
Abstract
Over 5000 epilepsy-related articles are indexed annually, posing a challenge for clinicians to stay updated on all relevant research. Clinical Practice Guidelines (CPGs) are vital tools for translating evidence into practice and promoting equitable, high-quality care while addressing practice variations. This review examines CPG applicability for epileptologists, emphasizing the nuances between primary and specialty care, addressing disparities, and comparing guideline usage in the United States and internationally. CPGs are utilized differently across specialties. General practitioners often manage initial epilepsy cases guided by first-seizure and new-onset epilepsy guidelines. Specialists, dealing with complex cases like treatment-resistant epilepsy, face challenges as guidelines may lag behind emerging therapies. Yet, evidence shows specialists heavily rely on CPGs to ensure optimal care. The use of race in medical algorithms highlights disparities, with examples like race-based adjustments in glomerular filtration rate calculations raising equity concerns. While frameworks exist to reduce biases, ongoing monitoring and inclusive approaches are critical. Globally, CPG implementation varies. The UK's centralized system integrates cost-effectiveness analyses, while the United States adopts a decentralized approach prioritizing clinical efficacy. Emerging technologies, such as electronic medical records and clinical decision support systems, improve CPG adoption and patient outcomes. Success stories like the “Get with the Guidelines” stroke program illustrate the potential of structured CPG frameworks. However, challenges persist, such as inconsistencies in epilepsy guidelines for acute seizure management. Ultimately, bridging the gap between evidence and practice requires rigorous, inclusive guideline development, effective communication, and proactive implementation strategies tailored to diverse healthcare systems.
Introduction
Over 5000 articles related to “epilepsy” are indexed annually on PubMed (https://pubmed.ncbi.nlm.nih.gov/). Clinicians cannot read every potentially relevant article to maintain familiarity with all epilepsy research; various tools (including Epilepsy Currents) assist epileptologists in maintaining a high practice standard. Clinical practice guidelines (CPG) are a systematic translation of research findings into clinical practice and are thus an important way to ensure that the benefit of advances in healthcare reaches individual patients. Knowledge translation also helps reduce the risk of iatrogenic harm and limits unnecessary costs to healthcare systems. 1 Guidelines can reduce practice variation—discrepancies in clinical decision-making within and between providers for comparable patient scenarios. By reducing practice variation, guidelines can support the equitable delivery of high-quality care while improving costs of care overall. 2 Yet, for epilepsy and other complex, highly individual chronic medical conditions, clinicians must consider guideline use in the full context of care. This review will highlight particular considerations for epileptologists in terms of guideline applicability, addressing disparities, use in the United States versus internationally, and changing clinical practice.
Clinical Practice Guidelines: Primary Versus Specialty Care
In primary care, CPGs shape annual wellness visits with recommended preventative screenings and immunizations. One barrier to the effective implementation of guidelines in epilepsy is a perception of a lack of applicability to subspecialty care. Although guidelines may be used differently by specialists and subspecialists compared to general practitioners, guidelines have important implications for all clinicians.
Distinctions in Guideline Use Patterns Across Specialties
Generalists typically face initial management decisions. By definition, these decisions address common scenarios in clinical practice. For example, about 10% of the population experiences a single seizure, 3 and about a third of these go on to develop epilepsy.3,4 Most new-onset epilepsy is initially managed by primary care doctors, who will rely on first-seizure guidelines,5,6 and new-onset epilepsy guidelines. 7
Approximately a third of people with epilepsy will develop intractable disease 8 ; these patients typically make up the largest patient subgroup in a subspecialist clinic. While there are established guidelines describing medical management of treatment-resistant epilepsy,7,9 these guidelines are almost always, by nature of their rigorous development process, 1 step behind the most recent literature on several of the newest antiseizure medications. Thus clinicians, in particular subspecialists, are often faced with scenarios that go beyond the commonplace majority; eg individuals who have tried all the established antiseizure medications and for whom novel therapies, that may not be addressed in the current clinical guidelines, should be considered.
Nonetheless, many subspecialists also encounter new-onset seizures. Likewise, subspecialists only see intractable epilepsy patients after identification and preliminary management by a generalist, during the many months before a referral visit can be obtained. Thus overall, both generalists and specialists have a broad spectrum of cases that we are required to manage.
The idea that guidelines are not applicable to subspecialists is contravened by current literature. Investigators at the Mayo Clinic in Rochester surveyed prescribing clinicians in family medicine, general internal medicine, and cardiology, at the main campus and at 2 community sites. 10 Of 617 prescribers initially invited, the final analysis included 250 responses, 38% of whom were specialists. Respondents were asked to rate their level of agreement on a scale of 1 to 6 with a series of statements about variation in clinical practice and the use of guidelines. The study found no significant differences in the use of clinical guidelines by specialty. In fact, on average, specialists expressed the strongest dependence on practice guidelines for optimal care and the greatest agreement that clinicians should encourage patients to follow guideline recommendations for diagnosis and treatment. 10 In addition, several clinical guidelines primarily address subspecialty needs, including guidelines for the use of functional magnetic resonance imaging (fMRI) to lateralize language and memory functions and to predict postsurgical language and memory outcomes, in patients with intractable focal epilepsies, 11 and consensus-based expert recommendations such as the special report on the diagnostic utility of invasive EEG monitoring. 12 These guidelines can help avoid over- or under-utilization of important tools in the epilepsy specialist's armamentarium.
Contravening Guidelines in Generalist or Specialist Care
Every patient needs management that is applicable to their own clinical situation. Yet, not every clinical scenario can be covered by the guidelines. For example, generalists will often use the recommendation to avoid valproate in people with childbearing potential to limit the risk of multiple adverse outcomes. 13 Nonetheless in a clinical case where other medications have been tried and failed to control seizures, and pregnancy is not desired, discussion with that patient may reveal that valproate may be the best solution. Importantly, a lack of access for an individual or a community does not mean recommendations should be ignored; appropriate guidelines should be pursued, and if necessary, healthcare policies should change to recognize the standard of care. 14
In cases where a clinician believes that following guidelines would cause a patient more harm than good, the following ethical obligations have been proposed
15
:
Clinicians should be self-aware and transparent—acknowledging to ourselves and others areas where our own cognitive biases may color our perception of developments in medical knowledge. Clinicians should also respect patient autonomy, involving them in the decision-making when they so desire, and accepting the possibility that a given patient may weigh the risks and benefits of specific interventions with a different lens than that of the clinician. Clinicians should communicate a clear rationale verbally and in documentation.
Observing these practices will help to ensure that any deviation from current clinical guidelines is appropriate for the patient and reflects the best use of resources.
How Do Clinical Practice Guidelines Affect Health Disparities?
Guidelines and algorithms should aim to ensure that all patients receive appropriate care. However, some clinical decision-making tools incorporate assumptions or “corrections” based on patient race, raising concerns about their impact on healthcare disparities and demanding careful consideration.
The use of “Race” in US medical practices dates back to the era of slavery, rooted in unfounded assumptions that biological differences are determined by race. For example, patients with darker skin were subjected to increased radiation doses based on the assumption that black individuals have denser bone and thicker skin. 16 Similarly, a blood pressure medication was developed and marketed specifically for patients who self-identified as black. 17 These 2 examples reveal the potential harm and perpetuation of stereotypes generated by race-based medicine.
Race is a social construct that may be associated with health outcomes due to a complex interplay of ancestry, socioeconomic, structural, institutional, and cultural influences, demographic variables, and other unknown determinants. 18 The uncertainty surrounding the use of race as a variable in medicine is exemplified by the similar distinctive use of Ethnic groups such as Latine/x or Hispanic in medicine, which can encompass individuals of multiple races. Nonetheless, it is clear that the use of race can have valid social implications in health outcomes and should be reported as such in all research.
To better explain biological differences, some groups have advocated for the use of ancestry in medicine instead of race and avail the use of polygenic risk scores and methylation risk scores. These approaches have to be used carefully to understand the limitations of ancestry and the current limited data on diverse ancestry. 19 In addition, clear explanations and interactions with social/environmental factors as well as changes in these factors over time have to be considered.
The controversial use of race in clinical algorithms gained significant attention with the publication of “Hidden in Plain Sight: Reconsidering the Use of Race Correction in Clinical Algorithms” in 2020. The article highlighted multiple examples of race-based corrections in clinical medicine and their potential negative impact on health equity. 20 Notable examples include the Vaginal Birth after Cesarian (VBAC) risk calculator, which can decrease black mother's trials of labor and pulmonary function test adjusted by race leading to misclassification of COPD in black patients. The most prominent and debated was the use of race to estimate glomerular filtration rate (GFR), based on unsubstantiated assumptions about increased creatinine due to muscle mass in black individuals. This practice may cause delayed referral to a kidney specialist and delay listing for transplantation. 21 In response, the National Kidney Foundation and the American Society of Nephrology convened a task force that looked at 26 equations for calculating GFR. Their final recommendation was to adopt the CKD-EPI (chronic kidney disease epidemiology collaboration) equation without the use of race aiming to promote equity in care. 22
To minimize harm, the Office of Civil Rights under the Affordable Care Act has established protections against algorithmic discrimination in healthcare which applies to all clinical tools. 23 Additionally, the Agency for Healthcare Research and Quality examined the use of race and ethnicity in healthcare algorithms to assess their effect. They focused on 2 areas: the outcomes associated with race algorithms and the effectiveness of design to mitigate bias in algorithms. The findings revealed that algorithms can mitigate, perpetuate, or exacerbate racial disparities, with their impact heavily influenced by the intention behind their design and implementation. 24 A guiding framework proposed by Chin et al provides a structured process to prevent disparities. 25 Successful implementation of algorithms requires comprehensive guidance and training for clinicians, a strong emphasis on dissemination, and ongoing monitoring of outcomes. Artificial intelligence can play a key role in monitoring efforts, helping to ensure that the use of algorithms promotes equity and minimizes harm. The caveat is that machine learning algorithms are also subject to bias and require the same rigor in development and scrutiny upon implementation.
The use of algorithms in epilepsy care will continue to grow, and monitoring the intentional use of race will be crucial. Many examples highlight topics that still need to be addressed. These include establishing clear guidance on the use of race when assessing the risk of adverse drug reactions with carbamazepine in populations with possibly increased HLAB-1502 allele frequency. The current guidance is vague, may not include all patients at risk, and could inadvertently exclude some. Additionally, it is important to supervise the use of race in neuropsychological testing during presurgical evaluation and follow outcomes to prevent bias. Fortunately, we are not alone in our aim for health equity in algorithms but will have to remain vigilant to prevent unintended inequities for people with epilepsy. 26
How Are Guidelines Used in the United States Versus Internationally?
CPGs are increasingly used worldwide to guide quality medical practice and inform practitioners, patients, and healthcare system decision-making. There are significant differences in guideline development and use among countries, affected by different healthcare systems, regional and local policies, and cultural differences. 2 Some countries like the United Kingdom (UK) have national processes coordinating guideline development and use, whereas many countries like the United States have a decentralized approach. Each approach has its own strengths and limitations.
Guideline Development and Use in the United States
In the United States, there is no national coordination for guideline development. Funding for guideline development comes from a variety of sources, 27 and multiple bodies, including professional societies (eg American Epilepsy Society), government-funded organizations (eg Centers for Disease Control and Prevention), and private national, regional, and local organizations (eg National Comprehensive Cancer Network, hospitals and healthcare systems) are involved in guideline development. 27 Trustworthy guidelines are developed using structured frameworks. 28 However, different organizations use slightly different methodologies, which can result in heterogeneity in the quality of guidelines and recommendations, and even conflicting recommendations for identical clinical scenarios. This might also create decision-making complexity for local organizations, impeding guideline implementation. 29
Cost-effectiveness analyses are important to inform decision-making in healthcare, for public policies as well as individual patient care. 30 However, cost-effectiveness analyses are not consistently integrated into the process of guideline development in the United States, which has a stronger emphasis on clinical efficacy and safety rather than economic consideration in guidelines and payers’ decisions. 31 This approach may be more flexible, incorporating new treatments and technologies in clinical practice, even though at a higher cost.
Implementing guidelines requires changes at multiple levels, facing potential barriers. Without a centralized healthcare system in the United States, guideline implementation can be inconsistent, and impacted by geography, healthcare systems, practitioner preferences, and insurance coverage. 29 In addition, resource limitations impeding guideline use can result in inequity in access to care for patients.
Guideline Development and Use in the United Kingdom
Guideline development in the United Kingdom is coordinated through national processes. In England, the National Institute for Health and Care Excellence (NICE) within the National Health Service (NHS) is an independent public body that, in collaboration with professional associations, develops CPGs across the system to improve health and social care through the NHS. 32 As in the United States, guideline development in the United Kingdom adheres to a structured process, as described in a regularly updated manual. Guideline topics are selected in collaboration with NHS to reflect national health priorities. Healthcare professionals, patients, advocates, and the public can be registered stakeholders with the opportunity to comment on the draft guidelines. This can facilitate guideline dissemination and implementation following the development. Patients and caregivers are directly involved in the guideline development process as stakeholders in the United Kingdom. 33
The NHS has a finite budget and a mandate to care for the whole population. Therefore, unlike in the United States, NICE integrates cost-effectiveness analyses into the guideline development process to ensure resources are focused on interventions that are both effective and cost-effective. 34 National processes for guideline development and implementation support more standardized care across the United Kingdom. To address health inequalities, NICE also provides specific recommendations for disadvantaged subgroups with socioeconomic or geographical barriers.
Guidelines Use in China and Japan
In China, CPGs are developed by different organizations, including professional societies, or are adopted from existing international guidelines. 35 Lack of a structured framework for guideline development, suboptimal reporting, minimal engagement from stakeholders, and industry funding may result in variability in guideline quality and implementation. In Japan, guideline development and updates are performed by academic societies and research groups, with government initiatives, and are supported by public funding. Although patient involvement and methodology have improved, expert involvement and implementation remain challenging. 36
Despite recent advancements in the frameworks to develop trustworthy guidelines, no international standards are uniformly accepted across countries and organizations. A better understanding of the barriers and facilitators for guideline use across different healthcare systems is essential to develop quality, useful, and adaptable guidelines.
Do Guidelines Change Practice and Outcomes?
CPGs are decision-making tools developed by expert clinicians and methodologists using rigorously synthesized evidence. However, whether these recommendations—or simplistically put, words—translate into action and bring the desired outcomes depends on several factors. Some are related to the CPGs themselves, and others lie in the hands of policymakers and their intended end users.
Creating CPGs That Promote Adoption
Improving CPG adoption depends on 2 key areas: content creation and communication. 37 Overall, ensuring quality and clarity lays the foundation for CPG's success. To enhance uptake, CPGs must be developed by unbiased experts who consider all stakeholder perspectives, including end-users. The evidence synthesis should be transparent, reproducible, and methodical, balancing the timeliness, quality, quantity, and consistency of the evidence with stability over time. Conveying a considered judgment that accounts for complex trade-offs of benefits and harms, alternate options, clinical applicability, and values of patients and care providers enhances real-world adoption. The feasibility of CPG implementation should be deliberated during the development phase, considering resource constraints and the novelty in behavior change it requires from the practitioner and the patient. Effective communication is critical. The language should be unambiguous, written in short sentences, and ideally in bullet points. CPGs should be simple by limiting the number of elements or conditional factors within each recommendation. In addition, persuasive language that highlights potential improvements over past practices fosters organic adoption. CPGs should also be formatted in various versions, with visualization and components tailored according to the intended user of the information, eg, lay language version for patients or brief guides for clinical use.
Facilitators of CPG Implementation
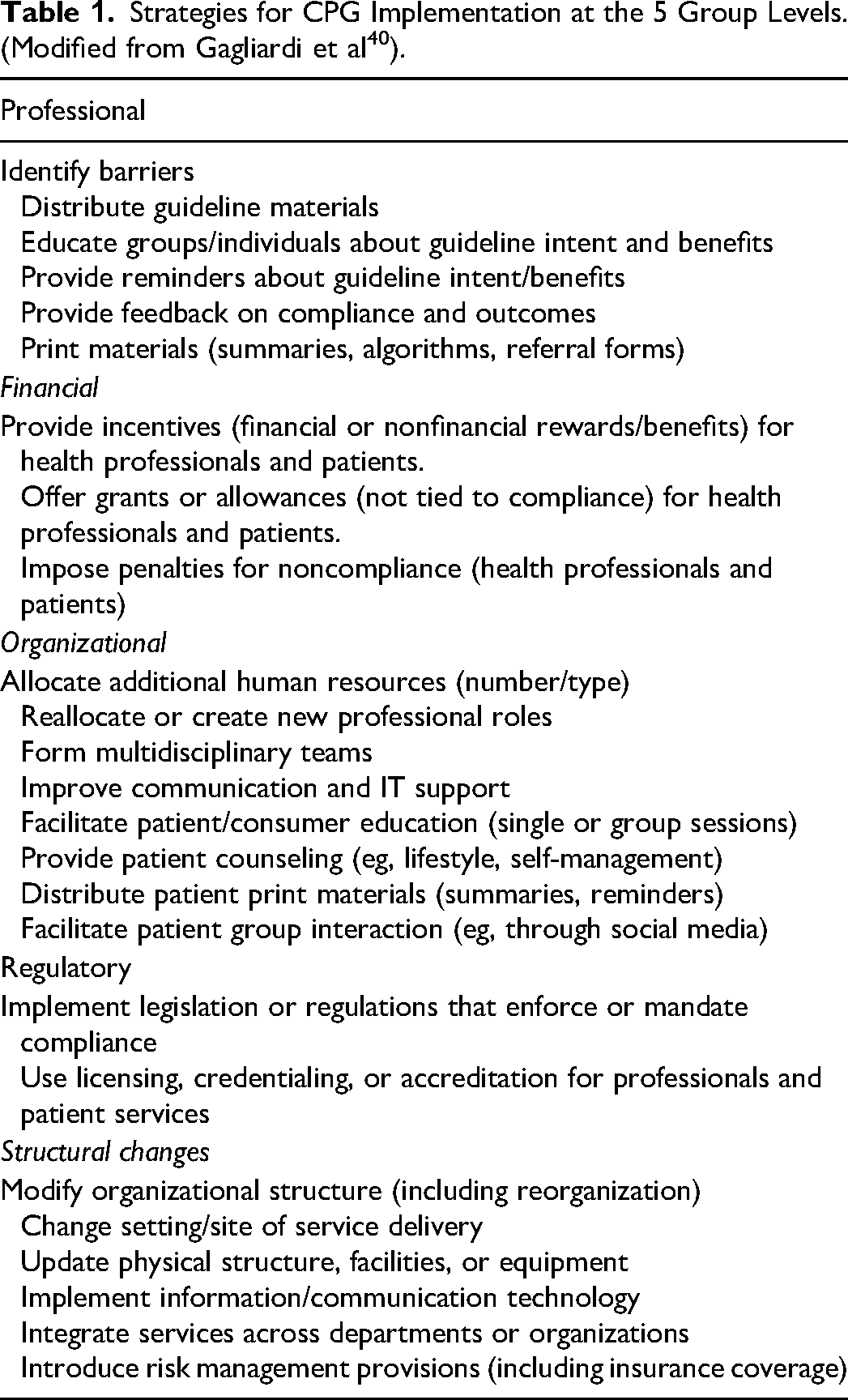
The last few decades have seen tremendous growth in implementation science, which promotes population health by examining effective ways of incorporating CPGs into routine clinical care. 38 Most studies investigating CPG implementation are geared toward quality improvement (QI). 39 Over 50 CPG implementation interventions organized into 5 groups have been identified, including professional, structural changes, organizational, financial, and regulatory (Table 1). 40 Many of these interventions are applied at the level of the healthcare provider and the patient.
Strategies for CPG Implementation at the 5 Group Levels. (Modified from Gagliardi et al 40 ).
Role of Electronic Medical Records in CPG Adoption
The rapid growth of electronic medical records (EMRs) has opened new opportunities for improving CPG implementation. The ongoing integration of patient portals into EMRs can effectively educate and engage patients to enhance CPG implementation. 41 EMRs can embed reminders or prompts to support behavior change among healthcare providers. For instance, an EMR alert for scheduling post-acute symptomatic seizure (PASS) clinic visits in a large healthcare system nearly doubled patient access to specialized care. It was associated with an 8-fold increase in the odds of receiving an outpatient EEG. 42 Additionally, EMRs can facilitate audits by extracting discrete data elements or analyzing clinician notes using natural language processing (NLP), allowing for real-time monitoring of CPG adherence. 43 The most impactful tool for CPG implementation is clinical decision support systems (CDSS), which have revolutionized healthcare delivery. 44 Knowledge-based CDSS use "if-then" rules based on CPGs to guide clinical decisions, while non-knowledge-based CDSS leverage machine learning (ML) and statistical pattern recognition to identify patterns and assist decision-making. A pre-COVID meta-analysis of over 100 studies found that CDSS increased the likelihood of patients receiving recommended care by 6%. 45 A 2023 review showed that over 70% of CDSS tools used AI, requiring clinicians to validate findings such as sepsis risk or imaging results. Although the impact on patient outcomes remains mixed, advancements in CDSS could be key to further improving CPG implementation. 46
Success and Challenges in CPG Implementation
CPGs have notably succeeded in shaping practice in some areas, resulting in improved patient outcomes. One prominent example is the "Get With The Guidelines" (GWTG) program in stroke care. This Quality Improvement-based stroke registry, which just celebrated its 20th year, encourages hospitals to follow evidence-based guidelines. It improved the quality of stroke care and, more importantly, significantly enhanced patient outcomes while achieving a "level of growth that greatly exceeded expectations.” 47 The secret to the success of this program lies in several key elements: the hospital certification process that relies on data-driven metrics, the ability to compare themselves to other peer hospitals, the recognition of hospital success through awards, and the identification of opportunities for QI. Their flagship campaign, "Target: Stroke," brought down door-to-needle tPA administration below 60 min in less than 3 years of launch across the nation. 48 It was associated with reduced in-hospital mortality and an increased proportion of patients discharged home. Data-driven initiatives like GWTG show that CPGs can significantly shape clinical practice with a structured framework for tracking, incentivizing, and promoting adherence.
A parallel in epilepsy to the countrywide impact of GWTG in improving stroke care is the National Association of Epilepsy Centers (NAEC) accreditation program, which has similarly improved nationwide access to quality epilepsy care. 48 Aligning NAEC accreditation with measurable outcomes, especially for drug-resistant epilepsy, may enhance care quality. Mandatory, transparent reporting of epilepsy surgery outcomes, like GWTG's data-driven approach, could promote healthy competition among centers, incentivize outcome improvements, and help patients make informed decisions based on publicly available data. This could also accelerate the adoption of evidence-based practices, particularly epilepsy surgery, which remains severely underutilized despite strong evidence and CPG recommending its use. 49
In contrast to the GWTG success story, the CPGs may face substantial challenges, similar to the recommendations on the management of acute symptomatic seizures (ASyS) by various stroke organizations. The European Stroke Organization advises against secondary antiseizure medication (ASM) prophylaxis after ischemic stroke, while AHA/ASA guidelines recommend ASMs only for recurrent ASyS.50,51 For intracerebral hemorrhage, AHA/ASA guidelines suggest treating ASyS with ASMs without specifying duration, and for subarachnoid hemorrhage, they recommend a 7-day ASM course.52,53 These inconsistencies stem from weak evidence, leading clinicians to rely on professional judgment over unclear guidelines, as an international survey reflected that more than 95% of respondents treat and over 80% discharge ASyS patients on ASMs.53,54
Conclusions
While CPGs are designed to bridge the gap between evidence and practice, their implementation can be challenging and requires clinicians to be aware of the applicability and limitations of individual patients. Ultimately, the successful implementation of CPGs depends on their content, the broader healthcare infrastructure, and the engagement of clinicians and patients.
Footnotes
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This work was supported by the National Institutes of Health (grant number K23AG063899).