
Abstract
This feature article explores how Danish authorities have worked to secure public health in cooperation with citizens, companies, and civil society organizations amid an unfolding pandemic.

On March 11, 2020, the Danish prime minister, Mette Frederiksen, announced extensive lockdown measures to curb the coronavirus outbreak in Denmark. She accompanied the declaration with a plea: We are going to need societal spirit [in Danish, ‘samfundssind’]. We are going to need helpfulness. I would like to thank citizens, companies, organizers, NGOs—everyone who, to this day, has shown that this is what we have in Denmark—societal spirit.
This article explores the co-production of care that unfolded in the Scandinavian welfare state of Denmark in the weeks that followed Frederiksen’s plea. We report findings from a social media analysis, a representative population survey, and qualitative interviews that are part of our ongoing research project on solidarity, voluntary work, and co-production of care during the COVID-19 pandemic.
The concept of co-production refers to modes of governance that encourage cross-sectorial partnerships and expect citizens, companies, community organizations, and NGOs to cooperate in the production of welfare, care, and public health. In contexts like community health care, co-production can mean that volunteers collaborate with professionals and patients to improve service availability, quality of care, or other desired outcomes. Over the last decade, co-production has been an increasingly popular model of service delivery in Denmark and other welfare states across Europe. In times of crisis, the call for co-production is, therefore, unsurprising, and the prime minister thanks citizens, companies, and NGOs for their compliance in advance.
Mobilization of Civil Society in the Co-Production of Public Health
Citizens, companies, and NGOs did organize corona-related care, and our research demonstrates that they did it with remarkable rapidity and geographical spread in Denmark.
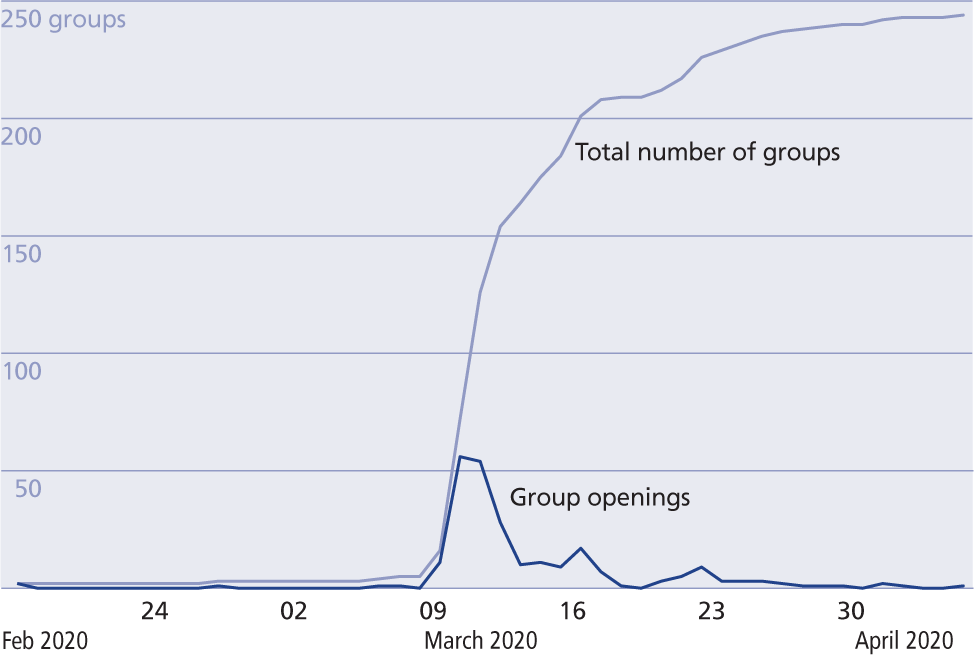
One indicator of the tempo was the rapid formation of corona help groups on Facebook, a social media platform used daily by most of the Danish population. NGOs and private citizens initiated around 250 new groups with the stated purpose of caring for those in need of help during the pandemic (see Timeline for the Formation of Facebook Corona Help Groups).
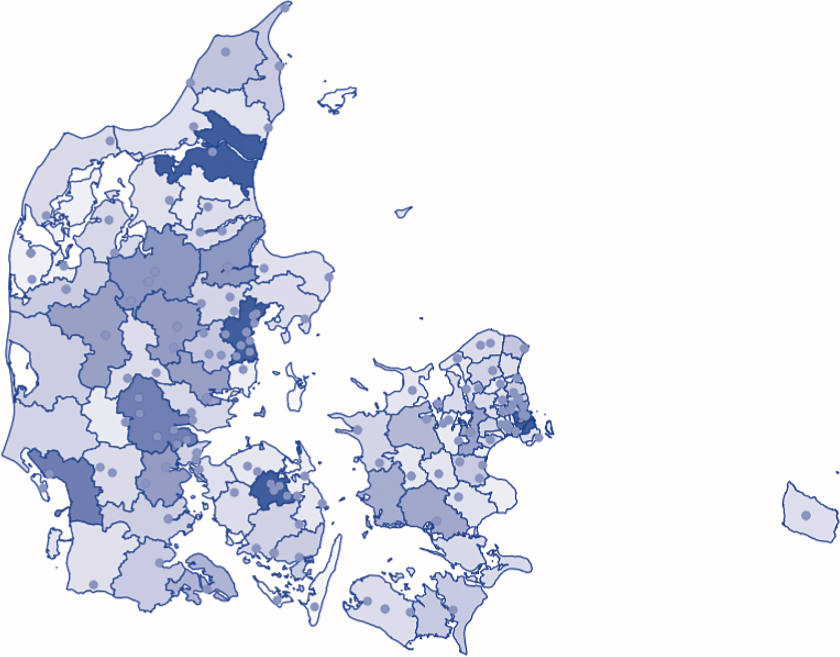
Geographically, the mobilization covered all Danish regions (see The Geography of Corona Help Groups in Denmark), and several hundred thousand (out of a population of 5.8 million) joined a Facebook corona help group.
People also volunteered through other channels, with some measures oriented toward managing the healthcare crisis while others aimed to cope with the secondary effects of the pandemic. An example of the first was the Corona Job Bank, a register in which volunteers with health care skills signed up to help alleviate potential shortages of health care personnel. A few days after the prime minister’s plea, all five regions in Denmark had Corona Job Banks with thousands of registered volunteers (doctors, nurses, and other health care workers).
An example of an initiative aimed at alleviating secondary effects was the Danish Red Cross’s Corona Support Network. More than 10,000 citizens quickly signed up to help people who were quarantined, sick, or otherwise in need of care. The volunteers provided support and practical assistance, such as taking care of groceries, walking dogs, and picking up medicines.
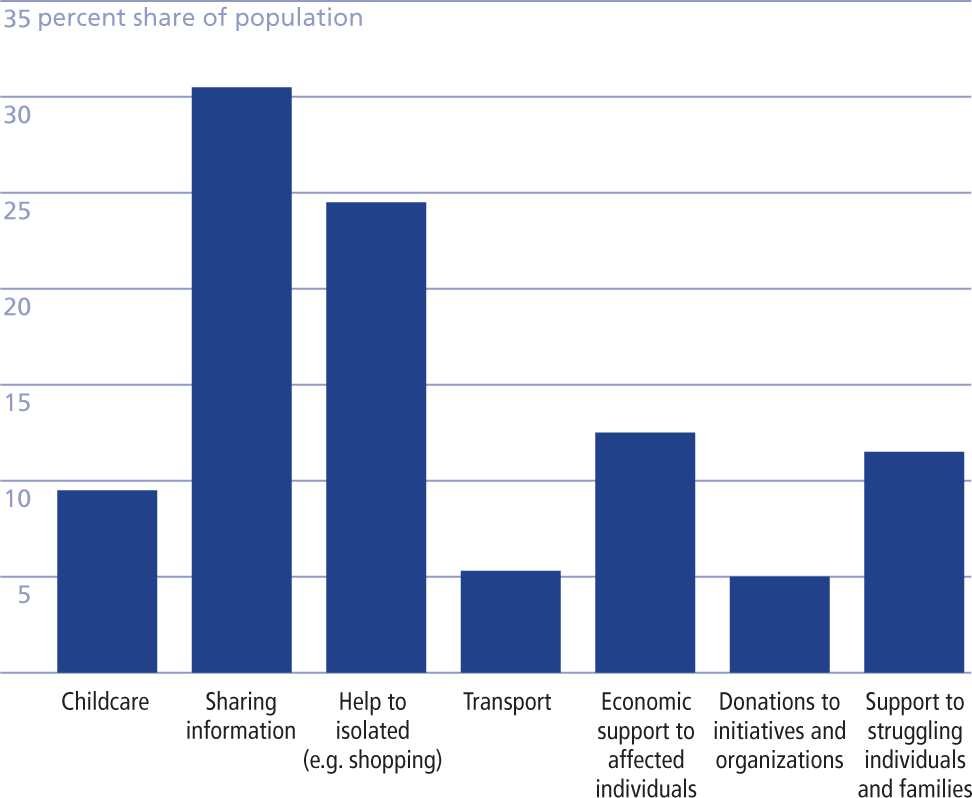
Overall, our research shows that more than half of the Danish population volunteered to help through one channel or another. In a nationally representative population survey, 53 percent of 3,389 respondents report having carried out corona-related aid. The most common way to help was disseminating COVID-19 information; around a quarter of the population report having helped in this way. The second most prevalent form of care was to help people in isolation, which about one in five Danes report having done. Repertoire of Voluntary Help in the Danish Population During the COVID-19 Pandemic illustrates the repertoire of aid types and their prevalence in the Danish population.
Timeline for the formation of facebook corona help groups
Note. N=247. The black line indicates the number of new Facebook groups per day, and the grey line shows the total number of corona help groups. The dotted dropline marks the date of the lockdown announcement (March 11, 2020), while the solid black line marks the start of the lockdown. We used an extensive Facebook search with a national/ regional focus and corona-related search terms (Corona, covid, quarantine).
While informal help was also widely prevalent in Denmark pre-COVID, the types of care reported in our research relate to COVID-19 and indicate an increase in the total sum of support. Our findings are paralleled by the German researchers Sebastian Koos and Ariane Bertogg, who show that the total sum of care activities increased during the pandemic and that a quarter of the helpers mobilized had not been engaged in informal help before the COVID-19 crisis. Hence, COVID-19 sparked solidarity and the willingnessto volunteer in the co-production of care in Denmark.
The geography of corona help groups in denmark
An illustration of the geographical spread of Facebook help groups in Denmark. Blue dots represent Facebook help groups self-reporting a regional attachment. The map displays municipality borders; dark blue indicates high population density, light blue indicates low.
Trust, Collaboration, and Social Mobilization in National Responses to COVID-19
Several factors facilitated the rapid mobilization of Danish citizens, companies, and NGOs in the co-production of care. First, collaboration requires mutual trust, and Denmark has a long history of a high level of generalized trust. Second, volunteering is familiar; about one-third of the Danish population are routinely involved in organized voluntary work. Third, the rapid mobilization of society requires structures geared to support cooperation.
In Denmark, one example of a key structure is “the Danish model,” in which unions and employers routinely negotiate labor market regulations. As soon as March 16, the Danish state entered the first of a series of agreements with employers and unions to avoid mass layoffs and bankruptcies. This kind of cooperation reduced citizens’ fear of layoffs and enabled (in combination with a relatively generous level of cash benefits to unemployed citizens) people to stay home if they experienced symptoms, thereby reducing risks of spreading the virus.
It seems likely that “the Danish model” and the high degree of generalized trust helped make civil society into an agent of co-production and cooperation instead of one of opposition and resistance. In Denmark, very little contentious anti-government protest happened in response to the lockdown policies. In our extensive Facebook search for COVID groups in the spring of 2020, we found only a handful of protest groups compared to more than 200 in support of authorities. Civil society broadly endorsed and encouraged compliance in response to public health needs as defined by the government and health authorities. In the Facebook corona help groups, the government’s guidelines to stop contagion were an omnipresent part of the discourse.
By October 20, 2020, the number of deaths and the case fatality rate remained very low in Denmark in an international comparison (cf. the COVID-19 pandemic worldwide monitoring, Johns Hopkins University). The high level of generalized trust, familiarity with voluntary work, and consolidated models of cooperation between labor market parties appear to have (so far) helped Denmark reduce the virus spread. While these factors make a difference, we should not overstate the importance of national characteristics. According to sociological research on pandemics by Dingwall, Hoffman & Staniland, “Emerging diseases provoke common reactions, which are only slightly modified by national environments,” and the capability to co-produce is not innately linked to Danish society. Denmark is neither the first nor the only welfare state to encourage co-production in response to the threat of pandemics. In China, for example, local social mobilization has played a crucial part in reducing the spread of the coronavirus, and in the UK, more than a million have volunteered to help the National Health Services (NHS) and others during the COVID-19 outbreak.
The high level of generalized trust, familiarity with voluntary work, and consolidated models of cooperation between labor market parties appear to have (so far) helped Denmark reduce the virus spread.
Repertoire of voluntary help in the danish population during the COVID-19 pandemic
Note. N=3,389. Data collected by Statistics Denmark April 3-May 11 using a mixed-mode survey design (CAWI/CATI) and a random sample of 7,964 individuals aged 16-99. 3,389 respondents (42.6 percent) completed the questionnaire. Results are weighted by socioeconomic status, gender and age. Respondents can help in more than one way, so the sum exceeds 100 percent.
Altruistic Superbloom or ‘Imposed Voluntarism’
The American author Rebecca Solnit has described the global spread of mutual aid groups in the wake of the coronavirus as “a superbloom of altruistic engagement.” While we share the hope that something good grows out of the crisis, we also want to draw attention to two critical concerns.
First, replacing state-sponsored care with voluntary help undermines the right-based care that is particularly important for vulnerable citizens. The Danish lockdown included a withdrawal of some forms of state-sponsored care. While volunteers and NGOs rapidly mobilized, they did not reach all citizens in need. The importance of a social network in voluntarism is well-documented by previous research, and our findings confirm that the transformation of state-sponsored care to voluntary aid makes a network paramount. The survey reveals that a personal network by far facilitates the majority of help, and an estimated 64 percent of the care mobilized during the pandemic spring was organized through networks. Citizens who depend on state-sponsored care and lack social networks are vulnerable, as their needs are difficult for NGOs to see and satisfy.
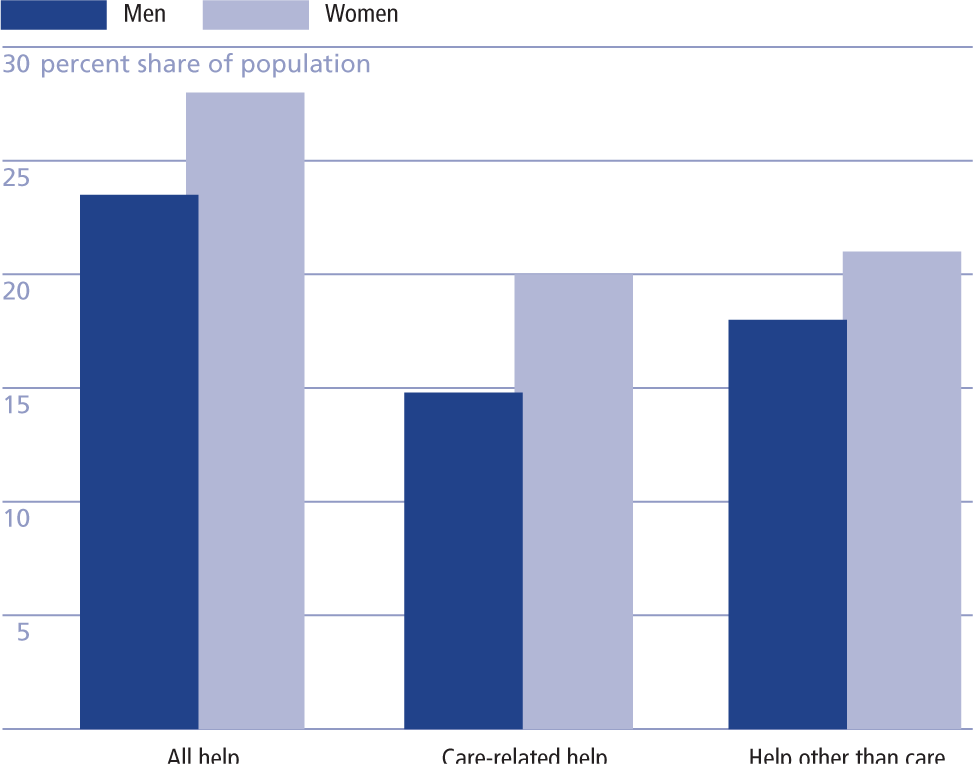
Second, burdens of care work are often distributed in ways that reproduce social inequalities in societies. In Denmark, as in many other societies around the world, women routinely do the majority of voluntary, unpaid care work, and this was also the case during COVID-19 (see Gender Distribution of Voluntary Help in the Danish Population Aged 16-99). While gender bias is clear, it is not evident whether the gaps are reduced in the context of state-led co-production. As authorities called attention to the value of care work, sociologists may expect the heightened status to make more men volunteer. We do not have the comparative data that allows us to investigate this hypothesis, but what our research can document is that women in Denmark provided significantly more unpaid care work than men during the pandemic overall and that the gender bias increased if we focus on care-related help.
Gender distribution of voluntary help in the Danish population aged 16-99
N=3,389. For data source, see note to the figure above, Repertoire of Voluntary Help in the Danish Population During the COVID-19 Pandemic. Results were weighted by gender “Care-related help” includes Childcare, Help to isolated, and Support to struggling individuals and families. “Help other than care” refers to Dissemination of information, Transport, Economic support, and Donations. The differences are statistically significant (p<.05).
In 2020, sociologist Sophia Woodman discussed the importance of local mobilization in the Chinese COVID-19 response. In China, females also do most of the unpaid care work, and Woodman remarks:
While official discourses around the community being a “big family” can be seen as the authorities taking advantage of neighborliness—enlisting gendered forms of unpaid care in the service of the state—I witnessed instances in which the committees were important in mobilizing help for residents facing health and family crises.
We want to argue that the two ways of viewing the care are not mutually exclusive: Authorities may take advantage of gendered forms of unpaid care in the service of the state while the mobilization at the same time is important for people experiencing the urgent crises.
We found this duality reflected in the qualitative interviews we conducted in our research. Several volunteers described experiences of being compelled to provide vital help to people whom they knew one way or the other. For example, one woman explained how an elderly relative suffering from dementia was left without state-sponsored care during the lockdown, and the awareness of this made her feel obliged to provide “voluntary” care. She did not feel she had a choice. As she put it: “Of course one could just be an asshole, but I think that there are things you simply have to do.” Another woman explained that her regular paid care work as a home counselor for vulnerable citizens was suspended during the lockdown, and she was directed to other care work. However, her regular clients still needed help, and she started to visit them again on a “voluntary” basis—defacto working two care jobs. She was exhausted “but did it anyway” due to a sense of obligation and a “responsibility toward my job and care for the citizens.”These women conveyed experiences that we conceptualize as “imposed voluntarism.” They volunteered to care, but they felt they did not have much of a choice.
Summing up, our research shows, on the one hand, that the pandemic revealed a widespread readiness in the Danish population to participate in the co-production of care. In this way, COVID-19 may be seen as strengthening solidarity. On the other hand, the pandemic exposed how the transferal of state-sponsored care to voluntary care reproduces gender inequalities and leaves the most vulnerable citizens without the care they need.
Footnotes
Funding
This research was supported by the Independent Research Fund Denmark (Grant number: 9038-00038B/PI: Ditte Andersen, and 0213-00028B/PI: Jonas Toubøl and Hjalmar Bang Carlsen) and the Faculty of Social Science, University of Copenhagen. Jonas Toubøl’s research was supported by the Carlsberg Foundation (grant number: CF17-0199)