
Abstract
Introduction:
The COVID-19 pandemic placed unprecedented strain on global healthcare systems, with clinical laboratory professionals serving at the critical frontline of diagnostic response. This study examines the relationship between formal biosafety commitments and the realities faced by healthcare professionals (HCPs) on the frontlines. It evaluates the effectiveness of a targeted, in-person biosafety training program for HCPs, particularly clinical laboratory scientists, in the Philippines.
Methods:
This mixed-methods, convergent analysis compares training outcomes with participants’ self-reported workplace challenges during the pandemic. The objective is to explore the connection between knowledge acquisition and the systemic constraints affecting practical application.
Results:
The quantitative analysis of ∼200 participants demonstrates the significant success of the training intervention, with overwhelmingly positive evaluations from participants. In contrast, qualitative thematic analysis of open-ended responses revealed a surprisingly different reality in the field. The findings highlight a “preparedness paradox”; that while the professionals were successfully upskilled through training, they returned to systemically broken environments where their enhanced competency was undermined by institutional deficiencies.
Conclusion:
The study provides crucial local evidence, as it contextualizes broader international trends within the specific challenges and resource constraints of the Philippines, laying the groundwork for understanding how adjustments and training innovations can improve biosafety outcomes in low- and middle-income country contexts. Finally, the study argues that effective pandemic preparedness requires a holistic, multilevel strategy that integrates personnel training with robust systemic support, including resource management, mental health services, and equitable compensation structures, to build a truly resilient healthcare workforce.
Keywords
Background
The recent COVID-19 pandemic was an unprecedented litmus test for health systems worldwide, uncovering hidden vulnerabilities and weaknesses in health infrastructures, particularly in resource-constrained settings. Needless to say, the pandemic triggered an unparalleled global demand for laboratory services. 1 The sudden expansion of laboratory testing capacity included both increased output from existing labs and the creation of new ones, some in unsuitable facilities. At the same time, the worldwide scientific community was occupied with urgent research efforts to analyze SARS-CoV-2 and to develop crucial vaccines, therapies, and diagnostic tools. 2 This rapid increase in both the volume and, in some cases, the risk level of laboratory work underscored the critical importance of having adequately trained personnel who could perform their duties safely and effectively, minimizing the risk of Laboratory-Acquired Infections (LAIs) and accidental releases of the pathogen.
Thus, an effective biorisk management (BRM) program is essential for preventing the spread of LAIs and promoting safe practices in biomedical research. 3 As BRM is heavily anchored with education and training, such plays a vital role in creating a culture of biosafety and biosecurity, improving practices, and addressing gaps in knowledge and implementation.4,5 Various initiatives aim to enhance biosafety and BRM through training and education. In the Philippines and Pakistan, a sustainable program utilized a train-the-trainer methodology to equip professionals in BRM, successfully developing a local network of biosafety trainers. In the Philippines, graduates of the 6-week Philippine Advanced Biorisk Officers’ Training (PhABOT) provided local biosafety experts in their respective regions. PhABOT graduates became instrumental in expanding local biosafety awareness among relevant stakeholders.3,6 Regulatory frameworks and international guidelines, although available, are often insufficiently adapted to local contexts, leading to inconsistencies in practice and risky exposures among laboratory personnel, especially in low- and middle-income countries (LMICs). As such, the literature emphasizes the need for strengthened training models that effectively integrate global standards with local realities. 7
In the Philippines, the Department of Health (DOH) explicitly mandated that personnel working in COVID-19 testing laboratories undergo training covering specific areas to ensure compliance with national biosafety standards and to obtain laboratory accreditation. A crucial aspect emphasized in these training programs was the importance of adhering to the latest internationally recognized guidelines and standards and locally applying them based on professional judgment and risk assessment.6,8 Extensive lockdowns, travel restrictions, and physical distancing mandates made conventional face-to-face training workshops and courses largely unfeasible, particularly in the early and most acute phases of the pandemic in the Philippines. There was a rapid and extensive shift toward online and virtual learning modalities for a wide array of educational purposes, including biosafety training. 9 This shift was driven by the urgency to continue capacitating laboratory personnel and other relevant stakeholders with essential biosafety knowledge and skills so as not to disrupt expanded diagnostic testing. Thus, virtual training allowed rapid, large-scale dissemination of biosafety education, reaching thousands of professionals despite lockdowns and travel restrictions.6,10 For instance, the Philippines successfully trained thousands of individuals in a relatively short period. Online learning offered considerable flexibility, allowing participants to access training materials and complete modules at their own pace and convenience, which could be beneficial for working professionals juggling multiple responsibilities, which was inherent in the Philippine setting. 6
This study explores the complex relationship between formal commitments to biosafety and the real-world experiences of healthcare professionals (HCPs) on the frontlines. It assesses the effectiveness of a targeted, in-person biosafety training program for HCPs, including many clinical laboratory scientists, in northern Philippines. The analysis compares participants’ self-reported workplace challenges encountered during the peak of the pandemic.
Methods
Sampling Procedures and Participants
The study population comprised clinical laboratory scientists and other professionals who participated in intensive, in-person biosafety and biosecurity training workshops conducted in the northern Philippines. Eight batches were organized and implemented between June and December 2022 to comply with the accreditation requirements for clinical laboratories by DOH. During the training proper, pretest, post-test, and lecture evaluations were conducted. Data collection was conducted in person, immediately following the conclusion of the 3-day training workshop. Before the administration of the survey, participants were fully briefed on the study’s objectives, procedures, and the voluntary nature of their participation. The names and other personal information of the study participants were protected, and only those who provided their consent were included.
Training Design
The biosafety training was composed of 11 modules, some of which (denoted by *) include a separate participant-led activity such as presentations or skill demonstrations:
introduction to biosafety and good microbiology practices (1.5 h), biosecurity (1 h), biorisk assessment (1.5 h*), overview of biorisk mitigation measures (1.5 h), biosafety cabinet use (1 h), personal protective equipment (1 h*), infectious substance transport (triple packaging system) (1 h*), emergency response and spill management (1 h*), administrative controls and SOPs (1 h*), disinfection, sterilization, and decontamination (1 h), and biological waste management (1.5 h).
Note: Time indicated shows actual lecture times and excludes the time for participant-led activities.
The modules were designed based on the Centers for Disease Control and Prevention Biosafety in Microbiological and Biomedical Laboratories (5th Edition), World Health Organization (WHO) Laboratory Biosafety Manual (3rd and 4th Editions), in compliance with national guidelines outlined in another study. 6 Lecturers were volunteer-certified biorisk officers from the Philippine Advanced Biosafety Officers’ Training Course nearest the locale. Topics were assigned based on his/her expertise. Lecture materials were prepared and delivered by the same lecturer across all batches, ensuring uniformity in delivery. To quantitatively assess knowledge acquisition, a 50-item, multiple-choice examination covering the core concepts of all 11 training modules was administered. The same instrument was used for both the pretest and the post-test. The pretest was administered at the beginning of the first day, prior to any formal instruction, while the post-test was administered after the lecture evaluations at the conclusion of the final module. Last, a significant duration of the training was dedicated to the culminating activity, which allows them to present their mitigation plan based on site-specific risk assessment (SSRA) of their facility. Participant SSRAs were critiqued by a panel of PhABOT graduates who were currently practicing as biosafety officers in their respective institutions.
Research Instrument
A four-part, structured questionnaire was developed and modified from existing literature, forming a composite instrument designed to capture the specific context of the study. The sections include: Sociodemographic and Professional Profile, Training Program Evaluation, Learning Modality Preferences and Experiences, and COVID-19 Biosafety Experience.11–13 Beyond the structured survey items, open-ended questions were added, providing a platform for participants to articulate their greatest challenges and offer further commentary on their pandemic experience. These qualitative responses offer a narrative complement to the quantitative data.
Data Analysis
Descriptive statistics, including frequencies, percentages, means, and standard deviations (SDs), were calculated to summarize participants’ sociodemographic characteristics and survey responses. A paired-samples t-test of pre- and post-test assessed the effectiveness of the training workshop in enhancing knowledge of participants. Multivariate Analysis of Variance (MANOVA) examined the impact of participant characteristics on professional engagement during the pandemic, with the dependent variable being the Biosafety and Biosecurity Engagements composite profile, derived from two key indicators: (1) the mean rating of the perceived relevance of all 11 training topics to the participant’s job (relevance), and (2) the self-reported percentage of their job that involves BRM (job involvement). Predictor variables included sociodemographic factors from Part 1 of the survey (e.g., age, gender, employer type, and occupation). Analysis was performed using IBM SPSS Statistics (version 27), with significance and confidence levels set at
Results
Sociodemographic and Professional Characteristics
All 217 professionals who attended the training completed the knowledge-based pre- and post-test assessments as part of the workshop’s standard evaluation. Of these attendees, a cohort of 128 participants provided written informed consent to complete the full, multipart survey questionnaire. The sociodemographic and professional profile of the respondents (Supplementary Figure S1) reveals a distinct cohort that shouldered the frontline diagnostic response in the region. The workforce was predominantly female, comprising 79.7% of participants. A significant majority (73.4%) were employed by government institutions, with their work primarily situated in hospitals or health facilities (75.8%) and specifically within the healthcare or clinical laboratory function (95.3%). Professionally, the group consisted overwhelmingly of allied HCPs, such as registered medical technologists, who accounted for 90.6% of respondents. The workforce was also notably young, with the largest age bracket being 18–30 years old (45.3%). Data show that 78.1% had never attended an online biosafety or biorisk training course, and an almost identical proportion (78.9%) had never attended a face-to-face training course prior to this workshop.
Impact on Biosafety Knowledge: Pre- and Post-test Analysis
The results show a dramatic and statistically significant improvement. The mean pretest score for the 217 participants was 28.02 (SD = 4.753, median = 28.0, 95% CI = 27.38–28.65). Following the intervention, the mean post-test score increased to 36.58 (SD = 4.463, median = 37.0, 95% CI = 35.98–37.18), representing a significant improvement of over 8.5 points (
Participant Evaluation of Training Content and Delivery
Quantitative analysis of post-training evaluation surveys reveals overwhelmingly positive feedback from the 217 participants. Across all 11 training topics—ranging from foundational concepts like Introduction to Biosafety and Good Microbiological Practices to specialized areas such as Biosafety Cabinets and practical skills like Emergency Response/Spill Drill—participant feedback was exceptionally positive. Using a 5-point Likert scale (where 4.21–5.00 corresponds to “Excellent”), the mean scores for all seven evaluation criteria (relevance, activities, difficulty, pacing, instructor, presentation, and interest) consistently fell within the “Excellent” range for every module as shown in Table 1. The consistently narrow confidence intervals across all assessments reinforce the reliability of our findings and highlight the overwhelmingly positive evaluations from participants, indicating low variability in their responses. These detailed scores in the Supplementary Material indicate that the uniform delivery by expert lecturers was also a key factor in the training’s success.
Summary of participant evaluation of biosafety training modules
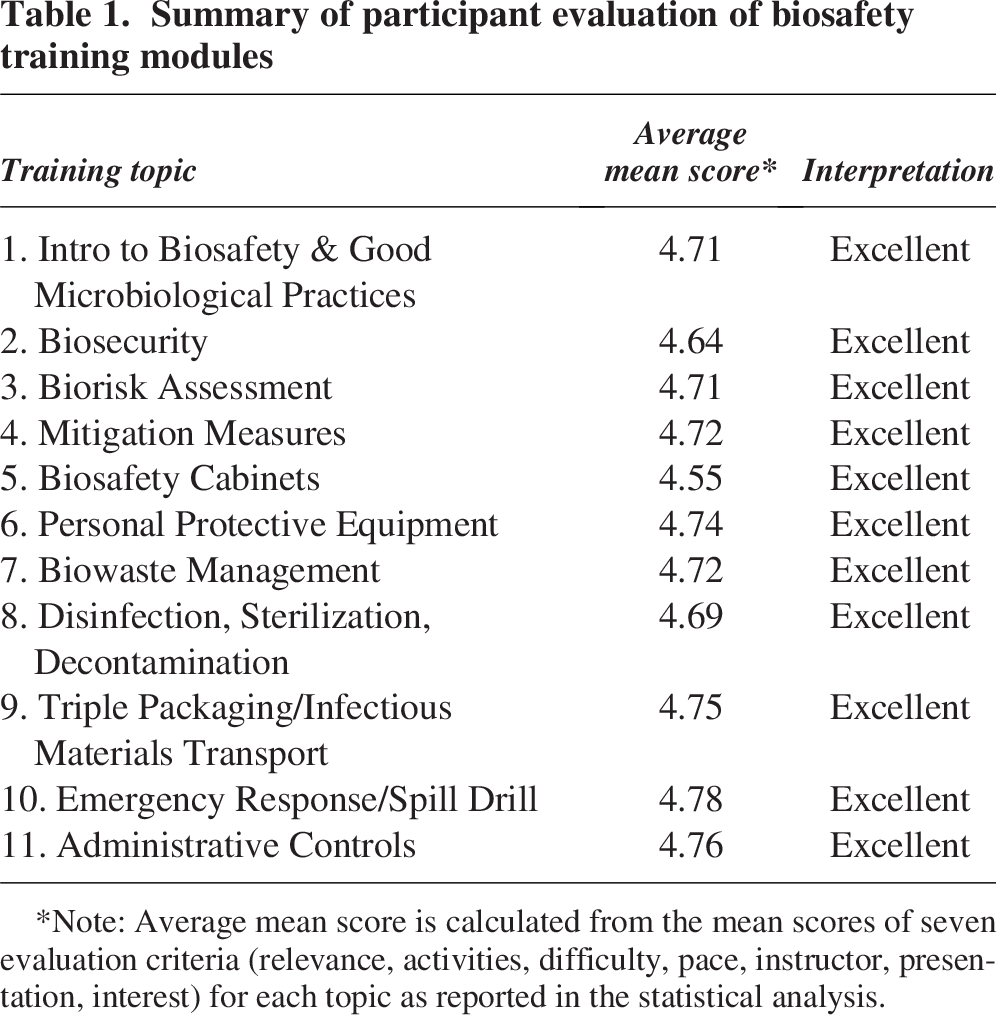
Note: Average mean score is calculated from the mean scores of seven evaluation criteria (relevance, activities, difficulty, pace, instructor, presentation, interest) for each topic as reported in the statistical analysis.
Learning Modality Preferences
A subset of the survey explored participants’ attitudes toward different learning modalities, revealing a strong and clear preference for traditional, in-person instruction for this type of technical training as presented through frequency distributions (Supplementary Data, Frequency Table 12) and descriptive statistics (Table 2). A combined total of 87.5% of respondents either “agreed” (25.0%) or “strongly agreed” (62.5%) with the statement that “Group discussions on BIOSAFETY & BIOSECURITY are more suitable delivered in classroom/traditional learning” yielding a mean score of 3.50 (95% CI = 3.35–3.64), which falls into the “strongly agree” category. Conversely, there was significant skepticism regarding the efficacy of distance learning for critical learning functions. A combined 66.4% of participants “disagreed” or “strongly disagreed” (mean = 2.10, 95% CI = 1.93–2.27) that clarifications are more suitably delivered via distance learning. Similarly, a combined 57.8% disagreed (mean = 2.09, 95% CI = 1.89–2.28) that communication with lecturers and fellow students is easier in a distance learning format. This dissatisfaction with remote modalities was coupled with a significant concern about academic integrity; 65.6% of respondents agreed or strongly agreed (mean = 2.64, 95% CI = 2.45–2.84) that distance learning provides an opportunity for students to cheat during assessments. The data therefore suggest that they view in-person training as a more effective and secure modality for mastering competencies where errors can have severe consequences. The one area of ambiguity in the dataset relates to self-directed learning. The response to whether distance learning provides “motivation for self-directed learning and eager to prepare learning materials before group discussion” was mixed (mean = 2.37, 95% CI = 2.18–2.55), which was interpreted as “mostly disagree, somehow agree.” While some participants may have felt empowered by the format, the overall sentiment remains that the distance modality is a less satisfying, less efficient, and less preferred method for biosafety education compared with its traditional approaches.
Summary of descriptive statistics of the responses related to training delivery
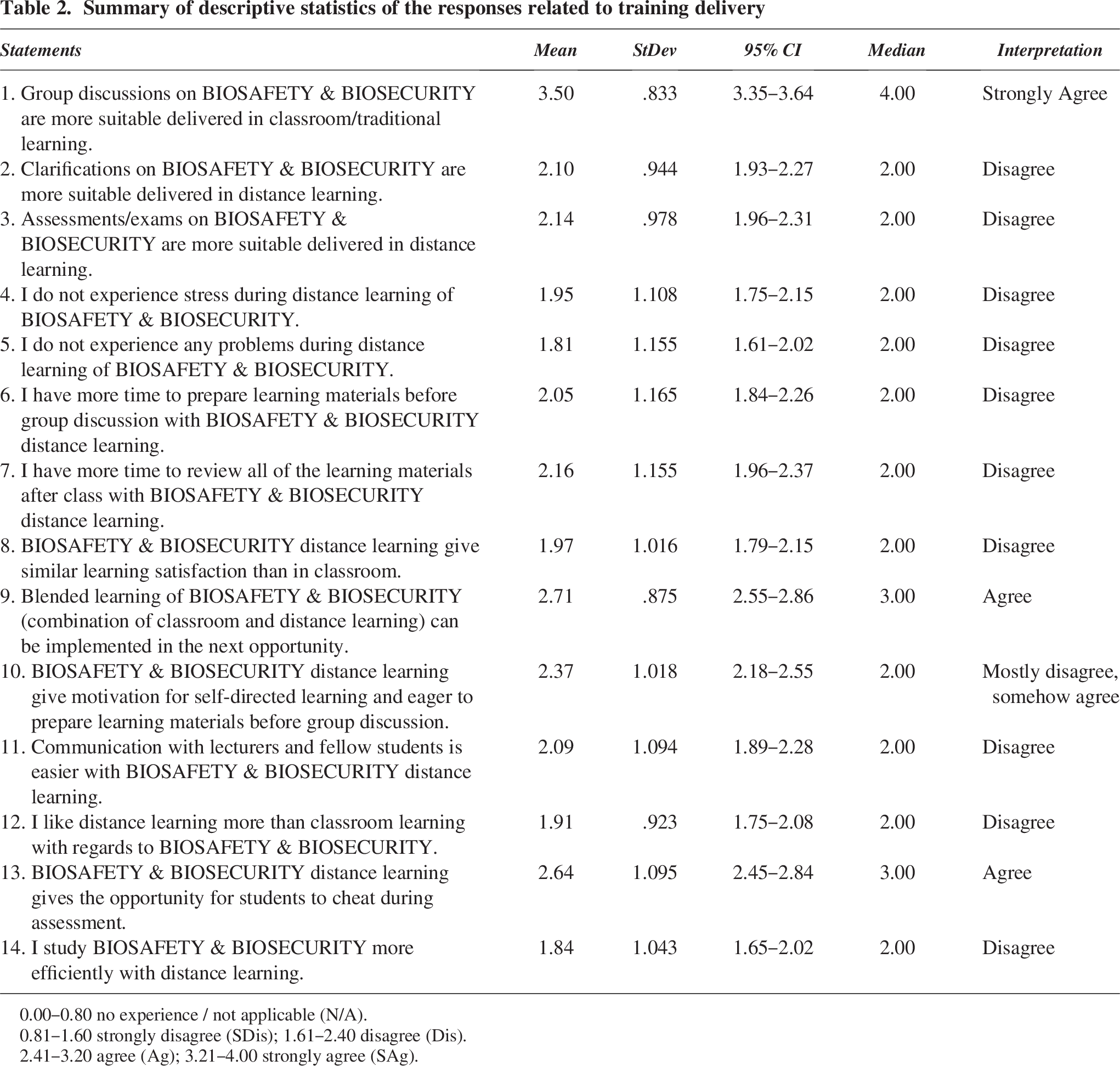
0.00–0.80 no experience / not applicable (N/A).
0.81–1.60 strongly disagree (SDis); 1.61–2.40 disagree (Dis).
2.41–3.20 agree (Ag); 3.21–4.00 strongly agree (SAg).
To explore whether individual characteristics influenced engagement in biosafety and biosecurity practices, a MANOVA was performed. The overall multivariate tests, which evaluate the impact of sociodemographic predictors on combined dependent variables, were found to be statistically nonsignificant (all
In stark contrast to the successful training experience, the qualitative data from open-ended questions paint a picture of the daily realities faced by these HCPs. A frequency analysis of key terms (Table 3) provides a quantitative glimpse into their primary concerns, with terms such as “workload,” “understaffing,” “PPE,” “swabbing,” and “compensation” appearing frequently. These keywords form the foundation of the three major themes that emerged from the analysis: (1) Workload, Staffing, and Scarcity; (2) Fear, Anxiety, and Burnout; and (3) Compensation and Professional Recognition. A formal codebook detailing these themes is presented in the Supplementary Material.
Frequency analysis of key terms in open-ended responses
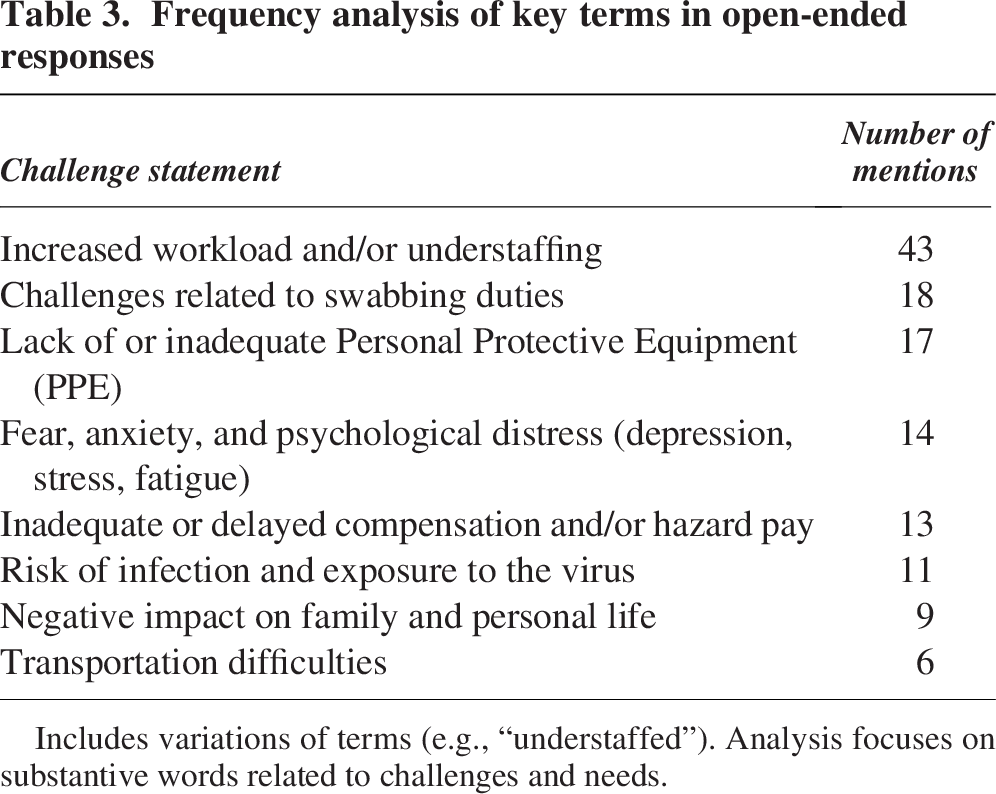
Includes variations of terms (e.g., “understaffed”). Analysis focuses on substantive words related to challenges and needs.
Theme 1: Systemic Collapse: Workload, Staffing, and Scarcity
This was the most pervasive and forcefully articulated theme. The issue of crushing workload and chronic understaffing was highlighted, with comments such as “increase workload,” “overworked and understaffed,” and “work overload due to understaffing” appearing throughout the responses. This was compounded by critical resource scarcity. Multiple participants cited a “limited PPE supply,” a “shortage of PPEs,” and a “lack of medical supplies” as major challenges. This lack of basic protective equipment not only increased their personal risk of infection but also added a significant layer of stress to their daily work. The task of collecting samples from suspected COVID-19 patients was described as “high-risk” and physically grueling, requiring them to wear cumbersome PPE for “15 h” or from “9 AM until 2–4 PM…often missing snacks and lunch.” These extended-wear practices, born of necessity, contradict fundamental biosafety protocols for doffing and decontamination, dramatically increasing the risk of self-contamination and infection.
Theme 2: The Psychological Burden: Fear, Anxiety, and Burnout
The emotional and mental toll of working on the pandemic’s frontline was profound. Participants explicitly stated that “anxiety is one of the greatest problem[s]” and spoke of the “fear of getting infected.” This fear was twofold: a fear for their own safety and an even greater anxiety about potentially spreading the virus to their families, captured in the sentiment of “overthinking of family’s safety.” This constant state of high alert, combined with the systemic pressures described above, led to deep physical and emotional exhaustion. Respondents reported being “overworked and stressful,” suffering from “depression,” and experiencing “overfatigue” with “no work–life balance.” The experience of one participant who became COVID-19 positive along with their family and had to work at an isolation unit while symptomatic encapsulates the extreme nature of this burden. This exhaustion was linked to the social and familial sacrifice required by the job. The need to quarantine and isolate meant “not being able to go home and be with family” and “sacrificing family time,” severing critical support networks when they were needed most.
Theme 3: The Call for Value: Compensation and Professional Recognition
The demand for inadequate and delayed compensation was the most forceful and repeated comment in the second open-ended question. Participants stated unequivocally that “hazard pay should be given” and that there should be a “release of hazard pay and other compensation.” They lamented the “low compensation,” “no compensation,” and “low wage even if working overtime and on holidays.” This financial grievance was deeply intertwined with a sense of perceived inequity and lack of recognition. There was a palpable frustration that their critical role was being overlooked. The most telling comment on this subtheme came from a respondent who stated, “involvement of entire medical technology/clinical laboratory science community should be acknowledged for their efforts. Unfortunately, only nurses’ salary increased.” This statement reveals not only a feeling of being forgotten but also a degree of interprofessional resentment fueled by perceived disparities in recognition and reward. Despite these immense challenges, a resilient counternarrative of pride in service also emerged. A few respondents expressed that they were “proud to be a frontliner serving the people” and felt a sense of duty “to give… your best in serving fellow countrymen.” This duality highlights the complex motivations of a workforce that felt both a deep professional commitment and a profound sense of institutional neglect.
Discussion
A critical finding in our study emerged regarding prior professional development in biosafety: the vast majority of participants never had a formal biosafety training. Crucially, these participants were the very individuals who, despite their central role in the pandemic response, possessed a profound lack of formal, specialized training in biosafety. This highlights a significant systemic gap in proactive professional preparedness and points to a reactive approach to a critical training need, underscoring the absolute necessity and timeliness of the training intervention in this study. However, there may have been a form of selection bias with the attendees, assuming that those who have not attended prior training in biosafety are more likely to signify intent to participate in the training. Nevertheless, having shown that >75% of them declared that their job involves BRM shows that they were practicing the profession without formal BRM training, carrying the inherent risk of LAIs.
Modern biosafety practice emphasizes a culture of thorough assessment and continuous improvement. It advocates for a comprehensive, evidence-based, and transparent evaluation of risks on a case-by-case basis, moving beyond mere compliance with fixed rules to proactive risk management. Hence, the risk associated with a pathogen is not only an intrinsic property of the microbe but is also significantly influenced by the procedures employed, the volume of material handled, and the work environment.14,15 An SSRA systematically identifies hazards associated with laboratory work, evaluates the likelihood and consequences of undesirable events (such as exposure or release), and determines appropriate control measures to mitigate risk to an acceptable level.14,16 To operationalize this principle, the training conducted heavily utilized the risk assessment framework and templates detailed in the WHO’s Laboratory Biosafety Manual, 4th Edition, as a primary instructional guide
The consistency of high scores in the training evaluation demonstrates that the training was a successful, aligning with findings from international studies, which show that targeted, expert-led training significantly improves safety practices and knowledge. 17 In this context, several studies have highlighted the need for rapid adaptation and innovation in training programs to address emerging health risks while accommodating limitations imposed by lockdowns and movement restrictions.9,18 Online training modalities emerged as an attractive option during the pandemic due to their scalability, reduced logistical constraints, and ability to rapidly disseminate critical theoretical knowledge. 9 A recurring concern in the literature is the difficulty of effectively teaching and rigorously assessing hands-on laboratory skills in purely online formats.6,19 In traditional settings, direct supervision allows instructors to immediately correct procedural errors and provide tactile guidance, which is often diminished in virtual formats. 20 Conversely, online methodologies enable consistent dissemination of standardized content and allow participants to revisit modules at their own pace, a feature that is particularly valuable in rapidly evolving pandemic scenarios. 9 Nevertheless, the absence of direct hands-on components in digital platforms has raised concerns regarding the practical application of biosafety protocols. In our results, we showed that in situations where laboratory procedures are complex, the absence of a tangible demonstration may hinder the development of procedural confidence. Our study’s finding that participants strongly preferred a hybrid training setup—one that combines the flexibility of online delivery with the essential interpersonal and practical components of traditional face-to-face instruction—merits particular attention. Their mixed feedback on motivation and self-directed learning pace suggests that attending biosafety training classes while working depends on the institutional environment and may be attributed to participants juggling multiple responsibilities within their institutions, which is common in the Philippine setting. 6 Some participants often attend outside of and in addition to duty hours (rest days), while others attend on official duty. The findings may also indicate that participants’ value the practical sessions that complemented the lectures during the training. However, a significant limitation was that time constraints prevented the authors from quantifying the assessments relevant to this article. Nevertheless, the PhABOT facilitators made sure to correct and mentor participants who struggled to fully grasp the competencies until they successfully demonstrated their skills. It is therefore highly recommended that future training programs incorporate formal, graded practical examinations as a key component of the post-test evaluation.
A hybrid model capitalizes on the benefits of online platforms, such as broad accessibility and timely content updates, while simultaneously providing opportunities for hands-on demonstrations and interactive problem-solving that are vital for developing practical biosafety skills.9,21 In the Philippine context, where internet connectivity issues and a cultural preference for collaborative learning are noted, this integrated approach appears to offer a balanced solution, addressing both knowledge dissemination and skill acquisition effectively. Furthermore, by mitigating the shortcomings associated with pure online or in-person formats, a hybrid model can potentially lead to higher compliance rates and better overall biosafety performance in laboratory and clinical settings.22–24
As LMICs entered the pandemic, they faced preexisting constraints within their laboratory systems, including lack of infrastructure, shortage of trained personnel, fragile supply chains for diagnostics, and limited financial resources. Furthermore, the employment market for many HCPs is characterized by job insecurity, relying on short-term contracts that often lack the security and benefits of permanent positions. The pandemic magnified these existing fractures, pushing an already strained system closer to collapse.25–27 However, systemic pressures are not uniform, particularly in the Philippines, where significant staffing shortages and high workloads in primary care facilities are evident, especially in geographically isolated and disadvantaged areas. This situation reveals issues of resource maldistribution and an overreliance on temporary staffing solutions. 28 The unprecedented demands of the COVID-19 response threatened to overwhelm these already fragile systems, worsening existing vulnerabilities. Despite these challenges, many LMICs demonstrated considerable resilience in their strategic responses. Significant approach involved leveraging existing infectious disease control programs and infrastructure—such as those established for tuberculosis to support COVID-19 testing and related activities. 1 This highlights a crucial point that prior and well-sustained investment in general infectious disease infrastructure and human capacity in LMICs, even if not specifically designed for a pandemic of this nature, provided a vital foundational platform for a more effective COVID-19 response. Conversely, countries lacking such foundational capacity encountered significantly greater obstacles in scaling up their responses.
The MANOVA showed that while sociodemographic factors do not predict overall perceived relevance of biosafety and biosecurity topics, they do significantly predict the percentage of an individual’s job that involves BRM. This suggests that while the perceived importance of biosafety is universal, the actual distribution of biosafety-related duties is not random. Instead, it appears to be structured by institutional context (e.g., hospital vs. stand-alone lab) and possibly by seniority or experience (age). These indicate that the workforce is unanimously aware of the importance of biosafety, yet their engagement with biosafety tasks varies according to their specific roles and work environments. This reinforces the study’s core “preparedness paradox”; the issue lies not in individual motivation or understanding but in a systemic failure to create an environment where this understanding can be implemented safely and consistently. The factors that truly drive biosafety practices are more likely to be institutional and structural rather than personal attributes. However, our study lacks sufficient population characteristics to strengthen this hypothesis quantitatively and requires further investigation.
This study presents a surprising paradox that bridges the abovementioned findings in literature with actual field data in this study. On the one hand, the quantitative evaluation of the biosafety training program shows that HCPs in northern Philippines are motivated, capable, and eager to acquire the critical knowledge needed to protect themselves and their communities. On the other hand, their qualitative testimonies reveal a troubling work environment where systemic failures—chronic understaffing, severe resource scarcity, and institutional neglect—undermine their ability to apply this knowledge. The core contradiction illuminated by this research is the gap between training efficacy and practical feasibility. The significant increase in post-test scores indicates that HCPs learned and understood biosafety principles, from proper PPE usage to biowaste management and decontamination procedures. Yet, their own words reveal an environment where these principles were often difficult to implement. These firsthand accounts mirror the findings of systematic analyses of the Philippine healthcare system, which have utilized methodologies like the WHO’s Workload Indicators of Staffing Need to quantitatively identify high workload pressures and staffing shortages in certain regions. 28 The themes of “overwhelming workload,” “understaffing,” and “PPE shortages” that dominated the qualitative responses in our study are not isolated anecdotes; they are local manifestations of a national problem. The Philippine health system entered the pandemic already facing a massive exodus of its pool of health professionals.27,28 As HCPs fell ill, the burden on the remaining staff intensified, fueling burnout and accelerating resignations. One report found that in the first year and a half of the pandemic, a staggering 40% of nurses in private hospitals had resigned, further crippling the system’s capacity. 29 Similarly, the “limited PPE supply” mentioned by participants was a global challenge. The nation’s reliance on imported supplies, created a fragile supply chain that quickly buckled under pandemic-related demand and logistical disruptions. This scarcity directly led healthcare workers to adopt unsafe practices, such as reusing single-use equipment or improvising protective gear. 30 The disconnect between knowing what to do and being able to do it is a classical efficacy–implementation gap, driven by powerful environmental and systemic factors. 31 In the context of the Philippines, particularly in provincial settings like in this study, this gap is widened by a historical reliance on manual laboratory methods, which inherently increases the risk of exposure when ideal protocols cannot be strictly enforced due to overwhelming patient loads or lack of supplies. 31 The study’s findings powerfully demonstrate that individual knowledge, while a necessary condition for safety, is not sufficient. Without a supportive system that provides the necessary tools, time, and personnel, even the best training cannot translate into safe practice. The competence of the individual is effectively nullified by the constraints of the system.
The self-reported “anxiety,” “fear,” and “depression” among the study participants align with a large body of research documenting the pandemic’s severe mental health impact on HCPs. Studies found alarmingly high prevalence rates of anxiety (up to 70.7%) and depression (up to 51.0%) among this population. 32 The fear of contracting the virus and, more profoundly, of transmitting it to their families, was a primary and pervasive stressor that led to intense psychological distress and social isolation. 26 However, to fully capture the nature of this suffering, it is necessary to look beyond standard diagnostic labels and apply the concept of moral injury. Moral injury is distinct from burnout; it is the profound psychological distress that arises from “perpetrating, failing to prevent, or bearing witness to acts that transgress deeply held moral beliefs and expectations.” 33 The very success of the biosafety training may have, paradoxically, heightened their risk of moral injury. A trained professional who is acutely aware of the correct, safe protocol—the “right” way to do things—and is then forced by systemic constraints (e.g., no PPE, no time, no staff) to violate that protocol, experiences a profound sense of transgression and personal failure. They are caught in an impossible “lose-lose” choice where they must compromise safety standards to provide any care at all. 33 It is the dilemma of the laboratory staff who know their PPE is contaminated but cannot change it because there are no more available. This experience is often compounded by a sense of betrayal by the institutions that had a duty to provide the necessary resources and support but failed to do so—a key component of moral injury. 34 The participants in this study were not just tired or stressed; they were, in many cases, morally injured by a system that forced them to compromise the very standards of care and safety they were trained to uphold.
In summary, hybrid training approaches—integrating online theoretical modules with practical, in-person exercises—represent a promising strategy for enhancing biosafety education and compliance. These findings, corroborated by international studies as well as this effort in the Philippines, highlight the importance of adaptable, multifaceted training frameworks capable of addressing both the theoretical and practical challenges posed by emerging diseases in resource-limited settings. This study also revealed the duality of biosafety preparedness and realities among HCPs, particularly clinical laboratory scientists, in the Philippines during the COVID-19 pandemic. This study also opens several avenues for future inquiry. Longitudinal studies are needed to track the long-term mental health outcomes and career trajectories of this cohort of frontline workers to understand the full impact of their pandemic experience. Finally, there is a need for research into the development and implementation of a national, standardized biosafety curriculum that can be deployed across all healthcare education and training institutions in the Philippines to ensure a consistent and high level of baseline preparedness for future public health threats.
Authors’ Contributions
G.E.L.U. and A.P.Y. have contributed equally in this work, which includes conceptualization, field data collection, analysis and interpretation, writing, and finalization of this article. R.C.-N. and A.d.T. were major contributors in the data collection, organization, and analysis. R.V.D. was a major contributor in analysis, interpretation, and writing the article. All authors read and approved the final article.
Footnotes
Acknowledgments
The authors are grateful to all participants who consented to participate in the study. The authors also appreciate the support of the local health units during the implementation of this project.
Author Disclosure Statement
The authors declare no competing interests.
Funding Information
No funding was received for this article.
Data Availability
Supplemental Material
Supplemental Material
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.