
Abstract
When properly used and adequately maintained, a biological safety cabinet (BSC) provides protection to the laboratory worker, the products, and the environment. Knowledge about proper use of the BSC is therefore important. This study evaluated BSC usage knowledge and practices and the effect of prior experience on training outcomes. Thirteen participants randomly selected from research centers were evaluated through a structured questionnaire covering biosafety considerations involved in using a BSC as per the World Health Organization’s Laboratory Biosafety Manual, third edition. The questionnaire was administered before and after the training. Training was conducted using the NUITM-KEMRI biosafety training program, enhanced to include more modules on BSCs. Differences in the participants’ knowledge and practices regarding BSC usage were observed. After training, the participants were able to give correct responses. Furthermore, participants who had fewer years of experience showed the greatest improvement. Results indicate the need for proper training of laboratory workers early in their careers, coupled with close supervision, mentorship, and regular refresher training.
Keywords
Primary containment is defined as “the protection of personnel and the immediate laboratory from exposure to infectious agents, provided by both good microbiological techniques and use of appropriate safety equipment.” 1 Biological safety cabinets (BSCs) are primary containment equipment that have been used to protect experimental materials from cross-contamination and to protect the user and environment from infectious or hazardous aerosols generated when manipulating such materials. 2 The absence of protection for laboratory workers has largely been linked to laboratory-associated infections (LAIs). However, Pike 3 reported that >80% of LAIs studied were not traceable to incidents that may have caused them, indicating the need for close observation of all biosafety strategies. BSCs are capable of separating a laboratory worker from microorganisms and infectious aerosols produced during laboratory procedures. 4 When properly maintained and used in combination with good laboratory techniques, BSCs are effective in protecting the environment, reducing LAIs, and decreasing cross-contamination of experimental materials due to aerosol exposure.5,13
The first design of a BSC was a ventilated hood fitted with a vacuum pump that drew in air through a cotton filter. 4 Earlier, prototype clean air cubicles were designed to protect the materials being manipulated from environmental or worker-generated contamination rather than to protect the laboratory worker. To protect the worker, the earliest designs for primary containment devices were essentially nonventilated “boxes” built of wood and later of stainless steel, within which simple operations such as weighing materials could be accomplished. Early versions of ventilated cabinets; the forerunners of the Class I BSC, did not have adequate or controlled directional air movement. Thus, since the air was unfiltered, the cabinet was contaminated with environmental microorganisms and other undesirable particulate matter. In the 1940s, the High Efficiency Particulate Air (HEPA) filter was developed to provide dust-free work environments. 4 Later, BSCs incorporating many of the design features of today’s modern cabinet were made available, followed by the evolution of the laminar flow principle in the 1960s. Since then, different companies have developed and improved their safety cabinets to enhance protection.
There are 3 classes of BSCs: Class I, Class II, and Class III. Selection and use of the appropriate BSC must be based on a thorough risk assessment, considering the risk groups and nature of the organisms to be handled, manipulations to be conducted, equipment needed, and the nature of the hazards involved (biological, chemical, and/or radioactive). The overall risk must also be matched with the biosafety level and the chemical safety level of the laboratory used. 1
To ensure adequate protection for the operator, the laboratory environment, and the experimental materials, one must therefore choose the appropriate type of BSC, adhere to good microbiological practices, and ensure that the BSC is properly maintained and serviced. To achieve this, every employee working in a BSC must be adequately trained on its correct use to a level of competence that ensures that each can safely work with infectious agents.
Nagasaki University Institute of Tropical Medicine, in collaboration with Kenya Medical Research Institute (NUITM-KEMRI), conducts annual biosafety training workshops for new biosafety level 3 users. The program is aimed at enhancing competency and proficiency among new biosafety level 3 users and promoting appropriate behaviors and practices that enhance biosafety and biosecurity. The training has 3 phases: initial assessment, training phase (including theory and hands-on practice), and a final assessment.6,7 The objective of this study was to evaluate participants’ knowledge and practical skills in BSC usage. The impact of biosafety and biosecurity training on BSC usage, as well as the effect of prior experience on training outcomes, were also examined.
Materials and Method
Thirteen laboratory workers attending a 3-day biosafety training workshop participated in the study. These were drawn from parasitology, bacteriology and virology research laboratories. Before commencement of the study, participants received a detailed description of the study and consented to participate in the survey.
The study had 3 components: a preworkshop survey, training program delivery, and a postworkshop survey. The NUITM-KEMRI biosafety training program was used. 6 Usually, the training program is delivered through an annual workshop and divided into initial assessment, training phase, and final assessment sessions. In the initial assessment session, a written test is given to establish the participants’ initial knowledge, which also helps to identify training needs. A similar test is administered during the final assessment phase. The training phase covers biosafety and biosecurity theory and practicum. In this study, the survey questionnaire was administered to the participants before and after training. Further, the training program was adjusted to include more theory and practical modules on BSCs to provide more comprehensive training on proper BSC usage. Practical training was achieved through a demonstration and a hands-on session with the participants divided randomly into 3 groups to allow for closer instruction and supervision. Table 1 shows a description of the aspects of BSCs covered in this study.
BSC Aspects Covered in the Training Workshop.
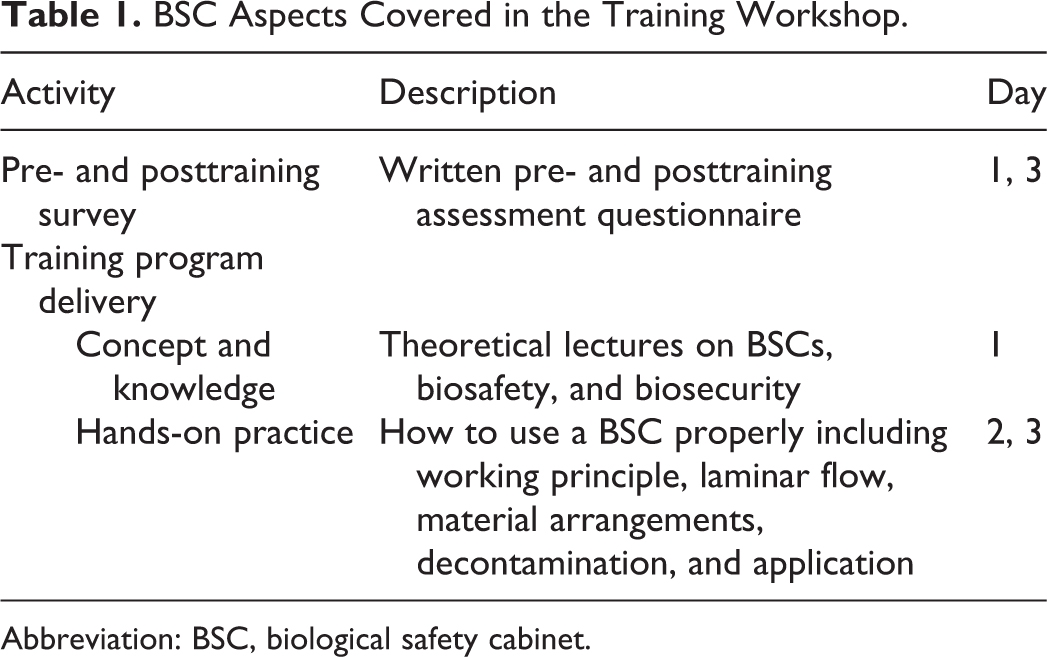
Abbreviation: BSC, biological safety cabinet.
Design of the survey questionnaire was based on guidelines on BSC usage from the World Health Organization’s (WHO) Laboratory Biosafety Manual, third edition, 5 and consisted of closed- and open-ended questions. Closed questions were designed to qualify a statement through true/false answers, while the open-ended questions allowed participants to support their answers by giving their opinions. The questionnaire included questions on location of a BSC, material placement, open flames, operation and maintenance, and supplementary information regarding usage of a BSC.
The preworkshop survey examined the diversity in knowledge and practices among the participants regarding usage of BSCs, while the postworkshop survey assessed the impact of the training. Data was analyzed using Stata 13. Descriptive statics were used to summarize the data, while differences in means were examined using Student’s t test.
Results
Of the 13 participants, there were 6 (46%) virologists, 5 (38%) bacteriologists, and 2 (16%) parasitologists. The length of their experience ranged from half a year to >20 years. The most commonly used BSC was BSC class II.
Out of the 13 WHO biosafety considerations regarding use of a BSC, 5 10 were included in the survey as shown in Table 2. The other 3 biosafety considerations (certification, alarms, and operator) were emphasized during the theoretical and hands-on training.
Summary of the Participants’ Performance as per the Biosafety Considerations.a
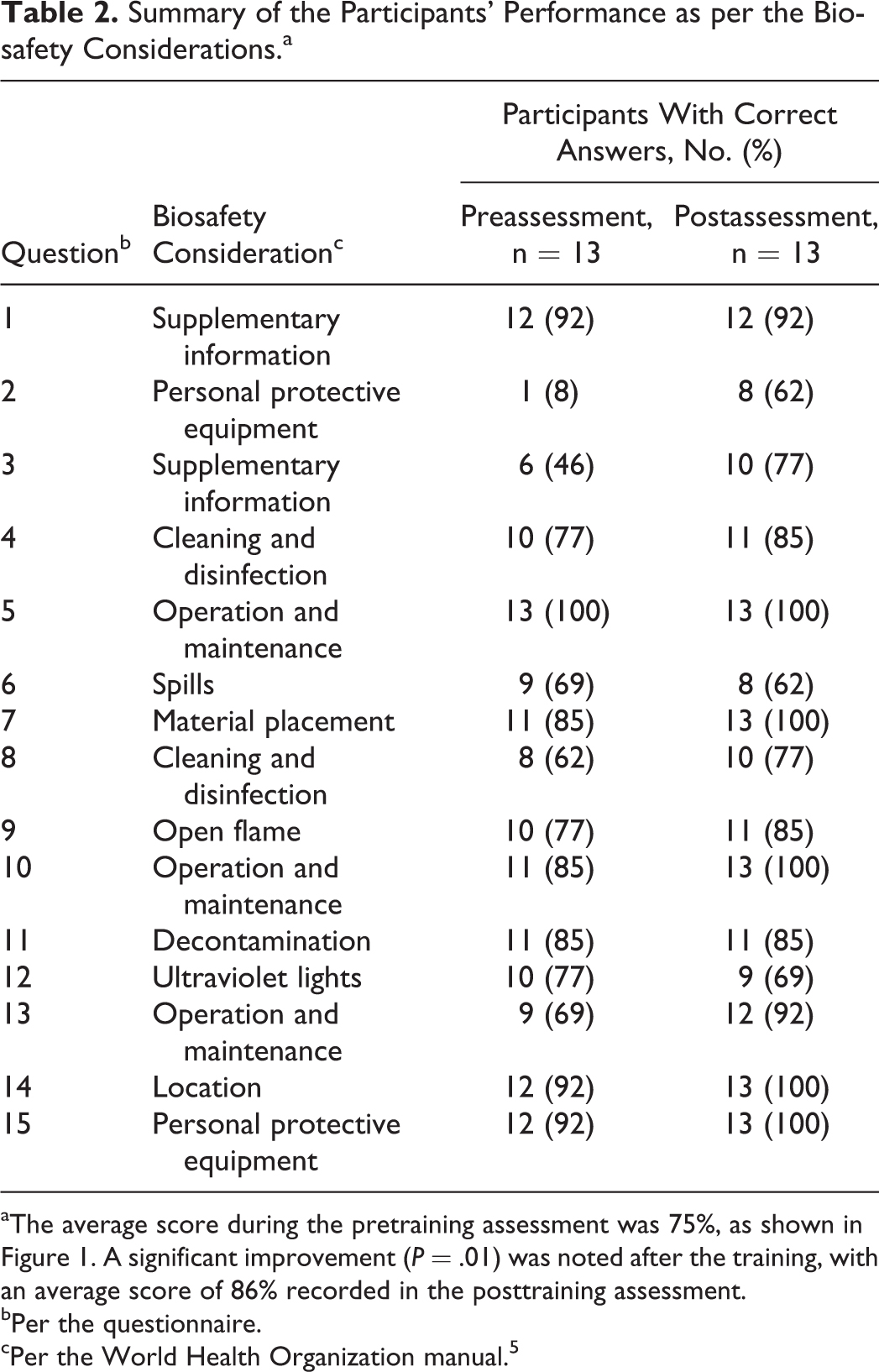
The average score during the pretraining assessment was 75%, as shown in Figure 1. A significant improvement (P = .01) was noted after the training, with an average score of 86% recorded in the posttraining assessment.
Per the questionnaire.
Per the World Health Organization manual. 5
The location consideration presented the highest score, at 92%. The greatest variation was observed on questions covering personal protective equipment (PPE), with an average score of only 50%. On the open-ended questions, some participants seemed to be aware of a concept, but in some instances they could not correctly justify their responses.
On grouping participants based on length of experience, 5 participants had <5 years of experience. This group had a lower average score (68%) in the pretraining assessment but presented a significant improvement (P = .02) after the training. The other group of participants, with >5 years of experience (n = 8), scored 80% in the pretraining assessment and 83% in the posttraining assessment, as shown in Figure 2. This improvement was not significant. Although no significant difference in the average scores of the 2 groups after training was noted, the scores of the participants with <5 years of experience were noticeably higher (Figure 2).
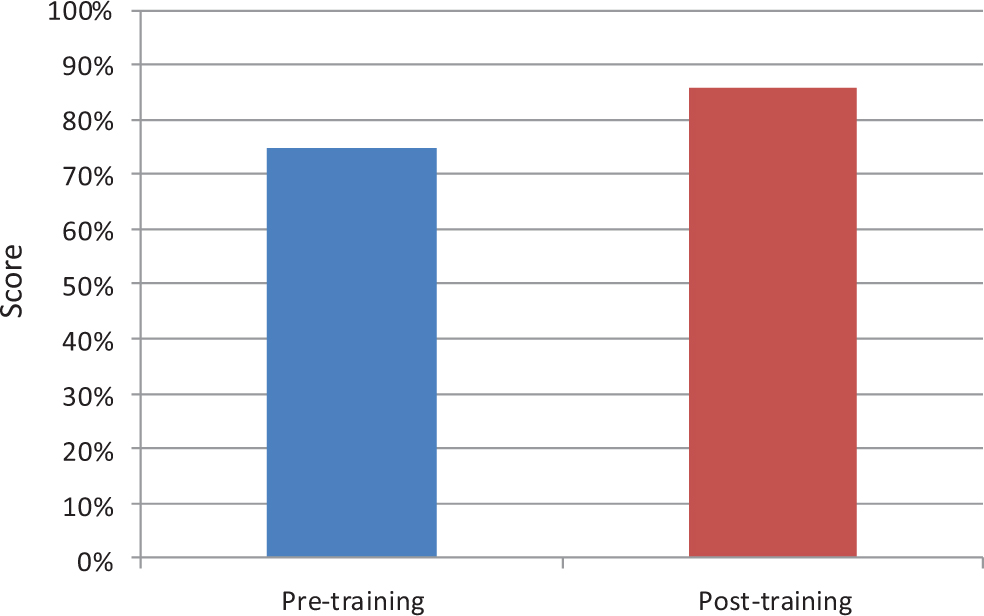
Mean score of pre- and posttraining survey scores (n = 13).
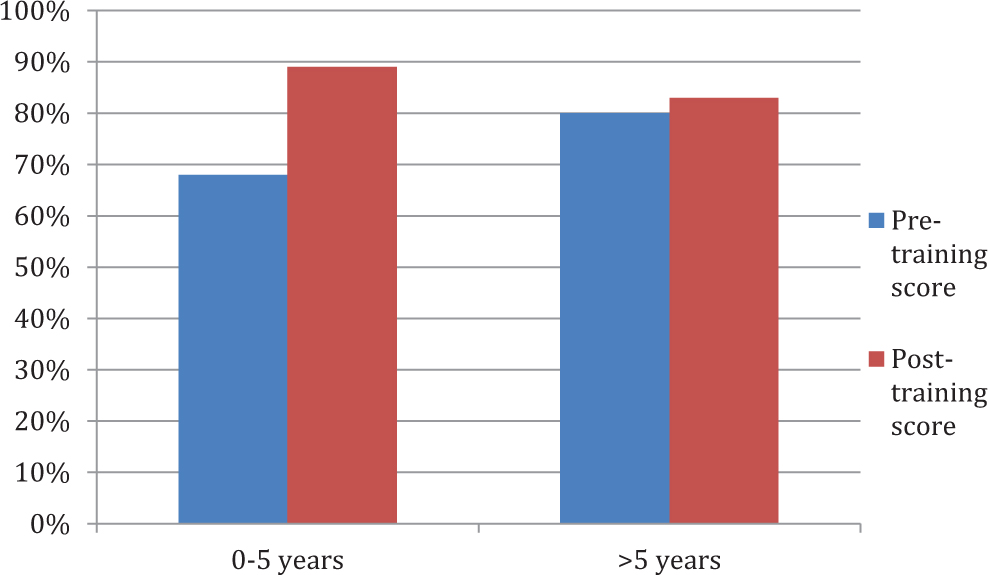
Pre- and posttraining scores by duration of experience.
Discussion
BSCs are capable of containing contagious materials. However, several biosafety considerations must be observed for them to function optimally. These, coupled with good microbiology practices, ensure protection of the user, product, and the environment. The WHO biosafety manual provides 13 specifications covering the entire spectrum of proper usage of a BSC. These are location, operators, material placement, operation and maintenance, UV light, open flames, spills, certification, cleaning and disinfection, decontamination, PPE, alarms, and supplementary information. All 13 biosafety considerations were emphasized during the theoretical and hands-on training. However, only 10 were included in the survey as shown in Table 2. Given the role played by BSCs in biosafety, knowledge and strict adherence to these biosafety considerations among laboratory workers are both of utmost importance.
In this study, diversity in knowledge and practices in usage of BSCs was observed. Of the 10 biosafety considerations, the highest agreement occurred in questions covering location of a BSC. The correct answer rate was 92%, suggesting that the participants had uniform basic knowledge about location conditions for a BSC in the laboratory. However, only 50% of them correctly explained that the location consideration aims to maintain directional airflow as specified in the WHO biosafety manual. 5 Concerning operation and maintenance, material placement, and decontamination of BSCs, 85% of the participants gave correct responses in each category. On the prior, although the majority of the participants agreed that one should wait a while before putting in materials after switching on the BSC, some participants could not correctly justify the statement. For instance, most participants observed that the purpose of the waiting period was to allow for airflow stabilization. Other participants explained that the waiting period was to allow for proper circulation of air. Time lag to allow the BSC to start was also indicated. The WHO biosafety manual specifies that a BSC should be turned on at least 5 minutes before beginning work and turned off 5 minutes after completing work to allow it to expel contaminated air.
Concerning choice of disinfectant under cleaning and disinfection biosafety consideration, 77% of the participants agreed that sodium hypochlorite is not the best disinfectant for BSC surfaces. 16% of the explanations cited the effectiveness of a specific disinfectant for the target organisms; 56% named prevention of corrosion of the BSC surface; and 16% provided an incorrect explanation. According to the WHO biosafety manual, the disinfectant of choice should be effective against the target organisms or one that can kill any microorganisms found inside the cabinet. 5 The highest diversity was observed on the questions covering PPE, where only 1 participant correctly answered that the criteria for choosing the type of PPE is determined by the biosafety level of the laboratory or the nature of material being worked on, rather than the class of BSC in use.
Hakim et al 8 observed similar diverseness in biosafety knowledge and practices while studying routine biosafety measures and proper waste disposal practices among health workers. Although BSCs from different manufacturers may have slight structural differences, their installation and operational procedures are rather universal. Discrepancies about their usage and application observed in this survey could have stemmed from personal and institutional-level factors. Among these is lack of proper training. In some institutions, laboratory workers are hardly provided with initial training on biosafety and biosecurity, with most relying on prior academic knowledge and knowledge acquired on the job. Subsequently, most laboratory workers are not thoroughly familiar with core biosafety and biosecurity principles, although they can apply the technologies. For instance, in the preworkshop assessment, the participants were not entirely clear on the difference between “level” and “class” in identifying the BSC that they were using. Given the role played by BSCs in containing infectious agents, good BSC user knowledge and skills are necessary. Initial and refresher training, combining theoretical and practical concepts, can help to increase knowledge and competence of laboratory staff while enhancing biosafety and biosecurity. Training must also factor in differences in research facilities and activities since procedures vary from organism to organism or laboratory to laboratory. Training should therefore allow for facility-specific adaptation. 9
Weak enforcement of biosafety and biosecurity strategies could also explain observed diversity. Although the WHO biosafety manual provides allows for modification of biosafety and biosecurity regulations to fit a laboratory’s operations, universal specifications are also provided that apply to all laboratories regardless of the organism handled. Poor enforcement reduces adherence to safety principles, which increases the risk of exposure to hazardous agents. 10 Moreover, differences in the way that different laboratories adapt WHO guidelines to fit their settings could further explain the differences in knowledge and practices observed.
To some extent, institutional support may also influence biosafety knowledge and practices. Institutional factors, such as limited funding, could affect the stability and efficiency of biosafety infrastructure. Weak biosafety infrastructure limits knowledge and adherence to safety regulations due to factors such as absence of biosafety and biosecurity equipment or poor mentorship and supervision.
An average improvement of 11% was observed after training, although there was increased disparity on the spills and UV irradiation biosafety consideration. In the case of a large spillage in a BSC, some participants stated that only the working surface should be decontaminated. However, the WHO biosafety manual recommends that not only the working surface but also the drainage system of the BSC must be decontaminated by following up the spill with a disinfectant. 5 The drainage vent should be closed during this operation and adequate time allowed for contact with the disinfectant. As for the UV irradiation, some participants stated that it can be used as the sole method for decontamination. However, UV irradiation alone is not recommended, since it is only a surface decontaminant and its effectiveness is limited by factors such as distance.
Generally, more participants gave correct responses to the survey questions and provided more correct explanations of their responses after training. This suggests that the training increased knowledge on BSC usage among the participants and biosafety and biosecurity awareness at large. A similar improvement in knowledge and competence after a biosafety training was observed by Inoue et al 7 while evaluating the effectiveness of the NUITM-KEMRI training program. Basically, training has been identified as an effective approach to increase the competence of laboratory workers and their biosafety and biosecurity knowledge, as well as to create awareness about the hazards posed by research and diagnostic laboratories. 10 Packaging these concepts into a program and delivering them through a formal training approach further facilitates learning, application, and adherence.7,11
On comparing training outcomes among participants with <5 and >5 years of experience, those with fewer years of experience presented a significant improvement in the postworkshop survey although they had a lower average score during the preworkshop survey. Chaudry et al 12 and Inoue et al 7 reported similar outcomes while assessing biosafety practices among undergraduates and postgraduates and biosafety training outcomes in exposed and unexposed participants, respectively. On the contrary, those with >5 years of experience would be expected to show greater improvement after the training, due to the higher level of understanding that comes with increased experience. A possible explanation could be that the more experienced participants had difficulties adopting new concepts and practices because they were different from those that they were used to. In most instances, laboratory workers are not offered formal biosafety and biosecurity training upon their initial placement in a laboratory setting and probably in subsequent placements as well. Therefore, laboratory workers mostly rely on on-the-job learning, majorly conducted by more experienced staff. Such training may not necessarily be comprehensive or up-to-date. With more time spent adhering to such concepts, more experienced laboratory workers may find adopting standardized practices difficult.
In conclusion, diversity in BSC usage knowledge and practices, the importance of biosafety and biosecurity training, and the confounding effect of prior experience on biosafety training outcomes were observed in this study. Generally, core biosafety and biosecurity principles as stipulated in the WHO biosafety manual should be uniform across all laboratories, with minor modifications to fit a laboratory’s settings and activities. Absence of expected uniformity therefore reveals gaps in knowledge on usage of BSCs and maybe in biosafety and biosecurity in general. To address these, proper training should be conducted. Training laboratory workers before they begin working in the laboratory may be best. Whether conducted at the initial placement or in the course of a laboratorian’s work life, such training should be sufficiently comprehensive yet based on recommended principles to enable a laboratory worker to work safely in a different laboratory. It should be accompanied by mentoring and supervision until capability to work independently is attained, with subsequent regular refresher training. Given the small sample used in this survey, a bigger study is recommended to fully ascertain the role of training in improving BSC biosafety knowledge and practices.
Training Module for Biological Safety Cabinets: Proper Use and Maintenance
Training modules
Module 1: Principles of containment
Module 2: Classes and types of BSCs
Module 3: Proper use and maintenance
Module 4: Decontamination and certification
Module 1: Principles of containment, Course overview
This module provides an overview of how BSCs function and how they provide protection through containment. It describes the principles of protection and the levels of protection to the environment, product, and personnel offered by various types of cabinets. The module also provides an essential background to understanding HEPA filters and their mechanisms of operation.
At the end of this module, students are expected to have mastered how BSCs offer protection through containment and the basic concepts of how HEPA filters operate.
Course content
Introduction
How a BSC provides protection through containment
HEPA filter
How HEPA filters operate
Module 2: Classes and types of BSCs, Course overview
This module provides an overview of the three classes of BSCs. Differences among the classes regarding intake air velocity, plenum pressure, air recirculation and exhaust, and common uses are explained in detail. Key considerations when choosing the appropriate BSC for a certain kind of procedure are also described.
At the end of this module, students are expected to know the different classes of BSCs and their differentiating aspects. They are also expected to know how to choose the appropriate BSC for a certain kind of laboratory procedure and how to work safely in a BSC.
Course content
Introduction
Classes of BSCs
Choosing the appropriate BSC iv). Proper placement of a BSC
Module 3: Proper use and maintenance, Course overview
This module focuses on safe work procedures and proper maintenance of BSCs. The module describes the key considerations when preparing to work in a BSC, while working, and after completing the work. These considerations are aimed at ensuring personnel, product, and environmental protection while working in a BSC. Students are also trained on how to maintain a BSC including certification. Necessary operation tools, such as standard operating procedures (SOPs) and maintenance sheets, are also described.
At the end of this module, students should have a comprehensive understanding of how to safely work in a BSC and how to adequately maintain them.
Course content
Introduction
Planning the work
Placing the materials
Working in a BSC
Maintenance
BSC SOPs
Emergency procedures
Module 4: Decontamination and certification, Course overview
While working in a BSC with infectious materials, inevitably the BSC surface will be contaminated and at times spills will occur. This module provides information on how and when to decontaminate a BSC. The various types and classes of disinfectants and methods of decontamination are explained in detail including the key considerations when choosing a disinfectant. How to handle spills within a BSC is also described.
At the end of this module, students are expected to know how and when to decontaminate and disinfect a BSC. They are also expected to know how to choose the most appropriate disinfectant while working with a certain infectious material.
Course content
Introduction
When to decontaminate a BSC
Methods of decontamination
Classes of disinfectants
Risk assessment considerations when choosing a disinfectant
Handling spills within a BSC
UV lights
Training Module for Practicum (Demonstrations and Hands-On Practice)
Practicum (demonstration and hands-on practice)
Practicum is very important in strengthening trainees’ knowledge and skills. This session is conducted through demonstration and hands-on practice, in two phases.
The first phase focuses on the correct procedure and considerations before, during, and after working in a BSC. The trainer demonstrates the correct procedure during the following occurrences:
Before working in a BSC
Planning the work Turning on a BSC and decontamination Arrangement/placement of materials in a BSC While working in a BSC
Arm movements Material/item placement, sterilization of loops Cleaning up spills Disposal of wastes After completing work
Clearing the work surface Decontaminating the work surface Filing the BSC usage records
The second phase is a trainee-led, hands-on practice session covering an actual work session in the BSC. In executing the work session, the trainee is expected to adhere to the recommended procedures and techniques as earlier demonstrated by the trainer. Each practical session takes about one hour and allows for both practice of the concepts learned and assessment of knowledge acquisition. The trainee executes the session based on instructions provided on a task card, with the trainer playing a supervisory role. During this time, the trainer assesses the correctness of the trainee’s actions. Each trainee undergoes the assessment individually.
Footnotes
Acknowledgments
We thank The Director of KEMRI for providing technical support for our project activities. We further express our appreciation to the biosafety trainers and BSL-3 laboratory staff for facilitating our annual biosafety workshops.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) confirmed receipt of the following financial support for the research, authorship, and/or publication of this article: This study was supported by grant-in-aid for scientific research, Japan (Research B:15H05286).