
Abstract
Objective:
Effective, non-pharmacological approaches to pain management for people with advanced cancer that can enhance quality of life while minimizing adverse effects are urgently needed. While music therapy has been demonstrated to be effective in reducing pain and improving pain-related outcomes across various patient populations, it has not been specifically examined in addressing chronic pain among people with advanced cancer. This study aims to enhance understanding of how people with advanced cancer experience music therapy for pain management.
Methods:
As part of a mixed methods intervention trial, we conducted semi-structured interviews with a subsample of 25 outpatients with advanced cancer (Stage 3 & 4) and chronic pain who had participated in 6 music therapy sessions designed to address psychosocial factors known to exacerbate the experience of chronic pain. We analyzed the interview transcripts using theoretical thematic analysis.
Results:
The findings suggest that engagement in music therapy enhanced psychosocial well-being, contributed to better pain management, and helped build early therapeutic rapport. Participants emphasized that co-creating and engaging in active music making enhanced their self-efficacy as they learned to use music to improve emotional regulation skills, increase physical functioning, relax, and decrease their medication use.
Conclusion:
Music therapy’s role in pain management goes beyond distraction and relaxation to include stress reduction, emotional expression, enhanced self-efficacy, and therapeutic connection and support through shared musical experiences. Incorporating board-certified music therapists into psycho-oncology care teams can help enable patients to effectively harness music as a daily tool for symptom management.
Introduction
Managing chronic pain remains one of the most significant challenges in advanced cancer care, affecting approximately 60% to 80% of patients.1 -3 There is a need for effective, non-pharmacological approaches to pain management as healthcare providers seek to develop more comprehensive pain management strategies that can enhance quality of life while minimizing adverse effects.
Music therapy (MT) is increasingly used as a non-pharmacological intervention for pain management across healthcare settings. This growing acceptance is supported by numerous systematic reviews demonstrating its effectiveness in reducing pain and improving pain-related outcomes across various patient populations.4 -6 Music therapy is the use of music experiences within a therapeutic relationship with a trained music therapist to support a participant’s resources and goals including optimization of their physical, social, communicative, emotional, cognitive, and spiritual health and well-being. 7 It encompasses various music interventions, including active music making, songwriting, music listening, and music-guided relaxation and is a recommended therapy for managing anxiety and depression during active cancer treatment. 8 While evidence supports MT’s effectiveness for cancer-related pain, 4 there remains a notable gap in research examining its role in addressing chronic pain among people with advanced cancer.
This paper presents qualitative findings from a mixed methods research study examining a 6-week MT protocol for chronic pain management in people with advanced cancer. The qualitative analysis explored participants’ experiences of the MT sessions and their personal insights into if and how MT influenced their pain management and well-being.
Methods
Study Design
To provide context for the qualitative findings reported here, we briefly describe the original clinical trial. The original study embedded qualitative data within a randomized controlled trial (RCT) comparing a 6-week MT protocol with a 6-week attention control condition. The primary aim was to examine anxiety, mood, emotional support, and pain-related self-efficacy as potential mediators of MT for pain interference and pain intensity. The results suggested that MT for chronic pain management was fully mediated through self-efficacy and are reported elsewhere. 9 The aim of the qualitative portion of the study was to enhance understanding of how participants experienced the MT intervention and how the MT sessions may have contributed to treatment benefits. Clinical trial registration: Clinicaltrials.gov NCT03432247.
Study Sites and Participants
The clinical trial was conducted at 2 major hospitals, including an NCI-Designated Comprehensive Cancer Center, on the East Coast of the United States between January 2018 and July 2021. Outpatients with advanced cancer (Stage 3 & 4) and chronic cancer pain were eligible to participate if they had (a) a diagnosis of locally advanced cancer; (b) cancer pain ≥ 4 on a 0 to 10 NRS; (c) chronic pain (≥3 months); and (d) Karnofsky score of ≥60. Patients with an expected survival of less than 3 months, within 3 weeks post-surgery, unable to speak or write in English, or moderate to severe hearing impairment were not eligible. The study was approved by the Drexel University Institutional Review Board (protocol: 1709005627) and participants provided informed consent.
Music Therapy Intervention
The MT protocol consisted of 6 individual sessions, each lasting 45 to 60 minutes, delivered by master’s level board-certified music therapists at the hospitals. The protocol was designed to address psychosocial factors known to exacerbate the experience of chronic pain, including anxiety, depressed mood, insufficient emotional support, limited emotional expressivity, and feelings of helplessness (Table 1). The program emphasized hands-on participation rather than passive listening, empowering patients with tools they could use independently after completing the protocol. Due to the COVID-19 pandemic, sessions transitioned from in-person to remote delivery. This shift created some technical challenges for interactive music making, particularly due to video call audio delays and the inability to share instruments directly. To facilitate active music engagement, we mailed egg shakers to participants and utilized Zoom’s built-in features, such as the chat function and whiteboard, to facilitate collaborative activities like songwriting.
Music Therapy Protocol Outline.

Semi-Structured Interviews
We invited a subsample of 25 participants to a follow-up interview after completion of their MT sessions. We used maximum variation sampling related to gender and patient global impression of change scores. 10 These 30-minute semi-structured interviews were conducted by research assistants trained in qualitative interviewing. The purpose of the interviews was to (1) document participants’ personal experiences with the MT intervention including potential benefits and (2) explore their perspectives on how MT contributed to any perceived benefits (Supplemental Materials). All interviews were recorded and transcribed verbatim.
Data Analysis
We conducted thematic analysis of the interview transcripts using MAXQDA. 11 The transcripts were coded by 4 coders—CC, MYL, CL, and LG—using theoretical thematic analysis procedures outlined by Braun and Clarke.12,13 This approach identifies patterns in the data based on predetermined research questions. Our analysis was guided by 3 key questions: (1) How did participants describe their experience of MT? (2) What benefits or potential negative effects did participants report? and (3) For those who experienced benefits, how did they understand the connection between MT and these improvements?
Results
Participants
A total of 25 participants completed an interview. Participant demographics and clinical characteristics are summarized in Table 2.
Participant Demographics and Clinical Characteristics (N = 25).

Interview Findings
Individuals who engaged in MT learned that music can be a resource to alleviate cancer-related psychosocial stressors and enhance psychosocial well-being (Theme 1), resulting in better pain management (Theme 2). The findings suggest that the quality of the therapeutic relationship is important and music plays a role in building early therapeutic rapport (Theme 3; Table 3). Many participants shared that music was already a part of their daily lives, but that MT “gave me that opportunity to use music in a different way. It was a different tool for me at this point. I was able to use it as a form of medicine. And that was helpful for me.” Other participants shared that it expanded their view of what music could do:
I learned so much. . . I kind of already had the idea that music was so helpful just in mood alteration but I didn’t really realize how it could affect, not thinking about it, and then possibly like eliminating or lessening pain in the body.
Themes with Supporting Quotes.
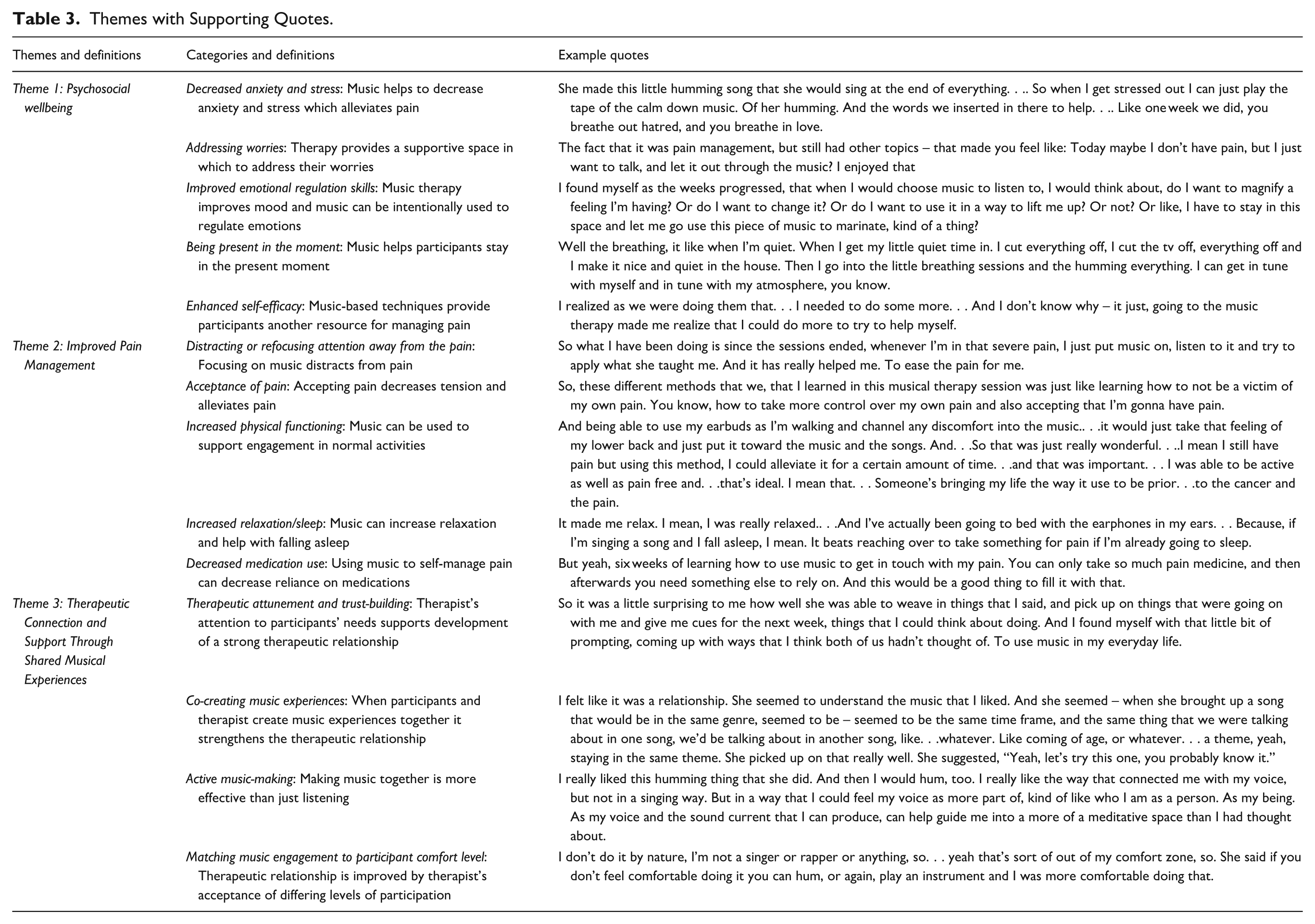
Theme 1: Enhanced Psychosocial Wellbeing
Participants shared that MT enhanced their psychosocial well-being by shifting their emotional and cognitive perspectives, specifically by (1) decreasing anxiety and stress; (2) addressing worries; (3) improving emotional regulation skills; and (4) being present in the moment; and (5) enhancing self-efficacy. Engaging in music experiences reduced anxiety and stress, leading to a sense of calmness. Decreased anxiety, in turn, helped with pain management, as one participant shared, “it makes it a lot easier to go through that pain without having the pain plus the anxiety from the day on top of that.” Participants appreciated having learned how to use music more purposively for dealing with day-to-day stress as illustrated in this quote: “I actually use that. . .almost on a day-to-day basis, as far as picking songs that I know will put me in a calm state if I am having like a rough patch throughout the day.”
The data indicated that the sessions provided space to address worries and discuss cancer-related experiences. Furthermore, several participants pointed out that MT may be particularly helpful for people who struggle with sharing their feelings. One participant explained,
Now unless you got cancer – even though you have family members who love you and everything, they don’t know. . .So this helps open things up. People that have cancer and don’t want to talk about it. Or stay closed. The music could help open them up.
Participants reported that the MT sessions helped to improve their mood. Numerous comments pointed to an increased and more intentional use of music at home to alter their mood. Music also helped them be present in the moment and in tune with themselves. Some reported experiencing a state of flow (ie, full absorption in the music), as reflected in this quote:
I was really in the zone, as they say. I didn’t have the thoughts coming in and out of my head. Just super in the moment and letting myself just be. Those were the moments where I was most in tune with myself.
Some explicitly connected staying in the present moment with pain relief, saying “I don’t think about the pain, I just think about, in that moment, where I am in that song.” Participant comments also suggested that through MT they felt more in control over their pain, leading to increased self-efficacy.
Theme 2: Improved Pain Management
Participants shared that MT helped them with pain management by (1) distracting or refocusing attention away from the pain, (2) acceptance of pain, (3) increased physical functioning, (4) increased relaxation/sleep, and (5) decreased medication use. While some participants described using music as a simple distraction, others described actively focusing their attention onto the music:
Sometimes when I’m in pain. . . I listen to the music, and then it sort of takes my mind off of what I’m going through. So it’s like a form of redirecting that energy and putting in a safe, comfortable place.
Participants also shared that participating in MT had led them to better accept their pain, which resulted in increased emotional resilience. One participant explained:
Cause a lot of the times when you have pain, it’s like we wanna just act like we don’t have the pain to numb it, but it actually makes us feel worse.. . . Yes, I’m experiencing pain right now, but I can still enjoy this moment and use different therapeutic ways to kind of help control that pain instead of putting more energy into acting like it don’t exist.
The data furthermore suggest enhanced physical functioning as music-based strategies helped improve coping and perceived control over pain. Participants shared that music had helped them return to their regular routines, including the completion of activities of daily living such as cooking.
Some participants discussed using music to help them go to sleep. Noteworthy is that some used active music making to reduce sleep latency: “I’d start humming a song or trying to sing it – I’d be laying in bed and getting in a lot of pain. . .it took my mind off the pain and let me fall asleep.” Participants shared that using music strategies enabled them to decrease their use of pain medications. For some, using music instead of pain medication at bedtime was particularly helpful: “I use it more, especially at night when I’m getting ready to lay down. It helps me get into that relaxed mode, and just try – because I’m trying to wean myself off the medication.”
Even though many participants talked about enhanced pain management because of their participation in MT, some voiced initial skepticism about whether MT would be able to reduce their pain. One participant stated, “mainly because of where my pain level is, it was – for me, in my mind, it’s like, “yeah, okay. Music’s going to help my pain level? Like, that didn’t make any sense to me.” The participant continued that after experiencing MT “it definitely opened my eyes to the possibility of how music could help with the pain. It helped so much that now I use it more.” One participant, however, found that the sessions did not help them: “I was just trying to be positive about it helping me with the pain. I mean, I’m disappointed that it didn’t. But I have to be honest, I kind of wasn’t really expecting it to. . .because of my pain level.”
Theme 3: Therapeutic Connection and Support Through Shared Musical Experiences
The quality of the therapeutic relationship seemed to have played a significant role in the benefits reported by participants. Besides therapeutic attunement and trust-building, many comments spoke to the essential role of music in facilitating early therapeutic rapport, specifically, co-creating music experiences, active music making, and matching music engagement to participant comfort level.
Participants frequently talked about how the therapist’s qualities, such as active listening and creating a nonjudgmental space, helped them feel deeply cared for. They talked about MT-specific experiences, such as co-creating music experiences with the therapist, as key factors in establishing therapeutic rapport. One important aspect of co-creation was the music therapist honoring their music preferences and learning their music, which they viewed as evidence of the therapist’s investment in music that was meaningful to them. One participant shared, “The fact that she could jump online and – even if she didn’t know the song – be able to find it and sing along with me, I loved that.” Another shared that they appreciated the therapist’s willingness to change instruments to meet their musical preferences: “Once we transitioned to the piano. . .that one was even better for me, because she knew that I loved the piano more than the guitar.” Participants felt cared for when music therapists created personalized musical experiences based on their conversations or created songs based on their life experiences: “And it’s funny because we talking about my life experiences and she made songs out of them. So, we laughing about, whether I told her about a good experience or a bad experience.”
Many participants emphasized the value of actively engaging with music rather than passively listening. Some found that humming and singing enhanced their body awareness and mindfulness practices. Others appreciated the use of live music in the sessions and the opportunity to play different instruments. Some participants noted feeling at ease in the sessions because the music therapist honored and afforded participants agency regarding their level of music engagement (eg, being given the option to hum or play instruments rather than sing). This feeling of comfort also contributed to participants’ willingness to try using music for pain management in ways they previously had not considered, as explained by a participant, “She made me comfortable, she definitely helped me step out of the box a little bit, with being more open and using music to my advantage to help me deflect the pain.”
Discussion
This qualitative study explored the experiences of people with advanced cancer of a 6-week MT protocol. The thematic analysis indicates that MT improved psychosocial well-being which resulted in better pain management. Besides in-session benefits, participants learned valuable music-based strategies for the self-management of stress, mood, and pain in their daily lives. The findings also point to the vital role of music in establishing early therapeutic rapport and facilitating emotional expression within the context of a supportive therapeutic relationship.
Research has consistently shown that music-based interventions effectively reduce anxiety in cancer patients, as demonstrated by multiple systematic reviews.4,13 However, despite regularly listening to music, many participants in our study had not yet considered using it deliberately as a stress management tool. Moreover, they described how music helped reduce their pain by lowering anxiety and lifting their mood. These findings align with research by Bradt et al, 14 which suggests that music’s therapeutic potential for managing chronic pain remains largely untapped in everyday life.
Participants also shared insights regarding music’s capacity to facilitate emotional expression. Music therapists are trained to create music experiences that help people connect with their emotions, guide them through active and receptive music experiences for deeper emotional engagement, and teach them how to use music for emotion regulation. Many participants reported that engaging with music helped them express their emotions and concerns about their cancer journey more freely. Emotional expression plays a vital role in reducing psychological distress and enhancing quality of life in people with cancer and can help reduce perceived pain.15,16 Music therapy may offer a viable alternative for people who struggle to verbalize their feelings and who may experience traditional talk therapy sessions as anxiety-provoking and uncomfortable. Additionally, MT may be indicated for those who do not have the verbal capacities or desire to reflect upon and discuss emotions evoked by the music. Music therapy may therefore present a lower initial barrier for people in need of psycho-oncology support services.
While some participants described using music listening for distraction or relaxation, many study participants emphasized that actively engaging with music in the music therapy sessions as well as outside of the sessions was more effective for pain management than passive listening. They reported that the focused listening techniques proved more beneficial than their previous casual listening habits. This aligns with research suggesting that active listening promotes absorption in music, creating a flow-like state in which bodily discomfort becomes less noticeable.17,18 Participants found singing, a key component of our MT protocol, particularly effective for pain management. One participant noted that singing along with the music helped her to maintain connection with the music rather than becoming detached. Singing, humming, and chanting create bodily vibrations that enhance physical awareness and offer a positive, creative way to connect with one’s body—a stark contrast to the negative relationship many develop with a body they perceive as failing them.14,19 The beneficial effects of singing on pain management were also reported in a prior RCT that compared the effects of a vocal music therapy protocol—a group intervention that uses singing, chanting, and vocal improvisations—to a waitlist control condition in people with benign chronic pain. Medium treatment effects for pain interference were supported by qualitative data, which suggested that “the act of creating music with one’s voice acted as a metaphor for having a voice and being heard” (p. 20). 14 A narrative review of group singing interventions for pain management (13 studies) reported mixed results. 20 However, this review included a mix of controlled trials that employed various control conditions, non-controlled studies, and qualitative studies, and wide-ranging populations (eg, benign chronic pain, malignant pain, stroke, Alzheimer’s disease).
Our protocol also encouraged participants to use body percussion and instruments to play along with the music. Prior research has suggested that sensorimotor synchronization with music amplifies its hypoalgesic effects. 21
Our findings indicate that participants developed greater symptom-related self-efficacy. Active music-making and focused music listening strategies likely enhance self-efficacy more than passive music listening because it positions patients as creators rather than just recipients of care. When patients actively engage with music, they develop new skills, exercise creative control, and experience tangible achievements. This shift from passive recipient to active participant can fundamentally alter how they view themselves—from someone who feels victimized by cancer and chronic pain to someone who can create, learn, and accomplish goals. This aligns with broader pain management research showing that patients who actively participate in their treatment plans and practice pain management strategies often experience better outcomes.22,23 Analysis also revealed that increased self-efficacy contributed to greater pain acceptance. Participants reported that having more pain management strategies allowed them to stop “acting like it don’t exist.” This causal explanation presents an intriguing contrast to existing literature, which typically positions pain acceptance as a precursor to enhanced self-efficacy and functional improvement.24,25
Finally, several participants shared that applying music-based strategies helped them to reduce pain medication intake, especially at nighttime. The effectiveness of music interventions for sleep enhancement has been well-documented across diverse health conditions, including cancer, insomnia, dementia, and chronic pain.26,27
Some participants initially doubted that MT could effectively manage their pain. This skepticism is valid—when dealing with serious conditions like cancer and chronic pain, MT might seem too simple or unconventional to be effective. Healthcare providers should therefore emphasize that MT is an evidence-based treatment option with documented success in pain management. Patient acceptance of a new intervention is crucial, as research demonstrates that treatment expectations significantly influence therapeutic outcomes. 28
Our analysis revealed that music proved essential in fostering early therapeutic rapport, a protective factor in preventing premature therapy termination. 29 Through shared musical experiences, participants developed trust and felt deeply cared for. This aligns with Skånland and Trondalen’s findings that shared aesthetic experiences through music foster mutuality and intimacy between clients and therapists. 30 Similarly, Lynch et al 31 found that allowing cancer patients to choose their songs and instruments enhanced the meaningfulness of MT sessions. In our study, participants felt particularly heard and valued when therapists honored their musical preferences. While research has long established that patient-preferred music is more effective at reducing pain than unfamiliar or disliked music,5,32 the relational significance of respecting musical preferences is rarely examined in music for pain management literature. Our findings suggest that honoring patients’ musical choices validates their voice and gives them a sense of control—particularly meaningful for individuals managing both chronic pain and life-threatening illnesses.
This study had several strengths and limitations. The analysis of 25 interviews allowed for data saturation to be reached. The sample included representation across cancer diagnoses, age and race. However, there was limited diversity in ethnicity and 80% of the interviewees were female participants. Finally, a sampling bias may exist in our findings, as participants who experienced positive outcomes from MT may have been more inclined to agree to an interview than those who found it less beneficial.
Conclusion
Our study expands the traditional understanding of music’s role in pain management, which primarily emphasizes distraction and relaxation mechanisms. While these remain important components, our findings reveal MT’s broader psychosocial impact on pain experience through multiple pathways: stress reduction, emotional expression through music, active music engagement, enhanced self-efficacy through music-based coping strategies, and therapeutic connection and support through shared musical experiences. Despite music’s ubiquitous presence in daily life, patients often lack knowledge about its therapeutic potential for pain management. Incorporating board-certified music therapists into psycho-oncology teams can help bridge this gap, enabling patients to effectively harness music as a daily tool for symptom management. However, integration of non-pharmacological therapies into standard care for pain management requires that cancer care centers prioritize such therapies in their financial and operational planning to ensure equitable access. 8
Supplemental Material
sj-docx-1-ict-10.1177_15347354251395283 – Supplemental material for Beyond Distraction: Music Therapy for Chronic Pain Management in People with Advanced Cancer
Supplemental material, sj-docx-1-ict-10.1177_15347354251395283 for Beyond Distraction: Music Therapy for Chronic Pain Management in People with Advanced Cancer by Joke Bradt, Lynn Gumert, Carrie Cottone, Ming Yuan Low, Clarissa Lacson, Kate Myers-Coffman, Karolina Bryl, Preethi Selvan, Jacelyn Biondo, Allison Millstein, Anna Cephas, Stephenie Sofield, Brooke Worster and Amy E. Leader in Integrative Cancer Therapies
Footnotes
Acknowledgements
We extend our gratitude to the study participants and hospital staff members for their assistance with trial recruitment.
ORCID iDs
Ethical Considerations
The study was approved by the Drexel University Institutional Review Board (protocol: 1709005627).
Consent to Participate
All participants provided written informed consent prior to participation in this study.
Author Contributions
Joke Bradt (obtained funding, supervision, coding, manuscript), Lynn Gumert (coding, manuscript), Carrie Cottone (coding, manuscript), Ming Yuan Low (coding, manuscript), Clarissa Lacson (coding, manuscript), Kate Myers-Coffman (study coordination), Karolina Bryl (study coordination), Preethi Selvan (site study coordination), Jacelyn Biondo (study coordination), Allison Millstein (interventionist), Anna Cephas (interventionist), Stephenie Sofield (interventionist), Brooke Worster (supervision), Amy E. Leader (supervision). All authors critically reviewed and approved the final version of the manuscript.
Funding
The authors disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This work was supported by the National Institute of Nursing Research of the National Institutes of Health (Award Number R01NR016681). The content is solely the responsibility of the authors and does not necessarily represent the official views of the National Institutes of Health. The study’s funder was not involved in the study’s design, data collection, analysis, interpretation, or manuscript preparation.
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Data Availability Statement
The dataset generated and analyzed during the current study are not publicly available due to reasons of protection of the individual privacy of the participants but are partially available from the corresponding author on reasonable request.
Supplemental Material
Supplemental material for this article is available online.
Clinical Trial Registration
Clinicaltrials.gov NCT03432247
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.