
Abstract
People with chronic spinal cord injury (SCI) experience a higher rate of secondary health conditions (SHCs) which affect their health and well-being. Self-management (SM) is a proven intervention approach, but formal programs may need to be tailored for the SCI population to reflect their needs and values. We sought to examine the feasibility and acceptability of the Spinal Cord Injury Self-Management (SCISM) Program and estimate its effect. A total of 32 individuals with SCI participated in the program. The primary outcomes were feasibility, acceptability, SHCs, and goal attainment. Participants were assessed at baseline, postintervention, and 3-month follow-up. Findings indicated that the SCISM Program was feasible and acceptable for use with moderate positive effects on SHCs and large positive effects in goal attainment. People with chronic SCI want to continue improving SM skills. The SCISM Program is feasible, acceptable, and should be examined further to reduce SHCs following SCI.
Plain Language Summary
People with spinal cord injuries (SCIs) have more health and medical problems than the general population due to their injury. This can result in poor health and premature death. Learning how to manage your health with SCI, called self-management, is a proven way to reduce this risk. However, most commonly available self-management programs do not address the unique needs of people with SCI. Therefore, programs tailored for people with SCI are needed. We sought to test a new program, the Spinal Cord Injury Self-Management (SCISM) Program, to see if people with SCI liked it and to see if it had any positive effects on their health. A total of 32 people with SCI participated and completed assessments related to mental health, physical health, reaching their goals, and their thoughts on the SCISM Program. Overall, participants liked the program, and there were some positive estimated effects on health and goal attainment. Overall, we should explore the use of the SCISM Program more because people with SCI want to be able to better manage their health.
Keywords
Introduction
Since the 1980s, there has been a significant increase (40%) in survival during the first 2 years after spinal cord injury (SCI; DiMarco & Dawson, 2014). However, there has been no significant impact made on long-term mortality for the SCI population, whose average life expectancy continues to be shorter than the general population in large put due to secondary health conditions (SHCs) associated with chronic SCI (National Spinal Cord Injury Statistical Center [NSCISC], 2023; Cao et al., 2019). For example, an individual in their twenties who sustains any level SCI with an American Spinal Association severity rating of A, B, or C will live 15 to 27 years less than their non-injured peers (NSCISC, 2023). These data highlight the need for ongoing care for the approximate 302,000 individuals living with SCI in the United States after discharge to the community to manage chronic SCI and prevent SHCs that are linked to premature death for the SCI population (Cao et al., 2019; NSCISC, 2023).
The chronic effects of SHCs following SCI have far-reaching and significant impacts on an individual, their family, and on the health care system. Most SHCs that lead to death, decreased quality of life (QoL), limited participation, and costly medical intervention are often well-documented, preventable, and treatable (Cao et al., 2019; Chan et al., 2013; Richards et al., 2004; White et al., 2017). A person with a high cervical injury in their twenties is, on average, going to incur nearly $6 million in lifetime health care costs; approximately $1.3 million in the first year and an excess of another $228,000 annually (NSCISC, 2023). Even for individuals injured later in life, for example at 50 years old, $3.2 million in medical expenses will incur. This cost also does not include any indirect costs for the individual associated with SCI such as lost wages, productivity, and fringe benefits, which is an average of almost $89,000 per year (NSCISC, 2023). A major contributor to this cost is rehospitalization. A person with SCI has a 30% chance of being rehospitalized each year, often due to SHCs with an average length of stay of 18 days (NSCISC, 2023). Not only does this result in significant financial and systematic burden but also is disruptive to successful engagement in meaningful life activities, community participation, and employment (Braaf et al., 2017; Piatt et al., 2016).
Persons with SCI are at a higher risk of developing SHCs compared with the general population, and according to prior research, the greatest risk factors for several secondary conditions, for example, urinary tract infections (UTIs), pressure sores, respiratory complications, and pain, are quadriplegic injuries, higher body mass, traumatic lesions, complete lesions, and aging with SCI (Haisma et al., 2007; Richards et al., 2004). The length of time since injury, age at the time of injury, etiology, and biological sex do not affect the likelihood of experiencing SHCs such as pressure ulcers, spasms, pain, UTIs, bowel dysfunction, circulation issues, and sexual dysfunction (New, 2016). The presence of one SHC can often lead to cyclical symptoms, the emergence of more SHCs, and have implications across several life domains. This is therefore essential for occupational therapy practitioners (OTPs) to consider addressing through intervention at the community level.
Self-Management and the SCI Population
One intervention proven to reduce these negative impacts of chronic diseases is self-management (SM). For chronic conditions, community-based SM programs and interventions have evidenced success (Allin et al., 2018; Grady & Gough, 2014; Hirsche et al., 2011; Lorig et al., 2005). However, gold-standard programs, such as the Chronic Disease Self-Management Program, have produced little success or satisfaction for those with SCI (Hirsche et al., 2011). This could in part be because SCI is a unique population whose SM needs may differ from that of other chronic disease populations and therefore require an individualized SM program.
To further explore the noted limitations with traditional SM programs for SCI, a cross-sectional survey was conducted to better understand the needs of persons with SCI for an SM program prior to program development (Kraus & Wolf, 2024). Participants responded to items using a Likert-type scale and input free-text responses. Participants also responded to a needs ranking for both program content and delivery. Participants indicated that the most critical aspect of an SCI SM program is incorporating psychological health and coping strategies and delivering the program via telehealth (Kraus & Wolf, 2024). Prior literature also states persons with SCI have greater engagement when information is presented by a peer or trusted health care professional, is discussed in groups, and that interactive telehealth platforms are well received in the SCI population (Allin et al., 2018; Newman et al., 2019). Due to the heterogeneity within the SCI population, it is important to consider individualization in goal setting related to SM. The results of this study clearly indicated the need for a new SM program that addresses mental health, includes a group aspect, and is virtual.
Telehealth for the SCI Population
Since the start of the Coronavirus pandemic in 2019, telehealth practices have surged. According to a recent study evaluating telehealth implementation for persons with neurological conditions, telehealth is not only becoming more accessible but is also well received by both clients and practitioners (Signal et al., 2020). For persons with SCI, a telehealth self-management program could be beneficial in reducing barriers related to transportation/transportation cost, psychological factors, lack of local resources/specialists and peers, SHCs exacerbation because of travel, and physical barriers to engagement (Kraus & Wolf, 2024; Munce et al., 2014). To address the severe impact of SHCs on individuals with SCI, this study was designed to fill a gap in current literature to assess the use of a tailored self-management intervention for the SCI population and to (a) determine the feasibility and acceptability of the Spinal Cord Injury Self-Management (SCISM) Program and (b) estimate the effect of the SCISM Program intervention.
Method
Research Design
This single-group quantitative pilot study assessed the feasibility and acceptability of the SCISM intervention with the SCI population and estimated the preliminary effect of the intervention. The Institutional Review Board of the University of Missouri, Columbia, reviewed and approved this study. Informed consent was obtained from all participants in this study. Participants were asked to virtually complete a baseline assessment battery (T1), the SCISM Program, post-assessment (T2), and follow-up assessment (T3) 3 months after the end of the SCISM Program.
Participants and Recruitment
This study took place at the University of Missouri in Columbia, MO. A convenience sample of participants was identified via word of mouth from local rehabilitation facilities, online, and from the University of Missouri Health Care System via email and phone. Participants were screened via telephone and included in the study if they were at least 18 years of age, had a documented SCI (traumatic or non-traumatic), were at least 6 months post injury, able to understand and speak English, and living in the community. Participants were excluded if they were living in a skilled/assisted nursing facility or had sustained their SCI less than 6 months prior to time of intervention. Potential participants (100) were contacted; n = 32 were included in the study, n = 8 were screened and did not meet study criteria, n = 25 did not respond to our initial contact attempt, n = 24 did not respond to follow-up contact, n = 7 were not interested, and n = 4 were interested but unable to attend group times due to scheduling. Participants were also removed from the study if they were unexpectedly hospitalized as an inpatient during the intervention period. Participants were scheduled to participate in one of three groups depending on availability and to limit the size of any one group (Biggs et al., 2020).
The SCISM Program Intervention
The Spinal Cord Injury Self-Management (SCISM) Program was developed based on previous literature regarding SM barriers and facilitators for persons with SCI, as well as data from the SCISM Survey (Allin et al., 2018; Conti et al., 2020; Hirsche et al., 2011; Kraus & Wolf, 2024; Munce et al., 2014). The SCISM Program consisted of 6 weeks of active intervention. Each week, participants met for a scheduled 2-hr group session via Zoom with two SCISM facilitators who were both occupational therapists. The topics for each week were (a) Introduction to Self-Management and Mental Health; (b) Pain and Spasticity; (c) Skin Care; (d) Diet, Exercise, Upper Extremity Health, and Aging; (e) Bowel and Bladder; and (f) Respiratory Function, Autonomic Dysreflexia, Sexual Functioning and Intimacy, and Advocacy and Resource Finding. Integrated into each group session were opportunities for brainstorming, one-on-one discussion, and active group participation. Each session, participants created a goal and action plan related to that week’s topic and rated their confidence of the action plan. Goal menus were provided to give examples of potential goals, but participants were encouraged to create and personalize their goals. Weekly, participants rated their current goal performance and their satisfaction with their performance to be recorded on the Canadian Occupational Performance Measure (COPM). Participants were asked to share their action plans and discuss them as a group. Each week, participants also met one-on-one with a facilitator via Zoom or telephone. During this session, facilitators performed a brief mental health check in, revisited participant goals, action plans, and discussed potential barriers or questions in a private environment that allowed for more individualization and support from a facilitator.
The PACE Framework
Within occupational therapy, the PACE framework has been developed to enhance effective telehealth implementation in research and clinical practice. The PACE framework outlines four domains necessary for consideration when implementing telehealth and each were utilized to guide development of the SCISM Program (Little et al., 2021). (P) Population and Health Outcomes: Evaluating prior literature and outcomes of previous SM programs for the SCI population was necessary to tailor this intervention for the population based on their needs and values. (A) Access for all clients: It was imperative to ensure that participation in a SM program includes various tech options to account for varied ability and function that exists within the SCI population. For example, minimal typing or touchpoints that could become barriers for clients’ successful participation. This required thoughtful preparation to ensure that implementation of the SCISM program can be utilized via tablets, phones, and/or computers so that users can utilize their most accessible device. It also meant using timetables and choosing group intervention times that would fall during the hours of 7 a.m. to 5 p.m. in every time zone to reduce geographical barriers. (C) Costs and cost-effectiveness: Due to socioeconomic barriers that impact the disability community, and SCI in particular (Walls & Dowler, 2015), we made an effort to ensure that participation in this program could capitalize on resources already owned and used by a majority of the general population such as computers, internet, and smart devices as well as free services such as Zoom and email. Resources were also provided to those who wished to participate but required additional products or services such as a smart device, a computer, a device stand, or wireless internet to reduce financial barriers to participation. (E) Experiences of clients and OTPs: Measures were included to evaluate the experiences of participants (Little et al., 2021). A separate qualitative study was also conducted and published by members of this research team to further evaluate experiences of SCISM Program participants.
SCISM Training and Fidelity
The SCISM Program was facilitated by two occupational therapists. The study team created a robust facilitation manual to enhance fidelity and reproducibility in group and individual session delivery. Facilitators were trained using the facilitation manual before the intervention started and asked to demonstrate proficiency through demonstration of mock sessions. Two occupational therapy clinical doctorate (OTD) students in the University of Missouri were trained to administer the assessment batteries at (T1), (T2), and (T3) as independent raters. They demonstrated proficiency with administration of each assessment (100% accuracy) to ensure fidelity and interrater consensus of scoring.
Measures
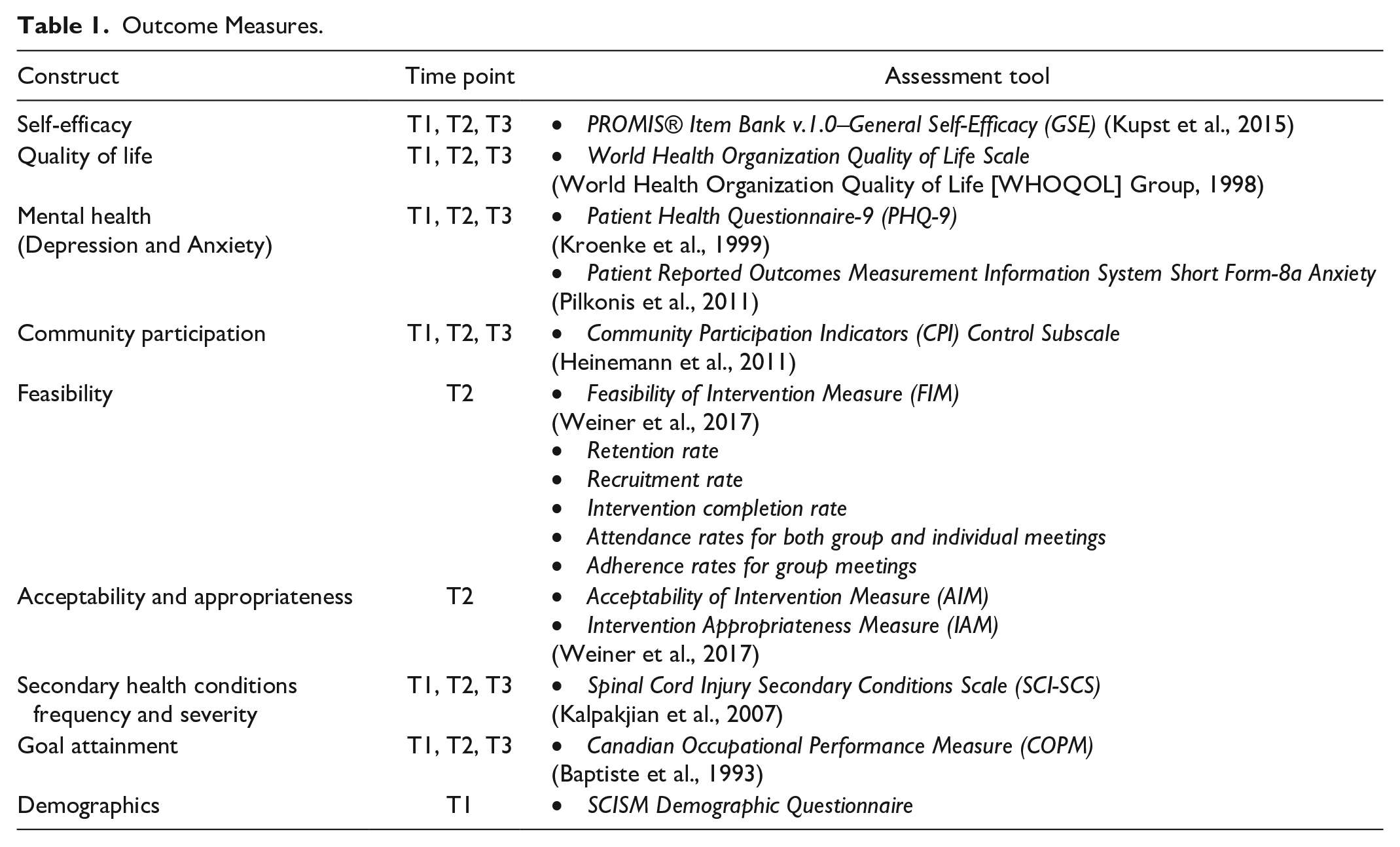
The following psychometrically sound measures (see Table 1) were collected at baseline (T1) before the start of intervention, within 2 weeks before intervention participation, post-assessment (T2), and 3-month follow-up (T3).
Outcome Measures.
Feasibility and Acceptability
The Acceptability of Intervention Measure (AIM), Feasibility of Intervention Measure (FIM), and Intervention Appropriateness Measure (IAM) are four-item Likert-type measures to assess stakeholder beliefs of an intervention’s acceptability, feasibility, and appropriateness. Responses range from 1 (completely disagree) to 5 (completely agree). Higher scores indicate more positive beliefs about the intervention. Depression and Anxiety. The Patient Health Questionnaire-9 (PHQ-9; Kroenke et al., 1999) is a Likert-type scale measure where lower scores (total scores range between 0 and 27) indicate lower depression. The Patient-Reported Outcomes Measurement Information System (PROMIS) Anxiety-8a (Pilkonis et al., 2011) is a short form anxiety measure and lower T-scores indicate less anxiety with a T-score of 50.0 to be considered the normal reference point. General Self-Efficacy. Participants responded to the General Self-Efficacy (GSE) scale (Kupst et al., 2015), where higher scores ranging from 1 to 4 indicate increased feelings of self-efficacy. Quality of Life. The World Health Organization Quality of Life (WHOQOL-BREF; WHOQOL Group, 1998) was utilized to assess quality of life. The WHOQOL-BREF is a Likert-type scale measure ranging from 1 to 5. Higher scores indicate better quality of life. Community Participation. Participants responded to the Control of Participation subscale from the Community Participation Indicator’s Enfranchisement scale (Heinemann et al., 2011). Secondary Health Conditions. The Spinal Cord Injury Secondary Conditions Scale (SCI-SCS; Kalpakjian et al., 2007) is a Likert-type scale measure with total scores ranging from 0 to 48 where participants are asked to rate how much certain SHCs related to SCI impact them. Lower scores indicate less impact from SHCs.
Goal-Attainment Scaling
We used the COPM (Baptiste et al., 1993) to assess goal attainment. Goal attainment scaling (GAS) is a formal approach introduced in the 1960s and includes a 5-point Likert-type scale to score whether a goal has been achieved better or worse than expected by the client (Kiresuk & Sherman, 1968; Turner-Stokes, 2009). In contrast, while the COPM is based on GAS, the client is asked to self-rate goal performance and satisfaction on a 10-point Likert-type scale, with higher scores indicating higher performance and satisfaction. In a study of relative utility, the COPM was found to provide as efficient and consistent individualized outcome measure for GAS (Cusick et al., 2006).
Administration and Scoring
All assessment visits were completed via Zoom with an independent rater. Participants were emailed a link to the research member’s Zoom room to access the assessment visit. To protect participant privacy and confidentiality, all electronic data were stored, and password protected via REDCap, a secure site for managing databases. All physical participant folders and data were secured in a locked cabinet within a locked office, which only the research team had access to.
Statistical Analyses
All data were checked for accuracy and completeness. The distribution of data was evaluated prior to a descriptive analysis with data visualization, skewness, and kurtosis −1/+1 testing. We assessed feasibility, acceptability, and estimated effect sizes for future trials. We accomplished this through calculating retention rate, adherence rate, recruitment rate, attendance rate, and intervention completion rate. Mean scores and standard deviations were calculated for the FIM, AIM, and the IAM (Weiner et al., 2017). Effect of intervention was estimated by calculating domain averages, mean change scores, and standard deviations of all measures and Cohen’s d effect sizes with precision around the estimate.
Results
Participant Demographics
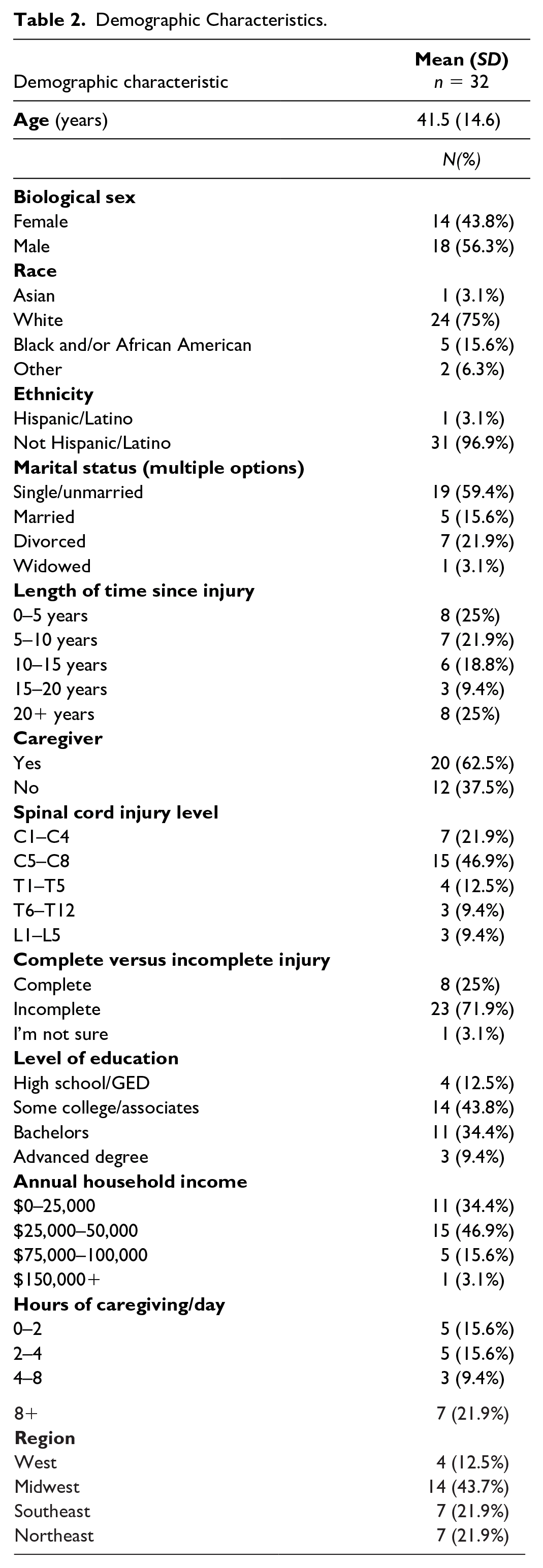
Participants (n = 32) were primarily White (75%), male (56.3%) with an average age of 41.5 (SD = 14.6). The majority had incomplete SCI (71.9%) and had sustained quadriplegic injuries (68.8%). Most participants had also been injured for 10 years or less (46.9%; see Table 2).
Demographic Characteristics.
Feasibility and Acceptability
Rates of Interest
Participants were recruited at a rate of 32% and retention rate from T1 to T2 was 84.4%; T1 to T3 was 81.3%. Of the five participants who did not complete the study, n = 3 were hospitalized during active intervention due to study independent health issues (sepsis, pneumonia, etc.), n = 2 completed the T1 but never attended an intervention session/responded to contact and we assume voluntary withdrawal, and n = 1 participant expired between T2 and T3 assessments. On average, group sessions lasted 110.5 min and individual sessions 38.7 min. 84.4% of participants completed the SCISM Program and adhered to 95.2% of group session minutes (excluding session total absences). The adherence rate includes minutes lost to internet issues, arriving late, leaving early, and family emergencies. Attendance rate for both group and individual sessions was 96.3%. The primary reasons for missing a session were sick (25%), traveling (25%), a previously scheduled health appointment (33.3%), and any other reason (16.7%).
AIM, FIM, IAM
Overall, participants indicated that they felt the SCISM Program was acceptable (M = 4.74; SD = 0.46), feasible (M = 4.64, SD = 0.54), and appropriate (M = 4.69; SD = 0.48). Participants’ responses ranged from 3 to 5 for all measure items.
Intervention Effectiveness Estimation
See Table 3 for further result details. Depression and Anxiety. From both T1–T2 and T1–T3, results indicated a small positive effect of the intervention on depression. There was a small positive effect from T1–T3 on anxiety. General Self-Efficacy. Compared with T1, T2 scores decreased and recovered slightly in T3. These scores indicated a moderate negative impact from T1–T2 and small negative effect from T1–T3. Quality of Life. Physical Health: Scores improved from T1–T3, indicating a small positive effect. There was also a small positive effect from T1–T3 in Environmental Health from T1–T3. When asked to rate their quality of life, participants’ responses improved at each time point and there was a small positive impact from T1–T3. Finally, when asked how satisfied they were with their health, a positive moderate effect was found both from T1–T2 and T1–T3, with improvements from T2–T3. Community Participation. Participants responded to the Control of Participation subscale from the Community Participation Indicator’s Enfranchisement scale (Heinemann et al., 2011). Lower scores indicate feelings of more control over participation. Participants’ scores showed small positive effect from T1–T3. Secondary Health Conditions. From T1–T2, there was a small positive effect. And from T1–T3, there was a moderate positive effect.
Means, Standard Deviations, Effect Sizes, and Confidence Intervals.
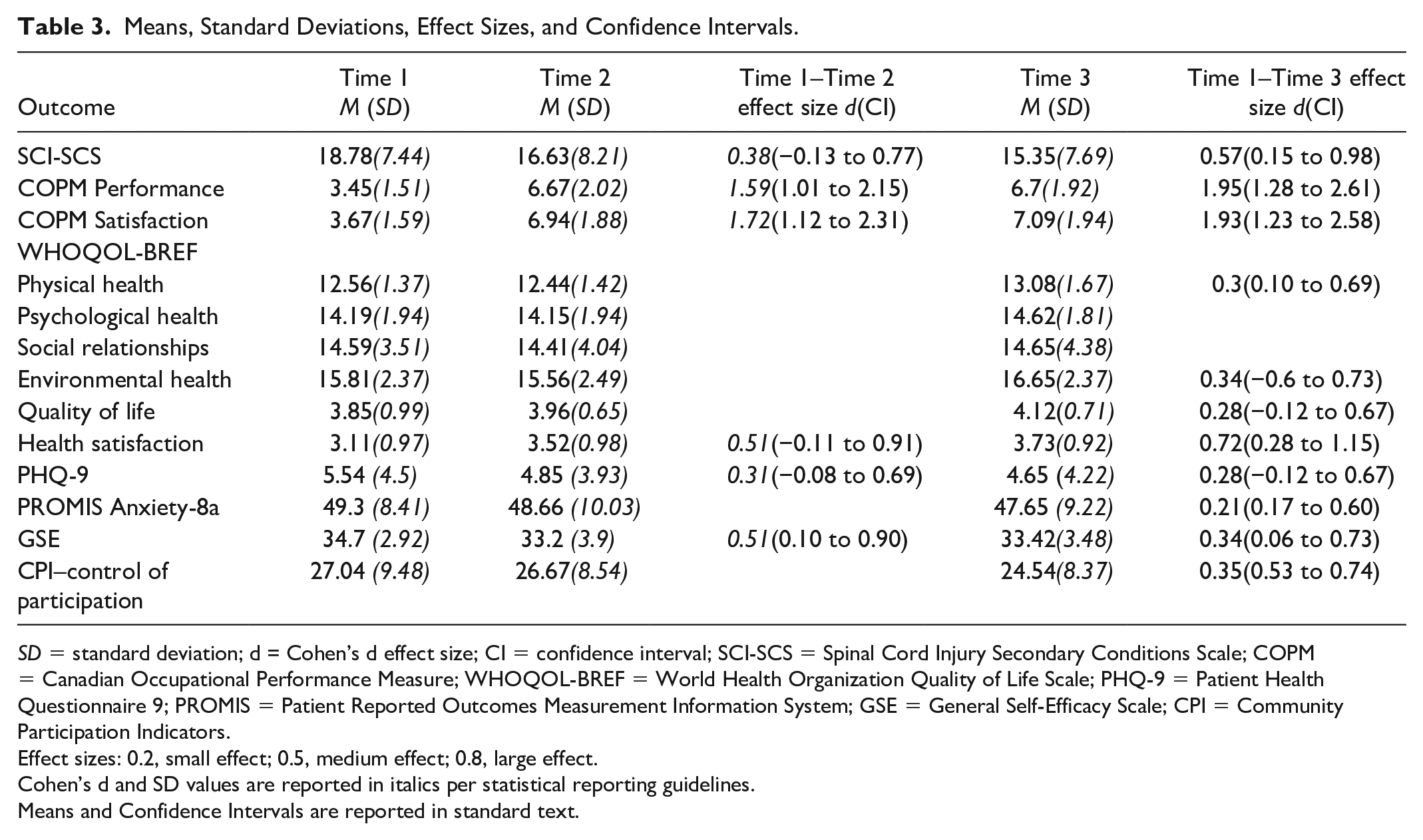
SD = standard deviation; d = Cohen’s d effect size; CI = confidence interval; SCI-SCS = Spinal Cord Injury Secondary Conditions Scale; COPM = Canadian Occupational Performance Measure; WHOQOL-BREF = World Health Organization Quality of Life Scale; PHQ-9 = Patient Health Questionnaire 9; PROMIS = Patient Reported Outcomes Measurement Information System; GSE = General Self-Efficacy Scale; CPI = Community Participation Indicators.
Effect sizes: 0.2, small effect; 0.5, medium effect; 0.8, large effect.
Cohen’s d and SD values are reported in italics per statistical reporting guidelines.
Means and Confidence Intervals are reported in standard text.
Goal Attainment
On average, participants set 5.52 goals during the SCISM Program, with the potential to create 6 (one each week of the program). For performance scores from T1–T2 and T1–T3, both indicated a positive large effect of the intervention. Similarly, satisfaction scores improved. From T1–T2 and T1–T3, there was a large positive effect. See Table 4 for examples of goals set by participants during the SCISM Program.
Example Participant Goals.
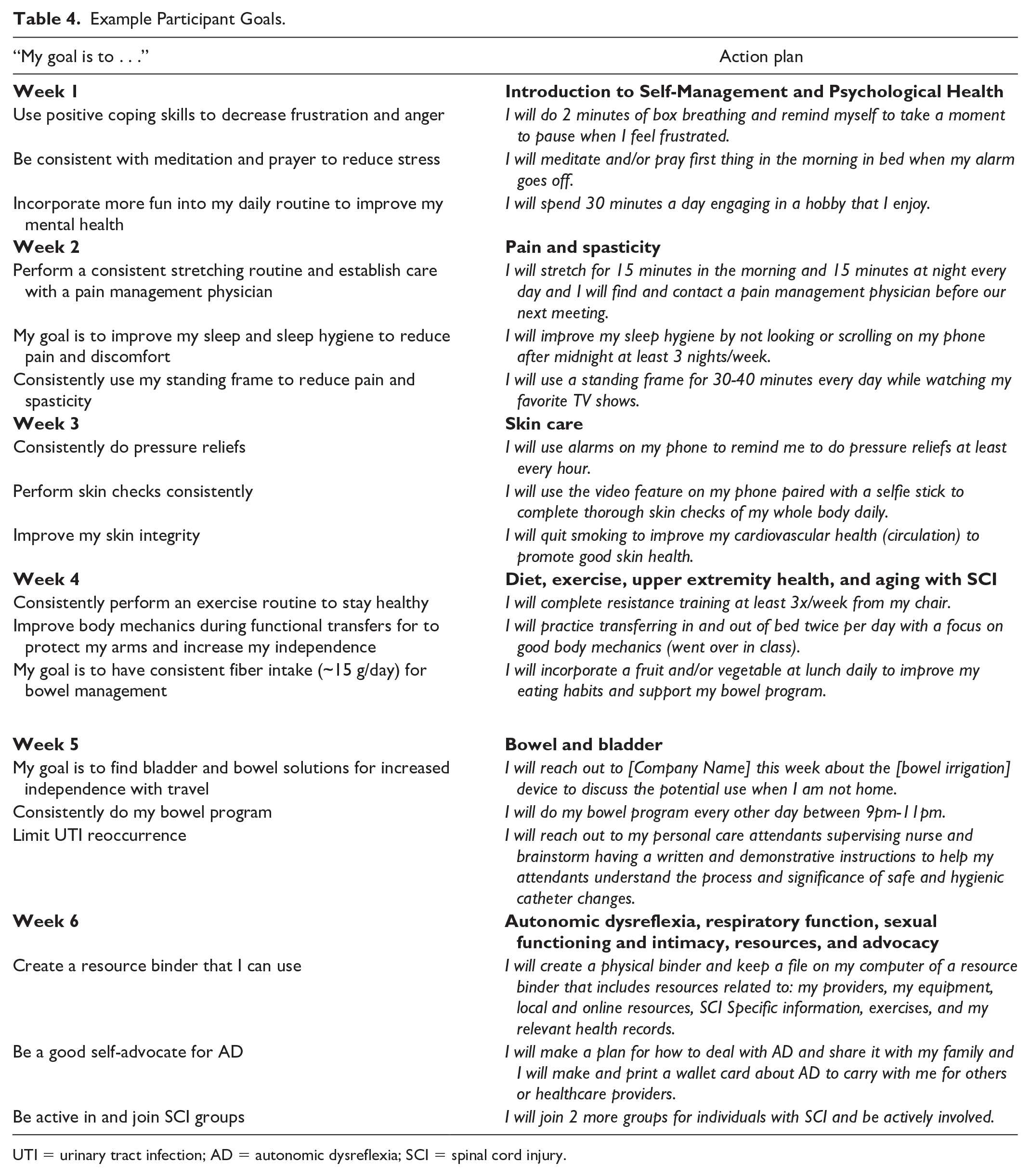
UTI = urinary tract infection; AD = autonomic dysreflexia; SCI = spinal cord injury.
Discussion
Overall, the findings from this study indicate that the SCISM Program is feasible, acceptable, and demonstrated that people with SCI value interventions that address SM in the chronic stage of injury. Most participants (75%) were at least 5 years post injury, 25% of which were 20 years or more post injury, indicating that even people in the chronic phase of SCI were able to benefit from an SM program focused on SHCs reduction. Results from the feasibility measures, acceptability measures, and the rates of interest were overwhelmingly positive. Intervention completion rates were relatively high at the end of the study compared with prior literature. For example, in programs previously piloted for individuals with SCI, intervention completion rates were 50% for an online module-based SM program (Verwer et al., 2016), 68.4% for an in-person SM program (Meade et al., 2016), and 76.92% for a physical exercise–focused SM program (Brawley et al., 2013). The most common reason for withdrawal in this study was hospitalization secondary to health conditions independent of the study. However, this is an important consideration when working with the SCI population due to their high rate of yearly rehospitalization (NSCISC, 2023). Another consideration should be the potential for response shift that may have occurred from pre- to post-intervention.
The phenomenon of response shift is well established within intervention literature, which results from participants’ understanding of a phenomenon at pre-test not being the same as understanding at post-test (Howard & Dailey, 1979; Schwartz et al., 2006; Vanier et al., 2021). Despite improvements in all other areas, it is possible that the introduction of new information and reprioritization of SM behaviors and preventing SHCs during the SCISM Program could have elicited more conservative post-assessment self-ratings of self-efficacy.
One potential method of limiting this effect is re-baselining. According to research, the most appropriate way to do this with minimal risk to validity is to re-baseline immediately following post-assessment and on a separate form (Daniels, 2018; Howard & Dailey, 1979). In studies of self-efficacy related to learning, participants who were re-baselined following completion of a science course, a systematically scored their “pre” self-efficacy lower than their actual baseline ratings upon reflection (Cantrell, 2003; Miller et al., 2023). Researchers suggest that utilizing re-baselining to reduce response-shift bias resulted in greater validity of findings (Howard & Dailey, 1979). In future implementation of the SCISM Program, re-baselining should be utilized to determine whether the decrease in self-efficacy is an accurate representation of participants’ experiences, or whether this was an instance of response shift resulting from a change in understanding of SM, SHCs, and associated behaviors.
Results also indicated that the intervention had a greater effect on goal attainment and health than on participation. While health is a necessary precursor to participation in meaningful activities, there may need to be more deliberate focus on the former for successful engagement. For those who complete the SCISM Program, it may be beneficial to create a secondary program or extend the program to address areas of community and social participation. It is also possible that implementing a tapered dosage of sessions may help to foster the translational impact of health on participation more successfully.
Anecdotally, several participants expressed that they wished the program was longer, and the research team feels the data reflect the possible benefit of increased intervention length or dosage. This was demonstrated through more positive effects at T3 than at T2 across measures. This is potentially due to participants having more time to address their goals, carry out action plans, and experience the results of their efforts. For example, at T2, some goals may have only been set the week prior, leaving little time for action plan modification and execution, let alone the fruition of positive results. To help support participants going forward, tapering additional sessions or providing booster sessions may aid in further SM behavior salience. Related to salience and sustained change over time, it is also important to consider participants’ readiness to change in relation to SM behaviors.
For example, some participants in this study later expressed that they joined to help the other members but were already happy with their own SM strategies and health. This resulted in them making less goals or having difficulty establishing relevant goals and could have resulted in a ceiling effect on their outcome measures. We recognize these individuals would perhaps serve as valuable peer facilitators rather than participants in future program implementation. A possible solution to this is to employ a readiness to change screener.
Readiness to change is the extent to which an individual is primed, motivated, and capable of executing change (Holt et al., 2010). Readiness to change is often evaluated at the organizational level; however, Beasley et al. (2021) identified several scales to assess individual readiness to change. In particular, the Acceptance of Change scale (Di Fabio & Gori, 2016) and Resistance to Change scale (Oreg, 2003) were suitable for use within the context of health care (Beasley et al., 2021). Either one of these measures may be valuable screening tools for participation in the SCISM Program. The SCISM Program seeks to support factors that have positive impacts on readiness to change such as psychological empowerment, which is an intrinsic motivation and a sense of control over personal engagement, and psychological capital, which is comprised of self-efficacy, hope, and optimism (Lizar et al., 2015). This also includes individualized goal setting and action planning to facilitate salience and intrinsic motivation. However, a baseline willingness and openness to change may be necessary for optimal benefit of the SCISM Program to improve SM.
Clinical Implications
The need for SM education and behavior acquisition persists throughout the chronic stages of SCI, highlighting the need for continued services at the community level to reduce the impact of SHCs. It is feasible and acceptable to employ the SCISM Program that incorporates both a virtual group and individual component to address SM. For clinicians working with individuals with the SCI population, consider facilitating continued SM behaviors by recommending programs tailored to the SCI population that meet their needs and experiences.
Limitations
Some potential limitations to this study include that the times offered for group sessions may have disproportionately affected persons with SCI who work full time as all group sessions overlapped with business hours in at least one time zone in the United States. Also, there is the chance that those already with more positive attitudes toward telehealth agreed to participate in this study, missing those who are either unsure or unfamiliar with its use and who could have provided valuable insight. Finally, as participants spanned diverse geographic areas with varying services, it may have affected the utility of peer-to-peer recommendations if their state/town did not offer the same type or quality of resources.
Next Steps
While this study established that the SCISM Program is feasible and acceptable, it is necessary to modify the SCISM Program before a larger efficacy trial is conducted. Future studies need to implement re-baselining in attempts to reduce any effects of response shift which may give a truer sense of change in self-efficacy, will incorporate a readiness to change measure as a screening tool, and will attempt to incorporate a peer-facilitator. Finally, steps will be made to offer group time variations outside of working hours.
Conclusion
Individuals with chronic SCI experience higher rates of SHCs resulting in decreased health and long-term survival compared with the general population. SM is an evidenced approach to improve health and reduce SHCs; however, general SM programs have not been successful with the SCI population. We tested the feasibility and acceptability of a tailored telehealth intervention, the SCISM Program, and estimated its effect. We found that the intervention was feasible, acceptable, and had positive effects on depression, anxiety, quality of life, control of participation, SHCs, and goal attainment.
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This work was supported by the University of Missouri Spinal Cord Injury/Disease Research Program (SCIDRP).
Research Ethics Section and Patient Consent
The study was approved as exempt by the Institutional Review Board at the University of Missouri (IRB #2095262).