
Abstract
Blood Markers of Cardiac Stress After Generalized Convulsive Seizures. Nass RD, Motloch LJ, Paar V, Lichtenauer M, Baumann J, Zur B, Hoppe UC, Holdenrieder S, Elger CE, Surges R. Epilepsia. 2019;60(2):201-210. doi:10.1111/epi.14637. Epub 2019 Jan 15. PMID: 30645779 Generalized convulsive seizures (GCS) are associated with high demands on the cardiovascular system, thereby facilitating cardiac complications. To investigate occurrence, influencing factors, and extent of cardiac stress or injury, the alterations and time course of the latest generation of cardiac blood markers were investigated after documented GCS. Adult patients with refractory epilepsy who underwent video-electroencephalography monitoring along with simultaneous one-lead electrocardiography recordings were included. Cardiac biomarkers (cardiac troponin I [cTNI]; high-sensitivity troponin T [hsTNT]; N-terminal prohormone of brain natriuretic peptide; copeptin; suppression of tumorigenicity-2 [SST-2]; growth differentiation factor 15, [GDF-15]; soluble urokinase plasminogen activator receptor [suPAR]; and heart-type fatty acid binding protein [HFABP]) and catecholamines were measured at inclusion and at different time points after GCS. Peri-ictal cardiac properties were assessed by analyzing heart rate (HR), HR variability (HRV), and corrected QT intervals (QTc). Thirty-six GCS (6 generalized-onset tonic-clonic seizures and 30 focal to bilateral tonic-clonic seizures) were recorded in 30 patients without a history of cardiac or renal disease. Postictal catecholamine levels were elevated more than 2-fold. A concomitant increase in HR and QTc, as well as a decrease in HRV, was observed. Elevations of cTNI and hsTNT were found in 3 (10%) of 30 patients and 6 (26%) of 23 patients, respectively, which were associated with higher dopamine levels. Copeptin was increased considerably after most GCS, whereas SST-2, HFABP, and GDF-15 displayed only subtle variations, and suPAR was unaltered in the postictal period. Cardiac symptoms did not occur in any patient. The use of more sensitive biomarkers such as hsTNT suggests that signs of cardiac stress occur in about 25% of the patients with GCS without apparent clinical symptoms. Soluble urokinase plasminogen activator receptor may indicate clinically relevant troponin elevations. Copeptin could help to diagnose GCS but specificity needs to be tested.Objective:
Methods:
Results:
Significance:
Commentary
Sudden cardiac death, from lethal cardiac arrhythmia or acute myocardial infarction, is more frequent in patients with epilepsy. This may be in part attributed to a higher burden of cardiovascular risk factors and a higher prevalence of cardiac disease in this population. However, seizures, especially generalized convulsive seizures (GCS), themselves can cause serious cardiac events. Extreme examples of life-threatening arrhythmia, ST segment or T-wave abnormalities suggestive of myocardial infarction, QT interval changes, stunned myocardium (aka Takotsubo cardiomyopathy), and even myocardial necrosis complicate generalized convulsive status epilepticus. 1 The hyperadrenergic state resulting from the prolonged convulsions is the likely mechanism. Whether or not uncomplicated GCS can cause cardiac stress and injury is more debated. Prior studies revealed subclinical elevation of cardiac troponin I levels (cTNI) in up to 12% of patients admitted to an emergency room after a GCS and acute myocardial infarction in up to 2.2%. 2,3 These events occurred mostly in patients with preexisting coronary heart disease and known vascular risk factors. However, other studies in patients with drug-resistant epilepsy failed to replicate these findings. 4 Cardiac TNI is highly specific for myocardial injury but may lack sensitivity to detect mild injury or stress. More sensitive biomarkers have recently emerged, including N-terminal prohormone of brain natriuretic peptide (NT-proBNP), high-sensitivity Troponin T (hsTNT), soluble suppression of tumorigenicity (SST-2), copeptin, growth differentiation factor 15 (GDF-15), soluble urokinase plasminogen activator receptor (suPAR), and heart-type fatty acid binding protein (HFABP). These newcomers are well known to cardiologists, emergency, and critical care physicians, but neurologists will not likely be familiar with them. They are summarized in Table 1.
Nature and Observed Changes in Blood Markers of Cardiac Stress After Generalized Convulsive Seizures.
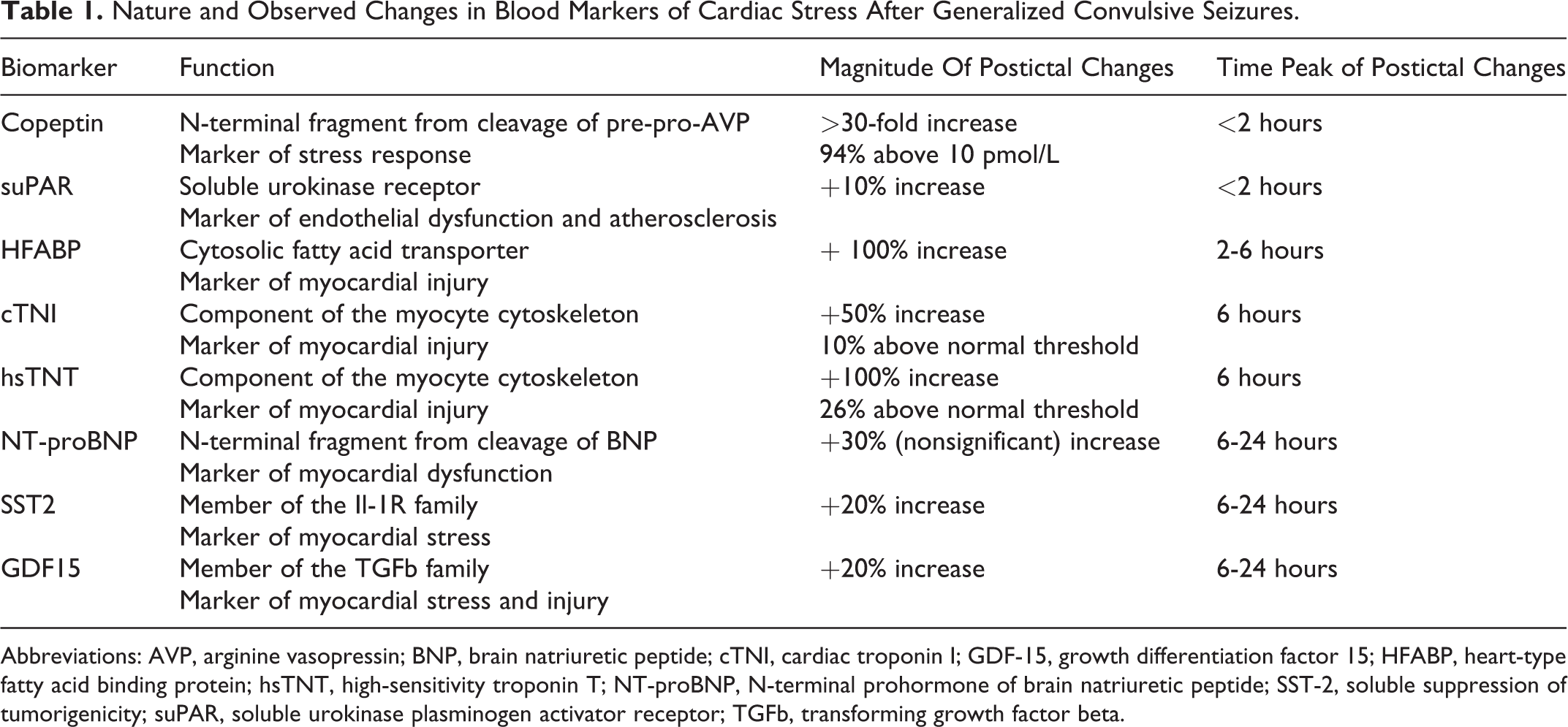
Abbreviations: AVP, arginine vasopressin; BNP, brain natriuretic peptide; cTNI, cardiac troponin I; GDF-15, growth differentiation factor 15; HFABP, heart-type fatty acid binding protein; hsTNT, high-sensitivity troponin T; NT-proBNP, N-terminal prohormone of brain natriuretic peptide; SST-2, soluble suppression of tumorigenicity; suPAR, soluble urokinase plasminogen activator receptor; TGFb, transforming growth factor beta.
In the study by Nass and colleagues, the authors prospectively investigated post-GCS myocardial stress and injury by performing serial EKG studies and measuring serial levels of catecholamines, markers of stress (copeptin), and markers of cardiac injury (cTNI, hsTNT, SST2, GDF-15, suPAR, and HFABP) at baseline, immediately after, and 2 hours, 6 hours, and 24 hours after 36 GCS in 30 patients admitted to their epilepsy monitoring unit. Both primary generalized-onset tonic-clonic seizures and focal-to-bilateral tonic-clonic seizures were included. Most patients had localization-related epilepsy, and the majority of foci were located in the temporal lobe. Half of the cohort had at least one vascular risk factor, mostly smoking, but only one patient had a history of stable coronary arterial disease.
Cardiac arrhythmias other than sinus tachycardia and respiratory arrhythmia occurred in 2 patients. One had supraventricular tachycardia and bundle branch block, and the other tachycardia with idioventricular rhythm. Both spontaneously subsided within 2 minutes of seizure cessation. Significant QT interval changes occurred in most patients. No ST segment alteration was noted. Pulse oximetry was unavailable or unreliable during and after most seizures. Catecholamine levels increased during seizures by up to 3-fold and normalized within 2 hours, indicating a transient hyperadrenergic state. Copeptin levels peaked immediately after seizures and returned to baseline within 2 hours, indicating a transient hormonal stress response. An abnormally high-copeptin level (>10 pg/mL), corresponding to a suggested cutoff for myocardial infarction, was observed in 94% of tested seizures. Markers of myocardial injury (cTNI and hsTNT) increased 2 to 6 hours after seizures. Cardiac TNI levels were abnormal in only 10% of patients but elevated hsTNT levels were found in 26%. Growth differentiation factor 15, HFABP, SST-2, suPAR, and NT-proBNP levels showed changes that were mild or limited to a minority of patients.
Altogether, these findings confirm the sympathetic response to GCS. This response is nearly always associated with a hormonal stress response, as indicated by the almost ubiquitous elevation of copeptin levels. The study further reveals that up to a quarter of GCS are associated with significant subclinical myocardial injury. None of the seizure characteristics, including type (generalized onset vs focal-to-bilateral), location of the seizure onset zone, total seizure duration, or duration of the tonic and clonic phases was associated with greater levels of cardiac injury markers. Similarly, the presence of vascular risk factors did not predict cardiac injury, either. The only factor found to strongly correlate with the levels of cTNI and hsTNT was dopamine level, suggesting that cardiac injury from GCS is indeed associated with a stronger sympathetic response.
Frequency of GCS seizures is the strongest risk factor for sudden unexpected death in epilepsy (SUDEP) and most cases of documented SUDEP appear to result from post-GCS respiratory dysfunction. 5 Some, but not all, studies have also found an association between the duration of postictal generalized electroencephalography suppression (PGES) and the presence of postictal respiratory dysfunction, on the one hand, and the magnitude of the postictal sympathetic response, on the other hand. 6 Given this study finding that postictal sympathetic response is associated with biological sign of myocardial injury, it would have been interesting to further explore the association between PGES, postictal respiratory dysfunction, and cardiac injury. As pointed out by the authors, subtle chronic myocardial lesions are observed in patients with chronic epilepsy, including in cases of SUDEP. 5 Sudden cardiac death in epilepsy is a rare occurrence, however, which does argue against postictal acute cardiac injury or chronic cardiac injury from repetitive GCS being a primary cause of death in patients with epilepsy, except perhaps in a minority of patients at special risk. It is nonetheless possible that high-sensitivity myocardial injury markers, such as hsTNT, might be used in conjunction with other markers to identify patients at higher risk of SUDEP.
Another potential application of these new markers is in the differential diagnosis of GCS with other causes of transient loss of consciousness. Of course, this diagnosis should rely first and foremost on history, especially from reliable witnesses. Oftentimes, though, this information is lacking and serum markers might become useful in differentiating GCS from syncope or even psychogenic nonepileptic spells. Several measures are already available, including prolactin, creatine kinase, and lactate, but all have their shortcomings. 7 As found in this study and another recent study in children with febrile seizures 8 , copeptin might represent a potentially useful new addition to this armamentarium and should be further investigated for this indication.
Finally, this study further underscores that seizures, especially GCS, are not innocuous events. Their impact extends beyond the obvious effects of loss of consciousness, risk of environmental injury, and poor quality of life. The evidence that they strain the whole organism, with potentially lethal short- and long-term consequences, provides yet another motivation to aim for the most effective antiseizure treatment and seizure freedom.