
Abstract
Sudden unexpected death in epilepsy (SUDEP) is the leading cause of death in patients with refractory epilepsy, accounting for up to 17% of deaths in patients with epilepsy. The pathophysiology of SUDEP has remained unclear, largely because it is unpredictable and commonly unwitnessed. This poses a great challenge to studies in patients. Recently, there has been an increase in animal studies to try to better understand the pathophysiology of SUDEP. In this current review, we focus on developments through seizure-induced death models and the preventative strategies they may reveal.
Introduction
Epilepsy affects more than 70 million people globally. 1 Although seizures can be fatal in several ways, 2 sudden unexpected death in epilepsy (SUDEP) accounts for up to 17% of death in patients with epilepsy. 3 Sudden unexpected death in epilepsy is second only to stroke in potential life-years lost due to neurological disease. 4 Sudden unexpected death in epilepsy is defined as the sudden, unexpected, witnessed or unwitnessed, nontraumatic, and nondrowning death in a patient with epilepsy, excluding known status epilepticus and in who the postmortem examination provides no structural or toxicological causes of death. 5 Sudden unexpected death in epilepsy most commonly follows a seizure, especially a generalized one. 6 Other risk factors include young age of onset, poor medication compliance, nocturnal seizures, sleeping prone, long seizure duration, and long epilepsy history. 7, 8 The landmark MORTality in Epilepsy Monitoring Unit Study (MORTEMUS) demonstrates a cascade of cardiorespiratory events preceding death, 9 suggesting SUDEP is the consequence of a complex and heterogeneous process. Proposed pathophysiological mechanisms for SUDEP include respiratory, cardiac, and arousal dysregulation and have implicated several neurotransmitter and neuromodulator systems. 2,7,10 -12 The unpredictable and largely unwitnessed nature of SUDEP poses a great challenge to studies in patients. Herein, we will review basic science developments in SUDEP research, focusing primarily on animal models (Table 1) in the context of etiology they recapitulate and preventative strategies these models may reveal.
A Summary of Animal Models in the Context of SUDEP Etiology.
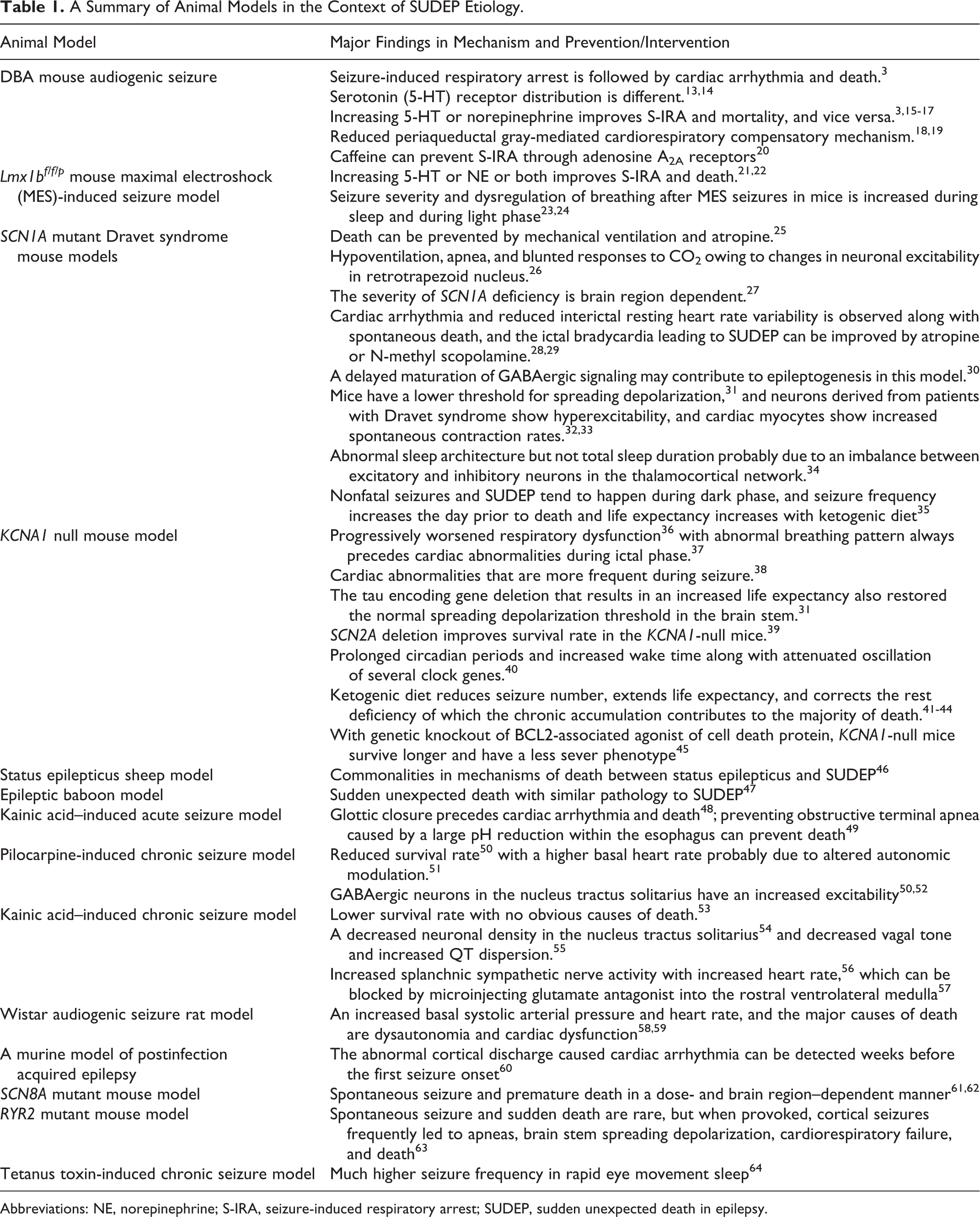
Abbreviations: NE, norepinephrine; S-IRA, seizure-induced respiratory arrest; SUDEP, sudden unexpected death in epilepsy.
Respiratory Mechanisms
Seizures frequently affect breathing. 65 In patients who succumbed to SUDEP in epilepsy monitoring units in the MORTEMUS study, terminal apnea preceded terminal asystole. 9 To better understand mechanisms for how seizures affect breathing, several groups have turned to animal models.
Several animal models recapitulate a seizure-induced respiratory arrest (S-IRA) phenotype. Perhaps the most well-known models are the DBA/1 and DBA/2 mouse audiogenic seizure (AGS) models. These mice commonly exhibit S-IRA following AGS. S-IRA can be rescued by mechanical ventilation. 3 If resuscitation is delayed, mice will then develop cardiac arrhythmia and eventually die from the AGS. 3 While DBA/1 mice usually need several stimuli before consistently showing AGS with S-IRA, DBA/2 mice are more likely to have an S-IRA in their first AGS. 3 This phenomenon can at least be partially attributed to the difference in serotonin 5-hydroxytryptamine (5-HT) receptor expression. 3,13,14 Selective 5-HT reuptake inhibitors such as fluoxetine and sertraline, and a 5-HT-releasing drug fenfluramine, reduce the likelihood of S-IRA, whereas a nonselective 5-HT receptor antagonist cyproheptadine facilitates occurrence of S-IRA in DBA mice. 3,15,66 Optogenetic activation of 5-HT neurons suppresses S-IRA in the DBA/1 mice. 67 An insufficiency in the periaqueductal gray-mediated cardiorespiratory compensatory mechanism which can be enhanced by fluoxetine may underlie the death of DBA/1 mice. 18,19 5-HT2C receptor-null mutant mice are also susceptible to AGS and death. 68 Mice with a genetic deletion of 5-HT neurons in the central nervous system (Lm1xbf/f/p) show increased susceptibility to and mortality from chemically and electrically induced seizures. 21 These mice demonstrate S-IRA following maximal electroshock (MES)-induced seizures, which can be prevented by 5-HT2A receptor agonists. 21 This evidence suggests 5-HT plays an important role in S-IRA and SUDEP. Norepinephrine (NE) also regulates arousal and respiration in the brain. An NE reuptake inhibitor (NRI) atomoxetine suppresses the S-IRA in the DBA/1 mice. 16 ,17 Atomoxetine and another NRI, reboxetine, also reduce S-IRA following MES-induced seizures. 22 This suggests a role for NE in modulating S-IRA and death.
The role of airway obstruction in SUDEP has also been explored. Recurrent seizures induced with kainic acid, a glutamate receptor agonist, in anesthetized Sprague Dawley rats, result in complete glottic closure which is followed by ST-segment elevation, bradycardia, and eventually death, while central apnea only causes minimal cardiac changes. 48 In another study, laryngospasm which causes obstructive terminal apnea is accompanied by a large pH reduction within the esophagus. 49 More importantly, when obstructive apnea is prevented by blocking the acidification, there are no sudden deaths, 49 suggesting a novel strategy for intervention.
Peri-ictal and postictal respiratory dysfunction have also been identified in genetic mouse models. Dravet syndrome, a childhood-onset epileptic encephalopathy which often progresses into a refectory epilepsy, is associated with a high SUDEP risk. 69 Mutation in SCN1A encoding the Nav1.1 voltage-gated sodium channel is found in 80% of patients with Dravet syndrome. 70 In SCN1AR1407X/+ mice, death can be prevented by mechanical ventilation and intracerebroventricular infusion of atropine, suggesting a central apnea mechanism in these cases with SUDEP. 25 Likewise, mice carrying a conditional SCN1A missense mutation exhibit hypoventilation, apnea, and blunted response to CO2 which can be explained by changes in neuronal excitability in the retrotrapezoid nucleus. 26 Mice lacking the Kv1.1 channel encoded by the KCNA1 gene have early-onset seizures and subsequent SUDEP. An array of respiratory dysfunction that progresses with age has been found in KCNA1-null mice, 36 and the abnormal breathing pattern always precedes cardiac abnormalities during the ictal phase. 37
In addition, a sheep model of bicuculline-induced status epilepticus reveals a doubled peak pulmonary vascular pressure without cardiac changes and a rapid rise in serum (CO2) and rapid drop in serum (O2) in animals that died. 46 Baboons with genetic generalized epilepsy are more likely to die young without apparent cause except pulmonary edema, which suggests death from SUDEP. 47
Cardiac Mechanisms
Seizures commonly affect cardiac function. Cardiac dysrhythmias have been implicated in SUDEP. A number of animal models demonstrate seizure-associated cardiac phenotypes that may be useful in understanding the pathophysiology of SUDEP.
Rats with epilepsy induced by the administration of pilocarpine, a cholinergic muscarinic agonist, have a higher basal heart rate compared to controls. 51 Mice subjected to pilocarpine have a lower survival rate compared to age-matched controls. 50 GABAergic neurons in the nucleus tractus solitarius (NTS), a key locus in cardiorespiratory regulation, 54 of these mice display a glutamate-dependent increase in spontaneous action potentials and reduced A-type potassium current, suggesting increased excitability likely contributing to reduced survival. 50 ,52 Similarly, rats subjected to kainic acid-induced epilepsy have a high mortality rate at 24 months, which has been attributed to SUDEP. 53 These rats have decreased neuronal density in the NTS, 54 decreased vagal tone, and increased QT dispersion. 55 In addition, they show a 2-fold increase in splanchnic sympathetic nerve activity with increased heart rate, 56 which can be blocked by microinjecting a glutamate antagonist into the rostral ventrolateral medulla. 57
When subjected to acoustic stimulation, Wistar audiogenic rats can have AGSs and die from them. These rats show an increased basal systolic arterial pressure and heart rate, and the major causes of death are dysautonomia and cardiac dysfunction. 58 ,59 In a murine model of postinfection-acquired epilepsy which has an SUDEP phenotype, 71 cardiac arrhythmia is preceded by abnormal cortical discharges, and this brain–heart interaction can be detected weeks before the first seizure onset, 60 supporting the idea that cardiac abnormalities originate in the brain.
Some genes that cause cardiac arrhythmia, such as long QT syndrome, are also involved in SUDEP. 72,73 For example, both the SCN1A-deficient models and the knock-in mouse model of the human mutation SCN1AR1407X/+ recapitulate characteristic seen in patients. 27 Reduced interictal resting heart-rate variability has been found in the SCN1A-deficient model, and the ictal bradycardia leading to SUDEP can be improved by atropine or N-methyl scopolamine. 28 SCN1AR1407X/+ mice display a range of cardiac abnormalities including QT prolongation, ventricular fibrillation, and focal bradycardia. 29 Interestingly, the effect of SCN1A deficiency is brain region dependent. The lack of Nav1.1 in inhibitory GABAergic neurons causes a more severe phenotype, but when combined with forebrain excitatory neuron deficiency, SUDEP incidence is reduced. 27 Delayed maturation of GABAergic signaling may contribute to epileptogenesis in this model. 30 Mice carrying a de novo mutation of SCN8A die prematurely in a dose-dependent manner. 61 This mutation causes an increase in persistent sodium current density in hippocampal CA1 and CA3 pyramidal neurons, and CA3 bipolar neurons, suggesting regional and neuronal specificity. 62 Potassium channel–encoding genes are also implicated in SUDEP and cardiac arrhythmias. KCNA1-null mice show cardiac abnormalities including bradycardia, premature ventricular contractions, and increased atrioventricular conduction blocks which are more frequent during seizures. 38 Mutations in several other cardiac-related genes including SCN2A, SCN5A, KCNQ1, KCNQ2, RYR2, HCN, and SENP2 are also associated with spontaneous seizures and an increased risk of SUDEP. 72
A possible mechanism that contributes to SUDEP in these animal models is spreading depolarization, a self-propagating depolarizing wave that silences neuronal networks. A lower threshold for spreading depolarization has been found in SCN1A mutant mice, KCNA1-null mice, Cacna1aS218L, and RYR2RQ/+ mice. 31,63,74 Although spontaneous seizure and sudden death are rare in RYR2RQ/+ mice, when provoked, cortical seizures frequently lead to apneas, brain stem spreading depolarization, cardiorespiratory failure, and death due to enhanced excitation in cortex and brain stem autonomic microcircuits. 63 These findings indicate a causal relationship between spreading depolarization and SUDEP. 75
An interesting way to explore effects of mutation on cellular function is to use induced pluripotent stem cells (iPSCs) from patients with epilepsy. Forebrain-like pyramidal- and bipolar-shaped neurons derived from patients with Dravet syndrome show increased sodium currents, spontaneous firing, and other signs of hyperexcitability compared to neurons derived from healthy controls. 32 ,76 Cardiac myocytes derived from iPSC of patient with Dravet syndrome show increased sodium current and spontaneous contraction rates. 33 Remarkably, cardiac abnormalities identified from iPSC-derived cardiac myocytes were confirmed clinically for the subject with the most profound increase in sodium current, 33 suggesting patient-derived iPSCs are a valuable tool for risk assessment. Progress has also been made in other neurological diseases that have a seizure phenotype such as Rett syndrome using the iPSC platform. 32
Arousal, Sleep, and Time of Day
In 7 of the 10 cases from the MORTEMUS study for which adequate data were available to determine vigilance state, SUDEP occurred following nocturnal seizures. 9 Seizure severity and dysregulation of breathing after MES seizures in mice is increased during sleep and during the inactive phase. 23 ,24 An SCN1A haploinsufficiency Dravet syndrome mouse model shows abnormal sleep architecture but not total sleep duration probably due to an imbalance between excitatory and inhibitory neurons in the thalamocortical network. 34 KCNA1-null mice have a prolonged circadian period and altered sleep architecture. 40 ,77 Death tends to happen during the dark phase in SCN1AR1407X/+ and KCNA1-null mice, and seizure frequency increases the day prior to death. 34,41,78 In a tetanus toxin model of temporal lobe epilepsy, seizure frequency is much higher during rapid eye movement sleep. 64 These findings suggest that SUDEP may have a circadian- and/or sleep-state dependence. 79,80
The ketogenic diet, an alternative seizure treatment for refractory epilepsy, reduces the mortality in SCN1AR1407X/+ mice without modifying seizure frequency or light–dark predilection. 35 Moreover, the ketogenic diet reduces seizure number and extends longevity in KCNA1-null mice, in a gender- and age-dependent manner. 41 -43 In addition, rest deficiency seen in KCNA1-null mice is reduced with ketogenic diet treatment. 44 Mice with genetic knockout of BCL2-associated agonist of cell death (BAD) protein increase the use of ketone bodies in neurons by reducing their ability to use glucose and show a decreased seizure severity when injected with kainic acid. 81 Double knockout of KCNA1 and BAD lessens seizure severity and prolongs survival. 45
Both 5-HT and NE, which have been implicated in SUDEP, are also involved in arousal regulation, and their concentrations oscillate in a time-of-day-dependent manner. 80 Adenosine, which is involved in homeostatic regulation of sleep through adenosine A1 and A2A receptors, 82 is also implicated in SUDEP. 83 Some adenosine receptors are exclusively activated by the rise in adenosine during seizures, which contributes to the seizure-cessation mechanism. However, if the clearance of adenosine is compromised, the high adenosine levels could suppress respiratory function and also cause sedation. Blockade of adenosine metabolism worsens seizure severity and increases mortality from kainic acid–induced seizures. 84 Caffeine, a potent A2A receptor antagonist, prevents S-IRA in DBA/2 mice. 20
Conclusions
Sudden unexpected death in epilepsy is an important public health problem. Before preventive strategies can be implemented, we need to better understand the pathophysiology. Basic science studies, especially those involving animal models, are rapidly advancing our understanding of the pathophysiology of SUDEP. An important way forward will be to continue to develop models that recapitulate as many key features of human SUDEP as possible.
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: Dr. Buchanan is supported by NIH/NINDS R01 NS095842 and the Beth L. Tross Epilepsy Professorship at the University of Iowa, Carver College of Medicine.