
Abstract
People with spinal cord injury experience secondary health conditions (SHCs) at a high rate which impacts life expectancy and functional performance. Self-management (SM) is an evidence-based approach to reduce the negative effects of SHCs, but prior SM programs have not been successful for the spinal cord injury (SCI) population. We sought to describe the experiences of participants completing a group-based telehealth program that is tailored to the SCI population: The Spinal Cord Injury Self-Management (SCISM) Program. We conducted interviews using Interpretive Phenomenological Analysis to examine participants’ experiences. Twenty-two participants completed the interviews. Four themes (“A Sense of Community,” “Being Held Accountable,” “I’m Still Learning,” and “Being Proactive Instead of Reactive”) emerged. People with SCI require continued support throughout the chronic stage of SCI particularly at the community level to address mental health as well as the learning and application of SM skills through tailored interventions that foster community and accountability.
Plain Language Summary
People with spinal cord injury (SCI) experience secondary medical conditions because of their injuries that impact their health and quality of life. Self-management is a way to reduce these medical conditions, but prior self-management programs have not been well-liked or successful for people with SCI. We wanted to understand the experiences of people with SCI who completed a tailored group self-management program virtually, called the Spinal Cord Injury Self-Management (SCISM) Program. Twenty-two participants completed semi-structured interviews after completing the program, and we analyzed them. Four themes were generated: A Sense of Community, Being Held Accountable, I’m Still Learning, and Being Proactive instead of Reactive. We found that people with SCI likely need more self-management and mental health support after going home from the hospital through community and accountability.
Introduction
Since the 1980s, individuals with spinal cord injury (SCI) have experienced dramatic improvements in acute survivorship with a 40% improvement in survival rate in the first 2 years (DiMarco & Dawson, 2014). However, a significant disparity in life expectancy continues compared to the general population (National Spinal Cord Injury Statistical Center [NSCISC], 2023). The average life expectancy in the United States is 77.7 years; however, for persons with high quadriplegic SCI, this number falls to 50.9 years, and to 62.7 years for persons with paraplegic injuries (NSCISC, 2023). This significant gap is largely due to secondary health conditions (SHCs). SHCs often result in costly hospital stays, decreased participation in life, limitations in functional performance, and premature death (Cao et al., 2019; Krause & Saunders, 2011; New et al., 2016; Scott et al., 2004; Strauss et al., 2006). This highlights the need for chronic SCI care and SHC management and prevention at the community level.
One evidence-based approach to mitigate SHCs is self-management (SM) which has recently been formally recognized by the American Occupational Therapy Association (AOTA). “Health Management” was added as an area of occupation to AOTA’s Occupational Therapy Practice Framework Fourth Edition in 2020 (AOTA, 2020). Health management is defined as “activities related to developing, managing, and maintaining health and wellness routines including SM with the goal of improving or maintaining health to support participation in other occupations” (AOTA, 2020).
SM reduces emergency department visits, rates of depression, and hospitalizations and improves disease-specific quality of life, physical functioning, and performance in activities of daily living (Brody et al., 2002; Jones & Riazi, 2011; Ory et al., 2013; Rush et al; 2018 Wolf et al., 2017). Barriers such as lack of transportation, limited funding, accessibility, physical and/or mental health complications, and lack of caregiver support and facilitators like discussing with peers and getting information from a trusted health professional or peer have been identified in relation to SCI SM participation (Allin et al., 2018; Conti et al., 2020; Munce et al., 2014). However, little is known about the experiences of persons with SCI participating in a SCI-specific telehealth SM program.
Previously, the authors sought to explore which SM program delivery components and content are most important to the SCI community. Participants expressed that the two most important components of SM program delivery were virtual meetings and working with others with SCI in addition to healthcare professionals (Kraus & Wolf, 2024). Regarding telehealth interventions, a systematic review found that telehealth approaches for chronic disease populations was comparable to, or more effective than, conventional approaches (Rush et al., 2018). There is amounting literature supporting the potential benefits of telehealth utilization for the SCI population to address health-related concerns (Irgens et al., 2018; Mirbaha et al., 2023; Touchett et al., 2022). Literature suggests telehealth interventions may not only be more accessible but may be preferred by the SCI population due to barriers such as transportation, extensive travel exacerbating health complications, limited SCI providers, and inaccessibility (Kraus & Wolf, 2024; Munce et al., 2014). Considering challenges regarding transportation and physical distance, finding peers with SCI can be a challenge at the community level, and telehealth programs may address these barriers.
Despite the creation of gold-standard SM programs, such as the Chronic Disease Self-Management Program (CDSMP), for chronic neurologic populations; the efficacy, attrition, and satisfaction for these programs have been low for those with SCI (Allin et al., 2018; Hirsche et al., 2011; Jaglal et al., 2013; Lorig et al., 2001). Participants reported peer support/feedback, positive outlook, and acceptance as facilitators to SM, indicating that the group component was well received yet they still desired an individualized intervention (Munce et al., 2014). These data indicate that a tailored group SCI SM intervention may be necessary to produce positive outcomes for this population.
In a group-based SCI intervention, Dyck et al. (2021) examined the experiences of an in-person multi-family group education and support program for persons with SCI and their caregivers. They found that passive coping was reduced, and overall social support was higher among the dyads. Participants expressed an enhanced sense of belonging, increased opportunities for engagement, knowledge, and teamwork (Dyck et al., 2021). However, for future implementation of successful telehealth programs, it is critical to understand how stakeholders with SCI perceive group interventions via a telehealth delivery model. Therefore, the purpose of this study was to answer the following research question: “How do individuals with SCI experience and perceive participation in the Spinal Cord Injury Self-Management (SCISM) Program?”
Methods
To understand how participants experienced and perceived participation in the SCISM Program, we used the Interpretive Phenomenological Approach (IPA) and a subsequent thematic analysis to analyze the responses. IPA assumes that individuals are actively engaged in their experiences as self-interpreting beings (phenomenology) and considers the researchers’ interpretation of participant experiences (hermeneutics; Pietkiewicz & Smith, 2014; Taylor, 1985). Interviews were transcribed verbatim to preserve the richness of the data (ideography). As themes emerged, patterns and relationships were identified and described to authentically describe participants’ experiences and our interpretations. Participants consented to participate in this study that was reviewed and approved by the University of Missouri-Columbia’s institutional review board. See Supplementary Appendix A for Consolidated Criteria for Reporting Qualitative Research (COREQ-32) Checklist.
Participants
Participants were recruited from an ongoing study evaluating the SCISM intervention. This study sample included individuals older than 18 years with SCI living in the community who completed a group-based telehealth SCI SM program. Participants were initially recruited for the parent study (n = 32) via email and phone from the University of Missouri Health Care System, social media, and word of mouth and were included if they were over the age of 18 years, living in the community, diagnosed with an SCI, were at least 6 months post-injury, and English-speaking.
The SCISM Program
The SCISM Program (see Supplementary Appendix B) is a 6-week telehealth intervention for persons with SCI facilitated by two occupational therapists (OTs). Three groups of 8–10 participants met weekly, and topics were covered during group sessions related to common SHCs and SM behaviors. Participants created a personalized goal and action plan each week. Participants also completed an individual session with a facilitator each week to address their goals and action plans utilizing motivational interviewing (Rubak et al., 2005; Vansteenkiste & Sheldon, 2006).
Data Collection
We approached participants following completion of the SCISM Program to indicate their willingness to participate in this qualitative study. All interviews were conducted at the University of Missouri via Zoom (Zoom Video Communications, 2023). Participants completed the interviews on their own with an independent member of the research team. Interviews were semi-structured, which allowed for alignment with IPA through variation in question sequence, natural exploration of topics, and expansion upon participant responses as needed until data saturation was reached (Pietkiewicz & Smith, 2014). All interviews were de-identified immediately and kept on a secure password-protected server to protect participant privacy.
Data Analysis
Transcripts of each interview were auto-generated by Zoom, de-identified, and checked for accuracy with the interview audio recording. Cleaned transcripts were then uploaded to Lumivero (2020) NVivo (NVivo 14) qualitative analysis software for visualization and coding (QSR International Pty Ltd, 2020). Braun and Clarke’s (2006, 2021) six-step process for qualitative thematic analysis was the basic structure utilized in analyzing the transcript data.
Data familiarization: Each transcript was read by all three members of the research team, one OT/PhD Candidate and two occupational therapy doctoral students.
Systematic data coding: Authors completed simultaneous initial coding. The authors then compared open codes and reviewed them together to generate coding categories based on similar concepts.
Generating initial themes: Independently, the authors re-reviewed the coded data within the coding categories to create focused codes and create initial themes.
Develop and review themes: These initial themes were then shared among the authors to further delineate the themes as needed to produce clear conceptualized clusters of data.
Naming the themes: The authors then explored each initial theme to further define and label it, using participant’s own words when able.
Report writing: Authors sought to amplify participants’ experiences as well as expand upon the themes and their potential implications within a broader context (Braun & Clark, 2006, 2021).
Results
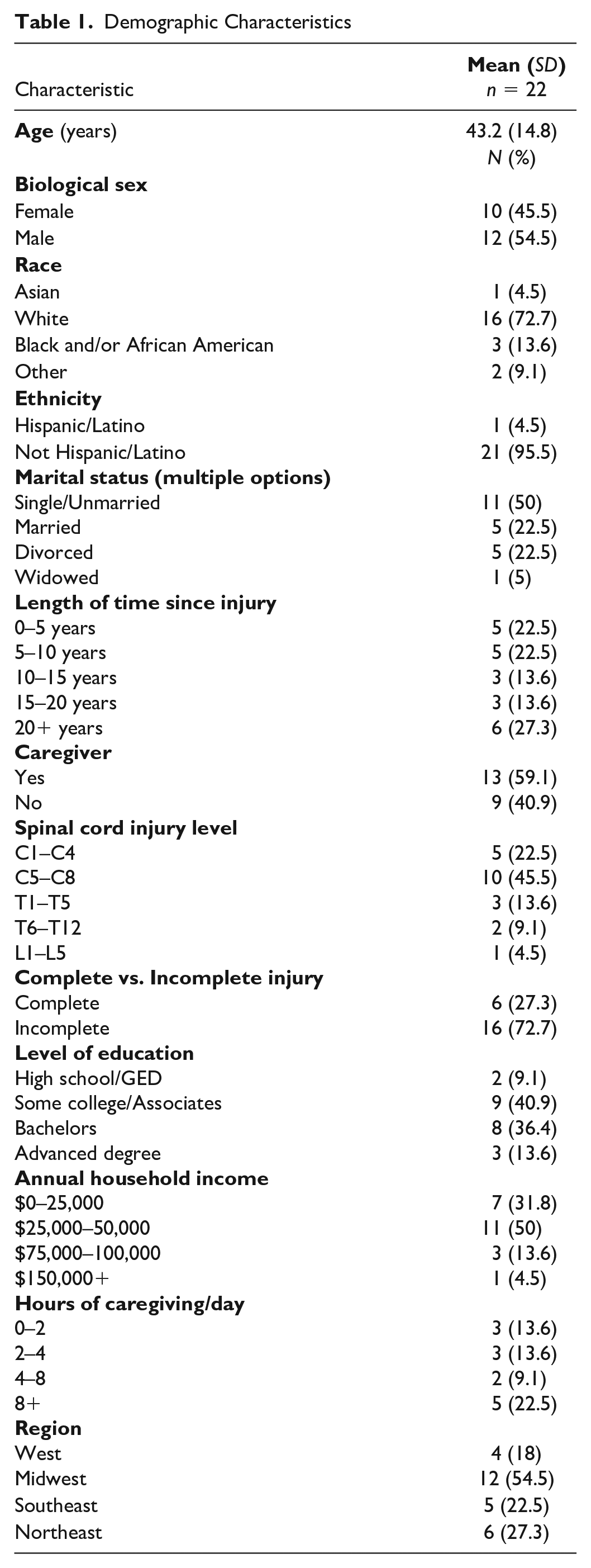
Twenty-two (n = 22) participants completed this study. All interviews ranged from 5 to 28 minutes (M = 13.72 minutes). Most individuals were White (72.7%), male (54.5%), had incomplete SCI (72.7%), and had quadriplegic injuries (78%). See Table 1 for participant demographics.
Demographic Characteristics
Participants reported a range of experiences while participating in the program from initial hesitancy to excitement, emotional support, changes in their perceptions/behaviors related to SM, and feelings of renewed confidence and motivation. Based on their responses, four themes were generated to describe these experiences: (a) A Sense of Community and two subthemes, I’m Not Alone in This and Just Push a Couple Buttons; (b) Being Held Accountable; (c) I’m Still Learning; and (d) Being Proactive Instead of Reactive.
A Sense of Community
Participants felt that the SCISM Program provided them with a sense of community that may be lacking in their physical environment or via social media, “. . . you don’t really see anyone out and about [with a SCI]. So, it’s kind of nice seeing people over Zoom, not just like the Facebook groups I’m part of,” (Participant 16). And “When you’re in like other online groups or what not, like, you really don’t get to see people’s faces you don’t get to see like just their emotions on their face,” (Participant 3).
Participants discussed how this sense of community contributed to their buy-in of the program itself. Participant 22 stated, “I think the community played a very big part in it. Because you not only want the best for yourself, you want the best for others also. So, it’s engaging.”
Because of the group aspect, participants shared that they felt understood and validated in their struggles related to living with SCI and SM. The most common recommendations participants offered for the SCISM Program were to extend the program and create more ways for participants to connect. Participant 10 said, “[I would like to meet] more frequently or just longer . . .. We were all like, ‘Wow, where’d [the time] go?!’”
I’m Not Alone in This
Several participants stated participating made them feel like they were not alone and that they felt supported by their peers, which positively influenced their ability and willingness to address goals. Participants 1 said, “To know that you’re not alone in all the trials and things that you go through . . .. You feel like, you know. ‘Oh, okay, I’m not alone this.’”
Participant 3 said the following: I think the biggest thing that I got out of it was just seeing other people in a similar situation as mine. Understanding that I’m not alone in a lot of the stuff that I go through . . . that meant a lot to me.
These experiences led to participants more freely sharing ideas, suggestions, and help when other group members would bring up barriers to SM and SCI, which overall led to more learning and positive changes. Participants 9 and 14 said, “[The] group setting where you can like bounce ideas off of people and like learn a lot more than just from one person who has one idea and one solution to a problem . . . it makes [plans] a lot easier to implement.” And “I got to meet new people and make new connections. I learned a lot, not just about other people, but about myself.”
Just Push a Couple Buttons
Participants felt the telehealth aspect of the program created this community rather than despite it. Participants expressed that engaging in the program was relatively easy. Most had reported that they had either used Zoom before or that the software was intuitive enough that they did not have issues in learning. Participants stated that participating was achievable regardless of injury/physical function. Participant 1 said, “It was a hundred percent easy. I literally just had to push a couple buttons.”
Being Held Accountable
This theme reflects participants’ sense of accountability as a major contributor to positive changes. Participant 4 stated, “There’s other people to hold you accountable and make you want to do better.” Participants felt working together with peers established a greater sense of accountability for them to address their goals. Participant 18 felt, “[It helps in] making yourself more accountable, maybe because you had people joining you on the journey, not just alone.” Aside from peers, participants stated accountability from facilitators also made it easier to implement new strategies.
Participant 9 noted: Having that constant check-in and accountability, it just makes it so much easier to actually implement these goals . . . a completely like night and day difference between like, how I would actually implement something if I just went to an OT meeting and met with them [once].
Participants discussed how accountability was important to their approach to SM. Participant 4 said, “It makes you feel accountable when it’s written down in writing and like when someone checks up on you.”
I’m Still Learning
This theme relates to learning and internal changes such as improved mood or confidence related to SM. Participants reported an increase in awareness related to SM needs while participating in the program. “The biggest thing that I came away with is just like more awareness about these different conditions or secondary issues . . .” (Participant 9). And Participant 18 shared, “It makes you realize that these things are important, and that no matter how busy you are, it’s important.”
Participants reported SCISM provided a good “refresher” of information. Even those who had the information before felt it was beneficial to receive it again. Participant 4, “During inpatient or like even acute or outpatient rehab, it’s like one of those things where you’re not really ready to listen . . . it’s good to like have a check-in like later on down the line.” For this reason, many participants felt this program could be beneficial at any stage following an SCI, to serve as an education tool of the SM behaviors necessary for those with SCI. Participant 1 said, “. . . we need those reminders on how like we should be doing things.”
Participants reported changes in how they feel about SM and trying new things since being a part of the program. For example, Participant 10 shared feeling confident to do more: “[The SCISM program] actually helped me to speak up a lot more . . . like I’m getting ready to actually talk to my doctors about the pain that I continue to have.” Participant 4 said, “I [reached my goal] the first week . . .. It’s like, ‘Okay well I [accomplished this goal], so why can’t I do something else?’”
Motivation was another commonly discussed topic for participants. Participant 13 said, “[SCISM] really helped kick start my motivation again to really like set forth with my goals . . . [and] be more aware of everything that I’m doing on a daily basis.”
Being Proactive Instead of Reactive
Previous themes were all precursors to the final theme: Being Proactive Instead of Reactive. Participants reflected on how the different aspects of community, accountability, learning, and changes in their own thinking positively impacted them. This allowed for sustainable habit change to take place regarding their SM behaviors because they felt supported, empowered, and prepared to take responsibility for their own health. This sentiment was summed up by one participant, “it’s not about what happens [during] the one hour you’re in the hospital—it’s the other thousand [hours]” (Participant 6). This theme encompasses all external changes and actions participants have taken because of SCISM participation.
During the interviews, participants reported that because of the SCISM program, they started specific habits like working out, utilizing coping techniques, skin care, diet/hydration changes, cooking, stretching, establishing care with providers, participating/socializing in the community, and more. They stated this was in part due to the realization that they could address SM by making small changes. Participant 9, “There’s some like little things that I realized like I could be doing to make things easier, simple things like . . . stretching, or how I you know, deal with pain, or how I check my skin.”
Participants reported that engaging in this program changed their habits, routines, and actions to address their health. Participant 14 stated, “It’s really changed how I do things and when I do things . . .. I care more about taking care of myself than I did.” Several participants said they felt they were now “more proactive,” whereas before, they were “reactive” and waited for problems to arise before addressing them. Participant 1 said, “[I was] kind of more reactive rather than like proactive. Like [I] just did it when there was a problem . . .. I took care of things when I didn’t have any other option.” And Participant 22 said, “Through [SCISM], you’re learning how to prepare beforehand . . .. So now you can schedule it. You can plan for it. You can implement things that you know are coming down the pipeline.”
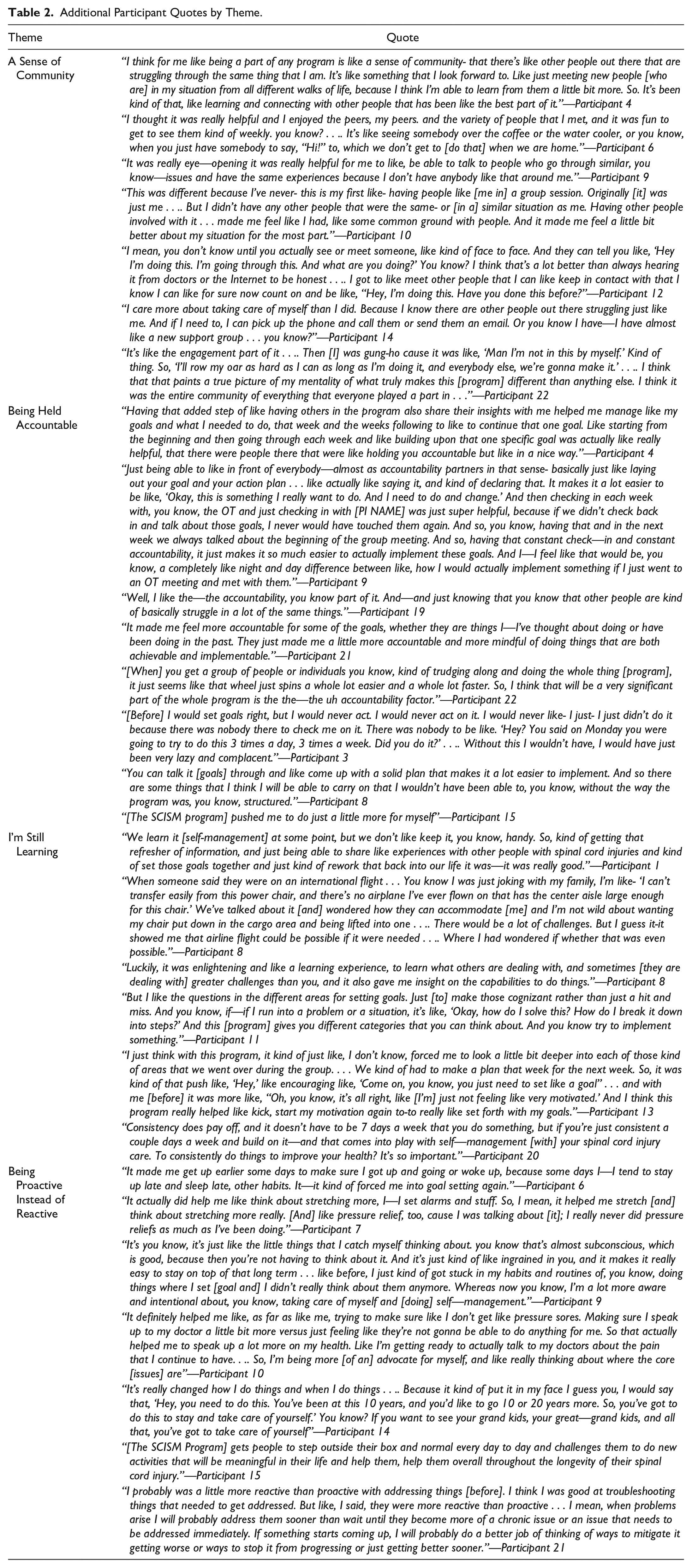
Some stated these habit changes were in part due to the structure of goal setting used in the SCISM Program. Participant 9 said, “It helped me to kind of put structure [to] some things that would help enhance my life.” Participant 4 stated, “I wish I would have [in the past] wrote [goals] down, created the habit—kind of in that step by step, way—create the goal. But the program helped me figure out how to do that.” And this structure spurred participants to check their progress outside of program. Participant 6 said, “I actually reviewed [my goals] the other day, I was doing my own self-assessment.” Participants expressed that not only would they continue with the SM habits but also would continue to build upon them. Participant 22 said, “I will definitely continue the things that I’ve already implemented, but then also add some additionals too.” See Table 2 for Additional Participant Quotes by Theme.
Additional Participant Quotes by Theme.
Discussion
This study sought to understand the experiences of participants who completed the SCISM program through qualitative analysis of semi-structured interviews after program completion. Participant’s responses generated four primary themes: A Sense of Community, Being Held Accountable, I’m Still Learning, and Being Proactive Instead of Reactive.
The theme I’m Still Learning illustrates that learning to live with SCI is a lifelong process. The acute phase after SCI has been described as “a phase of utter confusion and distress,” highlighted by being overwhelmed by their circumstances; being unprepared to receive, understand, or apply relevant information about SCI; and being unable to perceive the value of the information at the time (Conti et al., 2020, p. 5). This may be explained in part by the emotional and physical stress during the inpatient phase of recovery as learning can be compromised when experiencing mental health challenges (Conti et al., 2020). Some participants expressed shock, denial, and confusion during inpatient stays and not being ready to hear SM information at that time. Participants noted the benefits of the SCISM Program timing because they felt more receptive to learning during the program because it was more digestible than that in their hospital stays. This highlights that while education during the acute/subacute phases is necessary, it needs to be revisited throughout the chronic stage of injury when people are ready to learn and are able to apply SM information to their lives.
However, access to this information in the community can still be challenging for those with SCI. For some, geographic location and a lack resources means recovering alone, or with support systems who do not fully understand the impact of SCI. This is why providing accessible programs, like the SCISM Program’s telehealth platform, is imperative to consider. Another consideration is the ability for those to participate with already owned and common technology such as smartphones, tablets, or computers. This allows for reduced costs and physical limitations because it allows for varied participation modalities. Thanks to these features, participants felt that using telehealth was not only easy to use but also fostered the creation of a community. This was echoed throughout the theme A Sense of Community.
Participants expressed that finding a community of peers once returning home can be challenging, but data suggest that peer support and social interaction are critical for positive psychosocial adjustment and wellbeing following SCI (Fekete et al., 2017), which emphasizes the potential benefit and utility of group interventions for those with SCI like the SCISM Program. Several participants expressed making friends with SCI for the first time during the SCISM Program and that they interacted with each other outside of the program, seeking opportunities to foster these relationships because of the positive impact on their lives.
The community and relationships formed during the SCISM Program also contributed to the theme Being Held Accountable, for participants. Accountability aided in participants’ pursuits toward their goals. Because goal and action plan follow-up discussions were built into both SCISM group and individual sessions, consistent check-ins were expected, and as noted in the final theme, Being Reactive instead of Proactive prompted participants to act. In a study of people with SCI who had a peer mentor during the 90 days after discharge, participants were shown to have improved self-efficacy and had significantly fewer unplanned hospital stays after 6 months than those who did not (Gassaway et al., 2017). But it is possible that continued peer support, like in the SCISM Program, during the chronic stages of recovery is necessary to reflect the ongoing nature and psychosocial impacts of SCI at the community level, especially mental health.
Mental Health and SCI
The importance of addressing mental health is lifelong for the SCI population. SHC and mental health have a unique cyclical relationship, making it a critical consideration in all other SM behaviors (Braaf et al., 2017; Munce et al., 2016; Zurcher et al., 2019). When people are experiencing mental health problems, they are more likely to experience more severe SHC, extended hospital stays, decreased social integration, and decreased quality of life (Munce et al., 2016). This highlights that fostering positive mental health and psychosocial adjustment through coping and positive appraisals of injury (Dean & Kennedy, 2009) are not just a necessary component but a foundation to all other SM behaviors, and this was underpinned within each theme.
Building peer support, motivational interviewing, weekly mental health check-ins, and the formal mental health content into the SCISM Program provided frequent, consistent, and repeated opportunities to address mental health concerns. Participants could address these concerns with facilitators as well as peers, which contributed to the subtheme I’m Not Alone in This and positive intrapersonal changes expressed in I’m Still Learning like motivation and confidence. Considering that persons with SCI have expressed that the lack of peer support and psychological counseling are unmet needs upon return to the community, programs such as the SCISM Program may help to fill these gaps, which in turn may positively impact overall wellbeing (Trezzini et al., 2019).
Clinical Implications
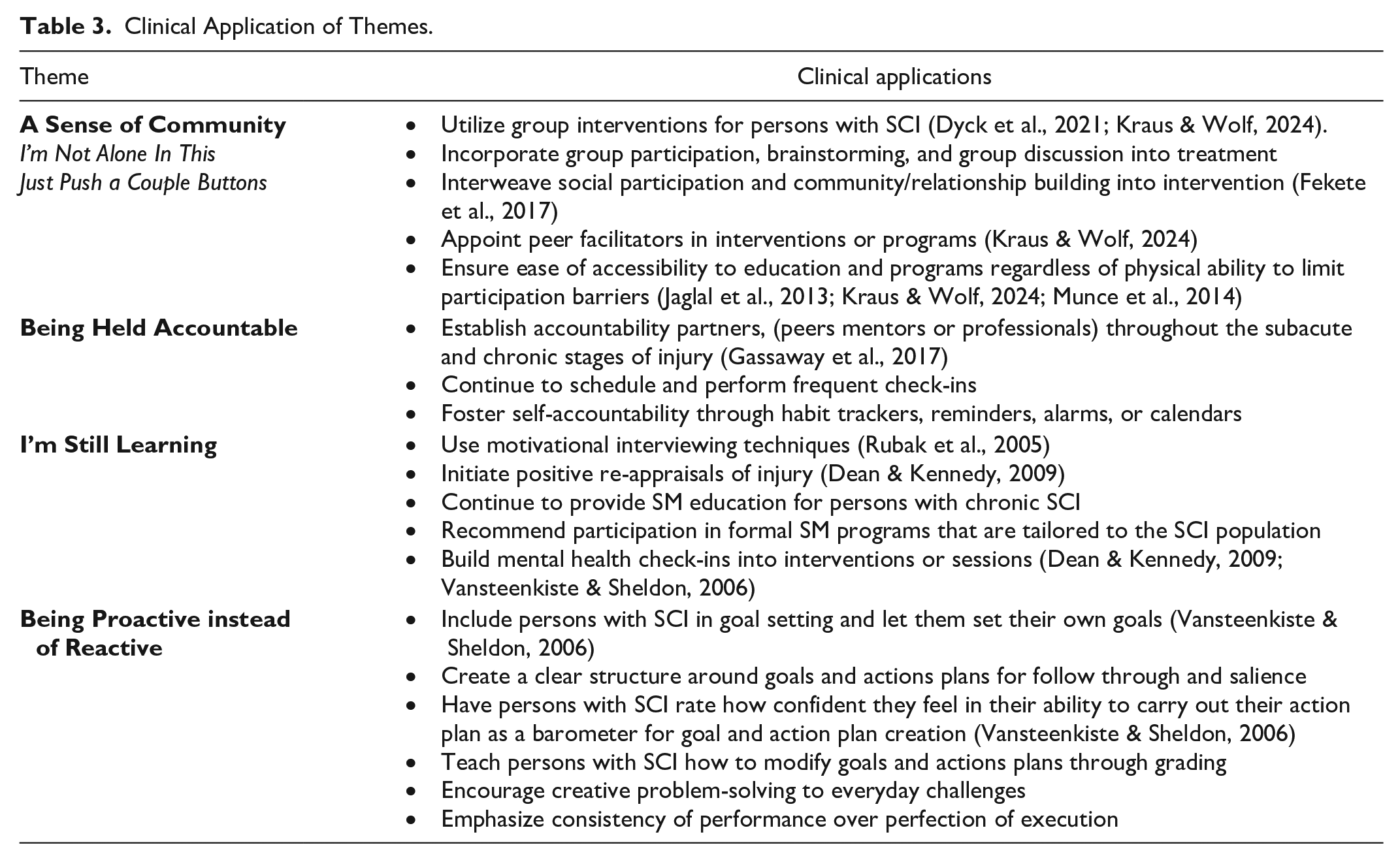
The SCISM Program comes at a time when SM is being formally recognized as an area for OT intervention. Therefore, as data continue to highlight the needs of those with SCI, it is imperative that OT interventions encompass the unique requirements of this population. See Table 3 for clinical application of themes.
Clinical Application of Themes.
Limitations
Some potential limitations with this study include the possibility that those with more openness to telehealth interventions were recruited at a higher rate since recruitment methods included social media and word-of-mouth sampling. Participants were geographically diverse, and while this can be beneficial for generalizability, it can pose challenges in terms of peer-to-peer recommendations due to location differences and what is available in different regions. Also, persons with SCI who are employed may have been disproportionately unable to participate due to the available program times since all groups overlapped working hours in at least one time zone. In the future, offering group times either on weekends or evenings may be beneficial. While most feedback regarding the SCISM Program was positive, participants noted limitations including feeling uncomfortable discussing sex/sexuality, lack of in-person meetups, and wanting more/longer intervention sessions to address topics further.
Conclusion
For individuals with SCI, experiencing SHCs can significantly impact health, functional performance, and quality of life. This study sought to understand the experiences of those with SCI participating in the SCISM Program through qualitative analysis. Four themes were identified following participant’s completion of the SCISM Program: A Sense of Community, Being Held Accountable, I’m Still Learning, and Being Proactive Instead of Reactive. OT practitioners should continue to address SM during the chronic stages of injury when those with SCI are ready to understand and apply the information. Underpinned within each of these themes was mental health. Mental health and SM behaviors are supported when people with SCI are in community with one another, and OT practitioners should seek to incorporate this into treatment approaches.
Supplemental Material
sj-docx-1-otj-10.1177_15394492241260648 – Supplemental material for “The Other Thousand Hours”: A Spinal Cord Injury Self-Management Program Qualitative Analysis
Supplemental material, sj-docx-1-otj-10.1177_15394492241260648 for “The Other Thousand Hours”: A Spinal Cord Injury Self-Management Program Qualitative Analysis by Bridget Kraus, Annie Lakin and Natalie Sherbrooke in OTJR: Occupational Therapy Journal of Research
Supplemental Material
sj-docx-2-otj-10.1177_15394492241260648 – Supplemental material for “The Other Thousand Hours”: A Spinal Cord Injury Self-Management Program Qualitative Analysis
Supplemental material, sj-docx-2-otj-10.1177_15394492241260648 for “The Other Thousand Hours”: A Spinal Cord Injury Self-Management Program Qualitative Analysis by Bridget Kraus, Annie Lakin and Natalie Sherbrooke in OTJR: Occupational Therapy Journal of Research
Footnotes
Acknowledgements
The authors would like to thank the members of the University of Missouri PAWPRINTS writing group, Anne Richardson, Tim Wolf, and each of the individuals who completed the SCISM Program for your contributions to this work.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Ethical Approval
The study was approved as exempt by the institutional review board at the University of Missouri (IRB #2095262).
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: Work is supported by the Missouri Spinal Cord Injuries/Disease Research Program (SCIDRP).
Supplemental Material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.