
Abstract
The study explores the awareness of technical terms used in evidence-based medicine (EBM) and manner of treating patients with migraine among a random sample of 500 general practitioners (GPs). A mailed questionnaire included questions on GPs' demographics and practice characteristics; awareness of EBM; sources of information about migraine and EBM; and patient's treatment behaviour. Only 27.2% of GPs agreed that clinical trials are needed to evaluate the efficacy of treatments and this awareness was higher in those who learned about migraine from scientific journals or continuing education courses and who attended courses on EBM. For two-thirds of GPs, disability is equivalent to illness diagnosis, and this behaviour was more prevalent in those who agreed that clinical trials are needed to evaluate the efficacy of preventive or curative treatments of migraine and that the clinical approach to migraine required an evaluation of clinical effectiveness, in those who treated a lower number of headache patients, who were older, and in those who did not use guidelines. The majority (93.1%) of GPs indicated that it is important to integrate clinical practice and the best available evidence, and this behaviour was significantly more frequent in those who agreed that the clinical approach to migraine required a clinical effectiveness evaluation, that clinical trials are needed to evaluate the efficacy of preventive or curative treatments of migraine, and in those who attended courses on EBM. Training and continuing educational programmes on EBM and guidelines on treatments of headache for GPs are strongly needed.
Introduction
Evidence-based medicine (EBM) promotes the use of current best evidence in making decisions about the healthcare of individual patients. Its practice means integrating individual clinical expertise with clinical evidence from systematic research and its main principle is that clinical decisions should be based on the best available scientific evidence of previous experience and the conclusions based on such evidence should stimulate quality improvements in patient care (1, 2). However, it should be noted that in several areas of the medical sciences the lack of good evidence for clinical decision-making remains an issue and the availability of good evidence necessarily does not get applied to patient care (3). Moreover, as clinicians deal with patients, there is a continuing increased need for clinical information, but for many reasons clinicians often do not obtain that vital evidence.
Evidence-based migraine treatment presents formidable challenges. The impact of migraine headaches is one of the major public health problems in several industrialized countries, with many patients reporting frequent and significant disability (4, 5). The aetiology and pathophysiology of migraine are not completely understood and prophylactic treatment suffers from a lack of an underlying pathophysiology framework. Moreover, no specific diagnostic test is available and the difficulty in differentiating migraine from tension headache at an early stage of the attack, as occurs in many patients who experience both types of headache, creates further difficulties in using International Headache Society criteria (6, 7).
Previous studies have assessed general practitioners’ (GPs) perceptions of EBM and its influence on healthcare decisions (8–10), but to the best of our knowledge no information is available about EBM influence on migraine, and information on this topic is needed since patients with migraine headaches often present family physicians with diagnostic and therapeutic challenges. Therefore, the purpose of the present study was to identify if GPs in Italy are aware of technical terms used in EBM and how they treat patients with migraine.
Materials and methods
During the period October to December 2002, a survey was conducted on a random sample of 500 GPs in Calabria (Italy). All the GPs sampled were invited to participate by receiving a letter emphasizing the importance of the study, an anonymous self-administered questionnaire, and a pre-addressed envelope to facilitate the return of the completed questionnaire. Informed written consent for their participation was obtained and confidentiality of responses was assured.
The questionnaire included questions focusing on GPs’ demographics and practice characteristics; their awareness of technical terms used in EBM; main sources of information about migraine and EBM; and their behaviour in terms of eventual treatment.
Responses concerning awareness of EBM were based on a three-point Likert scale with options for ‘agree’, ‘uncertain’, and ‘disagree’; whereas four responses for behaviour were in ‘yes/no’ format.
The validity of specific questions was addressed through a pilot study by administering the questionnaire to a convenience sample of GPs and on the basis of the results of the pretesting modifications were made to improve the validity of responses.
Statistical analysis
Multiple logistic regression was performed. In the models developed, variables were included that were considered likely to be associated with the following outcomes of interest: awareness that the clinical trials are needed to evaluate the efficacy of preventive or curative treatments of migraine (Model 1); awareness that the clinical trials are needed to establish a migraine therapy considering risks and benefits (Model 2); awareness that the cost–benefit analysis examines treatment costs and benefits for patient's health status (Model 3); prescribing diagnostic procedures in headache patients (Model 4); headache diagnosis behaviour (Model 5); combining clinical practice and best evidence available (Model 6). For the purposes of analysis, the outcome variables originally consisting of multiple categories were collapsed into two levels. In Model 1, GPs were divided into those who were aware that clinical trials are needed to evaluate the efficacy of preventive or curative treatments of migraine vs. all others; in Model 2, those who were aware that clinical trials are needed to establish a migraine therapy considering risks and benefits vs. all others; in Model 3, those who were aware that the cost–benefit analysis examines treatment costs and benefits for patient's health status vs. all others; in Model 4, those who prescribe diagnostic procedures with a neurologist's advice vs. all others; in Model 5, those who indicate disability as an equivalent sign for illness diagnosis in headache patients vs. all others; in Model 6, those who combine clinical practice and best evidence available vs. all others.
The following explanatory variables were included in all models: age (1 = ≤45, 2 = 46–50, 3 = 51–55, 4 = >55), sex (0 = female, 1 = male), duration of work activity (continuous, in years), number of headache patients treated per month (continuous), and having attended epidemiology or EBM courses (0 = no, 1 = yes). In Models 1–3 the following variables were also included: clinical practice and best evidence available were combined (0 = no, 1 = yes), modifying treatment when scientific evidence showed that another one is more efficacious (0 = never, 1 = rarely, 2 = sometimes, 3 = often, 4 = always), modifying treatment when scientific evidence showed that another one is less expensive than another (0 = never, 1 = rarely, 2 = sometimes, 3 = often, 4 = always), and scientific journals or continuing education courses as source of information (0 = no, 1 = yes). The following explanatory variables were also included in Models 4–6: awareness that the clinical approach to headache required a clinical effectiveness evaluation by performing controlled clinical trials (0 = no, 1 = yes), awareness that clinical trials are needed to evaluate the efficacy of preventive or curative treatments of migraine (0 = yes, 1 = no), awareness that clinical trials are needed to establish a migraine therapy considering risks and benefits (0 = yes, 1 = no), and scientific association guidelines as source of information (0 = no, 1 = yes). Finally, in Model 6 the following explanatory variables were also included: considering disability as an equivalent sign for illness diagnosis (0 = no, 1 = yes) and performing preventive treatment of headache patients (0 = no, 1 = yes). The significance level for variables entering the logistic regression models was set at 0.2 and for removing from the model at 0.4. The odds ratios (ORs) and 95% confidence intervals (CIs) were calculated. Data were analysed using the Stata software program (Stata Corporation, College Station, TX, USA) (11).
Results
Of 500 questionnaires distributed, responses were received from 455, a response rate of 91%. The mean age of the sample of GPs was 49.9 years (range 36–70 years), more than three-quarters were males, the mean duration of work activity as GP was 17 years, and they provided care to a mean number of 17 patients with migraine per month.
Respondents’ awareness of technical terms used in EBM is presented in Table 1. Broad level of awareness was lacking, since only 27.2% of GPs agreed that clinical trials are needed to evaluate the efficacy of preventive or curative treatments and 47.6% agreed that relative risk and ORs are measures used in clinical trials to establish whether a specific treatment is efficacious. However, a considerable proportion (71.8%) agreed that the meta-analysis uses statistical methods to combine the results of previous studies in order to provide a quantitative and cumulative summary of the overall treatment effect. Three-quarters of GPs agreed that the clinical approach to migraine required an effectiveness evaluation by performing controlled clinical trials. Regarding health economics, one-quarter agreed that studies in this field are useful for helping the GP in prescribing treatment for patients which is less expensive but of similar efficacy. The results of the multiple logistic regression analysis on the responses of GPs who are aware that clinical trials are needed to evaluate the efficacy of preventive or curative treatments of migraine indicated that, among all variables, sources of information and attending courses on epidemiology or EBM significantly predicted that awareness. Indeed, it was significantly higher for those respondents who learned about migraine from scientific journals or continuing education courses (OR 2.65, 95% CI 1.23, 5.70; P = 0.013) and for those who attended courses on epidemiology or EBM (OR 1.81, 95% CI 1.10, 2.98, P = 0.020) (Model 1 in Table 3). Overall, only 36.9% of GPs were aware that a clinical trial is needed to identify migraine therapy, considering risks and benefits, and multiple logistic regression analysis showed that this awareness was significantly greater in those with fewer years’ experience (OR 0.92, 95% CI 0.88, 0.96; P < 0.001), in those who attended courses of epidemiology or EBM (OR 2.52, 95% CI 1.57, 4.05; P < 0.001), and who used scientific journals or continuing education courses as source of information (OR 3.79, 95% CI 1.87, 7.65; P < 0.001) (Model 2 in Table 3). Moreover, the GPs who were aware that the cost–benefit analysis examined treatment costs and benefits for patient's health status were those who had a lower number of years in practice (OR 0.96, 95% CI 0.93, 0.99; P = 0.019), who attended courses on epidemiology or EBM (OR 1.66, 95% CI 1.03, 2.69; P = 0.038), who used scientific journals or continuing education courses as source of information (OR 2.72, 95% CI 1.35, 5.49; P = 0.005), and who would not modify the patients’ treatment when scientific evidence indicated that it is more expensive than the new treatment (OR 0.72, 95% CI 0.58, 0.89; P = 0.003) (Model 3 in Table 3).
Awareness of respondents about instruments used in evidence-based medicine

Logistic regression model results

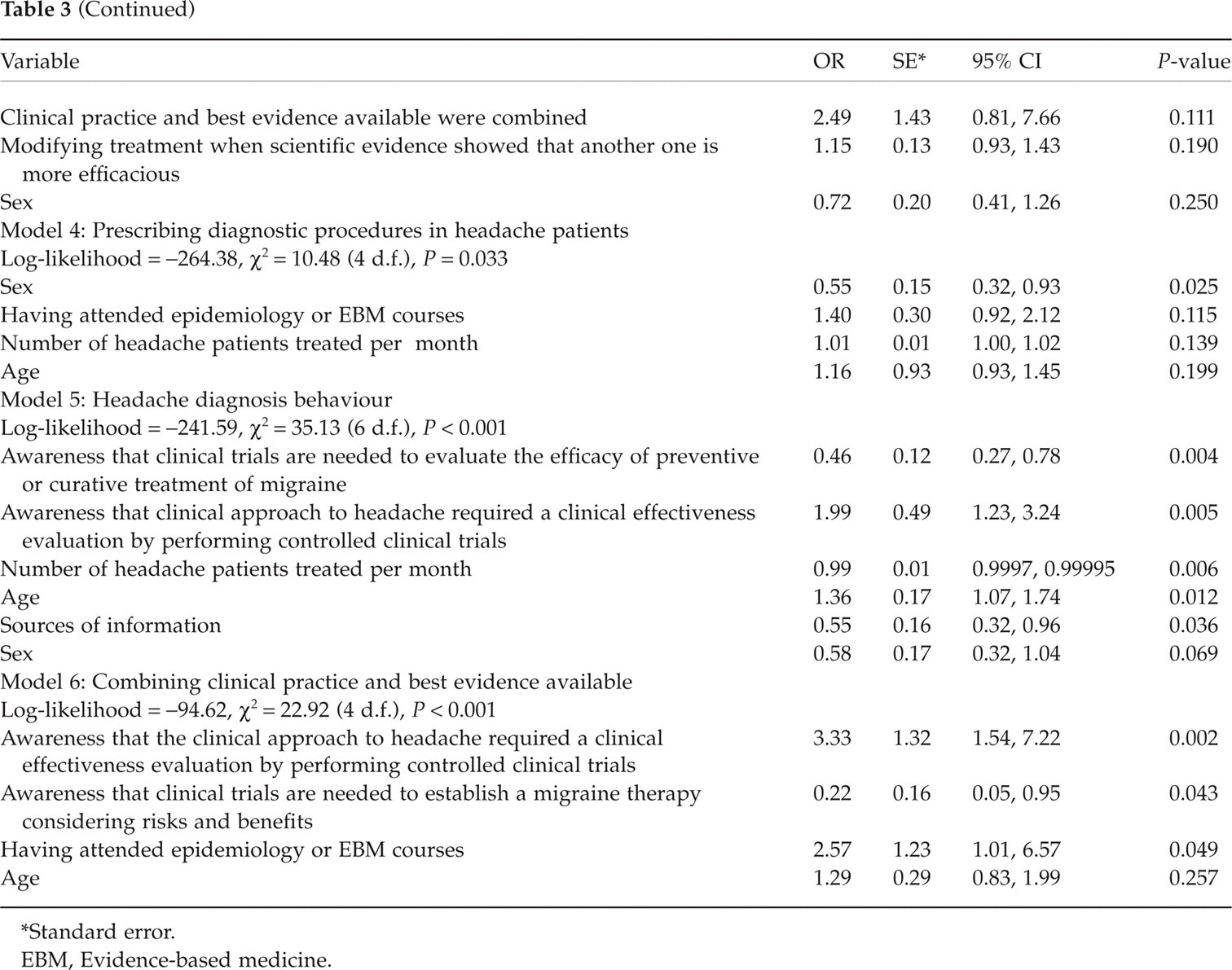
Standard error.
EBM, Evidence-based medicine.
Table 2 shows the respondents’ behaviour about EBM and headache patient management. Regarding the behaviour in clinical practice, the majority of the respondents (93.1%) indicated that it is important that the skills needed to provide a solution to a clinical dilemma should imply the integration between clinical practice and the best evidence available. However, this is in contrast to the result that when scientific evidence indicates that a current treatment is less efficacious or more expensive than the new treatment, only 14% and 3.1% of GPs, respectively, would modify the treatment. Half of the sample would prescribe diagnostic procedures such as encephalic computed tomography and magnetic resonance imaging with the advice of a neurologist. Among all variables tested, only female sex significantly predicted appropriate use of that particular diagnostic procedure (OR 0.55, 95% CI 0.32, 0.93; P = 0.025) (Model 4 in Table 3). For two-thirds of the sample (65.5%), disability in headache patients was equivalent to illness diagnosis, and regression analysis showed that this behaviour was significantly more likely in those GPs who agreed that clinical trials are needed to evaluate the efficacy of preventive or curative treatments of migraine (OR 0.46, 95% CI 0.27, 0.78; P = 0.004) and that the clinical approach to migraine required a clinical effectiveness evaluation by performing controlled clinical trials (OR 1.99, 95% CI 1.23, 3.24; P = 0.005), in those who treated a lower number of headache patients per month (OR 0.99, 95% CI 0.9997, 0.99995; P = 0.006), who were older (OR 1.36, 95% CI 1.07, 1.74; P = 0.012), and who used guidelines about treating migraine (OR 0.55, 95% CI 0.32, 0.96; P = 0.036) (Model 5 in Table 3).
Respondents’ behaviour concerning evidence-based medicine (EBM) and headache patient management

Numbers that do not add up to 455 are due to missing data for that variable.
NSAID, Non-steroidal anti-inflammatory drug; CT, computed tomography; MRI, magnetic resonance imaging.
Combining clinical practice and best evidence available in the management of headache patients was significantly more frequent in those GPs who agreed that the clinical approach to migraine required a clinical effectiveness evaluation by performing controlled clinical trials (OR 3.33, 95% CI 1.54, 7.22; P = 0.002), that clinical trials are needed to evaluate the efficacy of preventive or curative treatments of migraine (OR 0.22, 95% CI 0.05, 0.95; P = 0.043), and in those who attended courses on epidemiology or EBM (OR 2.57, 95% CI 1.01, 6.57; P = 0.049) (Model 6 in Table 3).
Questions concerning sources of information indicated that almost two-thirds of respondents (60.8%) did not attend courses on epidemiology or EBM, whereas the respondents learned about migraine mainly from scientific journals (61.7%) and continuing education courses (36.7%). However, almost all (97%) of GPs felt that they did not need additional information.
Discussion
Migraine remains a common disorder underdiagnosed and undertreated, and its care has the potential to improve greatly with the development of new management guidelines, the introduction of new treatments, and the use of EBM tools to rate and compare available therapies objectively.
Few studies have analysed in the past decade the impact of clinical practice guidelines and EBM among GPs (8, 10, 12–15). Some reviews have suggested headache evidence-based diagnostic and therapy evaluation (16, 17) and optimal strategy for managing acute headache (18–20), others have proposed revisions of diagnostic criteria for chronic daily headache (21). This study represents the first investigation of awareness of technical terms used in EBM and explicit presentation of evidence within guidelines and yielded a comprehensive picture of the behaviour in treating of patients with headache among GPs. We recognize that the present study has a potential methodological limitation in the way of collecting information on awareness of technical terms used in EBM and behaviour in management of headache patients that may have implications regarding the interpretation of the results, since such data were obtained from a self-administered questionnaire by the GPs and may therefore be subject to recall bias. Inattention to the interventions may have deflated actual prevalence. However, it is well known that when respondents are provided anonymity and privacy and when they believe the assessment is being conducted for important reasons, this method is considered valid for assessing their awareness and behaviour and for avoiding the problem of unreliable recall.
It is well known that EBM involves defining the questions arising from the encounter with the patient, then tracking down, critically appraising and applying the evidence to the patient, and finally evaluating the outcomes. Physicians commonly believe that they practise EBM, although most would agree that keeping up to date is difficult. Indeed, as physicians deal with patients, there is a perennial need for further clinical information, but it is often not obtained. Physicians also express frustration at the lack of good evidence for decision-making in many areas of medicine. Much useful evidence does exist, but is not necessarily applied in the front lines of patient care. EBM helps clinicians deal with numerous questions that impact on clinical decisions. Identifying evidence to support or refute patterns of healthcare has certain advantages: best care is suggested by the results of an appropriate literature review; it promotes uniformity of care so that the best care can become the standard care; it allows individual clinicians to become aware of the range of certainty and uncertainty in clinical decision making; and it suggests areas of clinical uncertainty that require more definitive evidence than usual practice. However, accessing and interpreting evidence to answer clinical questions is not such a straightforward issue, especially in primary care. When GPs do access the literature to find evidence about clinical problems, they should be aware of certain limitations, e.g. the applicability of the available medical evidence to general practice, as much of the information is not obtained from primary care. Practising EBM takes time to incorporate best external evidence with clinical expertise, clinicians and, in particular, GPs need to learn how to use tools that allow them to find, critically appraise and apply the evidence to their patients. A prerequisite is the recognition that there are knowledge gaps that need to be filled. Therefore, best external evidence should always be integrated with clinical expertise and it is the experienced clinician that decides whether and how the external evidence applies to a particular patient.
Despite an overall positive attitude toward evidence-based diagnostics, the GPs participating in this study were not aware that guidelines were the most favoured approach for moving from opinion-based medicine to EBM. Less than half (46.7%) of the GPs modify the treatment when and if new scientific evidence indicates that its use for a patient is less efficacious that the new one. Recommendations to change practice should take prior beliefs of GPs into account. The results of our study indicate a lack of GPs’ awareness, because only 27.2% and 26.5%, respectively, agreed that clinical trials are needed to evaluate the efficacy of preventive or curative treatment and that health economic evaluation is useful in prescribing treatment that should be less expensive but with similar efficacy. Published sources of guidance are used, since 61.7% and 17.9% of the respondents indicated scientific journals and medical association guidelines respectively, as additional sources of information on headache issues. In Canada, in a study of 3000 physicians, 52% reported using guidelines at least monthly as a convenient source of advice and good educational tools and 78% and 62% identified colleagues and major organizations, respectively, in deciding whether to adopt a set of guidelines in their practice (13). Moreover, in England 82% of the sample (directors of public health, of purchasing, clinical directors/consultants in hospitals and lead GPs) had previously consulted at least one source of EBM guidance and professionals in the health authorities were much more likely to be aware of the evidence-based guidance and had consulted more sources than GPs in primary care (8). The profile of a knowledgeable physician, compared with an unknowledgeable or uncertain physician, deserves a brief comment. As regards socio-demographic and practice characteristics, older age groups, those who had a lower number of years in practice, those who attended epidemiology or EBM courses, and those who learned about migraine from scientific journals or continuing education courses appear to have more awareness of EBM. Expected duration of working activity differences emerged: the ‘younger’ workers were much more likely to have a higher level of awareness. This aspect suggests that they are more aware of EBM due to its inclusion in the teaching goals of medical degree and teaching programmes over recent years.
Despite the major advances achieved in headache diagnosis and treatment, primary care physicians still face major challenges in making the correct diagnosis and selecting the most appropriate treatment for this common, disabling condition. Improving communication between patients and physicians will help to achieve better outcomes in terms of recognition of headache severity and treatment needs. Continuing education and raising awareness of the impact of headache will help to overcome barriers to headache care and improve headache management. As already stated, we found that attending courses on epidemiology or EBM was significantly associated with awareness of usefulness of clinical trials and cost–benefit analysis in headache management. Following assessment and diagnosis, most patients with disabling migraine can be treated effectively using a triptan. It is well known that triptan medication is efficacious, well tolerated, and highly effective, so many patients may prefer to take them to control their migraine attacks instead of less effective over-the-counter alternatives (22). It is important that individuals with migraine treat attacks appropriately from the outset. Only 43.7% of the GPs surveyed treated patients with acute moderate to severe headache attack giving triptans. The reports on drug treatments for acute migraine described several clinical trials that provided substantial evidence of the efficacy of various agents. However, it is difficult to translate this evidence into clinical practice, since most trials compare an active drug with a placebo and thus are of limited value for informing the choice among available agents; most trials report results within single migraine attacks over just a few hours; few trials test the effectiveness of a treatment plan that combines acute and rescue drug treatments or the effectiveness of an algorithmic approach to drug treatment selection based on prior response. It is well known that migraine treatment depends on the duration and severity of pain, associated symptoms, degree of disability, and initial response to therapy and there is convincing evidence that step care is inferior to stratified care (19). Step care requires initial treatment of acute migraine with a non-specific agent (a simple analgesic) and, if it fails, therapy is stepped up to include a migraine-specific therapy. In stratified care, the physician grades each patient as to the impact the migraine has on their lifestyle, then prescribes appropriate therapy according to the migraine's severity. Patients suffering from little or no impact can receive simple analgesic or combination medications, while those with significant impact may be provided with migraine-specific therapies from the outset (23, 24). A further challenge for physicians is the expanding choice of triptan medication and it is important that individual patient needs and preferences are considered for effective headache management.
In conclusion, additional training and continuing educational programmes on guidelines for treatment of headache for GPs are strongly needed.