagnosed with T2DM, and we recommended that they follow the same guidelines given to the participants with diabetes. We also provided them with free glucometers, strips, and laboratory testing that the participants received. Supporters without diabetes (70% of the total number of supporters), who are the focus of this article, were encouraged to follow recommendations that applied to them, such as diet restrictions and increasing physical activity levels, to prevent diabetes since these individuals were at high risk of developing diabetes in the future (see Figure 1). 19 If the supporter was a family member, he or she was encouraged to assist the participant with family issues related to implementing recommendations, such as grocery shopping and meal preparation. Supporters also were instructed to walk with their family member between sessions and help problem solve regarding barriers to adopting lifestyle recommendations. At data collection sessions, both participants and supporters were provided with laboratory results and at the exit interview, received personalized health recommendations based on their individual laboratory findings. Outcomes were measured for supporters at the same intervals as for the participants. Supporter data were coded separately for those with diabetes versus those without diabetes. This study was approved by the Institutional Review Boards of both universities involved in this study and all participants and supporters provided written informed consent to participate in the study.

Flow diagram of supporters of study participants.
Measures
Due to low literacy rates, language issues, and lack of availability of Spanish-language questionnaires when the initial investigation was conducted, we only used two questionnaires (diabetes-related knowledge and health beliefs). We focused on physiological outcomes as indicators of intervention effectiveness: A1C, FBG, lipids, and BMI. Blood samples (10 mL) were collected at baseline and at post-intervention intervals. FBG (10-hour fasting) was assessed with a desktop glucose analyzer (YSI Model 2300, STAT PLUS Glucose Analyzer; YSI, Yellow Springs, OH). A1C was analyzed at the University of Texas Health Science Center at Houston (Glyc-Affin; Isolab, Akron, OH). FBG and cholesterol testing were performed on site and results were reviewed with each study participant and his or her supporter at exit interviews held during data collection sessions. To track behavioral changes, we developed a checklist, not for analysis purposes but as a behavioral log designed specifically for individuals with low literacy levels. This checklist was used to provide feedback to participants and supporters, and also for intervention team members to use for tracking each participant’s progress and providing individualized guidance.
For the secondary analyses reported here, we focus on one of the primary, and most direct, indicators of behavioral changes aimed at preventing diabetes, A1C levels. We used two thresholds for A1C levels measured at baseline and 12 months later: ⩽7% and ⩽8%. The ⩽7% threshold is based on the national A1C target recommended by the American Diabetes Association (ADA). 20 The ⩽8% threshold was used to account for those supporters who may have had undiagnosed diabetes. Since supporters were not the targets of the DSME study and the intervention was not one of diabetes prevention, the supporters had not been screened for IGT at baseline. Also, given the high A1C levels we have seen and reported in this population (mean baseline A1C = 11.8%), and also for exploratory purposes, local health care providers frequently recommended, and were pleased when patients achieved, an A1C of 8%. So, we set a second A1C threshold at ⩽8% for further analyses.
Data analyses
The data from the parent study had been manually entered into a computer database and the quality of the data had been verified through double-entry procedures. Prior to conducting any analyses, data were screened for accuracy by checking original data against a computerized listing. A further check involved examining univariate descriptive statistics to determine whether all the values were within expected ranges and to determine whether means and standard deviations (SDs) were plausible. For the secondary analyses reported in this article, we used IBM SPSS Statistics for Macintosh statistical software, version 23.0, to conduct descriptive analyses (e.g. frequencies, overall and group means) and to examine group differences at 2 time points (baseline and 12 months) with independent t-test analyses.
Results
As shown in Table 1, ⩾75% of the supporters without diabetes were spouses or daughters; 85% met our target, that is, they were spouses or otherwise related to the study participants, all of whom had T2DM, and therefore, the supporters were at high risk of developing diabetes. There were no statistically significant group differences in baseline characteristics of supporters without diabetes, comparing individuals randomly assigned to the experimental group versus the 1-year WLC group; 78.5% of supporters were female. On average, supporters weighed 176 pounds (BMI = 31.5, SD = 5.9) and were 10 years younger on average than that of study participants with diabetes (see Table 1).7,8
Characteristics of non-diabetic supporters (n = 179).

BMI: body mass index; FBG: fasting blood glucose; SD: standard deviation.
To examine the benefits of participating as supporters in the Starr County study, we show in Table 2 the frequency of individuals whose A1C was below the two thresholds at baseline and 12 months later: ⩽7% and ⩽8%. Note that these data are from individuals who had not been diagnosed with T2DM at baseline, 179 supporters. Comparing non-diabetic supporters in the experimental group with those in the WLC group, the data showed that fewer supporters in the experimental group (n = 9) converted to an A1C above the 7% threshold, compared to the WLC group (n = 16). Although the group difference was not statistically significant at the p = .05 level, the trend in the data was in the preferred direction. We did find a statistically significant difference (p = .021) at 12 months in the number of supporters whose A1C was ⩽8%. That is, we found a statistically significant difference between the intervention and control groups in the number of individuals exceeding the 8% threshold, with fewer supporters above threshold at 12 months in the intervention group. Non-diabetic supporters had a reduction of 48% in the incidence of having an A1C ⩾8% at 12 months. The participant/supporter dyads that achieved the greatest improvements in A1C were the participant/spouse and participant/daughter dyads, in that order; however, these data must be interpreted cautiously since the rest of the dyad categories were much smaller than these two dyads.
Non-diabetic supporters’ A1C threshold at 12 months (n = 178).
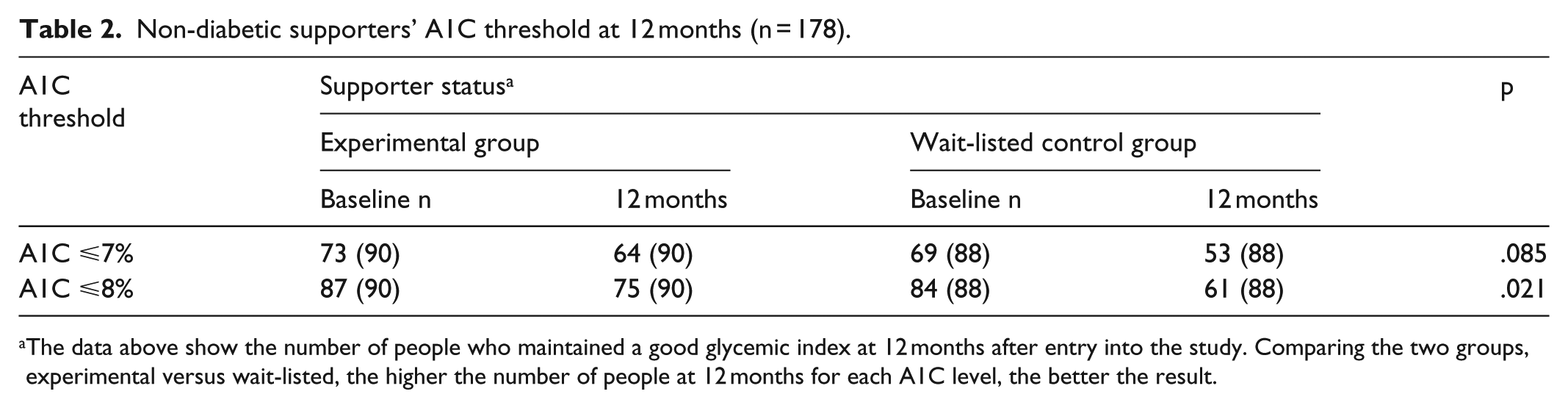
The data above show the number of people who maintained a good glycemic index at 12 months after entry into the study. Comparing the two groups, experimental versus wait-listed, the higher the number of people at 12 months for each A1C level, the better the result.
To explore potential interactions based on the relationship (kinship) between the participant and his or her supporter, we selected supporters in the intervention group and combined relationship categories into related supporters (children/siblings) versus nonrelated supporters (spouses, friends). In other words, this subanalysis was intended to compare those individuals who had a genetic relationship with the supporters to those who did not have a genetic relationship. Analyses found no statistically significant differences between related supporters compared to nonrelated supporters in baseline to 12-month A1C change (p = .35, n = 75). The mean change in A1C was +0.09 percentage point for nonrelated supporters (i.e. a slight increase in A1C), while the mean change in A1C was −0.16 percentage point for related supporters (i.e. a slight decrease in A1C).
To further explore intervention effects on supporters, we examined the 12-month A1C changes that occurred in a subsample of supporters (n = 70; 54 females, 16 males) who fit the criteria for prediabetes (baseline A1C levels of A1C 5.7%–6.4%). The overall mean A1C at baseline of this subsample was 6.1%. By 12 months post-intervention, the mean A1C of the experimental group supporters was 6.2% at baseline and 6.1% at 12 months. The mean A1C of the WLC group supporters was 6.0% at baseline and 6.3% at 12 months. While these differences were not statistically significant, the trends in these data and the potential impact of continued similar annual A1C increases over a longer period of time suggest that these results may be clinically meaningful.
Finally, to examine the mutual impact of support, we compared the supporters of the 20 study participants with diabetes who were most successful in reducing their A1Cs by 12 months (5.0 percentage point mean reduction in A1C) and the supporters of the 20 participants with diabetes who were the least successful (2.5 percentage point mean increase in A1C). There was a statistically significant difference in A1C improvements in their supporters as well, comparing the supporters of the successful participant group (1.5 percentage point mean reduction in A1C) with the supporters of the non-successful participant group (1.3 percentage point mean increase in A1C (p = .019)).
No other variables that were measured, except for diabetes-related knowledge, showed a statistically significant difference between the experimental and WLC groups. For diabetes-related knowledge at 12 months, experimental group participants had significantly higher knowledge scores (p = .007). There was no significant difference in body weight at 12 months between groups (p = .724). Supporter attendance at data collection sessions was consistently ⩾90% and 55.7% of the supporters attended ⩾50% of the intervention sessions. There was no specific dropout of study supporters; individuals attended as many of the sessions as they were able throughout the intervention period and they continued to attend data collection sessions.
Discussion
The purpose of these exploratory secondary analyses was to examine the potential scope of intervention effects of culturally tailored DSME interventions. Any effective DSME program is more clinically significant if it has a positive impact more broadly on the health of family members, and perhaps close friends, of study participants. Although the primary aim of the original DSME studies was to improve health outcomes of Mexican-American participants diagnosed with T2DM, here we wished to explore whether these efforts had any serendipitous preventive effects on supporters without diabetes. These individuals were at high risk of developing diabetes. Lack of access to care and personal resources among US–Mexico border residents posed major challenges to achieving significant A1C improvements in our previous studies. Logically, a superior approach would be to delay diabetes onset or prevent it altogether when possible.
Previous studies have determined that including family members of participants in DSME interventions enhances the positive health benefits of the participants through providing family support.21–23 The results reported here suggest that a diabetes behavioral intervention designed to include family involvement may have an even more widespread effect beyond those singular effects seen with study participants. Although this was a preliminary secondary analysis of data from a randomized clinical trial, the trends in these data are promising. At 1-year post entry into a DSME intervention, we found lower numbers of support individuals whose A1C levels exceeded recommended thresholds, comparing experimental and WLC groups. Furthermore, we found A1C improvements in supporters classified as having prediabetes, as well as a potential link between A1C improvements in successful DSME participants and successful supporters. Other exploratory analyses related to interactions based on the kinship of the supporters, although not statistically significant, found interesting A1C changes based on whether the supporter was related to the study participant or not; and these findings pose interesting questions for future research.
There were several limitations associated with the results reported here. These findings were derived from a secondary analysis of a previously conducted randomized clinical trial on DSME effectiveness in Mexican Americans who were diagnosed with T2DM. The sole purpose of these analyses was to answer the questions “Does DSME have broader effects and potential benefits beyond the glycemic control of study participants with T2DM?” “Can DSME prevent or delay diabetes onset in the non-diabetic family members of study participants who are at high risk of developing T2DM?” In order to begin to answer these questions, the primary focus of these analyses was on a key criterion for diagnosing T2DM, that is, A1C. Beyond A1C, there are many other health-related outcomes that are considered to be important for preventing as well as managing diabetes, such as other indicators of metabolic control (e.g. triglycerides) and key psychosocial outcomes (e.g. self-efficacy and depression). These variables were not included in these analyses. The targeted population was Spanish-speaking Mexican Americans who resided along the Texas–Mexico border in impoverished, medically underserved communities, thus limiting the groups to whom these results might be generalizable. The mechanisms by which these results can be achieved remain unclear and need further investigation.
While these results are preliminary, the findings support the notion that it may be important to incorporate family members in DSME programs and integrate their involvement beyond attendance but as targets of behavioral change as well. Such approaches have the potential for being cost-effective in the long term by preventing diabetes or delaying its onset in these high-risk individuals. Family-based interventions are consistent with Hispanic cultural values and can be implemented in accessible community settings at a fairly low cost. Preventing diabetes in this population that has few personal resources is essential for addressing the growing diabetes prevalence in Mexican Americans, and other high-risk minority groups, wherever they reside.
Footnotes
Acknowledgements
The content is solely the responsibility of the authors and does not necessarily represent the official views of the National Institutes of Health. The investigators thank the study participants and staff of the Research Field Office in Starr County, Texas, for their participation and assistance with this study. The study was approved by the IRBs of The University of Texas at Austin and the University of Texas Health Science Center at Houston.
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Ethical approval
Ethical approval for this study was obtained from The University of Texas at Austin IRB #2001-01-0015.
Funding
This study was supported by grant #DK048160 awarded by the National Institute of Diabetes and Digestive and Kidney Diseases, National Institutes of Health.
Informed consent
Written informed consent was obtained from all subjects before the study.